
Changes in Salivary Immunoglobulin A, Stress, and Burnout in a Workplace Mindfulness Intervention: A Pilot Study



Abstract
:1. Introduction
2. Materials and Methods
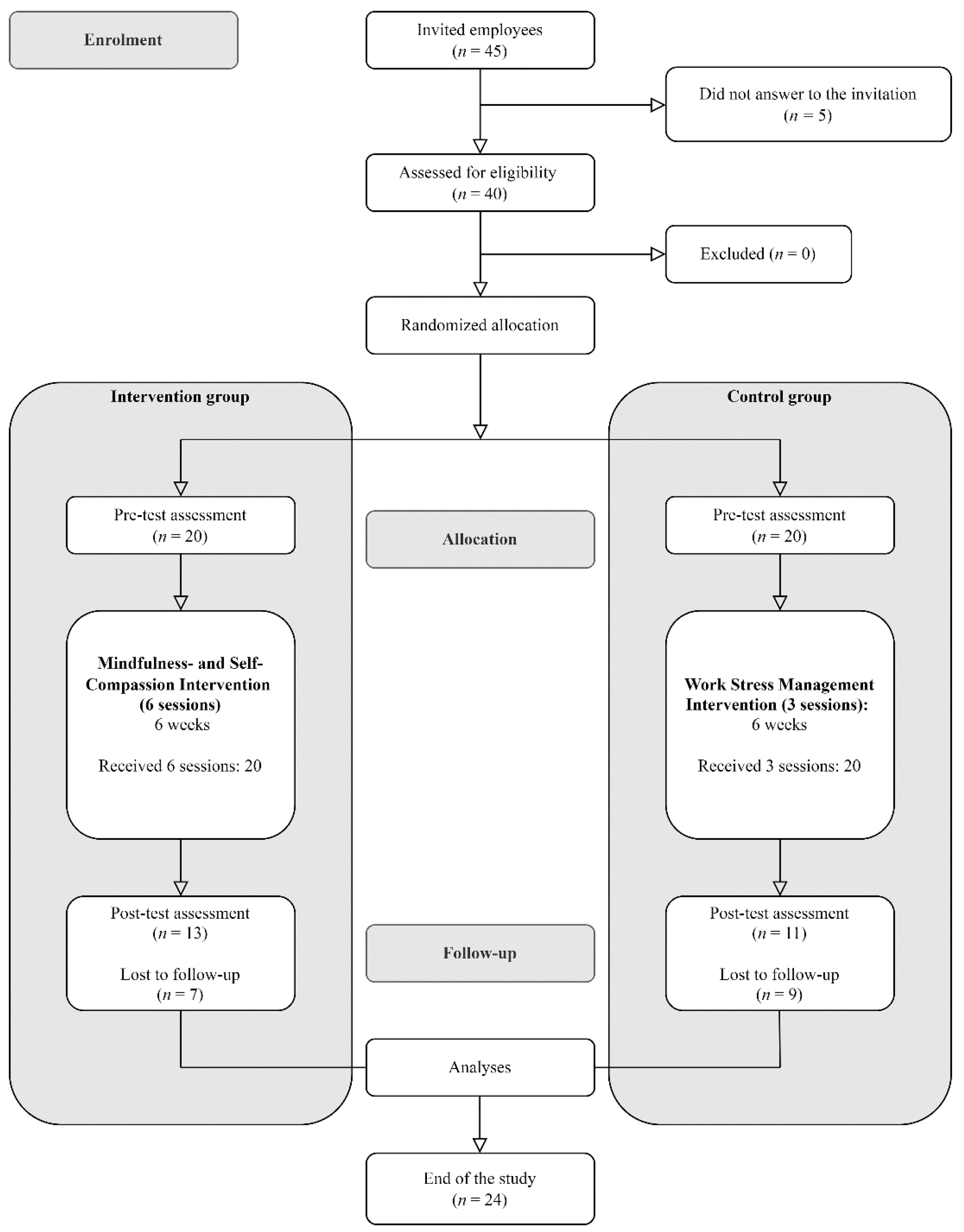
2.1. Participants
2.2. Procedure
2.3. Mindfulness and Self-Compassion Programme
2.4. Workplace Stress Management Intervention
2.5. Measures
2.5.1. Sociodemographic Information
2.5.2. Main Outcomes
2.6. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- European Agency for Safety and Health at Work (EU-OSHA). ESENER 2019—What Does It Tell Us About Safety and Health in Europe’s Workplaces? Office for Official Publications of the European Communities: Luxembourg, 2020. [Google Scholar]
- Siegrist, J.; Wahrendorf, M. Work Stress and Health in a Globalized Economy; Springer: Berlin/Heidelberg, Germany, 2016. [Google Scholar]
- Milczarek, M.; González, E.R.; Schneider, E. OSH in Figures: Stress at Work-Facts and Figures; Office for Official Publications of the European Communities: Luxembourg, 2009. [Google Scholar]
- Goetzel, R.Z.; Long, S.R.; Ozminkowski, R.J.; Hawkins, K.; Wang, S.; Lynch, W. Health, Absence, Disability, and Presenteeism Cost Estimates of Certain Physical and Mental Health Conditions Affecting US Employers. J. Occup. Environ. Med. 2004, 46, 398–412. [Google Scholar] [CrossRef]
- Maslach, C.; Jackson, S.E.; Leiter, M.P. MBI: Maslach Burnout Inventory; Consulting Psychologists Press: Palo Alto, CA, USA, 1996. [Google Scholar]
- Gil-Monte, P.R.; Moreno-Jiménez, B. El Síndrome de Quemarse Por El Trabajo (Burnout). Una Enfermedad Laboral en la Sociedad del Bienestar; Ediciones Pirámide: Madrid, Spain, 2006. [Google Scholar]
- Leiter, M.P.; Maslach, C. The Impact of Interpersonal Environment on Burnout and Organizational Commitment. J. Organ. Behav. 1988, 9, 297–308. [Google Scholar] [CrossRef]
- Pieper, C.; Schröer, S.; Eilerts, A.-L. Evidence of Workplace Interventions—A Systematic Review of Systematic Reviews. Int. J. Environ. Res. Public Health 2019, 16, 3553. [Google Scholar] [CrossRef] [Green Version]
- Jamieson, S.D.; Tuckey, M.R. Mindfulness Interventions in the Workplace: A Critique of the Current State of the Literature. J. Occup. Health Psychol. 2017, 22, 180. [Google Scholar] [CrossRef]
- Bishop, S.R.; Lau, M.; Shapiro, S.; Carlson, L.; Anderson, N.D.; Carmody, J.; Segal, Z.V.; Abbey, S.; Speca, M.; Velting, D. Mindfulness: A Proposed Operational Definition. Clin. Psychol. Sci. Pract. 2004, 11, 230. [Google Scholar] [CrossRef]
- Kersemaekers, W.; Rupprecht, S.; Wittmann, M.; Tamdjidi, C.; Falke, P.; Donders, R.; Speckens, A.; Kohls, N. A Workplace Mindfulness Intervention May Be Associated with Improved Psychological Well-Being and Productivity. A Preliminary Field Study in a Company Setting. Front. Psychol. 2018, 9, 195. [Google Scholar] [CrossRef] [Green Version]
- Allexandre, D.; Bernstein, A.M.; Walker, E.; Hunter, J.; Roizen, M.F.; Morledge, T.J. A Web-Based Mindfulness Stress Management Program in a Corporate Call Center: A Randomized Clinical Trial to Evaluate the Added Benefit of Onsite Group Support. J. Occup. Environ. Med. 2016, 58, 254. [Google Scholar] [CrossRef] [Green Version]
- Khoury, B.; Sharma, M.; Rush, S.E.; Fournier, C. Mindfulness-Based Stress Reduction for Healthy Individuals: A Meta-Analysis. J. Psychosom. Res. 2015, 78, 519–528. [Google Scholar] [CrossRef]
- Krasner, M.S.; Epstein, R.M.; Beckman, H.; Suchman, A.L.; Chapman, B.; Mooney, C.J.; Quill, T.E. Association of an Educational Program in Mindful Communication with Burnout, Empathy, and Attitudes among Primary Care Physicians. Jama 2009, 302, 1284–1293. [Google Scholar] [CrossRef] [Green Version]
- Hyland, P.K.; Lee, R.A.; Mills, M.J. Mindfulness at Work: A New Approach to Improving Individual and Organizational Performance. Ind. Organ. Psychol. 2015, 8, 576–602. [Google Scholar] [CrossRef] [Green Version]
- Kirby, J.N. Compassion Interventions: The Programmes, the Evidence, and Implications for Research and Practice. Psychol. Psychother. Theory Res. Pract. 2017, 90, 432–455. [Google Scholar] [CrossRef]
- Strauss, C.; Taylor, B.L.; Gu, J.; Kuyken, W.; Baer, R.; Jones, F.; Cavanagh, K. What Is Compassion and How Can We Measure It? A Review of Definitions and Measures. Clin. Psychol. Rev. 2016, 47, 15–27. [Google Scholar] [CrossRef] [Green Version]
- Lefebvre, J.-I.; Montani, F.; Courcy, F. Self-Compassion and Resilience at Work: A Practice-Oriented Review. Adv. Dev. Hum. Resour. 2020, 22, 437–452. [Google Scholar] [CrossRef]
- Ferrari, M.; Hunt, C.; Harrysunker, A.; Abbott, M.J.; Beath, A.P.; Einstein, D.A. Self-Compassion Interventions and Psychosocial Outcomes: A Meta-Analysis of RCTs. Mindfulness 2019, 10, 1455–1473. [Google Scholar] [CrossRef]
- Allen, T.D.; Eby, L.T.; Conley, K.M.; Williamson, R.L.; Mancini, V.S.; Mitchell, M.E. What Do We Really Know about the Effects of Mindfulness-Based Training in the Workplace? Ind. Organ. Psychol. 2015, 8, 652–661. [Google Scholar] [CrossRef]
- Saghaei, M. Random allocation software for parallel group randomized trials. BMC Med Res Methodol 2004, 4, 26. [Google Scholar] [CrossRef] [Green Version]
- Levenstein, S.; Prantera, C.; Varvo, V.; Scribano, M.L.; Berto, E.; Luzi, C.; Andreoli, A. Development of the Perceived Stress Questionnaire: A New Tool for Psychosomatic Research. J. Psychosom. Res. 1993, 37, 19–32. [Google Scholar] [CrossRef]
- Montero-Marin, J.; Piva Demarzo, M.M.; Pereira, J.P.; Olea, M.; García-Campayo, J. Reassessment of the Psychometric Characteristics and Factor Structure of the Perceived Stress Questionnaire’(PSQ): Analysis in a Sample of Dental Students. PLoS ONE 2014, 9, e87071. [Google Scholar] [CrossRef] [Green Version]
- Gil-Monte, P.R. Validez Factorial de La Adaptación al Español Del Maslach Burnout Inventory-General Survey. Salud Pública México 2002, 44, 33–40. [Google Scholar] [CrossRef] [Green Version]
- Corthésy, B. Multi-Faceted Functions of Secretory IgA at Mucosal Surfaces. Front. Immunol. 2013, 4, 185. [Google Scholar] [CrossRef] [Green Version]
- Tsujita, S.; Morimoto, K. Secretory IgA in Saliva Can Be a Useful Stress Marker. Environ. Health Prev. Med. 1999, 4, 1–8. [Google Scholar] [CrossRef]
- Raes, F.; Pommier, E.; Neff, K.D.; Van Gucht, D. Construction and Factorial Validation of a Short Form of the Self-Compassion Scale. Clin. Psychol. Psychother. 2011, 18, 250–255. [Google Scholar] [CrossRef]
- López, A.; Sanderman, R.; Smink, A.; Zhang, Y.; Van Sonderen, E.; Ranchor, A.; Schroevers, M.J. A Reconsideration of the Self-Compassion Scale’s Total Score: Self-Compassion versus Self-Criticism. PLoS ONE 2015, 10, e0132940. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Campayo, J.; Navarro-Gil, M.; Andrés, E.; Montero-Marin, J.; López-Artal, L.; Demarzo, M.M.P. Validation of the Spanish Versions of the Long (26 Items) and Short (12 Items) Forms of the Self-Compassion Scale (SCS). Health Qual. Life Outcomes 2014, 12, 4. [Google Scholar] [CrossRef] [Green Version]
- Bond, F.W.; Hayes, S.C.; Baer, R.A.; Carpenter, K.M.; Guenole, N.; Orcutt, H.K.; Waltz, T.; Zettle, R.D. Preliminary Psychometric Properties of the Acceptance and Action Questionnaire–II: A Revised Measure of Psychological Inflexibility and Experiential Avoidance. Behav. Ther. 2011, 42, 676–688. [Google Scholar] [CrossRef] [Green Version]
- Ruiz, F.J.; Herrera, Á.I.L.; Luciano, C.; Cangas, A.J.; Beltrán, I. Measuring Experiential Avoidance and Psychological Inflexibility: The Spanish Version of the Acceptance and Action Questionnaire-II. Psicothema 2013, 25, 123–129. [Google Scholar]
- Bartlett, L.; Martin, A.; Neil, A.L.; Memish, K.; Otahal, P.; Kilpatrick, M.; Sanderson, K. A Systematic Review and Meta-Analysis of Workplace Mindfulness Training Randomized Controlled Trials. J. Occup. Health Psychol. 2019, 24, 108. [Google Scholar] [CrossRef]
- Janssen, M.; Heerkens, Y.; Kuijer, W.; Van Der Heijden, B.; Engels, J. Effects of Mindfulness-Based Stress Reduction on Employees’ Mental Health: A Systematic Review. PLoS ONE 2018, 13, e0191332. [Google Scholar] [CrossRef]
- Calcagni, C.C.; Salanova, M.; Llorens, S.; Bellosta-Batalla, M.; Martínez-Rubio, D.; Borrás, R.M. Differential Effects of Mindfulness-Based Intervention Programs at Work on Psychological Wellbeing and Work Engagement. Front. Psychol. 2021, 12, 715146. [Google Scholar] [CrossRef]
- Kinnunen, S.M.; Puolakanaho, A.; Tolvanen, A.; Mäkikangas, A.; Lappalainen, R. Improvements in Mindfulness Facets Mediate the Alleviation of Burnout Dimensions. Mindfulness 2020, 11, 2779–2792. [Google Scholar] [CrossRef]
- Marshall, E.-J.; Brockman, R.N. The Relationships Between Psychological Flexibility, Self-Compassion, and Emotional Well-Being. J. Cogn. Psychother. 2016, 30, 60–72. [Google Scholar] [CrossRef] [PubMed]
- Atkins, P.W.B.; Parker, S.K. Understanding Individual Compassion in Organizations: The Role of Appraisals and Psychological Flexibility. AMR 2012, 37, 524–546. [Google Scholar] [CrossRef] [Green Version]
- Hashem, Z.; Zeinoun, P. Self-Compassion Explains Less Burnout Among Healthcare Professionals. Mindfulness 2020, 11, 2542–2551. [Google Scholar] [CrossRef] [PubMed]
- Reizer, A. Bringing Self-Kindness Into the Workplace: Exploring the Mediating Role of Self-Compassion in the Associations Between Attachment and Organizational Outcomes. Front. Psychol. 2019, 10, 1148. [Google Scholar] [CrossRef] [PubMed]
- Black, D.S.; Slavich, G.M. Mindfulness Meditation and the Immune System: A Systematic Review of Randomized Controlled Trials. Ann. New York Acad. Sci. 2016, 1373, 13–24. [Google Scholar] [CrossRef] [PubMed]
- Bellosta-Batalla, M.; Ruiz-Robledillo, N.; Sariñana-González, P.; Capella-Solano, T.; Vitoria-Estruch, S.; Hidalgo-Moreno, G.; Pérez-Blasco, J.; Romero-Martínez, Á.; Moya-Albiol, L. Increased Salivary IgA Response as an Indicator of Immunocompetence After a Mindfulness and Self-Compassion-Based Intervention. Mindfulness 2018, 9, 905–913. [Google Scholar] [CrossRef]
- Heckenberg, R.A.; Eddy, P.; Kent, S.; Wright, B.J. Do Workplace-Based Mindfulness Meditation Programs Improve Physiological Indices of Stress? A Systematic Review and Meta-Analysis. J. Psychosom. Res. 2018, 114, 62–71. [Google Scholar] [CrossRef]


{kind=link}
| Baseline Characteristic | MSCBI Condition (n = 20) | WSMI Condition (n = 20) | Full Sample (n = 40) | |||
|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | |
| Age | 41.18 | 9.43 | 42.83 | 11.23 | 41.93 | 10.17 |
| n | % | n | % | n | % | |
| Gender | ||||||
| Female | 7 | 35 | 8 | 40 | 15 | 37.5 |
| Male | 13 | 65 | 12 | 60 | 25 | 62.5 |
| Marital status | ||||||
| Single | 4 | 18.2 | 6 | 30 | 10 | 25 |
| Married | 10 | 50 | 10 | 50 | 20 | 50 |
| Divorced | 5 | 22.7 | 3 | 15 | 8 | 20 |
| Widowed | 1 | 4.5 | 1 | 5 | 2 | 5 |
| Occupation | ||||||
| Entry-level employees | 10 | 50 | 10 | 50 | 20 | 50 |
| Intermediate employees | 8 | 40 | 7 | 35 | 15 | 37.5 |
| Managers | 2 | 10 | 3 | 15 | 5 | 12.5 |
| Session | Program Topic | Meditations and Practices |
|---|---|---|
| Session 1 | Motivation and basic concepts | Awareness of Breath Meditation Exploring the present experience |
| Session 2 | Obstacles to practice Quiet the mind | Body Scan Acknowledgement journal |
| Session 3 | Attention training | Mindfulness of thoughts Walking meditation |
| Session 4 | The attitude of acceptance Relating to the experience | Acceptance and open-mindedness Listen carefully |
| Session 5 | The relationship with oneself A kinder mind | Impartiality and kindness Self-care |
| Session 6 | The relationship with others Compassion | Compassion (and self-compassion) |
| Scale | MSCBI Condition | t (12) | p | η2 | WSMI Condition | t (10) | p | η2 | ANCOVA | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre-Test | Post-Test | Pre-Test | Post-Test | F (1, 21) | p | ηp2 | |||||||
| PSQ | 53.69 (11.30) | 45.77 (12.13) | 2.45 | 0.031 | 0.33 | 54.18 (13.13) | 55.73 (12.38) | −0.79 | 0.448 | 0.06 | 6.64 | 0.018 | 0.24 |
| MBI-EE | 13.08 (7.38) | 6.08 (5.63) | 4.73 | 0.000 | 0.65 | 10.82 (4.98) | 10.82 (5.19) | 0.00 | 1.00 | 0.00 | 14.52 | 0.001 | 0.41 |
| MBI-D | 7.62 (3.99) | 3.85 (3.05) | 3.43 | 0.005 | 0.50 | 3.73 (2.61) | 3.91 (2.74) | −0.26 | 0.800 | 0.01 | 1.61 | 0.219 | 0.07 |
| MBI-PA | 28.85 (4.76) | 29.62 (5.77) | −0.62 | 0.547 | 0.03 | 26.36 (4.48) | 27.64 (4.74) | −1.49 | 0.167 | 0.00 | 0.00 | 0.971 | 0.00 |
| SCS-SF | 9.56 (1.89) | 10.42 (1.54) | −1.98 | 0.071 | 0.25 | 9.20 (1.65) | 8.18 (1.96) | 3.38 | 0.007 | 0.56 | 14.88 | 0.001 | 0.42 |
| AAQII | 21.00 (9.10) | 17.23 (10.22) | 2.52 | 0.027 | 0.35 | 18.55 (7.76) | 22.00 (8.34) | −1.87 | 0.092 | 0.28 | 8.37 | 0.009 | 0.29 |
| Immune Function (sIgA) | MSCBI Condition | t (12) | p | η2 | WSMI Condition | t (10) | p | η2 | ||
|---|---|---|---|---|---|---|---|---|---|---|
| Pre-Test | Post-Test | Pre-Test | Post-Test | |||||||
| First session | 7.44 (3.89) | 14.4 (8.26) | −4.81 | 0.001 | 0.66 | 7.07 (3.46) | 9.89 (8.04) | −1.36 | 0.204 | 0.16 |
| Last session | 5.09 (2.69) | 13.7 (7.14) | −4.95 | 0.000 | 0.67 | 5.38 (1.85) | 8.30 (3.24) | −4.26 | 0.002 | 0.64 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez-Borrás, R.; Navarrete, J.; Bellosta-Batalla, M.; Martínez-Brotóns, C.; Martínez-Rubio, D. Changes in Salivary Immunoglobulin A, Stress, and Burnout in a Workplace Mindfulness Intervention: A Pilot Study. Int. J. Environ. Res. Public Health 2022, 19, 6226. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106226
Martínez-Borrás R, Navarrete J, Bellosta-Batalla M, Martínez-Brotóns C, Martínez-Rubio D. Changes in Salivary Immunoglobulin A, Stress, and Burnout in a Workplace Mindfulness Intervention: A Pilot Study. International Journal of Environmental Research and Public Health. 2022; 19(10):6226. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106226
Chicago/Turabian StyleMartínez-Borrás, Rosa, Jaime Navarrete, Miguel Bellosta-Batalla, Cristina Martínez-Brotóns, and David Martínez-Rubio. 2022. "Changes in Salivary Immunoglobulin A, Stress, and Burnout in a Workplace Mindfulness Intervention: A Pilot Study" International Journal of Environmental Research and Public Health 19, no. 10: 6226. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106226