
Mental and Physical Well-Being and Burden in Palliative Care Nursing: A Cross-Setting Mixed-Methods Study

 , , ,
, , ,
Abstract
:1. Introduction
- -
- What causes of stress do palliative care nurses experience physically and psychologically and how do these affect everyday care?
- -
- How does the experience of stress differ for palliative care nurses across different settings?
- -
- What practical implications can be derived to improve aspects of clinical practice and the work environment to benefit palliative care nurses?
2. Materials and Methods
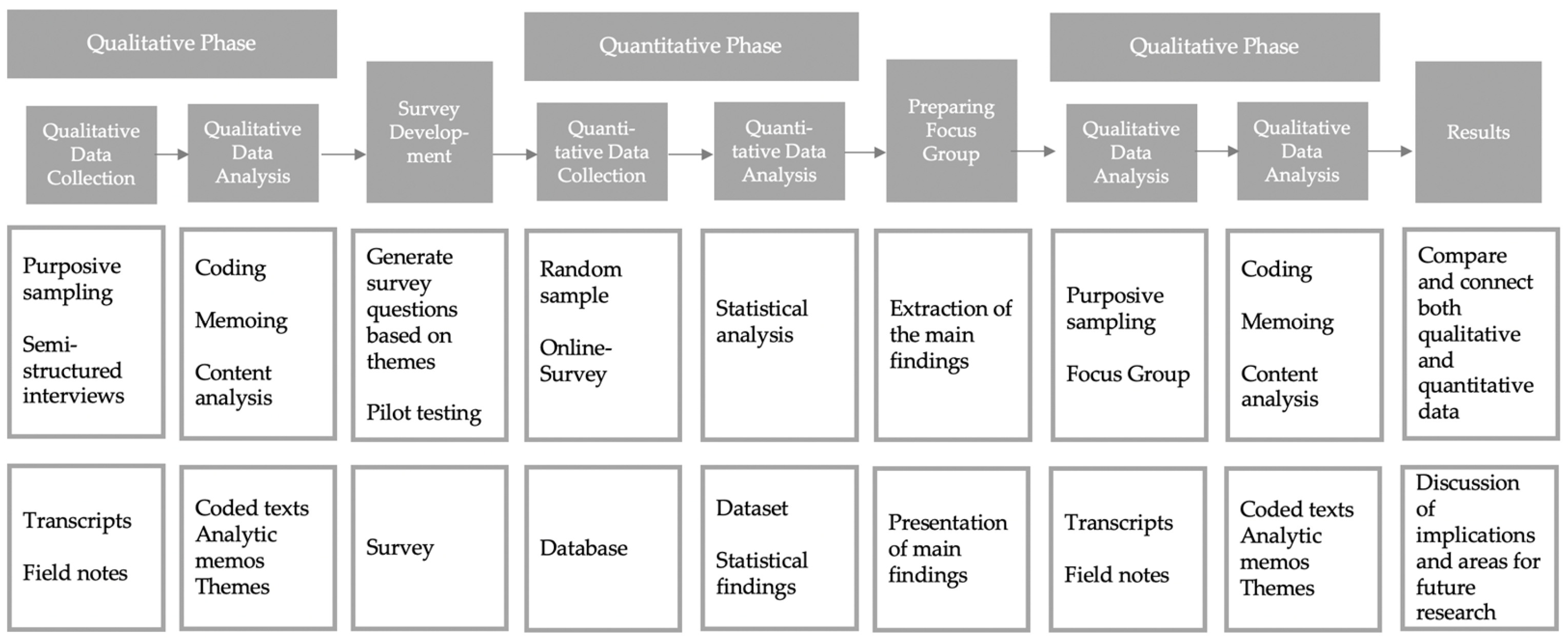
2.1. Study Design
2.2. Expert Interviews
2.3. Survey
2.4. Focus Group
2.5. Qualitative Content Analysis
3. Results
3.1. Expert Interviews
3.1.1. Patient-Related Causes of Stress
“It’s exhausting, you’re already exhausted and we’re also sad and cry with the people. It’s not that I’m desperate that they die. It’s more natural. When many people die, we are also emotionally involved and exhausted. But we are not desperate. On the contrary, I’m really fine. So I often say: “I’m happy”.”(5_PCU, Pos. 90)
3.1.2. Caregiver Related Causes of Stress
““And why can’t you do anything? You have a whole case full. Look at how she’s breathing.”. Well, the fact that we are always in such a pressure situation to really meet the requirements”(11_ SOPC, Pos. 12)
3.1.3. Causes of Stress Related to Working Conditions
3.1.4. Interventions Reducing Burdens
3.2. Survey
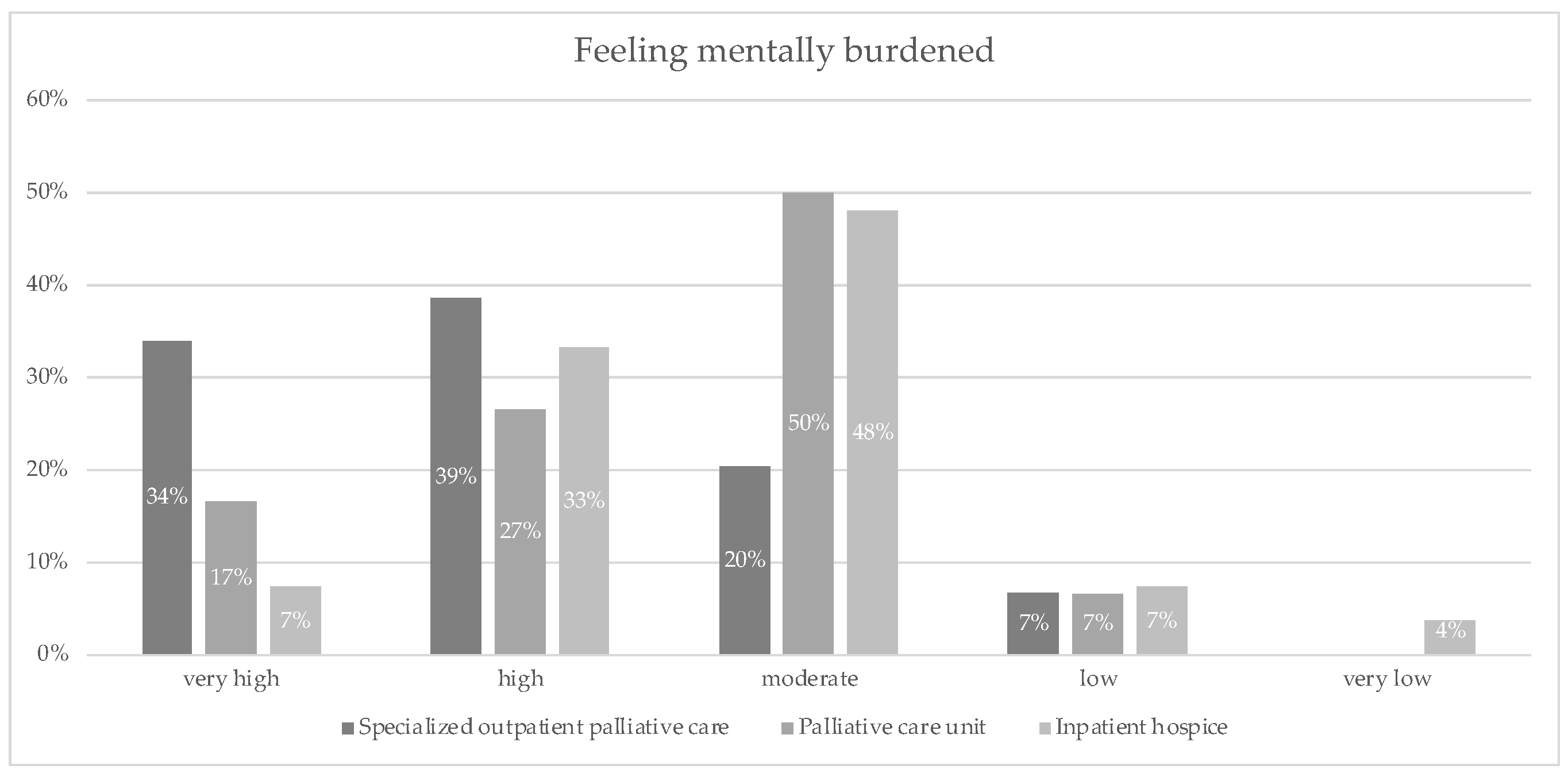
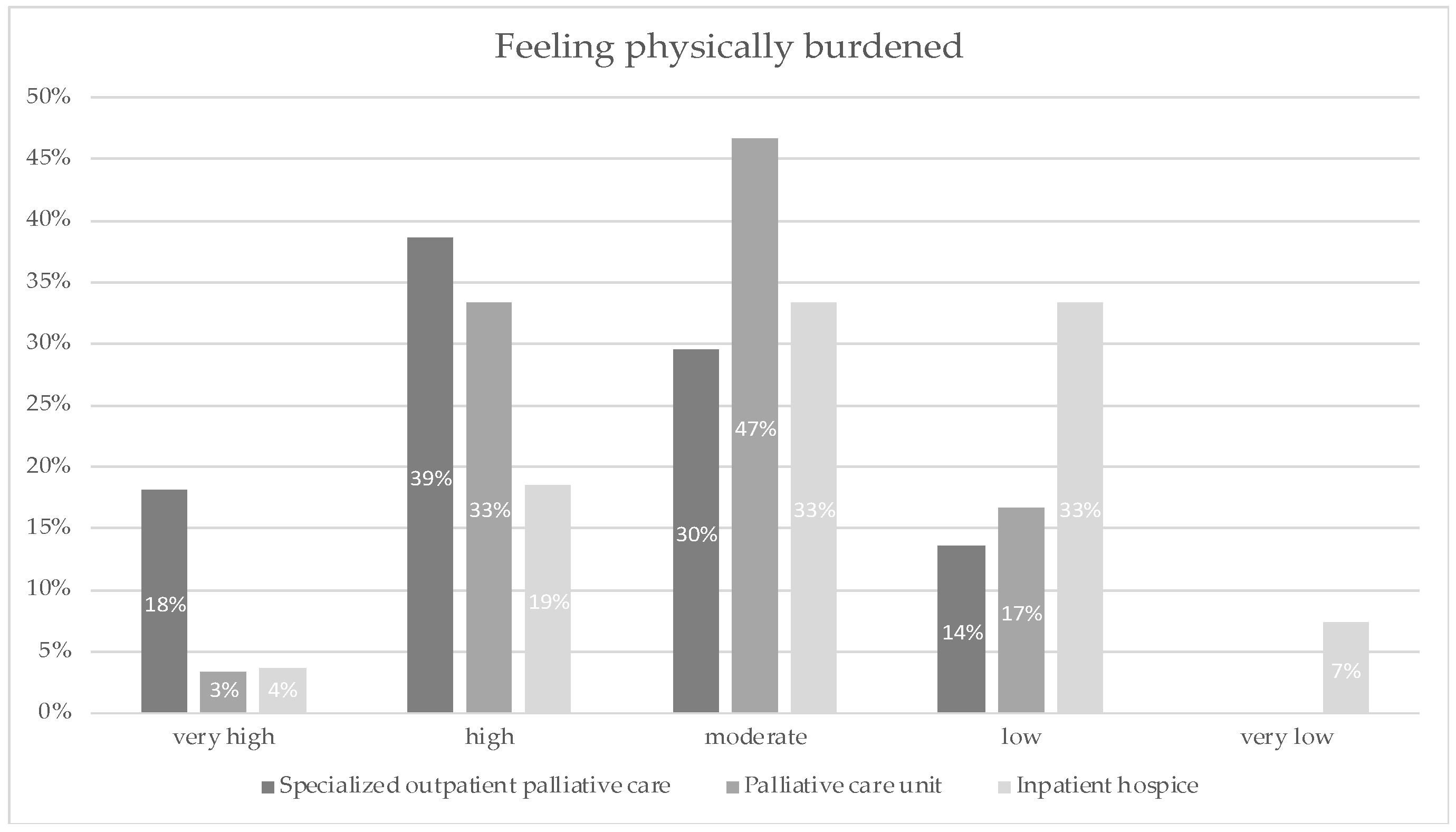
3.2.1. Perceived Mental and Physical Burden
3.2.2. Current Causes of Stress
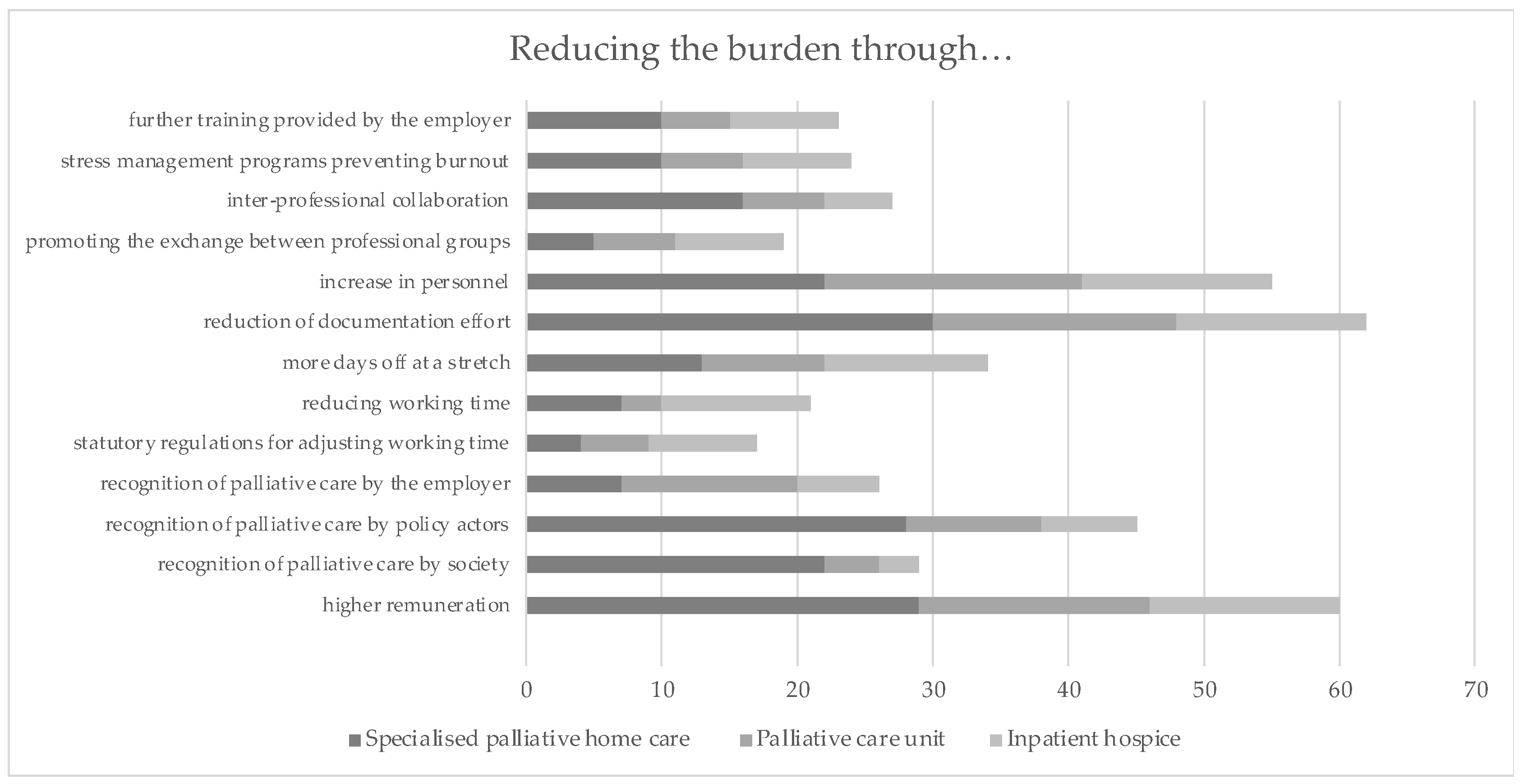
3.2.3. Measures Reducing Burden in Different Palliative Care Settings
3.3. Focus Group
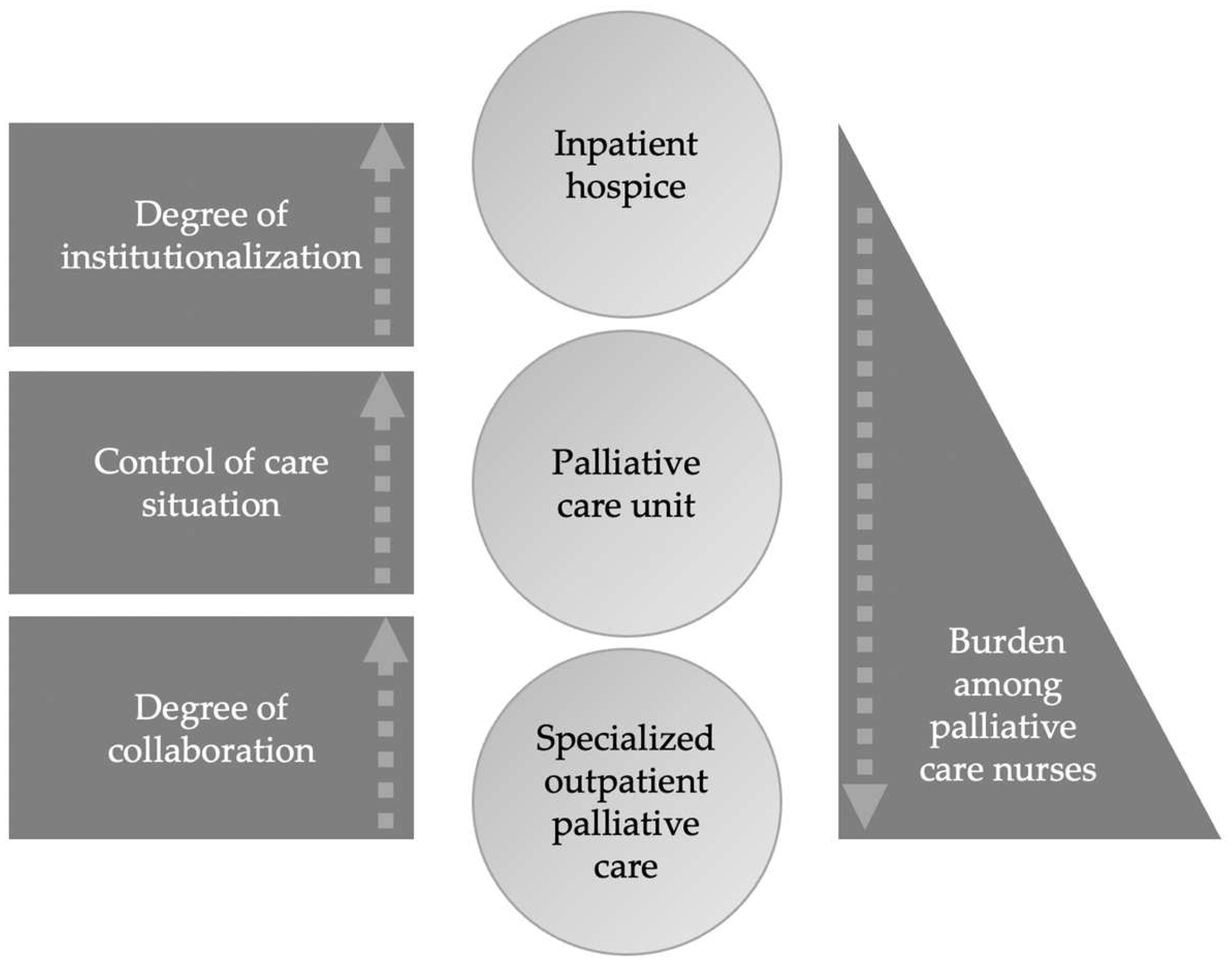
“I could imagine that SOPC might feel more burdensome because they have less control. Something we also said before, is that assistive devices are not at hand. When I’m in a hospice or inpatient setting, I’m at home, in a sense, that’s my professional role, I’m here, the patients come to me. I have all the basic requirements here. That’s not the case at the patients’ home. I first have to bring in aids, I have to get accustomed. Then not all the things I suggest are accepted or tolerated. The family decides. They can’t be implemented as easily as in inpatient care”.(Focus Group, Health Researcher and Nurse, Pos. 21)
“Of course, I am much more stressed in SOPC alone, because the patients are all in different places. In the hospice or in the clinic, I’m always in the same place”.(Focus Group, Coordinator Regional Association for Oncological Care, Pos. 17)
“If you look back at the stress factors we mentioned, then you could start there to relieve the burden and claim that there is enough time for each home visit, calculated distances, parking problems, logistical things that can be resolved quite easily”.(Focus Group, Palliative Care Physician, Pos. 36)
“The other thing that came to my mind spontaneously is that SOPC needs another name. That’s like everybody said, we all know what hospice is, it’s a term, SOPC is relatively new and not established yet”.(Focus Group, Coordinator Regional Association for Oncological Care. Pos. 50)
“I think that the job profile of caregivers, regardless of the level of qualification, means that in general, not only in SOPC, you are often very dependent on others. You are more of a service provider for the person you are caring for. This can also become a burden if you are not well supported and are in a good employment context. I must honestly admit that I speak from experience”.(Focus Group, Health Researcher and Nurse, Pos. 32)
“I assume that most of them are in this profession due to great intrinsic motivation and that they put up with a lot for it. That it’s not just the compensation, but because they enjoy doing it. And see it as personally fulfilling or resource enhancing”.(Focus Group, Health Researcher and Nurse, Pos. 83)
“I also believe that it is not only a question of remuneration, because this is also a social problem. Many young people don’t want to go into the nursing profession. They don’t want to work shifts and nights and drive out when the patient is unwell. That’s something that, from my point of view, is very difficult to overcome”.(Focus Group, Palliative Care Physician, Pos. 74)
“The lack of personnel is a decisive factor. If more staff were available, I think that would lead to greater job satisfaction, because it would solve the time problem. Then you would find more satisfaction and also meaningful fulfilment in your job, and you wouldn’t value the other things so much”.(Focus Group, Palliative Care Physician, Pos. 65)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| PCU | Palliative Care Unit |
| IH | Inpatient Hospice |
| SOPC | Specialized Outpatient Palliative Care |
References
- Worldwide Palliative Care Alliance. Global Atlas of Palliative Care at the End of Life; Worldwide Hospice Palliative Care Alliance: London, UK, 2014. [Google Scholar]
- Fitzsimons, D.; Mullan, D.; Wilson, J.S.; Conway, B.; Corcoran, B.; Dempster, M.; Gamble, J.; Stewart, C.; Rafferty, S.; McMahon, M.; et al. The challenge of patients’ unmet palliative care needs in the final stages of chronic illness. Palliat. Med. 2007, 21, 313–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaertner, J.; Siemens, W.; Meerpohl, J.J.; Antes, G.; Meffert, C.; Xander, C.; Stock, S.; Mueller, D.; Schwarzer, G.; Becker, G. Effect of specialist palliative care services on quality of life in adults with advanced incurable illness in hospital, hospice, or community settings: Systematic review and meta-analysis. BMJ 2017, 357, j2925. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Engeser, P.; Glassman, J.; Leutgeb, R.; Szecsenyi, J.; Laux, G. Early integration of palliative care for outpatients with advanced cancer in general practice: How is the situation?-a cohort study. Ann. Palliat. Med. 2021, 10, 2843–2848. [Google Scholar] [CrossRef] [PubMed]
- Leitlinienprogramm Onkologie (Deutsche Krebsgesellschaft, Deutsche Krebshilfe, AWMF): Palliativmedizin für Patienten mit Einer Nicht-Heilbaren Krebserkrankung, Lang-Version 2.01 (Konsultationsfassung), AWMF-Registernummer: 128/001OL. 2019. Available online: https://www.leitlinienprogramm-onkologie.de/leitlinien/palliativmedizin/ (accessed on 23 June 2021).
- Nantsupawat, A.; Kunaviktikul, W.; Nantsupawat, R.; Wichaikhum, O.-A.; Thienthong, H.; Poghosyan, L. Effects of Nurse Work Environment on Job Dissatisfaction, Burnout, Intention to Leave. Int. Nurs. Rev. 2017, 64, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Teng, C.I.; Hsiao, F.J.; Chou, T.A. Nurse-perceived time pressure and patient-perceived care quality. J. Nurs. Manag. 2010, 18, 275–284. [Google Scholar] [CrossRef] [PubMed]
- Vinckx, M.A.; Bossuyt, I.; Dierckx de Casterlé, B. Understanding the complexity of working under time pressure in oncology nursing: A grounded theory study. Int. J. Nurs. Stud. 2018, 87, 60–68. [Google Scholar] [CrossRef] [PubMed]
- Ingebretsen, L.P.; Sagbakken, M. Hospice nurses’ emotional challenges in their encounters with the dying. Int. J. Qual. Stud. Health Well-Being 2016, 11, 31170. [Google Scholar] [CrossRef]
- Harasym, P.; Brisbin, S.; Afzaal, M.; Sinnarajah, A.; Venturato, L.; Quail, P.; Kaasalainen, S.; Straus, S.E.; Sussman, T.; Virk, N.; et al. Barriers and facilitators to optimal supportive end-of-life palliative care in long-term care facilities: A qualitative descriptive study of community-based and specialist palliative care physicians’ experiences, perceptions and perspectives. BMJ Open 2020, 10, e037466. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Urquiza, J.L.; Albendín-García, L.; Velando-Soriano, A.; Ortega-Campos, E.; Ramí-rez-Baena, L.; Membrive-Jiménez, M.J.; Suleiman-Martos, N. Burnout in Palliative Care Nurses, Prevalence and Risk Factors: A Systematic Review with Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 7672. [Google Scholar] [CrossRef]
- Rohwer, E.; Mojtahedzadeh, N.; Harth, V.; Mache, S. Stressoren, Stresserleben und Stressfolgen von Pflegekräften im ambulanten und stationären Setting in Deutschland. Arb. Ergon. 2021, 71, 38–43. [Google Scholar] [CrossRef]
- Maslach, C.; Schaufeli, W.; Leiter, M. Job burnout. Annu. Rev. Psychol. 2001, 52, 397–422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borritz, M.; Rugulies, R.; Christensen, K.; Villadsen, E.; Kristensen, T. Burnout as a predictor of self-reported sickness absence among human service workers: Prospective findings from three year follow up of the PUMA study. Occup. Environ. Med. 2006, 63, 98–106. [Google Scholar] [CrossRef] [PubMed]
- Parola, V.; Coelho, A.; Cardoso, D.; Sandgren, A.; Apóstolo, J. Prevalence of burnout in health professionals working in palliative care: A systematic review. JBI Database Syst. Rev. Implement Rep. 2017, 15, 1905–1933. [Google Scholar] [CrossRef] [PubMed]
- Poghosyan, L.; Clarke, S.P.; Finlayson, M.; Aiken, L.H. Nurse burnout and quality of care: Cross-national investigation in six countries. Res. Nurs. Health 2010, 33, 288–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lyndon, A. Burnout among Health Professionals and Its Effect on Patient Safety. Available online: https://psnet.ahrq.gov/per-spectives/perspective/190/burnout-among-health-professionals-and-its-effect-on-patient-safety (accessed on 25 June 2017).
- Gapstur, R.L. Symptom burden: A concept analysis and implications for oncology nurses. Oncol. Nurs. Forum. 2007, 34, 673–680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pastrana, T.; De Lima, L.; Pettus, K.; Ramsey, A.; Napier, G.; Wenk, R.; Radbruch, L. The impact of COVID-19 on palliative care workers across the world: A qualitative analysis of responses to open-ended questions. Palliat. Supportive Care 2021, 19, 187–192. [Google Scholar] [CrossRef] [PubMed]
- May, S.; Stahlhut, K.; Allsop, M.; Heinze, M.; Muehlensiepen, F. ‘…you just put up with it for the sake of humanity’: An exploratory qualitative study on causes of stress in palliative care nursing during the COVID-19 pandemic in Germany. BMJ Open 2021, 11, e051550. [Google Scholar] [CrossRef]
- Green, J. COVID-19: A Lasting Impact on District and Community Nursing Teams? RCN DCN Forum COVID-19 Survey Results. 2020. Available online: https://tinyurl.com/y6dc7et7 (accessed on 10 December 2020).
- Green, J.; Doyle, C.; Hayes, S.; Newnham, W.; Hill, S.; Zeller, I.; Graffin, M.; Goddard, G. COVID-19 and district and community nursing. Br. J. Community Nurs. 2020, 25, 213. [Google Scholar] [CrossRef] [PubMed]
- Melching, H. Palliativversorgung—Modul 2-: Strukturen und Regionale Unterschiede in der Hospiz-und Palliativversorgung. Ed. Bertelsmann Stiftung. Gütersloh. 2015. Available online: https://faktencheck-gesundheit.de/fileadmin/files/BSt/Publikationen/GrauePublikationen/Studie_VV__FCG_Versorgungsstrukturen-palliativ.pdf (accessed on 20 May 2020).
- Simon, S.T.; Pralong, A.; Welling, U. Versorgungsstrukturen in der palliativmedizin: Behandlungspfad für patienten mit einer nichtheilbaren krebserkrankung [healthcare structures in palliative care medicine: Flowchart for patients with incurable cancer]. Internist 2016, 57, 953–958. [Google Scholar] [CrossRef]
- German Association for Palliative Medicine: Who Provides What in the Field of Hospice and Palliative Care? Available online: https://www.wegweiser-hospiz-palliativmedizin.de/en (accessed on 14 May 2022).
- Gencer, D.; Meffert, C.; Herschbach, P.; Hipp, M.; Becker, G. Belastungen im Berufsalltag von Palliativpflegekräften-eine Befragung in Mooperation mit dem Kompetenzzentrum Palliative Care Baden-Württemberg (KOMPACT). Das Gesundh. 2019, 81, 92–98. [Google Scholar]
- Diehl, E.; Rieger, S.; Letzel, S.; Nienhaus, A.; Pinzon, L.C. Belastungen und Ressourcen von Pflegekräften der spezialisierten Palliativversorgung—Eine explorative Querschnittstudie. Pflege 2019, 32, 209–223. [Google Scholar] [CrossRef] [PubMed]
- Diehl, E.; Rieger, S.; Letzel, S.; Schablon, A.; Nienhaus, A.; Escobar Pinzon, L.C.; Dietz, P. Burdens, resources, health and wellbeing of nurses working in general and special-ised palliative care in Germany—Results of a nationwide cross-sectional survey study. BMC Nurs. 2021, 20, 162. [Google Scholar] [CrossRef] [PubMed]
- National Academies of Sciences, Engineering, and Medicine; National Academy of Medicine; Committee on Systems. Approaches to Improve Patient Care by Supporting Clinician Well-Being. In Taking Action against Clinician Burnout: A Systems Approach to Professional Well-Being; National Academies Press: Washington, DC, USA, 2019. [Google Scholar]
- Creswell, J.W. Research Design: Qualitative, Quantitative, and Mixed Methods Approaches, 2nd ed.; Sage: Thousand Oaks, CA, USA, 2003. [Google Scholar]
- WMA Declaration of Helsinki. Ethical Principles Med Res Involving Hum Subjects. World Medical Association. 2013. Available online: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/20132013/ (accessed on 21 March 2021).
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Cathain, A.; Murphy, E.; Nicholl, J. The quality of mixed methods studies in health services research. J. Health Serv. Res. Policy 2008, 13, 92–98. [Google Scholar] [CrossRef]
- Witzel, A. Das Problemzentrierte Interview; Forum: Qualitative Sozialforschung, Art 2000; Beltz: Weinheim, Germany, 1985; Volume 1, p. 22. [Google Scholar]
- Etikan, I.; Musa, S.A.; Alkassim, R.S. Comparison of convenience sampling and purposive sampling. Am. J. Theor. Appl. Stat. 2016, 5, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Conover, W.J. Practical Non-Parametric Statistics; John Wiley & Sons: New York, NY, USA, 1999. [Google Scholar]
- Signorell, A.; Aho, K.; Alfons, A.; Anderegg, N.; Aragon, T.; Arachchige, C.; Arppe, A.; Baddeley, A.; Barton, K.; Bolker, B.; et al. DescTools: Tools for Descriptive Statistics. R Package Version 0.99.44. 2021. Available online: https://cran.r-project.org/package=DescTools (accessed on 4 April 2022).
- Armitage, P. Tests for Linear Trends in Proportions and Frequencies. Biom. Int. Biom. Soc. 1955, 11, 375–386. [Google Scholar] [CrossRef] [Green Version]
- Kuckartz, U. Qualitative Inhaltsanalyse; Beltz Juventa: Weinheim, Germany, 2018. [Google Scholar]
- Seipp, H.; Haasenritter, J.; Hach, M.; Becker, D.; Ulrich, L.R.; Schütze, D.; Engler, J.; Michel, C.; Bösner, S.; Kuss, K. How can we ensure the success of specialised palliative home-care? A qualitative study (ELSAH) identifying key issues from the perspective of patients, relatives and health professionals. Palliat. Med. 2021, 35, 1844–1855. [Google Scholar] [CrossRef] [PubMed]
- Monsalve-Reyes, C.S.; San Luis-Costas, C.; Gómez-Urquiza, J.L.; Albendín-García, L.; Aguayo, R.; Cañadas-De la Fuente, G.A. Burnout syndrome and its prevalence in primary care nursing: A systematic review and meta-analysis. BMC Fam. Pract. 2018, 19, 59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gómez-Urquiza, J.L.; De la Fuente-Solana, E.I.; Albendín-García, L.; Vargas-Pecino, C.; Ortega-Campos, E.M.; Cañadas-De la Fuente, G.A. Prevalence of burnout syndrome in emergency nurses: A meta-analysis. Crit. Care Nurse 2017, 37, e1–e9. [Google Scholar] [CrossRef] [Green Version]
- See, K.C.; Zhao, M.Y.; Nakataki, E.; Chittawatanarat, K.; Fang, W.F.; Faruq, M.O.; Wahjuprajitno, B.; Arabi, Y.M.; Wong, W.T.; Divatia, J.V.; et al. Professional burnout among physicians and nurses in Asian intensive care units: A multinational survey. Intensive Care Med. 2018, 44, 2079–2090. [Google Scholar] [CrossRef] [PubMed]
- Koh, M.Y.; Chong, P.H.; Neo, P.S.; Ong, Y.J.; Yong, W.C.; Ong, W.Y.; Shen, M.L.; Hum, A.Y. Burnout, psychologi-cal morbidity and use of coping mechanisms among palliative care practitioners: A multi-centre cross-sectional study. Palliat. Med. 2015, 29, 633–642. [Google Scholar] [CrossRef] [PubMed]
- Ercolani, G.; Varani, S.; Peghetti, B.; Franchini, L.; Malerba, M.B.; Messana, R.; Sichi, V.; Pannuti, R.; Pannuti, F. Burnout in Home Palliative Care: What Is the Role of Coping Strategies? J. Palliat. Care 2020, 35, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Garcia, C.D.L.; Abreu, L.C.D.; Ramos, J.L.S.; Castro, C.F.D.D.; Smiderle, F.R.N.; Santos, J.A.D.; Bezerra, I.M.P. Influence of Burnout on Patient Safety: Systematic Review and Meta-Analysis. Medicina 2019, 55, 553. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salyers, M.P.; Bonfils, K.A.; Luther, L.; Firmin, R.L.; White, D.A.; Adams, E.L.; Rollins, A.L. The Relationship between Professional Burnout and Quality and Safety in Healthcare: A Meta-Analysis. J. Gen. Intern. Med. 2017, 32, 475–482. [Google Scholar] [CrossRef] [PubMed]
- Pastrana, T.; De Lima, L.; Pettus, K.; Ramsey, A.; Napier, G.; Wenk, R.; Radbruch, L. Impact of COVID-19 Pandemic on Palliative Care Workers: An International Cross-sectional Study. Indian J. Palliat. Care 2021, 27, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Diehl, E.; Rieger, S.; Letzel, S.; Schablon, A.; Nienhaus, A.; Escobar Pinzon, L.C.; Dietz, P. Health and intention to leave the profession of nursing—Which individual, social and organisational resources buffer the impact of quantitative demands? A cross-sectional study. BMC Palliat. Care 2020, 19, 83. [Google Scholar] [CrossRef]
- Dean, W.; Talbot, S.; Dean, A. Reframing Clinician Distress: Moral Injury Not Burnout. Fed. Pract. 2019, 36, 400–402. [Google Scholar] [PubMed]
- Linzer, M.; Poplau, S. Eliminating burnout and moral injury: Bolder steps required. EClinicalMedicine 2021, 39, 101090. [Google Scholar] [CrossRef] [PubMed]
- Dzeng, E.; Curtis, J.R. Understanding ethical climate, moral distress, and burnout: A novel tool and a conceptual framework. BMJ Qual. Saf. 2018, 27, 766–770. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gesetz zur Verbesserung der Hospiz-und Palliativversorgung in Deutschland (Hospiz-und Palliativgesetz—HPG). 2015. Available online: http://www.bgbl.de/xaver/bgbl/start.xav?startbk=Bundesanzeiger_BGBl&jumpTo=bgbl115s2114.pdf (accessed on 25 April 2022).
- Magnet Hospitals. Attraction and Retention of Professional Nurses. Task Force on Nursing Practice in Hospitals. American Academy of Nursing. ANA Publ. 1983, i–xiv, 1–135. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| # | Age | Gender | Setting | Education | Position |
|---|---|---|---|---|---|
| 1 | 49 | Female | IHC | Nurse with palliative care training | Nurse |
| 2 | 49 | Female | PCU | Nurse with palliative care training | Head nurse |
| 3 | 27 | Female | PCU | Nurse with palliative care training | Nurse |
| 4 | 54 | Female | PCU | Paediatric nurse with palliative care training | Nurse |
| 5 | 54 | Female | PCU | Paediatric nurse with palliative care training | Nurse |
| 6 | 27 | Female | IHC | Nurse with palliative care training | Nurse |
| 7 | 46 | Female | IHC | Nurse with palliative care training | Nurse |
| 8 | 55 | Female | IHC | Nurse with palliative care training | Nurse |
| 9 | 37 | Female | SOPC | Geriatric nurse with palliative care training | Head nurse |
| 10 | 41 | Female | SOPC | Paediatric nurse with palliative care training | Head nurse |
| 11 | 60 | Female | SOPC | Nurse with palliative care training | Nurse |
| 12 | 58 | Female | SOPC | Nurse with palliative care training | Head nurse |
| 13 | 60 | Female | SOPC | Nurse with palliative care training | Nurse |
| 14 | 51 | Female | SOPC | Geriatric nurse with palliative care training | Head nurse |
| 15 | 60 | Female | PCU | Nurse with palliative care training | Nurse |
| 16 | 42 | Female | IHC | Geriatric nurse | Nurse |
| PCU | IHC | SOPC | |
|---|---|---|---|
| Staff shortages | Participants reported strain due to the lack of staff, as staff frequently changed between wards of the hospital. | Furthermore, staff shortages were common due to a lack of qualified staff and, often, the recruitment or temporary cover of other insufficiently qualified personnel. | Not mentioned. |
| “We always have a very large rotation among the wards. Then you just take someone off from one ward to the other. And because of that you almost never have full staff. And that is stressful” (5_PCU, Pos. 34) | “Half of them are geriatric nurses because of a lack of staff. And you notice that they are actually very close to their limits.” (7_ IHC, Pos. 16) | Not mentioned. | |
| Documentation effort | Documentation is perceived as burdensome because it is seen as hindering the ability of nurses to focus on the delivery of quality care. | Whilst recognition of the importance of documentation was acknowledged, it was seen as a time-consuming and unwelcome deviation of nurses away from the delivery of patient care. | Not mentioned. |
| “A big burden is documentation. It is the be-all and end-all. So if you don’t document, you haven’t done it. Of course, that takes up most of our time, that’s quite clear.” (2_PCU, Pos. 32) | “We try to reduce it [the documentation], but despite it all, of course, documentation has to be done. And in such times, things that we would otherwise like to do with the guests are neglected. Even going for a walk, organising other things or something like that, that can’t happen because you don’t have the energy.” (8_ IHC, Pos. 42) | Not mentioned. | |
| Organisation of work | Nurses reported stress because they have too few days off in a row. | Nurses reported stress due to shift patterns, being unable to have an adequate amount of time when working in a three-shift system. | In the context of outpatient care, nurses reported that they felt pressured to be constantly available and responsive to patients. |
| “These many shifts. We sometimes have ten shifts, all in a row. One day off, that’s just exhausting. You don’t feel like it anymore, that’s how I feel at the moment. I just don’t want to do anything anymore at the moment, I don’t know myself like that at all.” (4_ PCU, Pos. 28) | “I’ve noticed that there’s little time left in the full-time, three-shift system to do things that give me enough balance. Meeting friends, digging in the garden, whatever, reading. So there was too little time. And I know from my previous hospice years that if you have three days off at a stretch or something, you switch off in a completely different way and come back with much more energy.” (8_ IHC, Pos. 62) | “In SOPC, it is often like: I have to drop everything and leave now. This is sometimes, yes, exhausting.” (9_ SOPC, Pos. 12) | |
| Lack of time in daily routines | Due to lack of time, care cannot be provided adequately. | Not mentioned. | Lack of time for intensive care (physical as well as psychosocial) |
| “If I don’t have time, I can’t engage very intensively with the patient, which of course also makes me dissatisfied. Lack of time is already a big factor that weighs on you.” (2_PCU, Pos. 26) | Not mentioned. | “You do want to take your time: With some, you’re half an hour, with others you’re an hour and a half, or two. You never know. That’s why it’s always difficult and exhausting and you also have to work more sometimes.” (10_SOPC, Pos. 4) | |
| Nursing activities | Not mentioned. | Not mentioned. | Caring for patients without the support of nursing assistants is perceived as stressful. |
| Not mentioned. | Not mentioned. | “All the nurses who are on duty in the morning and do long hours of washing, or beds, or really do personal hygiene. They don’t have any support. You are alone. That gets to you.” (11_ SOPC, Pos. 12) |
| Anchor Quote | PCU * | IHC * | SOPC * | |
|---|---|---|---|---|
| Higher remuneration | “I simply wish for more recognition. If you will, also financially, so that recognition comes in the form of better pay, because we bear an incredible amount of responsibility at the end of our lives. It doesn’t matter whether I’m dealing with a judge or a lowly cleaner. They are all treated equally well, whether they are private patients or not. I would also like to be treated well, or to be recognised for what we do, for the competence it takes to do a good job.” (7_ IHC, Pos. 68) | x | x | x |
| Recognition of palliative care by society | “I would like to see a much higher recognition of our really versatile services that we strive to provide on a daily basis. Recognition in the financial area, but also in the social appreciation.” (11_SOPC, Pos. 28) | x | x | - |
| Recognition of palliative care by politicians | “You really have to go into politics. We should really go to the parliament and say: “ Please come here, I’ll show you how we provide care for a palliative patient, what it takes in terms of time. What it means to work in palliative care.” (14_SOPC, Pos. 72) | x | x | x |
| Recognition of palliative care by the employer | “Yes, money is one thing, I would say. But the employer could also reward our work differently, just value it more.” (4_PCU, Pos. 58) | x | - | - |
| Statutory regulations for adjusting working time | “Legal regulations on working time. Of course, of course. Yes, it would be nice if there were something like that. Or that they also said every second weekend off.” (2_PCU, Pos. 126) | x | - | - |
| Reducing working time | “And I have a desire to reduce working hours.” (7_IHC, Pos. 50) | - | x | - |
| More days off at a stretch | “That the legislator also really stipulates that after five days, there must be two days off.” (2_PCU, Pos. 120) | x | x | - |
| Reduction of documentation effort | “You could happily reduce the documentation by half.” (5_PCU, Pos. 54) | x | - | - |
| Increase in personnel | “We need staff (laughs). That is really the be-all and end-all, that you get more staff here. That you can eliminate all these burdensome things. That I can really say I can sit down and talk to the patient and don’t have to say I’ll come back in two minutes.” (2_PCU, Pos. 66) | x | x | x |
| Promoting the exchange between professional groups | “Well, an exchange with other professional groups would be great! That would really help at times.” (14_SOPC, Pos. 160) | - | - | x |
| Stress management programs preventing burnout | “And when I hear what palliative work was back then. Mrs. M., for example, has been there for fifteen or twenty years. When she talks like that, you can’t compare it with today’s situation. And that is actually a bit sad. I’ve already noticed that extremely in the four years that I’ve been there. This change in terms of palliative work. Well, in any case, burnout prophylaxis would be very important for me.” (3_PCU, Pos. 110) | x | - | - |
| Further training provided by the employer | “Advanced courses for palliative care nurses, or learning relaxation techniques. That would be something. There are great offers, but they are all expensive. And my employer boasts about its palliative care unit, which is on the website, brochures, everywhere we are always lifted to the skies, but when it comes to further training, nothing happens.” (4_PCU, Pos. 148) | x | - | - |
| SOPC *, n (%) | PCU *, n (%) | IHC *, n (%) | Total, n (%) | |
|---|---|---|---|---|
| Age (years) | ||||
| >20 | 0 (0) | 0 (0) | 1 (4) | 1 (1) |
| 21–30 | 0 (0) | 1 (3) | 3 (11) | 4 (4) |
| 31–40 | 8 (18) | 7 (23) | 6 (22) | 21 (21) |
| 41–50 | 20 (45) | 6 (20) | 6 (22) | 32 (32) |
| 51–60 | 16 (36) | 11 (37) | 9 (33) | 36 (26) |
| 61–70 | 0 (0) | 5 (17) | 2 (7) | 7 (7) |
| Sex | ||||
| Total | 44 (100) | 30 (100) | 27 (100) | 101 (100) |
| Female | 40 (91) | 25 (83) | 22 (81) | 87 (86) |
| Male | 4 (9) | 5 (17) | 5 (19) | 14 (14) |
| Professional experience (years) | ||||
| >10 | 3 (7) | 4 (9) | 9 (20) | 16 (16) |
| 11–20 | 16 (36) | 6 (14) | 6 (14) | 28 (28) |
| 21–30 | 16 (36) | 5 (11) | 4 (9) | 25 (25) |
| 31–40 | 8 (18) | 12 (27) | 6 (14) | 26 (26) |
| <41 | 1 (2) | 3 (7) | 2 (5) | 6 (6) |
| Mean | 23.5 | 26.7 | 20.6 | 23.7 |
| Median | 22.5 | 30.5 | 20 | 24 |
| Palliative care training | ||||
| Yes | 36 (82) | 21 (70) | 12 (44) | 69 (68) |
| No | 8 (18) | 9 (30) | 15 (56) | 32 (32) |
| Location | ||||
| City | 7 (16) | 20 (67) | 13 (48) | 40 (40) |
| Town | 16 (36) | 8 (27) | 3 (11) | 27 (27) |
| Provincial town | 14 (32) | 1 (3) | 2 (7) | 17 (17) |
| Rural area | 7 (16) | 1 (3) | 9 (33) | 17 (17) |
| Current Causes of Stress ** | Total (n = 101) | SOPC * (n = 44) | PCU * (n = 30) | IHC * (n = 27) | |
|---|---|---|---|---|---|
| Median | Median | Median | Median | ||
| Patient-related burdens | Close relationship with the patients | 4 | 4 | 4 | 4 |
| Omnipresence of death and dying | 4 | 4 | 4 | 4 | |
| Symptom burden of the patients | 3 | 3 | 3 | 3 | |
| Burdens related to relatives | Need for consulting and information of the relatives | 3 | 3 | 4 | 4 |
| Pressure of expectations on the part of relatives | 3 | 3 | 3 | 3 | |
| Burdens due to working conditions | Documentation effort | 2 | 2 | 2 | 3 |
| Changing personnel | 4 | 4 | 4 | 4 | |
| Understaffing | 2 | 2 | 2 | 3 | |
| Shift work | 4 | 3 | 4 | 4 | |
| Few days off at a time | 3 | 3 | 3.5 | 4 | |
| Physical Stress due to nursing activities | 3 | 3.5 | 3 | 3 | |
| Recurring overtime | 3 | 2 | 3 | 4 | |
| Administrative effort | 2 | 2 | 2.5 | 3 | |
| Permanent availability | 3 | 2 | 3.5 | 4 | |
| Remuneration of the work | 3 | 2 | 2.5 | 4 |
| Current Causes of Stress | JT | p-Value |
|---|---|---|
| Close relationship with the patients | 2004 | 0.014 |
| Omnipresence of death and dying | 1699 | 0.392 |
| Symptom burden of the patients | 1758 | 0.266 |
| Need for consulting and information of the relatives | 1926.5 | 0.045 |
| Pressure of expectations on the part of relatives | 1754 | 0.267 |
| Documentation effort | 2006 | 0.015 |
| Changing personnel | 1622.5 | 0.570 |
| Understaffing | 2022 | 0.011 |
| Shift work | 1918.5 | 0.049 |
| Few days off at a time | 1902 | 0.061 |
| Physical stress due to nursing activities | 1598 | 0.646 |
| Recurring overtime | 2267.5 | 0.001 |
| Administrative effort | 2012 | 0.016 |
| Permanent availability | 2264 | 0.001 |
| Remuneration of the work | 2001.5 | 0.017 |
| Reducing the Burden Through… | Total n, (%) | SOPC n, (%) | PCU n, (%) | IHC n, (%) |
|---|---|---|---|---|
| Higher remuneration | 60 (59) | 29 (66) | 17 (57) | 14 (52) |
| Recognition of palliative care by society | 29 (29) | 22 (50) | 4 (13) | 3 (11) |
| Recognition of palliative care by policy actors | 45 (45) | 28 (64) | 10 (33) | 7 (26) |
| Recognition of palliative care by the employer | 26 (26) | 7 (16) | 13 (43) | 6 (22) |
| Statutory regulations for adjusting working time | 17 (17) | 4 (9) | 5 (17) | 8 (30) |
| Reducing working time | 21 (21) | 7 (16) | 3 (10) | 11 (41) |
| More days off at a stretch | 34 (34) | 13 (30) | 9 (30) | 12 (44) |
| Reduction of documentation effort | 62 (61) | 30 (68) | 18 (60) | 14 (52) |
| Increase in personnel | 55 (54) | 22 (50) | 19 (63) | 14 (52) |
| Promoting the exchange between professional groups | 19 (19) | 5 (11) | 6 (20) | 8 (30) |
| Inter-professional collaboration | 27 (27) | 16 (36) | 6 (20) | 5 (19) |
| Stress management programs preventing burnout | 24 (24) | 10 (23) | 6 (20) | 8 (30) |
| Further training provided by the employer | 23 (23) | 10 (23) | 5 (17) | 8 (30) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
May, S.; Gabb, F.; Ignatyev, Y.; Ehrlich-Repp, J.; Stahlhut, K.; Heinze, M.; Allsop, M.; Stanze, H.; Muehlensiepen, F. Mental and Physical Well-Being and Burden in Palliative Care Nursing: A Cross-Setting Mixed-Methods Study. Int. J. Environ. Res. Public Health 2022, 19, 6240. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106240
May S, Gabb F, Ignatyev Y, Ehrlich-Repp J, Stahlhut K, Heinze M, Allsop M, Stanze H, Muehlensiepen F. Mental and Physical Well-Being and Burden in Palliative Care Nursing: A Cross-Setting Mixed-Methods Study. International Journal of Environmental Research and Public Health. 2022; 19(10):6240. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106240
Chicago/Turabian StyleMay, Susann, Franziska Gabb, Yuriy Ignatyev, Jana Ehrlich-Repp, Kerstin Stahlhut, Martin Heinze, Matthew Allsop, Henrikje Stanze, and Felix Muehlensiepen. 2022. "Mental and Physical Well-Being and Burden in Palliative Care Nursing: A Cross-Setting Mixed-Methods Study" International Journal of Environmental Research and Public Health 19, no. 10: 6240. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106240