
Monitoring Eye Movements Depending on the Type of Visual Stimulus in Patients with Impaired Consciousness Due to Brain Damage

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
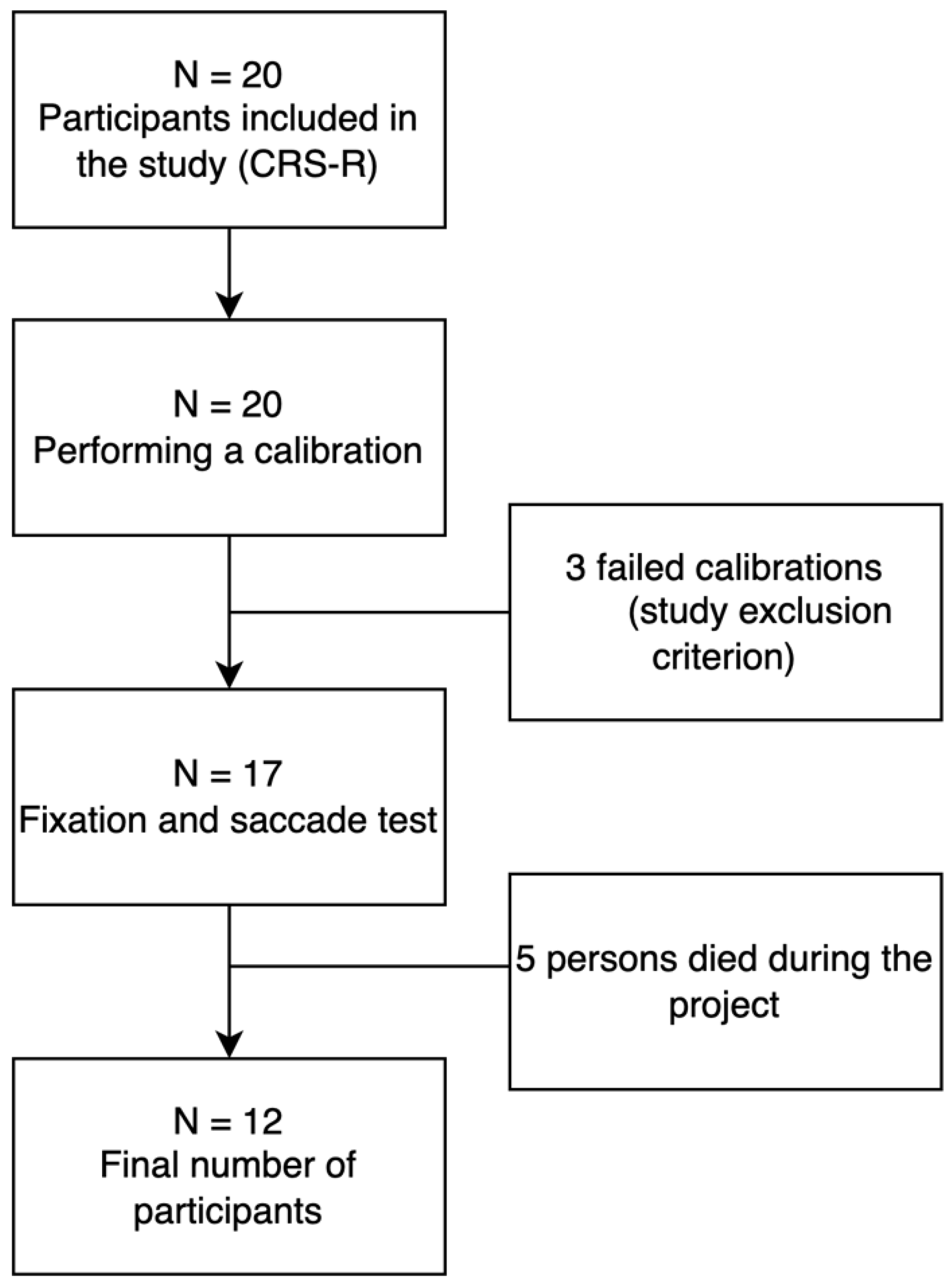
2.1. Group Characteristics
2.2. Research Tool
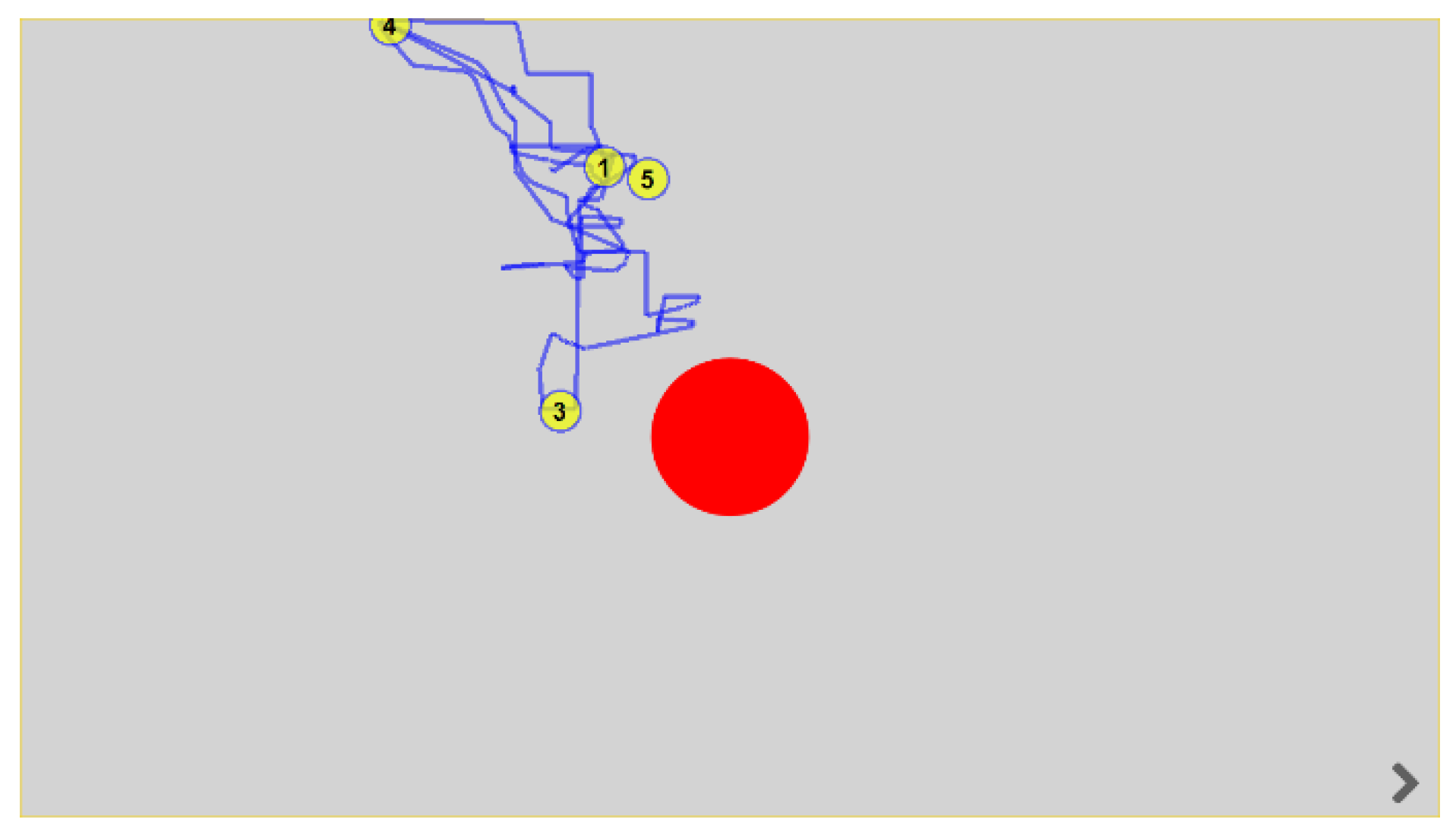
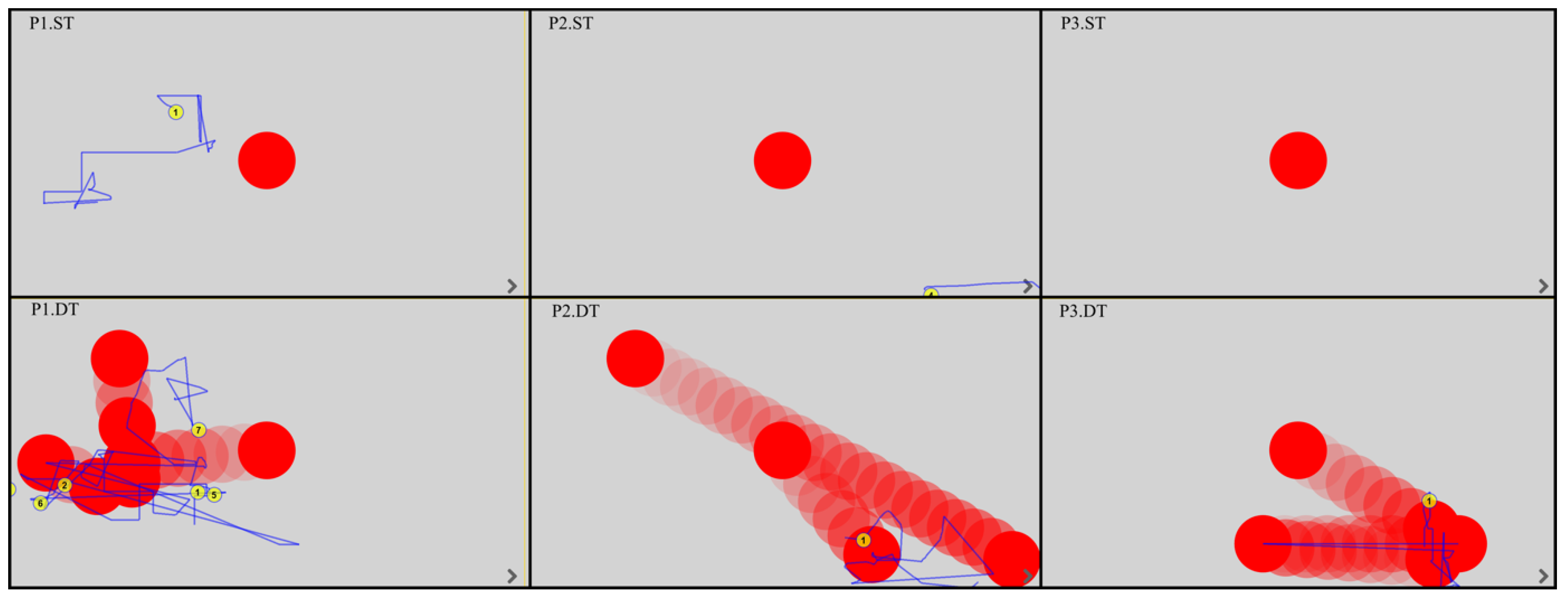
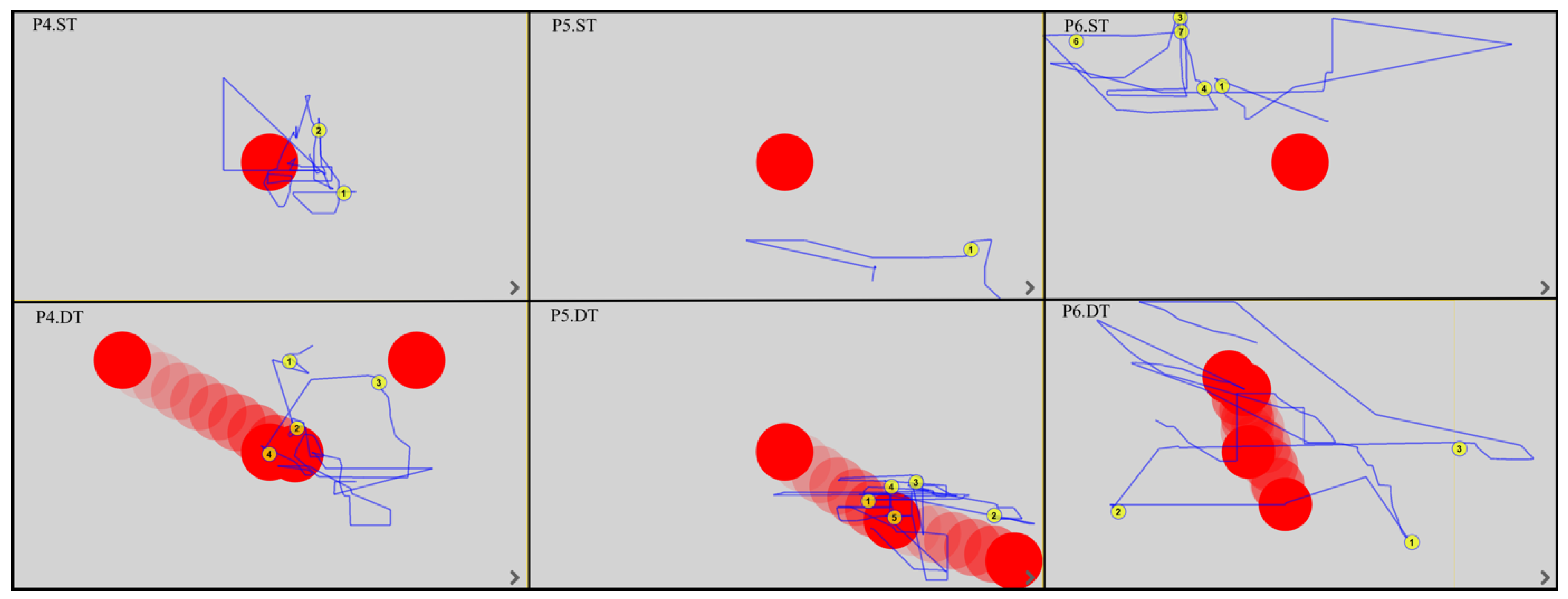
2.3. Fixation and Saccade Test
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
6. Limitation
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Martinez-Conde, S.; Macknik, S.L.; Hubel, D.H. The Role of Fixational Eye Movements in Visual Perception. Nat. Rev. Neurosci. 2004, 5, 229–240. [Google Scholar] [CrossRef]
- Duchowski, A.T. Taxonomy and Models of Eye Movements. In Eye Tracking Methodology: Theory and Practice; Duchowski, A.T., Ed.; Springer International Publishing: Cham, Switzeland, 2017; pp. 39–46. ISBN 978-3-319-57883-5. [Google Scholar]
- Jadanowski, K.; Budrewicz, S.; Koziorowska-Gawron, E. Zaburzenia Gałkoruchowe w Chorobach Ośrodkowego Układu Nerwowego. Pol. Przegląd Neurol. 2010, 6, 202–211. [Google Scholar]
- Nolte, J. The Human Brain. An Introduction to Its Functional Anatomy; Mosby Elsevier: Philadelphia, PA, USA, 2012; Volume 2. [Google Scholar]
- Bringmann, A.; Syrbe, S.; Görner, K.; Kacza, J.; Francke, M.; Wiedemann, P.; Reichenbach, A. The Primate Fovea: Structure, Function and Development. Prog. Retin. Eye Res. 2018, 66, 49–84. [Google Scholar] [CrossRef] [PubMed]
- Shaikh, A.G.; Ghasia, F.F. Physiology and Pathology of Saccades and Gaze Holding. NeuroRehabilitation 2013, 32, 493–505. [Google Scholar] [CrossRef] [PubMed]
- Nooij, S.A.E.; Pretto, P.; Bülthoff, H.H. More Vection Means More Velocity Storage Activity: A Factor in Visually Induced Motion Sickness? Exp. Brain Res. 2018, 236, 3031–3041. [Google Scholar] [CrossRef] [Green Version]
- Gremmler, S.; Lappe, M. Saccadic Adaptation Is Associated with Starting Eye Position. Front. Hum. Neurosci. 2016, 10, 322. [Google Scholar] [CrossRef] [Green Version]
- Morgante, J.D.; Zolfaghari, R.; Johnson, S.P. A Critical Test of Temporal and Spatial Accuracy of the Tobii T60XL Eye Tracker. Infancy 2012, 17, 9–32. [Google Scholar] [CrossRef]
- Shanidze, N.M.; Velisar, A. Eye, Head, and Gaze Contributions to Smooth Pursuit in Macular Degeneration. J. Neurophysiol. 2020, 124, 134–144. [Google Scholar] [CrossRef]
- Waespe, W.; Schwarz, U. Characteristics of Eye Velocity Storage during Periods of Suppression and Reversal of Eye Velocity in Monkeys. Exp. Brain Res. 1986, 65, 49–58. [Google Scholar] [CrossRef]
- Beh, S.C.; Frohman, T.C.; Frohman, E.M. Cerebellar Control of Eye Movements. J. Neuroophthalmol. 2017, 37, 87–98. [Google Scholar] [CrossRef]
- Shemesh, A.A.; Zee, D.S. Eye Movement Disorders and the Cerebellum. J. Clin. Neurophysiol. 2019, 36, 405–414. [Google Scholar] [CrossRef] [PubMed]
- Müller, T.J. Ocular movement and nystagmus: Basics and clinical diagnosis. HNO 2020, 68, 313–323. [Google Scholar] [CrossRef]
- Gorges, M.; Pinkhardt, E.H.; Kassubek, J. Alterations of Eye Movement Control in Neurodegenerative Movement Disorders. J. Ophthalmol. 2014, 2014, 658243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnett, B.P.; Singman, E.L. Vision Concerns after Mild Traumatic Brain Injury. Curr. Treat. Options. Neurol. 2015, 17, 329. [Google Scholar] [CrossRef] [PubMed]
- Kapoor, N.; Ciuffreda, K.J. Vision Disturbances Following Traumatic Brain Injury. Curr. Treat. Options. Neurol. 2002, 4, 271–280. [Google Scholar] [CrossRef] [PubMed]
- Thiagarajan, P.; Ciuffreda, K.J.; Capo-Aponte, J.E.; Ludlam, D.P.; Kapoor, N. Oculomotor Neurorehabilitation for Reading in Mild Traumatic Brain Injury (MTBI): An Integrative Approach. NeuroRehabilitation 2014, 34, 129–146. [Google Scholar] [CrossRef]
- Fox, S.M.; Koons, P.; Dang, S.H. Vision Rehabilitation After Traumatic Brain Injury. Phys. Med. Rehabil. Clin. N. Am. 2019, 30, 171–188. [Google Scholar] [CrossRef]
- Simpson-Jones, M.E.; Hunt, A.W. Vision Rehabilitation Interventions Following Mild Traumatic Brain Injury: A Scoping Review. Disabil. Rehabil. 2019, 41, 2206–2222. [Google Scholar] [CrossRef]
- Lee, T.L.; Yeung, M.K.; Sze, S.L.; Chan, A.S. Computerized Eye-Tracking Training Improves the Saccadic Eye Movements of Children with Attention-Deficit/Hyperactivity Disorder. Brain Sci. 2020, 10, 1016. [Google Scholar] [CrossRef]
- Xiao, J.; Xie, Q.; Lin, Q.; Yu, T.; Yu, R.; Li, Y. Assessment of Visual Pursuit in Patients With Disorders of Consciousness Based on a Brain-Computer Interface. IEEE Trans Neural. Syst. Rehabil. Eng. 2018, 26, 1141–1151. [Google Scholar] [CrossRef]
- Pierrot-Deseilligny, C. Eye movement: From basic semiology to cognitive neuroscience. Bull. Acad. Natl. Med. 2005, 189, 1505–1515. [Google Scholar] [CrossRef]
- Gray, J.A.B.; Malcolm, J.L. The initiation of nerve impulses by mesenteric Pacinian corpuscles. Proc. R. Soc. London Ser. B Biol. Sci. 1950, 137, 96–114. [Google Scholar] [CrossRef]
- Thonnard, M.; Wannez, S.; Keen, S.; Brédart, S.; Bruno, M.-A.; Gosseries, O.; Demertzi, A.; Thibaut, A.; Chatelle, C.; Charland-Verville, V.; et al. Detection of Visual Pursuit in Patients in Minimally Conscious State: A Matter of Stimuli and Visual Plane? Brain Inj. 2014, 28, 1164–1170. [Google Scholar] [CrossRef] [PubMed]
- Vanhaudenhuyse, A.; Schnakers, C.; Brédart, S.; Laureys, S. Assessment of Visual Pursuit in Post-Comatose States: Use a Mirror. J. Neurol. Neurosurg. Psychiatry 2008, 79, 223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Candelieri, A.; Cortese, M.D.; Dolce, G.; Riganello, F.; Sannita, W.G. Visual Pursuit: Within-Day Variability in the Severe Disorder of Consciousness. J. Neurotrauma 2011, 28, 2013–2017. [Google Scholar] [CrossRef] [PubMed]
- Dolce, G.; Lucca, L.F.; Candelieri, A.; Rogano, S.; Pignolo, L.; Sannita, W.G. Visual Pursuit in the Severe Disorder of Consciousness. J. Neurotrauma 2011, 28, 1149–1154. [Google Scholar] [CrossRef] [PubMed]
- Wannez, S.; Vanhaudenhuyse, A.; Laureys, S.; Brédart, S. Mirror Efficiency in the Assessment of Visual Pursuit in Patients in Minimally Conscious State. Brain Inj. 2017, 31, 1429–1435. [Google Scholar] [CrossRef]
- Monti, M.M.; Laureys, S.; Owen, A.M. The Vegetative State. BMJ 2010, 341, c3765. [Google Scholar] [CrossRef] [Green Version]
- Boltzmann, M.; Schmidt, S.B.; Gutenbrunner, C.; Krauss, J.K.; Stangel, M.; Höglinger, G.U.; Wallesch, C.-W.; Rollnik, J.D. The Influence of the CRS-R Score on Functional Outcome in Patients with Severe Brain Injury Receiving Early Rehabilitation. BMC Neurol. 2021, 21, 44. [Google Scholar] [CrossRef]
- Giacino, J.T.; Katz, D.I.; Schiff, N.D.; Whyte, J.; Ashman, E.J.; Ashwal, S.; Barbano, R.; Hammond, F.M.; Laureys, S.; Ling, G.S.F.; et al. Practice Guideline Update Recommendations Summary: Disorders of Consciousness: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology; the American Congress of Rehabilitation Medicine; and the National Institute on Disability, Independent Living, and Rehabilitation Research. Neurology 2018, 91, 450–460. [Google Scholar] [CrossRef] [Green Version]
- Sun, Y.; Wang, J.; Heine, L.; Huang, W.; Wang, J.; Hu, N.; Hu, X.; Fang, X.; Huang, S.; Laureys, S.; et al. Personalized Objects Can Optimize the Diagnosis of EMCS in the Assessment of Functional Object Use in the CRS-R: A Double Blind, Randomized Clinical Trial. BMC Neurol. 2018, 18, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stenberg, J.; Godbolt, A.K.; Möller, M.C. The Value of Incorporating Personally Relevant Stimuli into Consciousness Assessment with the Coma Recovery Scale—Revised: A Pilot Study. J. Rehabil. Med. 2018, 50, 253–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zihl, J.; von Cramon, D.; Mai, N. Selective Disturbance of Movement Vision after Bilateral Brain Damage. Brain 1983, 106 Pt 2, 313–340. [Google Scholar] [CrossRef]
- Zihl, J.; von Cramon, D.; Mai, N.; Schmid, C. Disturbance of Movement Vision after Bilateral Posterior Brain Damage. Further Evidence and Follow up Observations. Brain 1991, 114 Pt 5, 2235–2252. [Google Scholar] [CrossRef]
- Gygli, J.; Romano, F.; Bockisch, C.J.; Feddermann-Demont, N.; Straumann, D.; Bertolini, G. Effect of the Stimulus Duration on the Adaptation of the Optokinetic Afternystagmus. Front. Neurol. 2021, 12, 518133. [Google Scholar] [CrossRef] [PubMed]
- Fuster, J.M. Executive Frontal Functions. Exp. Brain Res. 2000, 133, 66–70. [Google Scholar] [CrossRef]
- Fuster, J.M. Jackson and the Frontal Executive Hierarchy. Int. J. Psychophysiol. 2007, 64, 106–107. [Google Scholar] [CrossRef]
- Pąchalska, M. Rehabilitacja Neuropsychologiczna: Procesy Poznawcze i Emocjonalne; Wydawnictwo Uniwersytetu Marii Curie-Sk\Lodowskiej: Lublin, Poland, 2008. [Google Scholar]
- van Erp, W.S.; Lavrijsen, J.C.M.; van de Laar, F.A.; Vos, P.E.; Laureys, S.; Koopmans, R.T.C.M. The Vegetative State/Unresponsive Wakefulness Syndrome: A Systematic Review of Prevalence Studies. Eur. J. Neurol. 2014, 21, 1361–1368. [Google Scholar] [CrossRef] [Green Version]
- Monti, M.M. Cognition in the Vegetative State. Annu. Rev. Clin. Psychol. 2012, 8, 431–454. [Google Scholar] [CrossRef] [Green Version]
- von Wild, K.; Laureys, S.T.; Gerstenbrand, F.; Dolce, G.; Onose, G. The Vegetative State—A Syndrome in Search of a Name. J Med. Life 2012, 5, 3–15. [Google Scholar]
- Kondziella, D.; Cheung, M.C.; Dutta, A. Public Perception of the Vegetative State/Unresponsive Wakefulness Syndrome: A Crowdsourced Study. PeerJ 2019, 7, e6575. [Google Scholar] [CrossRef]
- Formaggio, E.; Del Felice, A.; Cavinato, M.; Storti, S.F.; Arcaro, C.; Turco, C.; Salvi, L.; Avesani, R.; Piccione, F.; Manganotti, P. EEG to Identify Attempted Movement in Unresponsive Wakefulness Syndrome. Clin. EEG Neurosci. 2020, 51, 339–347. [Google Scholar] [CrossRef]
- Edlow, B.L.; Claassen, J.; Schiff, N.D.; Greer, D.M. Recovery from Disorders of Consciousness: Mechanisms, Prognosis and Emerging Therapies. Nat. Rev. Neurol. 2021, 17, 135–156. [Google Scholar] [CrossRef]
- Annen, J.; Laureys, S.; Gosseries, O. Brain-Computer Interfaces for Consciousness Assessment and Communication in Severely Brain-Injured Patients. Handb. Clin. Neurol. 2020, 168, 137–152. [Google Scholar] [CrossRef]
- Pan, J.; Wu, J.; Liu, J.; Wu, J.; Wang, F. A Systematic Review of Sleep in Patients with Disorders of Consciousness: From Diagnosis to Prognosis. Brain Sci. 2021, 11, 1072. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sex | Female | Male | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Patient | P2 | P3 | P8 | P10 | P11 | P1 | P4 | P5 | P6 | P7 | P9 | P12 | |
| Age | 43 | 42 | 65 | 50 | 27 | 65 | 25 | 31 | 40 | 26 | 67 | 67 | |
| Diagnosis | ISBH | ILSS | HRSS | IRSS | CT | HRSS | CT | CT | CT | CT | BSS | HRSS | |
| CRS-R | total | 6 | 8 | 20 | 4 | 13 | 16 | 16 | 18 | 9 | 22 | 8 | 22 |
| subscales | (2/1/2/ 0/0/1) | (2/1/2/ 1/0/2) | (4/5/5/ 2/1/3) | (1/0/2/ 0/0/1) | (3/5/2/ 1/0/2) | (3/5/4/ 2/1/1) | (4/5/2/ 2/0/3) | (4/5/2/ 2/2/3) | (2/1/2/ 2/0/2) | (4/5/6/ 2/2/3) | (2/1/2/ 1/0/2) | (4/5/6/ 2/2/3) | |
| CConscious state | UWS | UWS | eMCS | UWS | MCS | MCS | MCS | eMCS | UWS | eMCS | UWS | eMCS | |
| Patient | Fixation | |||
|---|---|---|---|---|
| In the Monitor Field | Outside the Monitor | In the Monitor Field | Outside the Monitor | |
| Type of Task | ||||
| ST [N] | DT [N] | |||
| P1 | 1 | 0 | 6 | 1 |
| P2 | 1 | 3 | 1 | 0 |
| P3 | 0 | 0 | 1 | 0 |
| P4 | 2 | 0 | 4 | 0 |
| P5 | 1 | 0 | 5 | 0 |
| P6 | 5 | 2 | 3 | 0 |
| P7 | 2 | 2 | 2 | 0 |
| P8 | 4 | 1 | 4 | 0 |
| P9 | 1 | 1 | 1 | 0 |
| P10 | 3 | 0 | 7 | 0 |
| P11 | 3 | 0 | 6 | 0 |
| P12 | 4 | 2 | 14 | 12 |
| Me (Q1; Q3) | 2 (1; 3.5) | 0.5 (0; 2) | 4 (1.5; 6) | 0 (0; 0) |
| Pair of Variables | Wilcoxon Paired-Rank Order Test The Marked Results Are Significant with p < 0.5000 | |||
|---|---|---|---|---|
| N | T | Z | p | |
| ST-M and ST-OM | 9 | 4.000000 | 2.191691 | 0.028403 |
| DT-M and DT-OM | 12 | 0.00 | 3.059412 | 0.002218 |
| ST-M and DT-M | 8 | 2.500000 | 2.170434 | 0.029975 |
| ST-OM and DT-OM | 7 | 9.000000 | 0.845154 | 0.398025 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kujawa, K.; Żurek, A.; Gorączko, A.; Olejniczak, R.; Zurek, G. Monitoring Eye Movements Depending on the Type of Visual Stimulus in Patients with Impaired Consciousness Due to Brain Damage. Int. J. Environ. Res. Public Health 2022, 19, 6280. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106280
Kujawa K, Żurek A, Gorączko A, Olejniczak R, Zurek G. Monitoring Eye Movements Depending on the Type of Visual Stimulus in Patients with Impaired Consciousness Due to Brain Damage. International Journal of Environmental Research and Public Health. 2022; 19(10):6280. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106280
Chicago/Turabian StyleKujawa, Katarzyna, Alina Żurek, Agata Gorączko, Roman Olejniczak, and Grzegorz Zurek. 2022. "Monitoring Eye Movements Depending on the Type of Visual Stimulus in Patients with Impaired Consciousness Due to Brain Damage" International Journal of Environmental Research and Public Health 19, no. 10: 6280. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106280