
Frailty as a Predictor of Poor Rehabilitation Outcomes among Older Patients Attending a Geriatric Day Hospital Program: An Observational Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Clinical Outcomes
2.3. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Grund, S.; Gordon, A.L.; van Balen, R.; Bachmann, S.; Cherubini, A.; Landi, F.; Stuck, A.E.; Becker, C.; Achterberg, W.P.; Bauer, J.M.; et al. European consensus on core principles and future priorities for geriatric rehabilitation: Consensus statement. Eur. Geriatr. Med. 2020, 11, 233–238. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.J.; Son, Y.J. Prevalence and associated factors of frailty and mortality in patients with end-stage Renal disease undergoing hemodialysis: A systematic review and meta-analysis. Int. J. Environ. Res. Public Health 2021, 18, 3471. [Google Scholar] [CrossRef] [PubMed]
- He, Y.Y.; Chang, J.; Wang, X.J. Frailty as a predictor of all-cause mortality in elderly patients undergoing percutaneous coronary intervention: A systematic review and meta-analysis. Arch. Gerontol. Geriatr. 2022, 98, 104544. [Google Scholar] [CrossRef] [PubMed]
- Viljanen, A.; Salminen, M.; Irjala, K.; Korhonen, P.; Wuorela, M.; Isoaho, R.; Kivela, S.L.; Vahlberg, T.; Viitanen, M.; Lopponen, M.; et al. Frailty, walking ability and self-rated health in predicting institutionalization: An 18-year follow-up study among Finnish community-dwelling older people. Aging Clin. Exp. Res. 2021, 33, 547–554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luk, J.K.; Chan, C.F. Rehabilitation outcomes of older patients at 6 months follow-up after discharged from a geriatric day hospital (GDH). Arch. Gerontol. Geriatr. 2011, 52, 327–330. [Google Scholar] [CrossRef] [PubMed]
- Pereira, S.R.; Chiu, W.; Turner, A.; Chevalier, S.; Joseph, L.; Huang, A.R.; Morais, J.A. How can we improve targeting of frail elderly patients to a geriatric day-hospital rehabilitation program? BMC Geriatr. 2010, 10, 82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stille, K.; Temmel, N.; Hepp, J.; Herget-Rosenthal, S. Validation of the clinical frailty scale for retrospective use in acute care. Eur. Geriatr. Med. 2020, 11, 1009–1015. [Google Scholar] [CrossRef] [PubMed]
- Rockwood, K.; Song, X.; MacKnight, C.; Bergman, H.; Hogan, D.B.; McDowell, I.; Mitnitski, A. A global clinical measure of fitness and frailty in elderly people. Can. Med. Assoc. J. 2005, 173, 489–495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stuck, A.K.; Mangold, J.M.; Wittwer, R.; Limacher, A.; Bischoff-Ferrari, H.A. Ability of 3 frailty measures to predict short-term outcomes in older patients admitted for post-acute inpatient rehabilitation. J. Am. Med. Dir. Assoc. 2021, 23, 840–844. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.M.; Aliberti, M.J.R.; Fortes-Filho, S.Q.; Melo, J.A.; Aprahamian, I.; Suemoto, C.K.; Jacob Filho, W. Comparison of 3 frailty instruments in a geriatric acute care setting in a low-middle income country. J. Am. Med. Dir. Assoc. 2018, 19, 310–314.e313. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.M.; Jiao, J.; Cao, J.; Huo, X.P.; Zhu, C.; Wu, X.J.; Xie, X.H. Frailty as a predictor of mortality among patients with COVID-19: A systematic review and meta-analysis. BMC Geriatr. 2021, 21, 186. [Google Scholar] [CrossRef] [PubMed]
- Cunha, A.I.L.; Veronese, N.; de Melo Borges, S.; Ricci, N.A. Frailty as a predictor of adverse outcomes in hospitalized older adults: A systematic review and meta-analysis. Ageing Res. Rev. 2019, 56, 100960. [Google Scholar] [CrossRef] [PubMed]
- Lan, X.; Li, H.; Wang, Z.; Chen, Y. Frailty as a predictor of future falls in hospitalized patients: A systematic review and meta-analysis. Geriatr. Nurs. 2020, 41, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Oviedo-Briones, M.; Rodríguez-Laso, Á.; Carnicero, J.A.; Gryglewska, B.; Sinclair, A.J.; Landi, F.; Vellas, B.; Rodríguez Artalejo, F.; Checa-López, M.; Rodriguez-Mañas, L. The ability of eight frailty instruments to identify adverse outcomes across different settings: The FRAILTOOLS project. J. Cachexia Sarcopenia Muscle 2022. Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Ono, T.; Tamai, A.; Takeuchi, D.; Tamai, Y. Factors related to day-care clinic outcomes for dementia patients: Differences between hospitalization in the dementia ward and institutionalization. Psychogeriatrics 2014, 14, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Oviedo-Briones, M.; Laso, A.R.; Carnicero, J.A.; Cesari, M.; Grodzicki, T.; Gryglewska, B.; Sinclair, A.; Landi, F.; Vellas, B.; Checa-Lopez, M.; et al. A comparison of frailty assessment instruments in different clinical and social care settings: The frailtools project. J. Am. Med. Dir. Assoc. 2021, 22, 607.e607–607.e612. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| General Characteristics | |
| Age, mean (sd) | 80.3 (7.0) |
| Age ≥ 75 years, n (%) | 391 (78.4) |
| Female, n (%) | 291 (58.3) |
| Living temporarily in assisted living facility upon admission, n (%) | 76 (15.2) |
| Primary indication for admission, n (%) - Neurological (e.g., stroke) - Chronic gait and balance disorder - Amputation/prosthesis - Orthopedic reason (surgery and/or acute fracture) | 116 (23.3) 273 (54.7) 12 (2.4) 98 (19.6) |
| Program duration, (days) mean (sd) | 85.7 (29.8) |
| Time to day hospital from current living setting, (minutes) mean (sd) | 11.5 (6.9) |
| Comorbidities | |
| Cardiovascular disease, n (%) | 346 (69.3) |
| Stroke or TIA, n (%) | 119 (23.8) |
| Diabetes, n (%) | 100 (20.0) |
| Gait and balance disorder, n (%) | 479 (96.0) |
| Falls, n (%) | 197 (39.5) |
| Depression, n (%) | 108 (21.6) |
| Malnutrition, n (%) | 34 (6.8) |
| Mild cognitive impairment, n (%) | 254 (50.9) |
| Dementia, n (%) | 37 (7.4) |
| Vision impairment, n (%) | 257 (51.5) |
| Hearing impairment, n (%) | 171 (34.3) |
| Functional status and setting | |
| Dependent on ADL (grooming), n (%) (a) | 235 (47.1) |
| Dependent on ADL (dressing), n (%) (b) | 174 (34.9) |
| Home alone, n (%) | 197 (39.5) |
| Stairs at home, n (%) (c) | 316 (63.3) |
| Walking aid, outdoor, n (%) (d) | 384 (77.0) |
| Walking aid, indoor, n (%) (b) | 282 (56.5) |
| Frailty | |
| Clinical Frailty Scale, median (IQR) | 5 (5–6) |
| Frailty status on CFS, n (%) - non-frail (CFS score = 4) - mild/moderate frailty (CFS score = 5–6) - severe frailty (CFS score = 7–9) | 431 (86.4) 68 (13.6) 351 (70.3) 80 (16.0) |
| Clinical outcomes | |
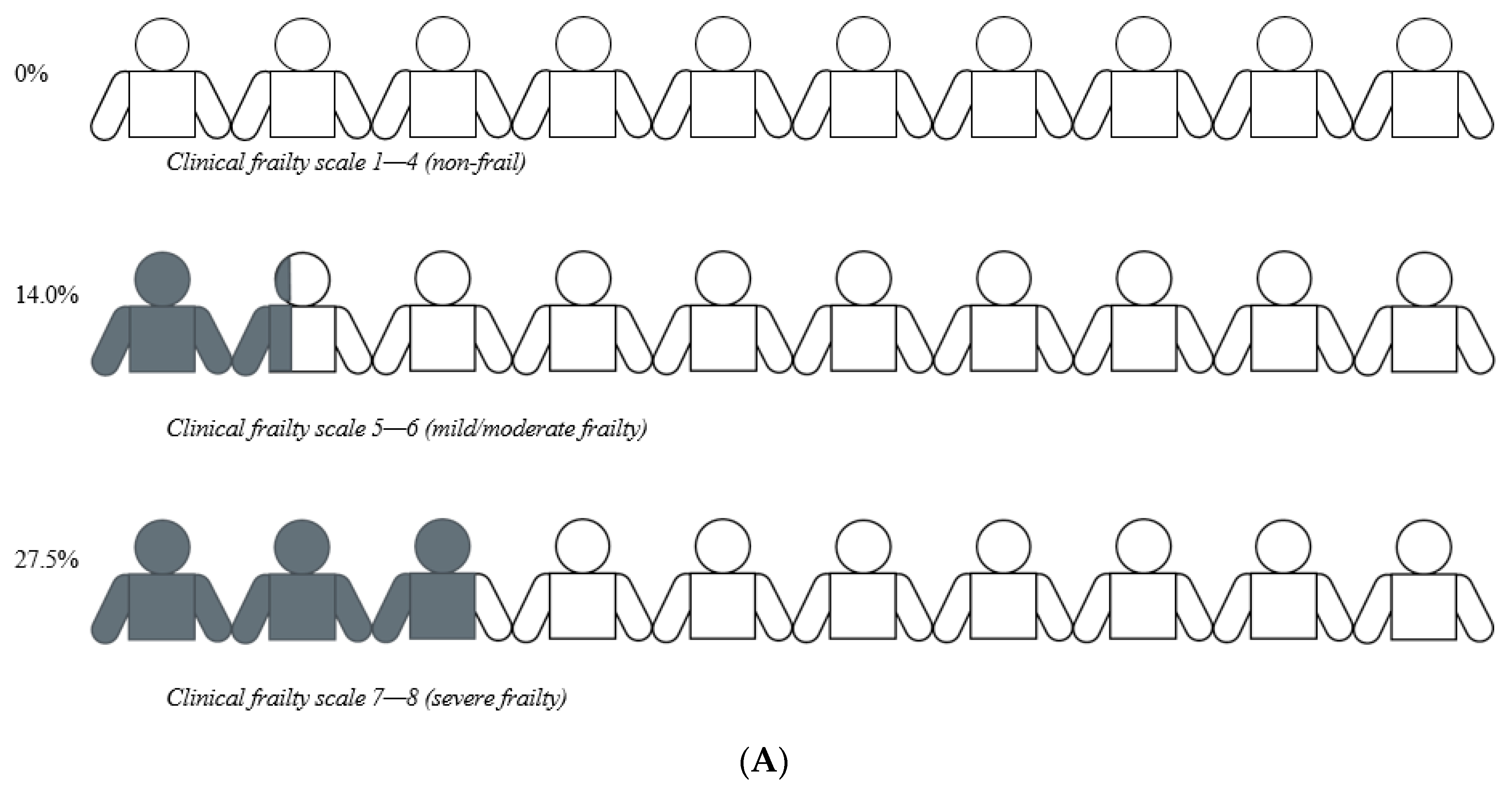
| Poor outcome, n (%) | 77 (15.4) |
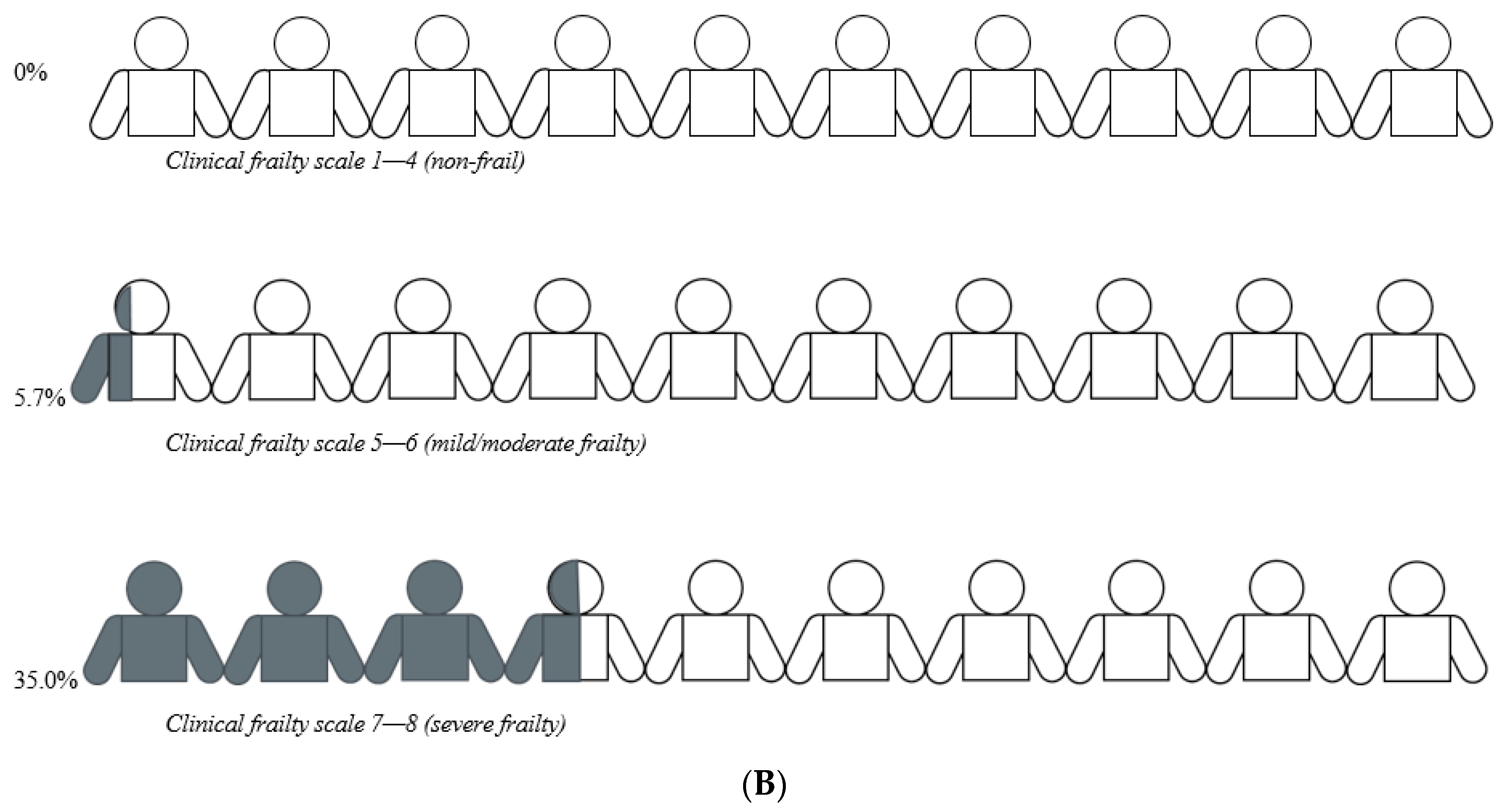
| Admission to permanent nursing home, n (%) | 48 (9.6) |
| (A) Clinical Characteristics by Poor Outcome (n = 499) | ||||||
| Regular Completion of GDH (n = 422) | Poor Outcome (n = 77) | Unadjusted Odds Ratio (95% CI) | p-Value | Adjusted Odds Ratio (95% CI) (a) | p-Value | |
| Age, mean (sd) (a) | 81.0 (6.8) | 80.1 (7.1) | 1.0 (0.98, 1.1) | 0.35 | 1.0 (0.98, 1.0) | 0.46 |
| Male gender, n (%) (a) | 170 (40.3) | 38 (49.4) | 1.4 (0.90, 2.4) | 0.14 | 1.4 (0.86, 2.3) | 0.18 |
| Cognitive impairment, n (%) (a) | 239 (56.6) | 50 (64.9) | 1.4 (0.85, 2.4) | 0.18 | 1.2 (0.72, 2.0) | 0.50 |
| Living temporarily in assisted nursing facility, n (%) (a) | 64 (15.2) | 12 (15.6) | 1.0 (0.52, 2.0) | 0.93 | 0.64 (0.30, 1.4) | 0.25 |
| Clinical frailty scale, median (IQR) (a) | 5 (5–6) | 6 (5-7) | 2.1 (1.3, 3.3) | <0.01 | 2.0 (1.3, 3.2) | <0.01 |
| (B) Clinical Characteristics by Admission to Permanent Nursing Home Care (n = 499) | ||||||
| Continued Community Living (n = 451) | Admission to Permanent Nursing Home Care (n = 48) | Unadjusted Odds Ratio (95% CI) | p-Value | Adjusted Odds Ratio (95% CI) (a) | p-Value | |
| Age, mean (sd) (a) | 80.5 (6.8) | 78.3 (8.9) | 0.96 (0.92, 1.0) | 0.04 | 0.97 (0.92, 1.0) | 0.18 |
| Male gender, n (%) (a) | 192 (42.6) | 16 (33.3) | 0.67 (0.36, 1.3) | 0.22 | 0.60 (0.26, 1.4) | 0.23 |
| Cognitive impairment, n (%) (a) | 256 (56.8) | 33 (68.8) | 1.7 (0.89, 3.2) | 0.11 | 1.9 (0.82, 4.6) | 0.13 |
| Living temporarily in assisted nursing facility, n (%) (a) | 36 (8.0) | 40 (83.3) | 57.6 (25.1, 132) | <0.01 | 34 (13.9, 83.3) | <0.01 |
| Clinical frailty scale, median (IQR) (a) | 5 (5-6) | 7 (6–7) | 9.5 (5.1, 17.7) | <0.01 | 2.9 (1.3, 6.3) | <0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andres, D.; Imhoof, C.; Bürge, M.; Jakob, G.; Limacher, A.; Stuck, A.K. Frailty as a Predictor of Poor Rehabilitation Outcomes among Older Patients Attending a Geriatric Day Hospital Program: An Observational Study. Int. J. Environ. Res. Public Health 2022, 19, 6276. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106276
Andres D, Imhoof C, Bürge M, Jakob G, Limacher A, Stuck AK. Frailty as a Predictor of Poor Rehabilitation Outcomes among Older Patients Attending a Geriatric Day Hospital Program: An Observational Study. International Journal of Environmental Research and Public Health. 2022; 19(10):6276. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106276
Chicago/Turabian StyleAndres, Daniel, Caroline Imhoof, Markus Bürge, Gabi Jakob, Andreas Limacher, and Anna K. Stuck. 2022. "Frailty as a Predictor of Poor Rehabilitation Outcomes among Older Patients Attending a Geriatric Day Hospital Program: An Observational Study" International Journal of Environmental Research and Public Health 19, no. 10: 6276. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106276