
Effect of Reconstructive Procedures of the Extracranial Segment of the Carotid Arteries on Damage to the Blood–Brain Barrier

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sobieszczyk, P.; Beckman, J. Carotid artery disease. Circulation 2006, 114, e244–e247. [Google Scholar] [CrossRef] [PubMed]
- Andziak, P. Zwężenia tętnic szyjnych wewnętrznych. Chirurgia tętnic i żył pod redakcją W. Noszczyk PZWL 2007, 35, 485–507. [Google Scholar]
- Ederle, J.; Brown, M. The evidence for medicine versus burgery for carotid stenosis. Eur. J. Radiol. 2006, 60, 3–7. [Google Scholar] [CrossRef] [PubMed]
- Flint, A.C.; Bhandari, S.G.; Cullen, S.P.; Reddy, A.V.; Hsu, D.P.; Rao, V.A.; Patel, M.; Pombra, J.; Edwards, N.J.; Chan, S.L. Detection of anterior circulation large artery occlusion in ischemic stroke using noninvasive cerebral oximetry. Stroke 2018, 49, 458–460. [Google Scholar] [CrossRef]
- Lee, J.M.; Zipfel, G.J.; Choi, D.W. The changing landscape of ischaemic brain injury mechanisms. Nature 1999, 399, A7–A14. [Google Scholar] [CrossRef]
- Emerich, D.F.; Dean, R.L.; Bartus, R.T. The role of leukocytes following cerebral ischemia: Pathogenic variable or bystander reaction to emerging infarct? Exp. Neurol. 2002, 173, 168–181. [Google Scholar] [CrossRef]
- McIlvoy, L.H. The effect of hypothermia and hyperthermia on acute brain injury. AACN Adv. Crit. Care 2005, 16, 488–500. [Google Scholar] [CrossRef]
- Kim, K.A.; Kim, D.; Kim, J.H.; Shin, Y.J.; Kim, E.S.; Akram, M.; Kim, E.H.; Majid, A.; Baek, S.H.; Bae, O.N. Autophagy-mediated occludin degradation contributes to blood-brain barrier disruption during ischemia in bEnd.3 brain endothelial cells and rat ischemic stroke models. Fluids Barriers CNS 2020, 17, 21. [Google Scholar] [CrossRef] [Green Version]
- Klionsky, D.J.; Abdelmohsen, K.; Abe, A.; Abedin, M.J.; Abeliovich, H.; Arozena, A.A.; Adachi, H.; Adams, C.M.; Adams, P.D.; Adeli, K.; et al. Guidelines for the use and interpretation of assays for monitoring autophagy (3rd edition). Autophagy 2016, 12, 1–222. [Google Scholar]
- Kago, T.; Takagi, N.; Date, I.; Takenaga, Y.; Takagi, K.; Takeo, S. Cerebral ischemia enhances tyrosine phosphorylation of occludin in brain capillaries. Biochem. Biophys Res. Commun. 2006, 339, 1197–1203. [Google Scholar] [CrossRef]
- Lakhan, S.E.; Kirchgessner, A.; Tepper, D.; Leonard, A. Matrix metalloprotein–ases and blood–brain barrier disruption in acute ischemic stroke. Front. Neurol. 2013, 4, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lok, J.; Zhao, S.; Leung, W.; Seo, J.H.; Navaratna, D.; Wang, X.; Whalen, M.J.; Lo, E.H. Neuregulin-1 effects on endothelial and blood-brain-barrier permeability after experimental injury. Transl. Stroke Res. 2012, 3, S119–S124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, F.; Ohashi, N.; Li, W.; Eckman, C.; Nguyen, J.H. Disruptions of occluding and claudin-5 in brain endothelial cells in vitro and in brains of mice with acute liver failure. Hepatology 2009, 50, 1914–1923. [Google Scholar] [CrossRef] [Green Version]
- Switzer, J.A.; Hess, D.C.; Ergul, A.; Waller, J.L.; Machado, L.S.; Portik-Dobos, V.; Pettigrew, L.C.; Clark, W.M.; Fagan, S.C. MatrixMetalloproteinase-9 in an Exploratory Trial of Intravenous Minocycline for Acute Ischemic Stroke. Stroke 2011, 42, 2633–2635. [Google Scholar] [CrossRef] [Green Version]
- Panickar, K.S.; Anderson, R.A. Effect of polyphenols on oxidative stress and mitochondrial dysfunction in neuronal death and brain edema in cerebral ischemia. Int. J. Mol. Sci. 2011, 12, 8181–8207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dobrogowska, D.H.; Vorbrodt, A.W. Immunogold localization of tight junctional proteins in normal and osmotically-affected rat blood-brain barrier. J. Mol. Histol. 2004, 35, 529–539. [Google Scholar] [CrossRef]
- Simard, M.; Arcuino, G.; Takano, T.; Liu, Q.S.; Nedergaard, M. Signalling at the gliovascular interface. J. Neurosci. 2003, 23, 9254–9262. [Google Scholar] [CrossRef]
- Kilminster, S.; Treasure, T.; McMillan, T.; Holt, D.W. Neuropsychological change and S-100 protein release in 130 unselected patients undergoing cardiac surgery. Stroke 1999, 30, 1869–1874. [Google Scholar] [CrossRef] [Green Version]
- Liapis, C.; Bell, S.P.; Mikhailidis, D.; Sivenius, J.; Nicolaides, A.; e Fernandes, J.F.; Biasi, G.; Norgren, L. ESVS guidelines. Invasive treatment for carotid stenosis: Indications, techniques. Eur. J. Vasc. Endovasc. Surg. 2009, 37, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Staikov, I.N.; Arnold, M.; Mattle, H.P.; Remonda, L.; Sturzenegger, M.; Baumgartner, R.W.; Schroth, G. Comparison of the ECST, CC, and NASCET grading methods and ultrasound for assessing carotid stenosis. European Carotid Surgery Trial. North American Symptomatic Carotid Endarterectomy Trial. J. Neurol. 2000, 247, 681–686. [Google Scholar] [CrossRef]
- Goyal, M.; Menon, B.K.; Van Zwam, W.H.; Dippel, D.W.J.; Mitchell, P.J.; Demchuk, A.M.; Dávalos, A.; Majoie, C.B.L.M.; Van Der Lugt, A.; De Miquel, M.A.; et al. Endovascular thrombectomy after large-vessel ischaemic stroke: A meta-analysis of individual patient data from five randomised trials. Lancet 2016, 387, 1723–1731. [Google Scholar] [CrossRef]
- Baek, J.H.; Kim, B.M.; Kim, D.J.; Heo, J.H.; Nam, H.S.; Yoo, J. Stenting as a Rescue Treatment after Failure of Mechanica Thrombectomy for Anterior Circulation Large Artery Occlusion. Stroke 2016, 47, 2360–2363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kimmel, E.R.; Al Kasab, S.; Harvey, J.B.; Bathla, G.; Ortega-Gutierrez, S.; Toth, G.; Jaksich, E.M.; Sheharyar, A.; Roa, J.; Hasan, D.M.; et al. Absence of Collaterals is Associated with Larger Infarct Volume and Worse Outcome in Patients with Large Vessel Occlusion and Mild Symptoms. J. Stroke Cerebrovasc. Dis. 2019, 28, 1987–1992. [Google Scholar] [CrossRef] [PubMed]
- Constantinou, J.; Jayia, P.; Hamilton, G. Best evidence for medical therapy for carotid artery stenosis. J. Vasc. Surg. 2013, 58, 1129–1139. [Google Scholar] [CrossRef] [Green Version]
- Wu, T.Y.; Anderson, N.E.; Barber, P.A. Neurological complications of carotid revascularization. J. Neurol. Neurosurg. Psychiatry 2012, 83, 543–550. [Google Scholar] [CrossRef]
- Terlecki, P.; Wroński, J.; Przywara, S.; Zubilewicz, T.; Feldo, M.; Kobusiwicz, W.; Kęsik, J.; Iłżecki, M.; Kropski, W. Urgent and early carotid revascularization in selected patients with acute ischemic stroke. II Międzynarodowe Sympozjum Naukowe “Środowiskowe źródła zagrożeń zdrowotnych. In Kazimierz Dolny 2007; Wydawnictwo Polihymnia: Lublin, Poland, 2007; Volume 2, p. 665. [Google Scholar]
- Rapp, J.H.; Wakil, L.; Sawhney, R.; Pan, X.M.; Yenari, M.A.; Glastonbury, C.; Coogan, S.; Wintermark, M. Subclinical embolization after carotid artery stenting: New lesions on diffusion-weighted magnetic resonance imaging occur postprocedure. J. Vasc. Surg. 2007, 45, 867–874. [Google Scholar] [CrossRef] [Green Version]
- Feiwell, R.J.; Besmertis, L.; Sardar, R.; Saloner, D.A.; Rapp, J.H. Detection of clinically silent infarcts after carotid endarterectomy by use of diffusionweighted imaging. Am. J. Neuroradiol. 2001, 22, 646–649. [Google Scholar]
- Roh, H.G.; Byun, H.S.; Ryoo, J.W.; Na, D.G.; Moon, W.-J.; Lee, B.B.; Kim, D.-I. Prospective analysis of cerebral infarction after carotid endarterectomy and carotid artery stent placement by using diffusion-weighted imaging. Am. J. Neuroradiol. 2005, 26, 376–384. [Google Scholar]
- Arkadiusz Szarmach, G.H. Carotid Artery Stenting and Blood–Brain Barrier Permeability in Subjects with Chronic Carotid Artery Stenosis. Int. J. Mol. Sci. 2017, 18, 1008. [Google Scholar] [CrossRef] [Green Version]
- Feuerstein, G.Z.; Liu, T.; Barone, F.C. Cytokines, inflammation, and brain injury: Role of tumor necrosis factor-alpha. Cerebrovasc. Brain Metab. Rev. 1994, 6, 341–360. [Google Scholar]
- Tarkowski, E.; Rosengren, L.; Blomstrand, C.; Wikkelso, C.; Jensen, C.; Ekholm, S.; Tarkowski, A. Intrathecal release of pro- and anti-inflammatory cytokines during stroke. Clin. Exp. Immunol. 1997, 110, 492–499. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Smith, C.; Shapiro, A.; Monette, R.; Hutchison, J.; Stanimirovic, D. Increased expression of bioactive chemokines inhuman cerebromicrovascular endothelial cells and astrocytes subjected to simulated ischemia in vitro. J. Neuroimmunol. 1999, 101, 148–160. [Google Scholar] [CrossRef]
- Kim, G.W.; Gasche, Y.; Grzeschik, S.; Copin, J.C.; Maier, C.M.; Chan, P.H. Neurodegeneration in striatuminduced by the mitochondrial toxin 3-nitropropionic acid: Role of matrix metalloproteinase-9 in early blood-brain barrier disruption? J. Neurosci. 2003, 23, 8733–8742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iłżecki, M.; Iłżecka, J.; Przywara, S.; Terlecki, P.; Grabarska, A.; Stepulak, A.; Zubilewicz, T. Serum Neuron-Specific Enolase as a Marker of Brain Ischemia-Reperfusion Injury in Patients Undergoing Carotid Endarterectomy. Acta Clin. Croat. 2016, 55, 579–584. [Google Scholar] [CrossRef] [Green Version]
- Jung, J.E.; Kim, G.S.; Chen, H.; Maier, C.M.; Narasimhan, P.; Song, Y.S.; Niizuma, K.; Katsu, M.; Okami, N.; Yoshioka, H.; et al. Reperfusion and neurovascular dysfunction in stroke: From basic mechanisms to potential strategies for neuroprotection. Mol. Neurobiol. 2010, 41, 172–179. [Google Scholar] [CrossRef] [Green Version]
- Abbruscato, T.J.; Davis, T.P. Combination of hypoxia/aglycemia compromises in vitro blood-brain barrier integrity. J. Pharmacol. Exp. Ther. 1999, 289, 668–675. [Google Scholar]
- Fischer, S.; Clauss, M.; Wiesnet, M.; Renz, D.; Schaper, W.; Karliczek, G.F. Hypoxia induces permeability in brain microvessel endothelial cells via VEGF and NO. Am. J. Physiol. 1999, 276, C812–C820. [Google Scholar] [CrossRef]
- Mark, K.S.; Davis, T.P. Cerebral microvascular changes in permeability and tight junctions induced by hypoxia-reoxygenation. Am. J. Physiol. Heart Circ. Physiol. 2002, 282, H1485–H1494. [Google Scholar] [CrossRef] [Green Version]
- Cipolla, M.J.; Crete, R.; Vitullo, L.; Rix, R.D. Transcellular transport as a mechanism of blood-brain barrier disruption during stroke. Front. Biosci. 2004, 9, 777–785. [Google Scholar] [CrossRef] [Green Version]
- Witt, K.A.; Mark, K.S.; Huber, J.; Davis, T.P. Hypoxia-inducible factor and nuclear factor kappa-B activation in blood-brain barrier endothelium under hypoxic/reoxygenation stress. J. Neurochem. 2005, 92, 203–214. [Google Scholar] [CrossRef]
- Yang, F.; Zhang, X.; Sun, Y.; Wang, B.; Zhou, C.; Luo, Y.; Ge, P. Ischemic postconditioning decreases cerebral edema and brain blood barrier disruption caused by relief of carotid stenosis in a rat model of cerebral hypoperfusion. PLoS ONE 2013, 8, e57869. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, X.-R.; Luo, M.; Yan, F.; Zhang, C.-C.; Li, S.-J.; Zhao, H.-P.; Ji, X.-M.; Luo, Y.-M. Ischemic postconditioning diminishes matrix metalloproteinase 9 expression and attenuates loss of the extracellular matrix proteins in rats following middle cerebral artery occlusion and reperfusion. CNS Neurosci. Ther. 2012, 18, 855–863. [Google Scholar] [CrossRef] [PubMed]
- Lukic-Panin, V.; Deguchi, K.; Yamashita, T.; Shang, J.; Zhang, X.; Tian, F.; Liu, N.; Kawai, H.; Matsuura, T.; Abe, K. Free radical scavenger edaravone administration protects against tissue plasminogen activator induced oxidative stress and blood brain barrier damage. Curr. Neurovasc. Res. 2010, 7, 319–329. [Google Scholar] [CrossRef]
- Yang, Y.; Estrada, E.Y.; Thompson, J.F.; Liu, W.; Rosenberg, G.A. Matrix metalloproteinase-mediated disruption of tight junction proteins in cerebral vessels is reversed by synthetic matrix metalloproteinase inhibitor in focal ischemia in rat. J. Cereb. Blood Flow Metab. 2007, 27, 697–709. [Google Scholar] [CrossRef] [PubMed]
- Giebel, S.J.; Menicucci, G.; McGuire, P.G.; Das, A. Matrix metalloproteinases in early diabetic retinopathy and their role in alteration of the blood-retinal barrier. Lab. Investig. 2005, 85, 597–607. [Google Scholar] [CrossRef]
- Wunderlich, M.T.; Ebert, A.D.; Kratz, T.; Goertler, M.; Jost, S.; Herrmann, M. Early neurobehavioral outcome after stroke is related to release of neurobiochemical markers of brain damage. Stroke 1999, 30, 1190–1195. [Google Scholar] [CrossRef]
- Connolly, E.S.; Winfree, C.J.; Rampersad, A.; Sharma, R.; Mack, W.J.; Mocco, J.; Yoshida, K.; Fujiwara, S.; Terasaki, K.; Kawamura, T.; et al. Serum S100B protein levels are correlated with subclinical neurocognitive declines after carotid endarterectomy. Neurosurgery 2001, 49, 1076–1083. [Google Scholar]
- Brightwell, R.; Sherwood, R.; Athanasiou, T.; Hamady, M.; Cheshire, N.J.W. The Neurological Morbidity of Carotid Revascularisation: Using Markers of Cellular Brain Injury to Compare CEA and CAS. Eur. J. Vasc. Endovasc. Surg. 2007, 34, 552–560. [Google Scholar] [CrossRef] [Green Version]
- Capoccia, L.; Speziale, F.; Gazzetti, M.; Mariani, P.; Rizzo, A.; Mansour, W.; Sbarigia, E.; Fiorani, P. Comparative study on carotid revascularization (endarterectomy vs. stenting) using markers of cellular brain injury, neuropsychometric tests, and diffusion-weighted magnetic resonance imaging. J. Vasc. Surg. 2010, 51, 584–591. [Google Scholar] [CrossRef] [Green Version]
- Solenov, E.; Watanabe, H.; Manley, G.T.; Verkman, A.S. Sevenfold-reduced osmotic water permeability in primary astrocyte cultures from AQP-4-deficient mice, measured by a fluorescence quenching method. Am. J. Physiol. Cell. Physiol. 2004, 286, C426–C432. [Google Scholar] [CrossRef]
- Amiry-Moghaddam, M.; Frydenlund, D.S.; Ottersen, O.P. Anchoring of aquaporin-4 in brain: Molecular mechanisms and implications for the physiology and pathophysiology of water transport. Neuroscience 2004, 129, 999–1010. [Google Scholar] [CrossRef] [PubMed]
- Papadopoulos, M.C.; Manley, G.T.; Krishna, S.; Verkman, A.S. Aquaporin-4 facilitates reabsorption of excess fluid in vasogenic brain edema. FASEB J. 2004, 18, 1291–1293. [Google Scholar] [CrossRef] [PubMed]
- Verkman, A.S.; Binder, D.K.; Bloch, O.; Auguste, K.; Papadopoulos, M.C. Three distinct roles of aquaporin-4 in brain functionrevealed by knockout mice. Biochim. Biophys. Acta 2006, 1758, 1085–1093. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higashida, T.; Kreipke, C.W.; Rafols, J.A.; Peng, C.; Schafer, S.; Schafer, P.; Ding, J.Y.; Dornbos, D.; Li, X.; Guthikonda, M.; et al. The role of hypoxia-inducible factor-1alpha, aquaporin-4, and matrix metalloproteinase-9 in blood–brain barrier disruption and brain edema after traumatic brain injury. J. Neurosurg. 2011, 114, 92–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davies, D.C. Blood–brain barrie breakdown In septic encephalopathy and brain tumours. J. Anat. 2002, 200, 639–646. [Google Scholar] [CrossRef]
- Manley, G.T.; Binder, D.K.; Papadopoulos, M.C.; Verkman, A.S. New insights into water transport and edema in the centralnervous system from phenotype analysis of quaporin-4 null mice. Neuroscience 2004, 129, 983–991. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Numer of Patients | % | ||
|---|---|---|---|
| Sex | Female | 21 | 23.9 |
| Male | 67 | 76.1 | |
| Right carotid artery stenosis | Absent | 44 | 50.0 |
| Present | 44 | 50.0 | |
| Left carotid artery stenosis | Absent | 19 | 21.6 |
| Present | 69 | 78.4 | |
| Symptoms | Stroke in anamnesis | 29 | 33.0 |
| TIA in anamnesis | 20 | 22.7 | |
| No symptoms | 39 | 44.3 | |
| Operated side | Right | 33 | 37.5 |
| Left | 55 | 62.5 | |
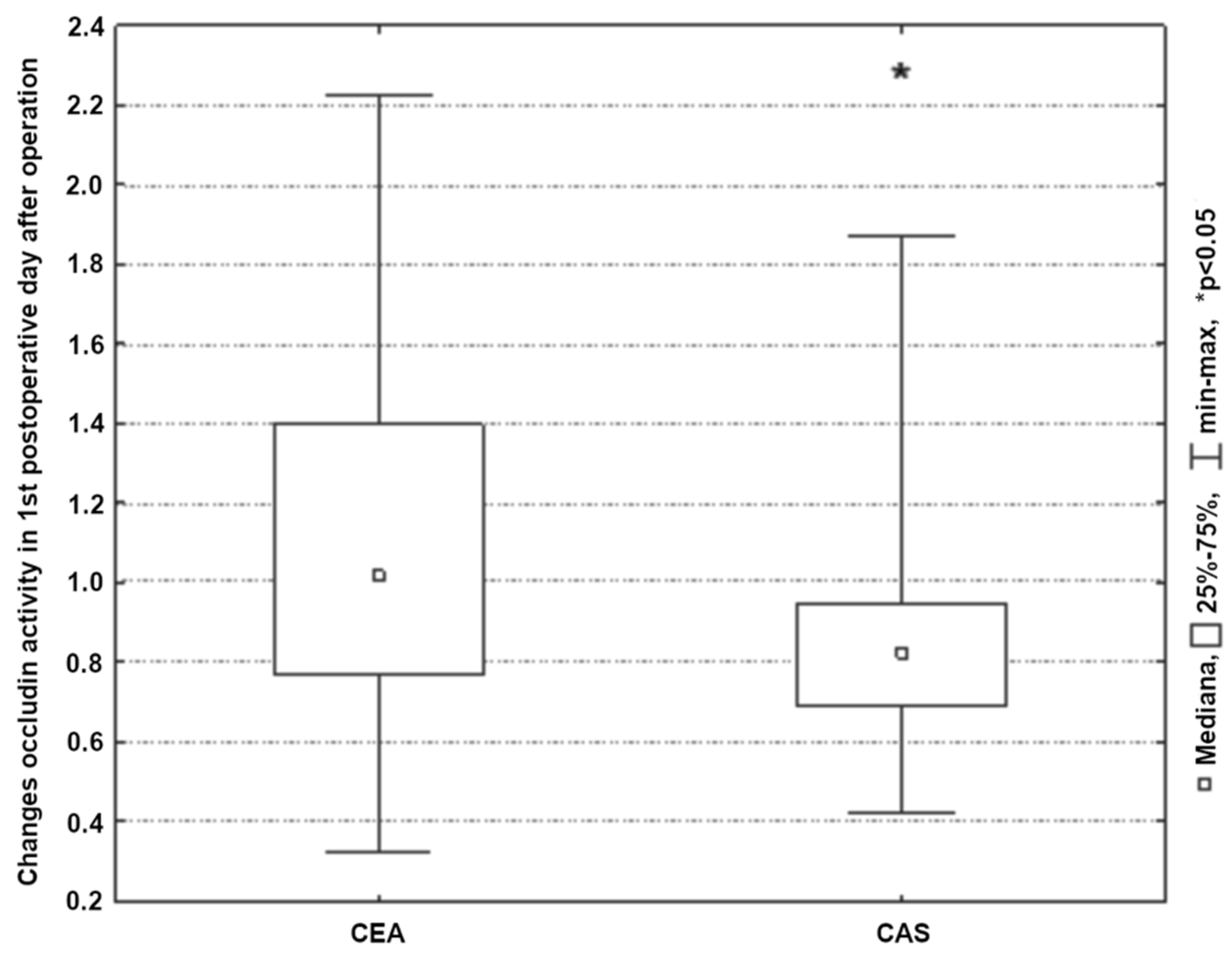
| Type of surgery | CEA | 66 | 75.0 |
| CAS | 22 | 25.0 | |
| Plaque stability post-surgery | Yes | 70 | 79.5 |
| No | 18 | 20.5 |
| Stages of Research | Sum.Rang CEA | Sum.Rang CAS | U | Z | n CEA | n CAS | Statistical Significance |
|---|---|---|---|---|---|---|---|
| 1 | 2694.00 | 1222.00 | 483 | −2.33 | 66 | 22 | p = 0.02 |
| 2 | 2661.50 | 1254.50 | 450 | −2.65 | 66 | 22 | p = 0.01 |
| 3 | 2791.50 | 1124.50 | 580 | −1.40 | 66 | 22 | p = 0.16 |
| 4 | 2781.00 | 1135.00 | 570 | −1.50 | 66 | 22 | p = 0.13 |
| Stages of Research | Plaque | Median | Interquartile Range | Statistical Significance | |
|---|---|---|---|---|---|
| Claudin-1 (ng/mL) | 1 | S | 0.05 | 0.03–0.08 | p = 0.73 |
| U | 0.06 | 0.02–0.11 | |||
| 2 | S | 0.06 | 0.03–0.16 | p = 0.56 | |
| U | 0.06 | 0.02–0.14 | |||
| 3 | S | 0.09 | 0.03–0.20 | p = 0.97 | |
| U | 0.09 | 0.03–0.26 | |||
| 4 | S | 0.13 | 0.07–0.29 | p = 0.23 | |
| U | 0.11 | 0.06–0.17 | |||
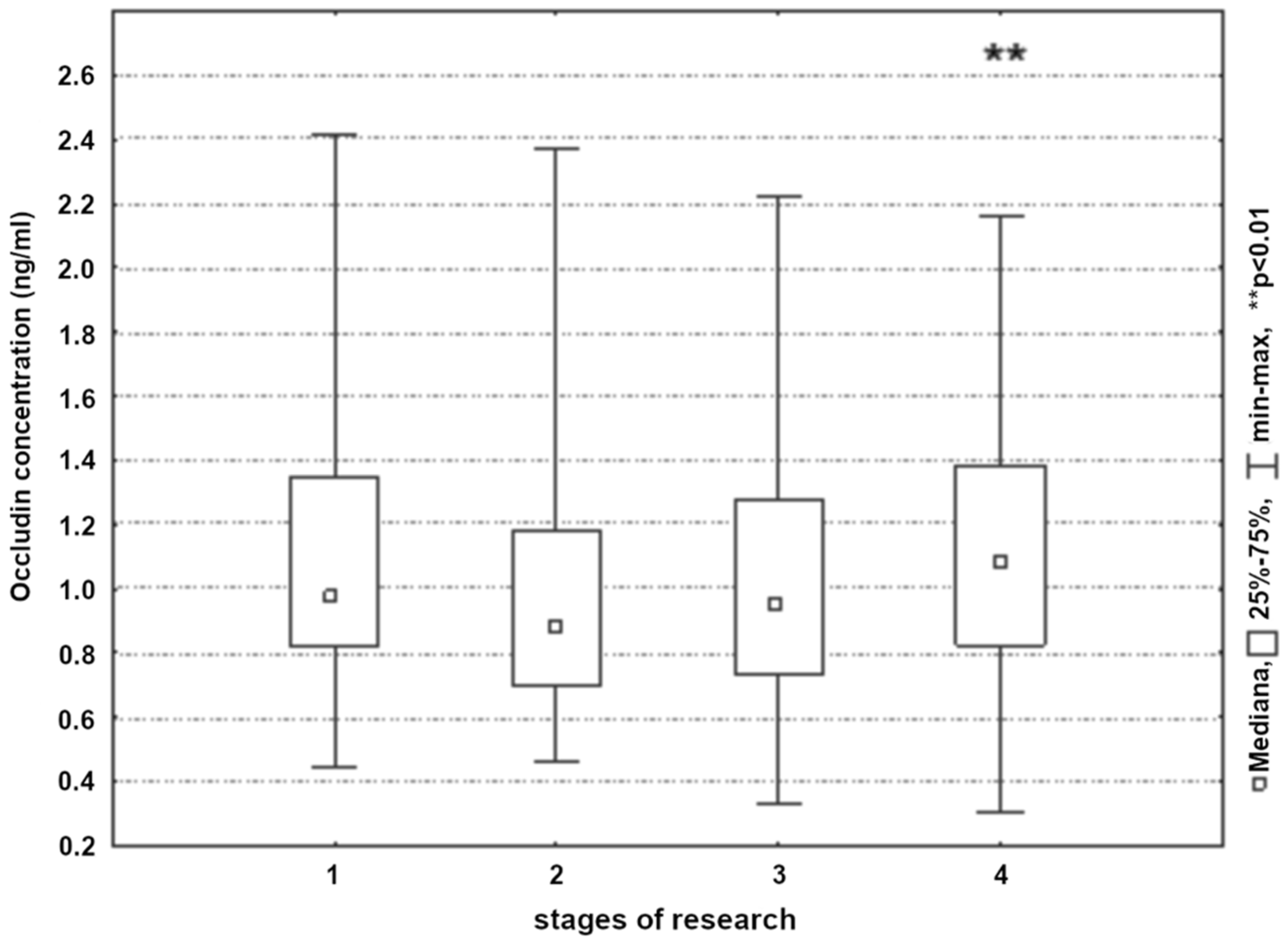
| Occludin (ng/mL) | 1 | S | 0.95 | 0.81–1.36 | p = 0.41 |
| U | 1.05 | 0.94–1.29 | |||
| 2 | S | 0.88 | 0.7–1.18 | p = 0.61 | |
| U | 0.92 | 0.75–1.35 | |||
| 3 | S | 0.94 | 0.7–1.34 | p = 0.49 | |
| U | 1.05 | 0.83–1.26 | |||
| 4 | S | 1.05 | 0.81–1.36 | p = 0.31 | |
| U | 1.1 | 0.94–1.45 | |||
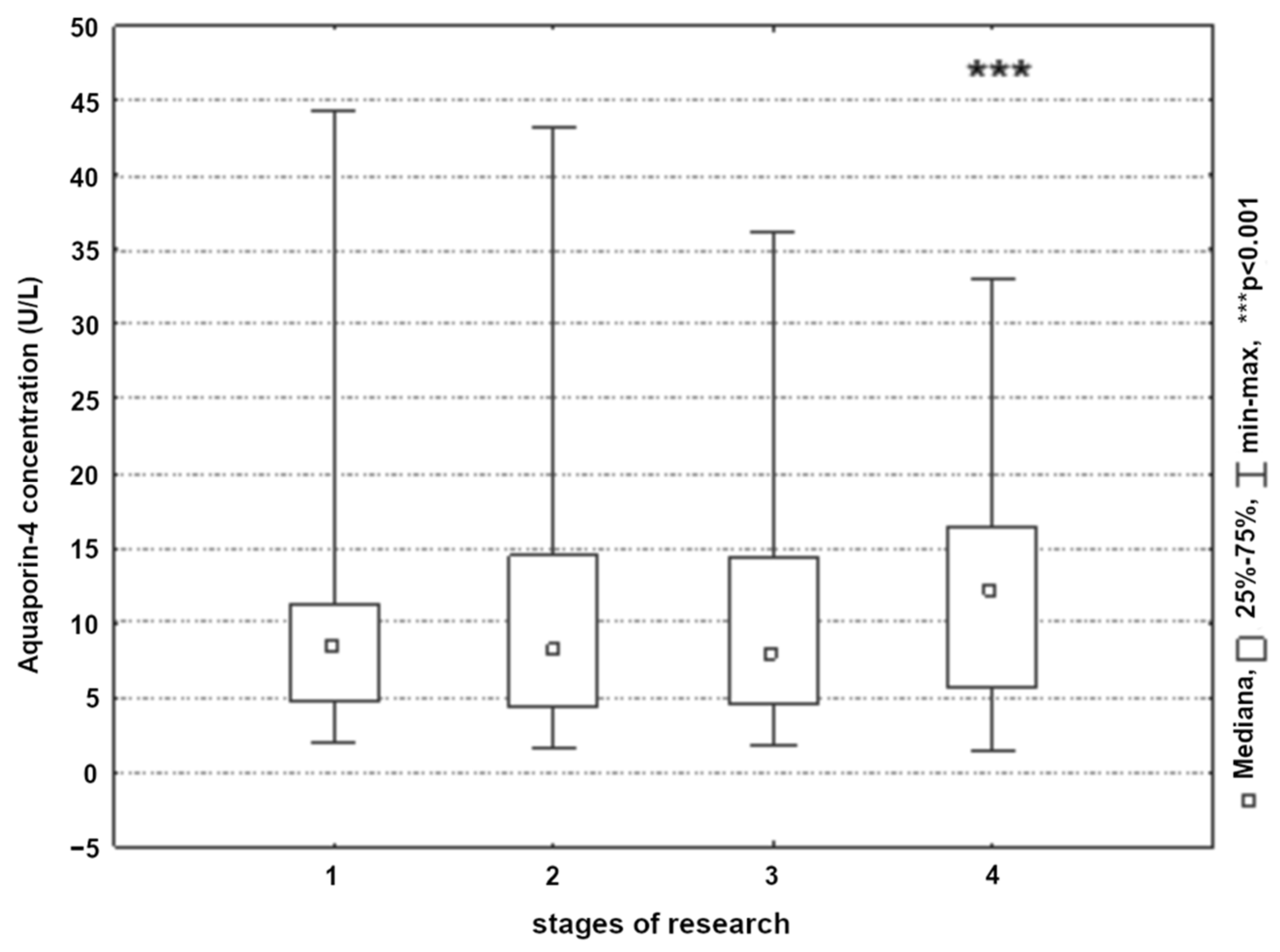
| Aquaporin-4 (U/L) | 1 | S | 7.98 | 5.11–10.59 | p = 0.85 |
| U | 8.67 | 3.92–11.85 | |||
| 2 | S | 7.46 | 4.31–14.29 | p = 0.38 | |
| U | 12.85 | 4.24–16.9 | |||
| 3 | S | 7.11 | 4.37–13.96 | p = 0.19 | |
| U | 10.69 | 5.28–15.55 | |||
| 4 | S | 10.98 | 5.5–15.76 | p = 0.2 | |
| U | 15.86 | 6.37–20.6 | |||
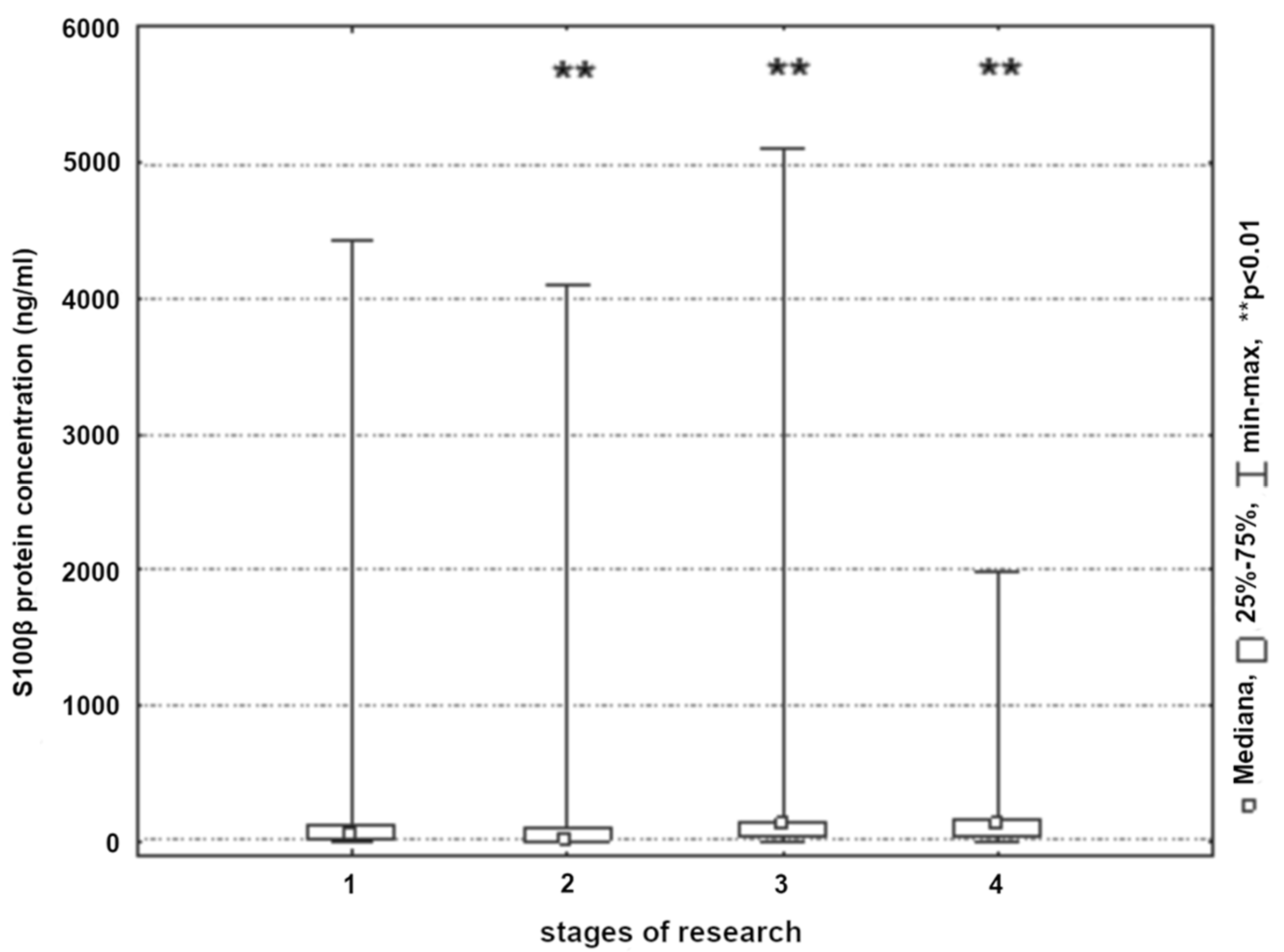
| S100β protein (ng/mL) | 1 | S | 36.24 | 13.35–119.7 | p = 0.02 * |
| U | 4.98 | 2.06–105.8 | |||
| 2 | S | 26.82 | 6.4–108.49 | p = 0.07 | |
| U | 6.49 | 3.43–32.3 | |||
| 3 | S | 109.39 | 59.28–146.54 | p = 0.95 | |
| U | 112.08 | 26.96–153.74 | |||
| 4 | S | 117.94 | 33.1–169.48 | p = 0.26 | |
| U | 63.37 | 4.67–148.6 | |||
| MMP-2 (U/L) | 1 | S | 27,385.83 | 1475.42–109,346.2 | p = 0.89 |
| U | 26,377.89 | 1495.89–72,648.7 | |||
| 2 | S | 18,398.3 | 368.23–78,037.9 | p = 0.72 | |
| U | 14,402.55 | 428.91–72,379.6 | |||
| 3 | S | 20,191.14 | 919.58–73,871.1 | p = 0.65 | |
| U | 14,444.78 | 1081.33–73,571.4 | |||
| 4 | S | 23,236.04 | 543.34–70,777.9 | p = 0.68 | |
| U | 21,306.02 | 1818.70–65,705.8 | |||
| MMP-9 (U/L) | 1 | S | 8577.03 | 1702.92–163,367.7 | p = 0.05 |
| U | 18,161.18 | 561.46–201,649.1 | |||
| 2 | S | 18,856.58 | 1083.04–210,380.5 | p = 0.13 | |
| U | 43,023.42 | 4508.04–135,847.3 | |||
| 3 | S | 15,813.51 | 314.43–200,731.2 | p = 0.36 | |
| U | 18,692.94 | 1367.15–227,834.6 | |||
| 4 | S | 7932.61 | 396.33–138,148.9 | p = 0.1 | |
| U | 24,738.39 | 2729.86–193,071.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Terlecki, P.; Przywara, S.; Terlecki, K.; Janczak, D.; Antkiewicz, M.; Zubilewicz, T. Effect of Reconstructive Procedures of the Extracranial Segment of the Carotid Arteries on Damage to the Blood–Brain Barrier. Int. J. Environ. Res. Public Health 2022, 19, 6210. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106210
Terlecki P, Przywara S, Terlecki K, Janczak D, Antkiewicz M, Zubilewicz T. Effect of Reconstructive Procedures of the Extracranial Segment of the Carotid Arteries on Damage to the Blood–Brain Barrier. International Journal of Environmental Research and Public Health. 2022; 19(10):6210. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106210
Chicago/Turabian StyleTerlecki, Piotr, Stanisław Przywara, Karol Terlecki, Dariusz Janczak, Maciej Antkiewicz, and Tomasz Zubilewicz. 2022. "Effect of Reconstructive Procedures of the Extracranial Segment of the Carotid Arteries on Damage to the Blood–Brain Barrier" International Journal of Environmental Research and Public Health 19, no. 10: 6210. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106210