
Digital Health Profile of South Korea: A Cross Sectional Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
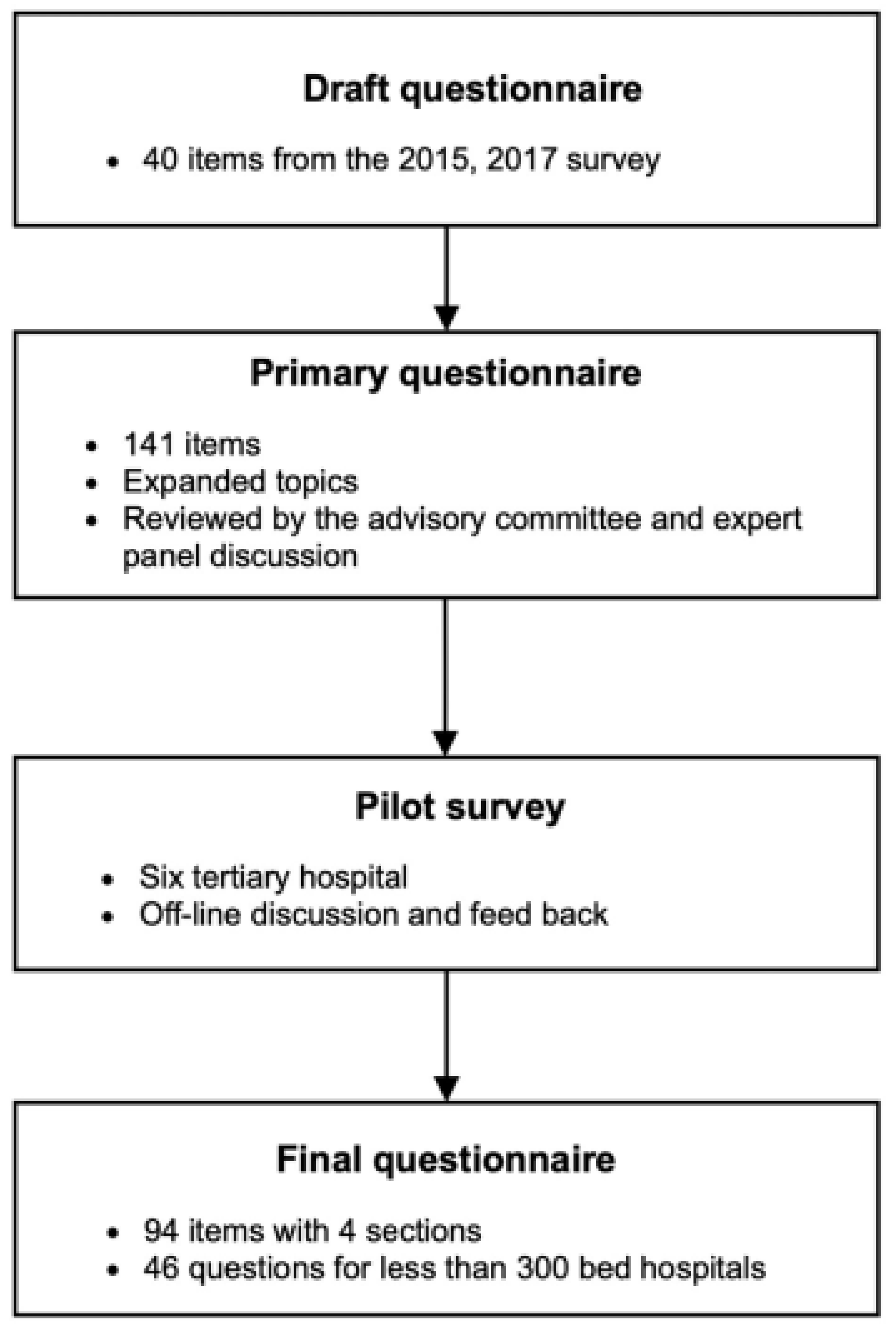
2.1. Study Design
2.2. Survey Target Hospitals and Sampling
2.3. Conducting a Survey
3. Results
3.1. Response Rate
3.2. Main IT Systems for Clinical Practices
3.3. PHR Use and Functionality
3.4. Health Information Exchange
3.5. Systems to Support Data Transfer to the Central Surveillance System
3.6. Advanced IT Systems for Secondary Use
3.7. Future Healthcare IT Infrastructure
4. Discussion
4.1. Summary of the Survey
4.2. The Korean Medical System’s Distinctive Features
4.3. Distinctions from Prior Survey
4.4. 4th Industrial Revolution and Smart Hospital
4.5. Limitation and Future Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization (WHO). Coronavirus Disease (COVID-19): Weekly Epidemiological Update; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Fauci, A.S.; Lane, H.C.; Redfield, R.R. COVID-19—Navigating the uncharted. NEJM 2020, 282, 1268–1269. [Google Scholar] [CrossRef]
- Blumenthal, D.; Fowler, E.J.; Abrams, M.; Collins, S.R. COVID-19—Implications for the health care system. NEJM 2020, 383, 1483–1488. [Google Scholar] [CrossRef] [PubMed]
- Lemos, D.R.Q.; D’angelo, S.M.; Farias, L.A.B.G.; Almeida, M.M.; Gomes, R.G.; Pinto, G.P.; Filho, J.N.C.; Feijão, L.X.; Cardoso, A.R.P.; Lima, T.B.R.; et al. Health system collapse 45 days after the detection of COVID-19 in Ceará, Northeast Brazil: A preliminary analysis. Rev. Soc. Bras. Med. Trop. 2020, 53. [Google Scholar] [CrossRef] [PubMed]
- You, J. Lessons from South Korea’s COVID-19 policy response. Am. Rev. Public Adm. 2020, 50, 801–808. [Google Scholar] [CrossRef]
- Health Metrics Network. Framework and Standards for Country Health Information Systems; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- World Health Organization (WHO). From Innovation to Implementation: EHealth in the WHO European Region; Regional Office for Europe: Copenhagen, Denmark, 2016. [Google Scholar]
- Valverde-Albacete, J.; Folkvord, F.; Lupiáñez-Villanueva, F.; Hocking, L.; Devaux, A.; Altenhofer, M.; Harshfield, A.; Faulí, C. Benchmarking Deployment of eHealth among General Practitioners; Final Report; European Commission, Directorate-General for Communications Networks: Brussels, Belgium, 2018. [Google Scholar]
- Dayton, L. How South Korea made itself a global innovation leader. Nature 2020, 581, S54. [Google Scholar] [CrossRef]
- Dolin, R.H.; Alschuler, L.; Boyer, S.; Beebe, C.; Behlen, F.M.; Biron, P.V.; Shabo, A. HL7 clinical document architecture, release 2. J. Am. Med. Inform. Assoc. 2006, 13, 30–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, Y.J. The South Korean health care system. Jpn. Med. Assoc. J. 2009, 52, 206–209. [Google Scholar]
- Aguirre, R.R.; Suarez, O.; Fuentes, M.; Sanchez-Gonzalez, M.A. Electronic health record implementation: A review of resources and tools. Cureus 2019, 11, e5649. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frost & Sullivan. Future of Smart Hospitals; Frost & Sullivan: New York, NY, USA, 2017. [Google Scholar]
- Kim, K.B.; Han, K.H. A study of the digital healthcare industry in the fourth industrial revolution. J. Converg. Inf. Technol. 2020, 10, 7–15. [Google Scholar]
- Yu, S.-J. 4th industrial revolution and artificial intelligence. Korea Multimed. Soc. 2017, 21, 1–8. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sections | Division | Subjects |
|---|---|---|
| Fundamental eHealth status (Data generation) | eHealth system | IT system investment, eHealth system build and design (general status, construction history, plan, type and coverage), IT system management strategy, priority of investment, interaction of external IT system |
| IT system governance | IT department status and workforce, data review committee, data quality management | |
| Information standard | Utilization of standard codes and terms, information exchange standard, obstacles to standard introduction | |
| Education and workforce | Clinical informatics education | |
| Hospital eHealth quality (Data management) | EMR status | EMR usage status, EMR data storage management, digital signature and certificate |
| EMR certification | EMR certification status, obstacles to EMR certification | |
| Privacy issue | Personal information protection activities, pseudonymization | |
| Information security | Security authentication protocol, security control, security incident response | |
| Advanced healthcare IT system status | Advanced EMR development | EMR function improvement and advancement, CDSS design |
| Information exchange | Engagement of the government-driven information exchange project | |
| PHR | Online patient convenience function, PHR system operation status, hospital data provision range, self-authentication method | |
| Smart hospital | Smart hospital service operation, smart hospital planning, smart hospital establishing policy | |
| eHealth system for secondary use | Data utilization and sharing | Secondary use scope and regulations, patient consent system, medical data open |
| IT system to support data analysis | Medical data analysis information system, CDW establishment status, CDW operation status, CDM establishment status, data sharing standard | |
| Infrastructure for secondary use | Clinical data utilization workforce, company participation research status, AI-based dataset construction, AI system usage status |
| Hospital Classes | Classification Criteria | Number of Hospitals | Number of Surveyed Hospitals (%) |
|---|---|---|---|
| • Over 100 beds | |||
| Tertiary care hospital | • Treatment of more than 20 specialized subjects | 42 | 42 () |
| • Focused treatment for intractable diseases | |||
| • Over 100 beds | |||
| General hospital | • 7 or more specialized subjects | 311 | 280 () |
| Hospital | • Over 30 beds | 1431 | 252 () |
| Adoption and Use of Mobile PHR | TH, (n = 42) | GH, (≥300 beds, n = 119) | GH, (<300 beds, n = 161) | Hospitals, (n = 252) | |
|---|---|---|---|---|---|
| Use status | Active in use | 61.9% | 22.6% | 4.4% | 2.4% |
| Adoption plan within 3 years | 31.3% | 10.8% | 11.8% | 10.8% | |
| Functions | Online appointment | 69.0% | 24.3% | 4.7% | 1.9% |
| Online payment | 59.5% | 23.6% | 1.3% | 0.9% | |
| Medical document assurance | 23.8% | 5.9% | 2.4% | 1.8% | |
| Providing educational material | 38.1% | 10.3% | 1.1% | 0.4% | |
| Medical information inquiry | 64.3% | 22.6% | 2.5% | 0.9% | |
| Medical information download | 11.9% | 0.8% | 0.6% | 0.4% | |
| Service | Applied Status | IoT | Cloud | Big Data | Mobile | AI | 5G | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| T | G | T | G | T | G | T | G | T | G | T | G | ||
| Communication between medical staff and patients | Active in use | 0 | 0 | 0 | 0 | 0 | 0.9 | 22.5 | 4.6 | 0 | 0.9 | 2.5 | 0.9 |
| Plan of action | 2.5 | 3.5 | 2.5 | 0 | 2.5 | 1.7 | 20.0 | 13.3 | 5.0 | 0.9 | 5.0 | 0.9 | |
| Medical service design and resource utilization | Active in use | 22.5 | 1.8 | 0 | 0 | 0 | 0.9 | 5.0 | 0 | 2.5 | 0.9 | 0 | 0 |
| Plan of action | 15.0 | 2.8 | 0 | 0 | 2.5 | 3.6 | 10.0 | 3.6 | 7.5 | 0.9 | 7.5 | 1.8 | |
| Medication error detection | Active in use | 2.6 | 0.9 | 0 | 0 | 12.8 | 1.7 | 0 | 0 | 7.7 | 0.9 | 0 | 0 |
| Plan of action | 0 | 2.6 | 2.5 | 0 | 5.0 | 8.8 | 5.0 | 6.2 | 12.5 | 3.5 | 2.5 | 0 | |
| AI-based decision support model | Active in use | 2.5 | 0.9 | 0 | 0 | 5.0 | 0.9 | 0 | 0 | 17.5 | 0.9 | 0 | 0 |
| Plan of action | 2.5 | 2.6 | 0 | 2.7 | 15.0 | 8.1 | 7.5 | 2.6 | 17.5 | 5.5 | 0 | 0 | |
| AI-based digital therapeutics | Active in use | 0 | 0.9 | 0 | 0 | 4.9 | 0.9 | 7.3 | 0.0 | 17.1 | 2.8 | 0 | 0.9 |
| Plan of action | 2.5 | 1.9 | 2.5 | 0.9 | 10.0 | 6.4 | 5.0 | 4.6 | 22.5 | 6.4 | 5.0 | 0.9 | |
| Early confrontation to infectious crisis | Active in use | 0.0 | 2.8 | 0 | 0 | 5.1 | 0.9 | 12.8 | 2.7 | 0 | 0 | 0 | 0.9 |
| Plan of action | 10.0 | 1.8 | 0 | 0 | 5.0 | 4.4 | 5.0 | 6.3 | 5.0 | 0 | 2.5 | 0.9 | |
| At-risk and emergency patients tracking | Active in use | 12.8 | 1.8 | 0 | 0 | 0 | 1.7 | 2.6 | 2.7 | 2.6 | 0.9 | 0 | 0.9 |
| Plan of action | 12.5 | 3.5 | 0 | 0 | 2.5 | 6.1 | 2.5 | 8.1 | 2.5 | 0.9 | 0 | 0.9 | |
| Hazard alert and monitoring | Active in use | 2.6 | 3.7 | 0 | 0 | 5.1 | 1.7 | 10.3 | 3.6 | 2.6 | 0 | 7.7 | 0.9 |
| Plan of action | 10.0 | 4.4 | 0 | 0.9 | 0 | 0.9 | 7.5 | 11.7 | 10.0 | 2.7 | 7.5 | 0 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, K.; Seo, L.; Yoon, D.; Yang, K.; Yi, J.-E.; Kim, Y.; Lee, J.-H. Digital Health Profile of South Korea: A Cross Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 6329. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106329
Lee K, Seo L, Yoon D, Yang K, Yi J-E, Kim Y, Lee J-H. Digital Health Profile of South Korea: A Cross Sectional Study. International Journal of Environmental Research and Public Health. 2022; 19(10):6329. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106329
Chicago/Turabian StyleLee, Kyehwa, Libga Seo, Dukyong Yoon, Kwangmo Yang, Jae-Eun Yi, Yoomi Kim, and Jae-Ho Lee. 2022. "Digital Health Profile of South Korea: A Cross Sectional Study" International Journal of Environmental Research and Public Health 19, no. 10: 6329. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106329