
Effectiveness of Warm-Up Intervention Programs to Prevent Sports Injuries among Children and Adolescents: A Systematic Review and Meta-Analysis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Definition of Terms
2.2. Search Strategy
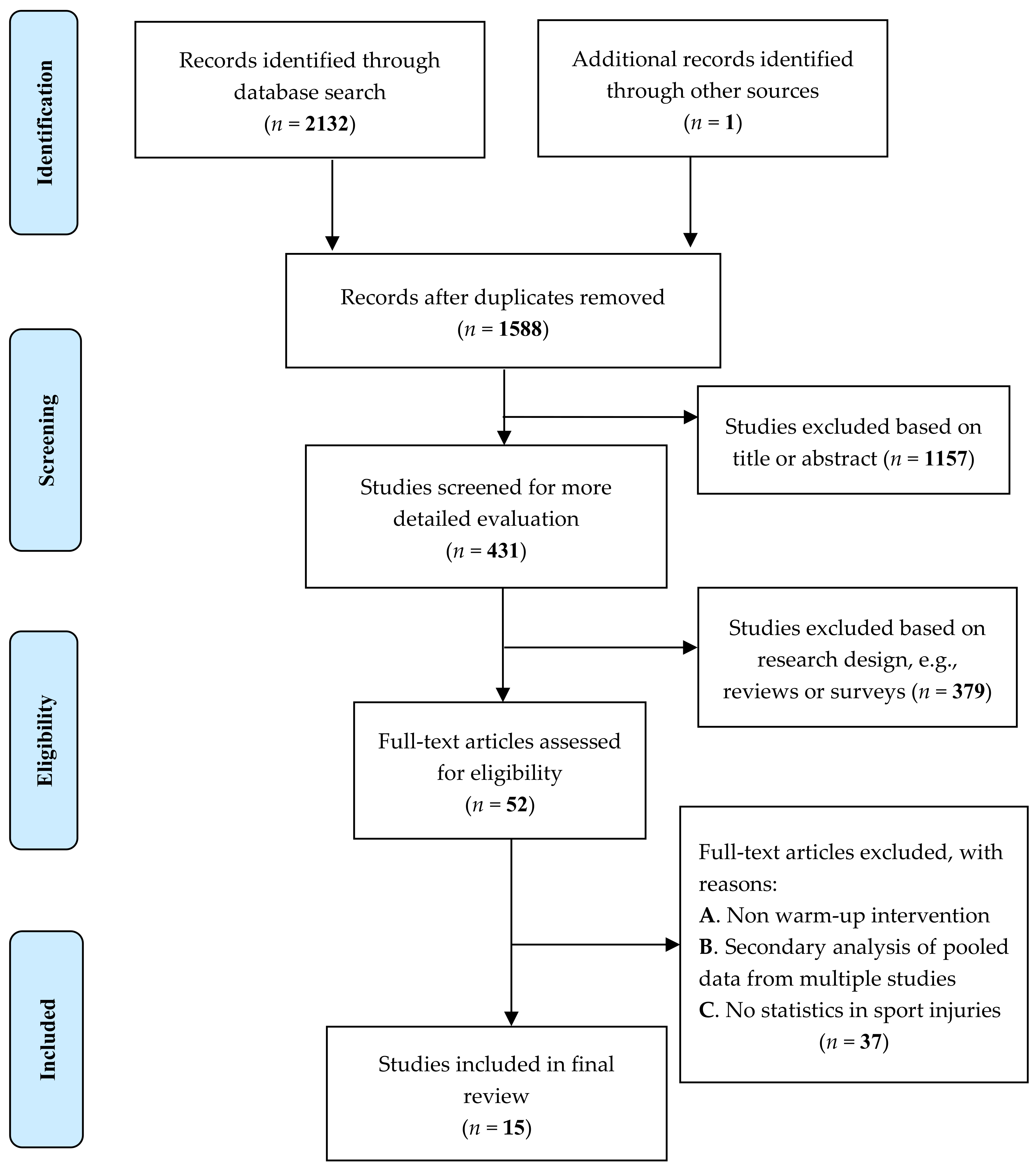
2.3. Selection of Studies
2.4. Data Extraction
2.5. Quality Evaluation of Selected Studies
2.6. Data Analysis
2.6.1. Meta-Analysis
2.6.2. Heterogeneity
2.6.3. Subgroup Analysis
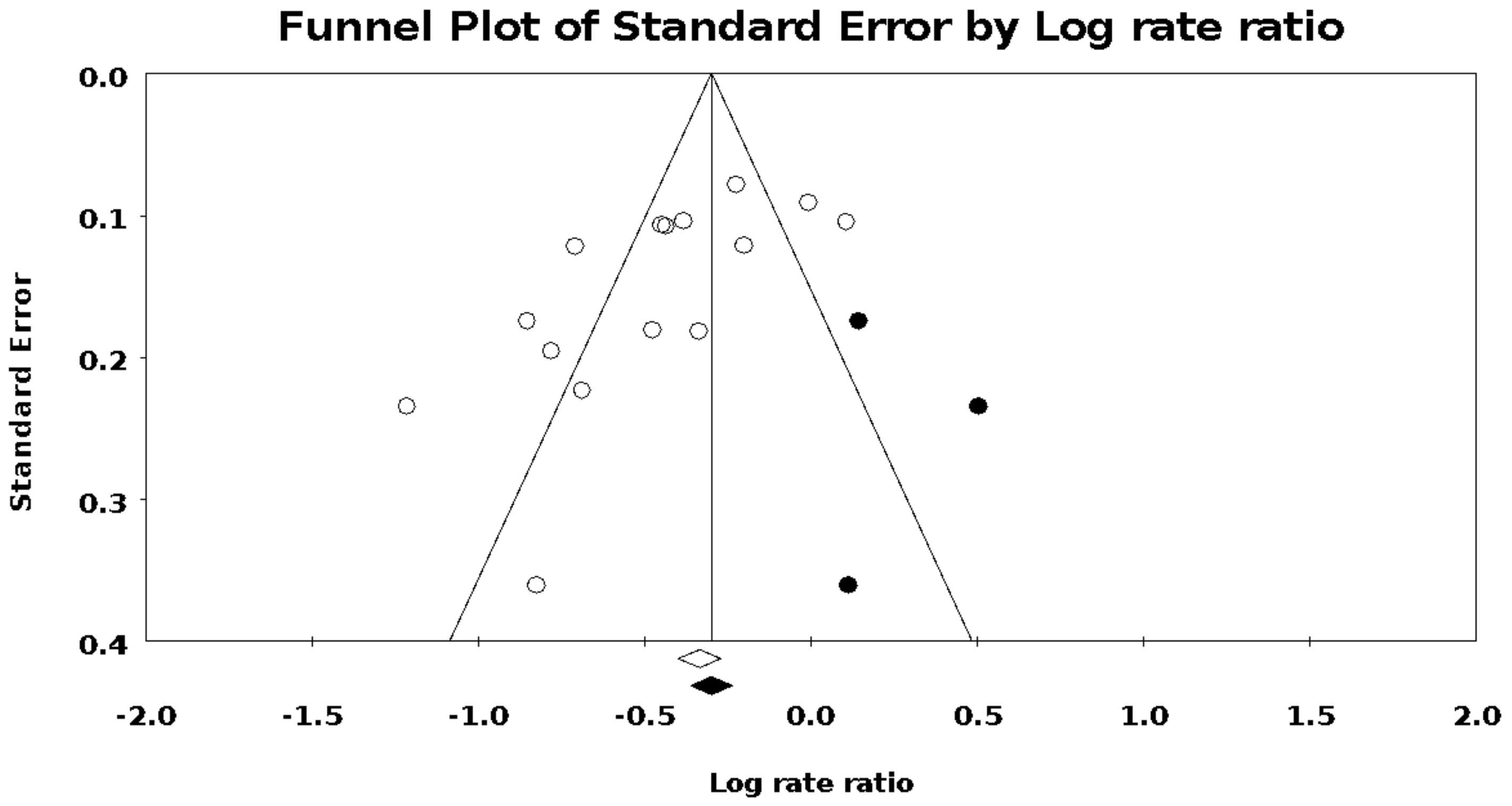
2.6.4. Publication Bias
2.6.5. Sensitivity Analysis
3. Results
3.1. Risk of Bias
3.2. Research Features
3.3. Meta Analysis: Injury Rate Ratio
3.4. Publication Bias
3.5. Subgroup Analysis
3.6. Sensitivity Analysis
4. Discussion
5. Conclusions
6. Implication
7. Research Strengths and Limitations
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Database | Total Records Found | Cumulative Total |
|---|---|---|
| Pubmed | 246 | 246 |
| Embase | 346 | 592 |
| Web of Science | 334 | 926 |
| Cochrane CRCT | 749 | 1675 |
| SportDISCUS | 457 | 2132 |
| Duplicates Removed | 544 | 1588 |
Appendix B
| No. | Terms | Variations | Result |
|---|---|---|---|
| #1 | Child and Adolescent | “Adolescents”[Title/Abstract] OR “Adolescence”[Title/Abstract] OR “Teens”[Title/Abstract] OR “Teen”[Title/Abstract] OR “Teenagers”[Title/Abstract] OR “Teenager”[Title/Abstract] OR “Youth”[Title/Abstract] OR “Youths”[Title/Abstract] OR “adolescents female”[Title/Abstract] OR “adolescent female”[Title/Abstract] OR “female adolescent”[Title/Abstract] OR “female adolescents”[Title/Abstract] OR “adolescents male”[Title/Abstract] OR “adolescent male”[Title/Abstract] OR “male adolescent”[Title/Abstract] OR “male adolescents”[Title/Abstract] OR “Children”[Title/Abstract] OR “Child”[Title/Abstract] OR “Adolescent”[MeSH Terms] | 3,154,768 |
| #2 | Intervention /prevention | “prevent *”[Title/Abstract] OR “prophylaxis”[Title/Abstract] OR “avoidance”[Title/Abstract] OR “comprehensive”[Title/Abstract] OR “intervention”[Title/Abstract] OR “warm-up”[Title/Abstract] OR “warmup”[Title/Abstract] OR “program”[Title/Abstract] OR “programme”[Title/Abstract] OR “training”[Title/Abstract] OR “neuromuscular”[Title/Abstract] OR “balance”[Title/Abstract] OR “plyometric”[Title/Abstract] OR “proprioceptive”[Title/Abstract] OR “proprioception”[Title/Abstract] | 3,634,058 |
| #3 | Athletic Injuries | “injuries sports”[Title/Abstract] OR “injury sports”[Title/Abstract] OR “sports injury”[Title/Abstract] OR “sports injuries”[Title/Abstract] OR “injuries athletic”[Title/Abstract] OR “athletic injury”[Title/Abstract] OR “injury athletic”[Title/Abstract] OR “Athletic Injuries”[MeSH Terms] | 31,211 |
| #4 | Randomized controlled trial | “randomized controlled trial”[Publication Type] OR “randomized controlled trials as topic”[MeSH Terms] OR “randomized controlled trial”[All Fields] OR “randomized controlled trial”[All Fields] | 736,366 |
| #5 | #1AND#2AND #3AND#4 | (“Adolescents”[Title/Abstract] OR “Adolescence”[Title/Abstract] OR “Teens”[Title/Abstract] OR “Teen”[Title/Abstract] OR “Teenagers”[Title/Abstract] OR “Teenager”[Title/Abstract] OR “Youth”[Title/Abstract] OR “Youths”[Title/Abstract] OR “adolescents female”[Title/Abstract] OR “adolescent female”[Title/Abstract] OR “female adolescent”[Title/Abstract] OR “female adolescents”[Title/Abstract] OR “adolescents male”[Title/Abstract] OR “adolescent male”[Title/Abstract] OR “male adolescent”[Title/Abstract] OR “male adolescents”[Title/Abstract] OR “Children”[Title/Abstract] OR “Child”[Title/Abstract] OR “Adolescent”[MeSH Terms]) AND (“prevent*”[Title/Abstract] OR “prophylaxis”[Title/Abstract] OR “avoidance”[Title/Abstract] OR “comprehensive”[Title/Abstract] OR “intervention”[Title/Abstract] OR “warm-up”[Title/Abstract] OR “warmup”[Title/Abstract] OR “program”[Title/Abstract] OR “programme”[Title/Abstract] OR “training”[Title/Abstract] OR “neuromuscular”[Title/Abstract] OR “balance”[Title/Abstract] OR “plyometric”[Title/Abstract] OR “proprioceptive”[Title/Abstract] OR “proprioception”[Title/Abstract]) AND (“injuries sports”[Title/Abstract] OR “injury sports”[Title/Abstract] OR “sports injury”[Title/Abstract] OR “sports injuries”[Title/Abstract] OR “injuries athletic”[Title/Abstract] OR “athletic injury”[Title/Abstract] OR “injury athletic”[Title/Abstract] OR “Athletic Injuries”[MeSH Terms]) AND (“randomized controlled trial”[Publication Type] OR “randomized controlled trials as topic”[MeSH Terms] OR “randomized controlled trial”[All Fields] OR “randomised controlled trial”[All Fields]) | 246 |
| No. | Terms | Variation | Results |
|---|---|---|---|
| #4 | #1 AND #2 AND #3 | 346 | |
| #3 | Randomized Controlled Trial | ‘randomized controlled trial’/exp OR ‘randomized controlled trial’ | 921,357 |
| #2 | Sport Injury | ‘injuries, sports’ OR ‘injury, sports’ OR ‘sports injury’/exp OR ‘sports injury’ OR ‘sports injuries’ OR ‘injuries, athletic’ OR ‘athletic injury’/exp OR ‘athletic injury’ OR ‘sport injury’/exp OR ‘sport injury’ | 38,111 |
| #1 | Youth Sport | ‘adolescent *’ OR ‘adolescence’/exp OR ‘adolescence’ OR ‘teens’ OR ‘teen’ OR ‘teenagers’ OR ‘teenager’/exp OR ‘teenager’ OR ‘youth’/exp OR ‘youth’ OR ‘youths’ OR ‘adolescents, female’ OR ‘adolescent, female’ OR ‘female adolescent’ OR ‘female adolescents’ OR ‘adolescents, male’ OR ‘adolescent, male’ OR ‘male adolescent’ OR ‘male adolescents’ OR ‘children’/exp OR ‘children’ OR ‘child’/exp OR child | 5,094,217 |
| Terms | Variations | Result |
|---|---|---|
| Adolescents, Athletic injuries/sport injuries, Randomized controlled trial | TS = (Adolescent OR Adolescents OR Adolescence OR Teens OR Teen OR Teenagers OR Teenager OR Youth OR Youths OR Adolescents, Female OR Adolescent, Female OR Female Adolescent OR Female Adolescents OR Adolescents, Male OR Adolescent, Male OR Male Adolescent OR Male Adolescents OR Children OR Child) AND TS = (Athletic Injuries OR Injuries, Sports OR Injury, Sports OR Sports Injury OR Sports Injuries OR Injuries, Athletic OR Athletic Injury OR Injury, Athletic) AND TS = (Randomized Controlled Trial OR Random) | 334 |
| No. | Terms | Variation | Results |
|---|---|---|---|
| #1 | Adolescent | MeSH descriptor: [Adolescent] explode all trees | 108,800 |
| #2 | (Adolescent *):ti,ab,kw OR (Teen *):ti,ab,kw OR (Teenager *):ti,ab,kw OR (Youth *):ti,ab,kw OR (Adolescent *, Female):ti,ab,kw (Word variations have been searched) | 149,109 | |
| #3 | (Female Adolescent *):ti,ab,kw OR (Adolescent *, Male):ti,ab,kw OR (Male Adolescent *):ti,ab,kw OR (Child *):ti,ab,kw (Word variations have been searched) | 252,069 | |
| #4 | #1 OR #2 OR #3 | 268,241 | |
| #5 | Athletic Injuries | MeSH descriptor: [Athletic Injuries] explode all trees | 753 |
| #6 | (Injur *, Sports):ti,ab,kw OR (Sports Injur *):ti,ab,kw OR (Injur *, Athletic):ti,ab,kw OR (Athletic Injury):ti,ab,kw (Word variations have been searched) | 2386 | |
| #7 | #5 OR #6 | 2593 | |
| #8 | #3 AND #7 | 749 |
| No. | Terms | Variation | Results |
|---|---|---|---|
| #1 | Adolescent and Child | DE “TEENAGERS” OR DE “SCHOOL children” OR adolescen * OR teen * OR child * | 169,694 |
| #2 | Athletic Injuries | DE “SPORTS injuries” OR DE “ACHILLES tendinitis” OR DE “AEROBICS injuries” OR DE “AQUATIC sports injuries” OR DE “BASEBALL injuries” OR DE “BASKETBALL injuries” OR DE “BOXING injuries” OR DE “COMMOTIO cordis” OR DE “CRICKET injuries” OR DE “DELAYED onset muscle soreness” OR DE “EQUESTRIAN accidents” OR DE “FOOTBALL injuries” OR DE “GOLF injuries” OR DE “GYMNASTICS injuries” OR DE “HIKING injuries” OR DE “HOCKEY injuries” OR DE “HORSE sports injuries” OR DE “IN-line skating injuries” OR DE “JOGGING injuries” OR DE “JUDO injuries” OR DE “JUMPER’S knee” OR DE “KARATE injuries” OR DE “MARTIAL arts injuries” OR DE “MOTORSPORTS injuries” OR DE “NETBALL injuries” ORDE “RACKET games injuries” OR DE “RUGBY football injuries” OR DE “RUNNING injuries” OR DE “SKATEBOARDING injuries” OR DE “SOCCER injuries” OR DE “TENNIS injuries” OR DE “TURF toe” OR DE “VAULTING injuries” OR DE “WALKING (Sports) injuries” OR DE “WEIGHT training injuries” OR DE “WINTER sports injuries” | 21,237 |
| #3 | #1 AND #2 | 1548 | |
| #4 | Warmup | DE “WARMUP” OR warmup OR balance OR “neuromuscular training” | 39,465 |
| #5 | Prevention | DE “PREVENTION” OR intervention” or program | 271,538 |
| #6 | #3 AND #4 | 102 | |
| #7 | #3 AND #5 | 424 | |
| #8 | #6 OR #7 | 490 | |
| #9 | #8 Limited to Scholarly (Peer Reviewed) Journals | 457 |
References
- Molcho, M.; Harel, Y.; Pickett, W.; Scheidt, P.C.; Mazur, J.; Overpeck, M.D. The epidemiology of non-fatal injuries among 11-, 13- and 15-year old youth in 11 countries: Findings from the 1998 WHO-HBSC cross national survey. Int. J. Inj. Control Saf. Promot. 2006, 13, 205–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gore, G.C.; Magdalinos, H.; Pless, I.B. School Injuries and Preventive Policies and Programs. Can. J. Public Health 2004, 95, 424–428. [Google Scholar] [CrossRef] [PubMed]
- Owoeye, O.B.A.; Palacios-Derflingher, L.M.; Emery, C.A. Prevention of Ankle Sprain Injuries in Youth Soccer and Basketball: Effectiveness of a Neuromuscular Training Program and Examining Risk Factors. Clin. J. Sport Med. 2018, 28, 325–331. [Google Scholar] [CrossRef] [PubMed]
- Hornbeck, K.; Peterson, A. Neuromuscular training program reduces knee injuries among adolescent female soccer players. J. Pediatrics 2012, 161, 970–971. [Google Scholar] [CrossRef] [PubMed]
- Beaudouin, F.; Rössler, R.; Aus der Fünten, K.; Bizzini, M.; Chomiak, J.; Verhagen, E.; Junge, A.; Dvorak, J.; Lichtenstein, E.; Meyer, T.; et al. Effects of the ’11+ Kids’ injury prevention programme on severe injuries in children’s football: A secondary analysis of data from a multicentre cluster-randomised controlled trial. Br. J. Sports Med. 2019, 53, 1418–1423. [Google Scholar] [CrossRef] [PubMed]
- Steffen, K.; Myklebust, G.; Olsen, O.E.; Holme, I.; Bahr, R. Preventing injuries in female youth football—cluster-randomized controlled trial. Scand. J. Med. Sci. Sports 2008, 18, 605–614. [Google Scholar] [CrossRef]
- Zakaria, A.A.; Kiningham, R.B.; Sen, A. Effects of Static and Dynamic Stretching on Injury Prevention in High School Soccer Athletes: A Randomized Trial. J. Sport Rehabil. 2015, 24, 229–235. [Google Scholar] [CrossRef]
- Emery, C.A.; van den Berg, C.; Richmond, S.A.; Palacios-Derflingher, L.; McKay, C.D.; Doyle-Baker, P.K.; McKinlay, M.; Toomey, C.M.; Nettel-Aguirre, A.; Verhagen, E.; et al. Implementing a junior high school-based programme to reduce sports injuries through neuromuscular training (iSPRINT): A cluster randomised controlled trial (RCT). Br. J. Sports Med. 2019, 54, 913–919. [Google Scholar] [CrossRef]
- McGowan, C.J.; Pyne, D.B.; Thompson, K.G.; Rattray, B. Warm-Up Strategies for Sport and Exercise: Mechanisms and Applications. Sports Med. 2015, 11, 1523–1546. [Google Scholar] [CrossRef]
- Woods, K.; Bishop, P.; Jones, E. Warm-Up and Stretching in the Prevention of Muscular Injury. Sports Med. 2007, 37, 1089–1099. [Google Scholar] [CrossRef]
- Furlan, A.D.; Pennick, V.; Bombardier, C.; van Tulder, M.; Editorial Board, C.B.R.G. 2009 updated method guidelines for systematic reviews in the Cochrane Back Review Group. Spine 2009, 34, 1929–1941. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef]
- Soomro, N.; Sanders, R.; Hackett, D.; Hubka, T.; Ebrahimi, S.; Freeston, J.; Cobley, S. The Efficacy of Injury Prevention Programs in Adolescent Team Sports: A Meta-analysis. Am. J. Sports Med. 2016, 44, 2415–2424. [Google Scholar] [CrossRef] [PubMed]
- Soligard, T.; Myklebust, G.; Steffen, K.; Holme, I.; Silvers, H.; Bizzini, M.; Junge, A.; Dvorak, J.; Bahr, R.; Andersen, T.E. Comprehensive warm-up programme to prevent injuries in young female footballers: Cluster randomised controlled trial. BMJ 2008, 337, a2469. [Google Scholar] [CrossRef] [Green Version]
- Rössler, R.; Junge, A.; Bizzini, M.; Verhagen, E.; Chomiak, J.; Aus der Fünten, K.; Meyer, T.; Dvorak, J.; Lichtenstein, E.; Beaudouin, F.; et al. A Multinational Cluster Randomised Controlled Trial to Assess the Efficacy of ’11+ Kids’: A Warm-Up Programme to Prevent Injuries in Children’s Football. Sports Med. 2018, 48, 1493–1504. [Google Scholar] [CrossRef] [Green Version]
- LaBella, C.R.; Huxford, M.R.; Grissom, J.; Kim, K.Y.; Peng, J.; Christoffel, K.K. Effect of neuromuscular warm-up on injuries in female soccer and basketball athletes in urban public high schools: Cluster randomized controlled trial. Arch. Pediatrics Adolesc. Med. 2011, 165, 1033–1040. [Google Scholar] [CrossRef] [Green Version]
- Marshall, D.A.; Lopatina, E.; Lacny, S.; Emery, C.A. Economic impact study: Neuromuscular training reduces the burden of injuries and costs compared to standard warm-up in youth soccer. Br. J. Sports Med. 2016, 50, 1388–1393. [Google Scholar] [CrossRef]
- Richmond, S.A.; Jian, K.; Doyle-Baker, P.K.; Nettel-Aguirre, A.; Emery, C.A. A School-Based Injury Prevention Program to Reduce Sport Injury Risk and Improve Healthy Outcomes in Youth: A Pilot Cluster-Randomized Controlled Trial. Clin. J. Sport Med. 2016, 26, 291–298. [Google Scholar] [CrossRef]
- Emery, C.A.; Meeuwisse, W.H. The effectiveness of a neuromuscular prevention strategy to reduce injuries in youth soccer: A cluster-randomised controlled trial. Br. J. Sports Med. 2010, 44, 555–562. [Google Scholar] [CrossRef]
- Emery, C.A.; Rose, M.S.; McAllister, J.R.; Meeuwisse, W.H. A prevention strategy to reduce the incidence of injury in high school basketball: A cluster randomized controlled trial. Clin. J. Sport Med. 2007, 17, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Slauterbeck, J.R.; Choquette, R.; Tourville, T.W.; Krug, M.; Mandelbaum, B.R.; Vacek, P.; Beynnon, B.D. Implementation of the FIFA 11+Injury Prevention Program by High School Athletic Teams Did Not Reduce Lower Extremity Injuries: A Cluster Randomized Controlled Trial. Am. J. Sports Med. 2019, 47, 2844–2852. [Google Scholar] [CrossRef] [PubMed]
- Rossler, R.; Donath, L.; Verhagen, E.; Junge, A.; Schweizer, T.; Faude, O. Exercise-based injury prevention in child and adolescent sport: A systematic review and meta-analysis. Sports Med. 2014, 44, 1733–1748. [Google Scholar] [CrossRef] [PubMed]
- Lauersen, J.B.; Bertelsen, D.M.; Andersen, L.B. The effectiveness of exercise interventions to prevent sports injuries: A systematic review and meta-analysis of randomised controlled trials. Br. J. Sports Med. 2014, 48, 871–877. [Google Scholar] [CrossRef] [PubMed]
- Hubscher, M.; Zech, A.; Pfeifer, K.; Hansel, F.; Vogt, L.; Banzer, W. Neuromuscular Training for Sports Injury Prevention: A Systematic Review. Med. Sci. Sports Exerc. 2010, 42, 413–421. [Google Scholar] [CrossRef]
- Bishop, D. Warm up II—Performance changes to structure the warm following active warm up and how up. Sports Med. 2003, 33, 483–498. [Google Scholar] [CrossRef]
- Olsen, O.E.; Myklebust, G.; Engebretsen, L.; Holme, I.; Bahr, R. Exercises to prevent lower limb injuries in youth sports: Cluster randomised controlled trial. BMJ 2005, 330, 449. [Google Scholar] [CrossRef] [Green Version]
- Owoeye, O. Efficacy of the FIFA 11+ Warm-Up Programme in Male Youth Football: A Cluster Randomised Controlled Trial. J. Sports Sci. Med. 2014, 13, 321. [Google Scholar]
- Akerlund, I.; Walden, M.; Sonesson, S.; Hagglund, M. Forty-five per cent lower acute injury incidence but no effect on overuse injury prevalence in youth floorball players (aged 12–17 years) who used an injury prevention exercise programme: Two-armed parallel-group cluster randomised controlled trial. Br. J. Sports Med. 2020, 54, 1028–1035. [Google Scholar] [CrossRef] [Green Version]
- Hilska, M.; Leppanen, M.; Vasankari, T.; Clarsen, B.; Aaltonen, S.; Bahr, R.; Haapasalo, H.; Parkkari, J.; Kannus, P.; Pasanen, K. Neuromuscular training warm-up in the prevention of overuse lower extremity injuries in children’s football: A cluster-randomized controlled trial. Transl. Sports Med. 2021, 4, 849–858. [Google Scholar] [CrossRef]
- Zarei, M.; Abbasi, H.; Namazi, P.; Asgari, M.; Rommers, N.; Rossler, R. The 11+Kids warm-up programme to prevent injuries in young Iranian male high-level football (soccer) players: A cluster-randomised controlled trial. J. Sci. Med. Sport 2020, 23, 469–474. [Google Scholar] [CrossRef] [PubMed]
- Di Scala, C.; Gallagher, S.S.; Schneps, S.E. Causes and Outcomes of Pediatric Injuries Occurring at School. J. Sch. Health 1997, 67, 384–389. [Google Scholar] [CrossRef] [PubMed]
- Longo, R. The FIFA 11+ Program Is Effective in Preventing Injuries in Elite Male Basketball Players: A Cluster Randomized Controlled Trial. Am. J. Sports Med. 2012, 40, 996–1005. [Google Scholar] [CrossRef] [PubMed]
- Soligard, T.; Nilstad, A.; Steffen, K.; Myklebust, G.; Holme, I.; Dvorak, J.; Bahr, R.; Andersen, T.E. Compliance with a comprehensive warm-up programme to prevent injuries in youth football. Br. J. Sports Med. 2010, 44, 787–793. [Google Scholar] [CrossRef] [PubMed]
- Steffen, K.; Emery, C.A.; Romiti, M.; Kang, J.; Bizzini, M.; Dvorak, J.; Finch, C.F.; Meeuwisse, W.H. High adherence to a neuromuscular injury prevention programme (FIFA 11+) improves functional balance and reduces injury risk in Canadian youth female football players: A cluster randomised trial. Br. J. Sports Med. 2013, 47, 794–802. [Google Scholar] [CrossRef] [Green Version]
- Rössler, R.; Verhagen, E.; Rommers, N.; Dvorak, J.; Junge, A.; Lichtenstein, E.; Donath, L.; Faude, O. Comparison of the ‘11+ Kids’ injury prevention programme and a regular warmup in children’s football (soccer): A cost effectiveness analysis. Br. J. Sports Med. 2019, 53, 309–314. [Google Scholar] [CrossRef] [Green Version]



| Study Name | Risk of Bias Assessment b | Score | % | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | |||
| LaBella et al., 2011 | + | + | − | − | − | + | + | + | ? | ? | + | + | 7 | 58.3 |
| Richmond et al., 2016 | + | + | + | − | ? | + | + | + | + | ? | + | + | 9 | 75.0 |
| Soligard et al., 2008 | − | + | − | − | + | + | + | + | + | ? | + | + | 8 | 66.7 |
| Emery et al., 2007 | + | ? | − | − | + | + | + | + | + | ? | + | + | 8 | 66.7 |
| Rossler et al., 2018 | + | ? | − | − | + | + | + | − | + | + | + | + | 8 | 66.7 |
| Emery et al., 2019 | + | + | + | + | + | + | + | ? | + | + | ? | + | 10 | 83.3 |
| Steffen et al., 2008 | − | + | − | − | − | + | + | + | + | ? | + | + | 7 | 58.3 |
| Emery and Meeuwisse, 2010 | ? | + | + | + | ? | + | + | + | + | ? | + | + | 9 | 75.0 |
| Longo et al., 2012 | + | + | − | − | + | + | + | + | − | + | + | + | 9 | 75.0 |
| Olsen et al., 2015 | + | + | ? | − | + | + | + | + | + | + | + | + | 10 | 83.3 |
| Owoeye et al., 2014 | + | ? | ? | − | − | + | + | + | + | + | + | 7 | 58.3 | |
| Akerlund et al., 2020 | + | − | − | − | + | + | + | ? | + | + | + | + | 8 | 66.7 |
| Slauterbeck et al., 2019 | + | − | − | − | ? | + | + | ? | + | + | − | + | 6 | 50.0 |
| Hiska et al., 2021 | + | + | + | − | + | + | + | ? | + | − | + | + | 9 | 75.0 |
| Zarei et al., 2020 | + | + | + | − | + | − | + | − | + | + | − | + | 8 | 66.7 |
| Study | Country | Settings | Sex | Age | Sport | Level | Design | Intervention | Outcomes | Quality |
|---|---|---|---|---|---|---|---|---|---|---|
| LaBella et al., 2011 | USA | School-based | F | N/A | S.B. | Amateur | Cluster-RCT | Neuromuscular | LE | 7 |
| Richmond et al., 2016 | Canada | School-based | Mx | 11–15 | P.E. | Amateur | Cluster-RCT | Neuromuscular | LE and UE | 9 |
| Soligard et al., 2008 | Norway | Non-School-based | F | 13–17 | S | Club | Cluster-RCT | Comprehensive | LE | 8 |
| Emery et al., 2007 | Canada | School-based | Mx | 12–18 | B | Amateur | Cluster-RCT | Balance | LE | 8 |
| Rossler et al., 2018 | Multi Countries | Non-School-based | Mx | 7–12 | S | Club | Cluster-RCT | Comprehensive | LE and UE | 8 |
| Emery et al., 2019 | Canada | School-based | Mx | 11–16 | P.E. | Amateur | Cluster-RCT | Neuromuscular | LE and UE | 10 |
| Steffen et al., 2008 | Norway | Non-School-based | F | 16–18 | S | Club | Cluster-RCT | Comprehensive | LE and UE | 7 |
| Emery and Meeuwisse, 2010 | Canada | Non-School-based | Mx | 13–18 | S | Club | Cluster-RCT | Neuromuscular | LE | 6 |
| Longo et al., 2012 | Italy | Non-School-based | M | 13.5 ± 2.3 | B | Club | Cluster-RCT | Comprehensive | LE | 9 |
| Olsen et al., 2005 | Norway | Non-School-based | Mx | 15–17 | H | Club | Cluster-RCT | Comprehensive | LE | 10 |
| Owoeye et al., 2014 | Nigeria | Non-School-based | M | 14–19 | S | Club | Cluster-RCT | Comprehensive | LE and UE | 7 |
| Akerlund et al., 2020 | Sweden | Non-school-based | Mx | 12–17 | F | Amateur | Cluster-RCT | Comprehensive | LE and UE | 8 |
| Slauterbeck et al., 2019 | USA | School-based | Mx | N/A | Ms | Amateur | Cluster-RCT | Comprehensive | LE | 6 |
| Hiska et al., 2021 | Finland | Non-school-based | Mx | 9–14 | S | Club | Cluster-RCT | Neuromuscular | LE | 9 |
| Zarei et al., 2020 | Iran | Non-school-based | M | 7–14 | S | Club | Cluster-RCT | Comprehensive | LE | 8 |
| Study | Sex | Level | Sport | Type of WIP | Intervention Program | Session | Duration | Compliance | |
|---|---|---|---|---|---|---|---|---|---|
| Intervention Group | Control Group | ||||||||
| LaBella et al., 2011 | F | Amateur | S.B. | NMT warm-up in progressive strengthening, plyometric, balance, and agility exercises 20 min | As usual warm-up | Neuromuscular | 3/wk appr. | 8 mon | 80.4% |
| Richmond et al., 2016 | Mx | Amateur | P.E. | Warm-up in NMT Ae sessions 10 min + Exercises for core/lower extremity strength and balance 5min | Warm-up in low-intensity jogging 10 min + static and Dy stretch 5 min | Neuromuscular | 2–3/wk | 3 mon | ≥84% |
| Soligard et al., 2008 | F | Club | S | Slow speed running + exercises for strength, balance and jumping + speed running with cutting movements 20 min | As usual | Comprehensive | ≥2/wk | 8 mon | 77% |
| Emery et al., 2007 | Mx | Amateur | B | Ae, St, Dy stretches 10 min + Sports-specific balance warm-up 5 min + home wobble board exercise 20 min | Ae, St, Dy stretches 10 min | Balance | 5/wk appr. | 12 mon | 73.3% |
| Rossler et al., 2018 | Mx | Club | S | 3 exercises for unilateral, Dy stability of the lower extremities +3 exercises for body and trunk strength/stability +1 exercise for falling skills 15–20 min | As usual | Comprehensive | ≥2/wk | 8 mon | N/A |
| Emery et al., 2019 | Mx | Amateur | P.E. | NMT warm- up including Ae, agility, Str and balance exercises 10–15 min | Warm- up including Ae, static and Dy stretch | Neuromuscular | ≥2/wk | 3 mon | 77.7% |
| Steffen et al., 2008 | F | Amateur | S | FIFA 11 20 min | As usual | Comprehensive | 1/wk | 8 mon | 52% |
| Emery and Meeuwisse, 2010 | Mx | Club | S | Ae, St, Dy stretches 5 min+ Strength, agility and balance 10 min + 1 home wobbleboard exercise 15 min | Ae, St, Dy stretches 15 min | Neuromuscular | 3/wk | 5 mon | 81.25 |
| Longo et al., 2012 | M | Elite | B | FIFA 11 + 20 min | As usual | Comprehensive | 3/wk | 9 mon | 100% |
| Olsen et al., 2005 | Mx | Club | H | running, cutting, and landing technique as well as neuromuscular control, balance, and strength. 15–20 min | As usual | Comprehensive | 1/wk | 8 mon | 87% |
| Owoeye et al., 2014 | M | Club | S | FIFA 11+ 20 min | As usual | Comprehensive | 2/wk | 6 mon | 60% |
| Akerlund et al., 2020 | Mx | Amateur | F | Swedish Knee Control program 10–15 min + a Standardized running 5 min | As usual | Comprehensive | 1.45/wk avg | 6.5 mon | 84% |
| Slauterbeck et al., 2019 | Mx | Amateur | Ms | FIFA 11 + 15–20 min | As usual warmup | Comprehensive | 1–2/wk | 12 mon | 32% |
| Hiska et al., 2021 | Mx | Club | S | Ae, squat jump, side plank, single leg balance, walking lunges, single leg jumps, speed running 20 min | As usual warmup | Neuromuscular | 2–3/wk | 5 mon | 63% |
| Zarei et al., 2020 | M | Club | S | Unilateral, dynamic stability of the lower extremity, trunk strength and stability, falling technique 20 min | Aerobic, dynamic stretching and football-specific movements | Comprehensive | 2/wk | 9 mon | 67% |
| Moderator: Subgroup (No.of Studies) b | Mixed-Effects Analysis Between-Subgroup Comparison | Subgroup Heterogeneity | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Point Estimate | 95% CI | p-Value | Possible IRR Reduction, % | Q Value | p Value | Q Value c | p Value d | Subgroup I2 | |
| 1. Age | |||||||||
| -Middle school (12) | 0.63 | 0.51–0.77 | 0.000 | 37 | 78.73 | 0.00 | 84.95 | ||
| -Primary school (3) | 0.68 | 0.54–0.85 | 0.001 | 32 | 0.23 | 0.64 | 0.01 | 0.92 | 64.51 |
| 2. Sex | |||||||||
| -Male (3) | 0.47 | 0.36–0.62 | 0.000 | 53 | 0.00 | ||||
| -Female (3) | 0.68 | 0.44–1.04 | 0.072 | 32 | 68.03 | 0.00 | 90.35 | ||
| -Mixed (9) | 0.67 | 0.55–0.81 | 0.000 | 33 | 4.56 | 0.10 | 10.71 | 0.01 | 83.04 |
| 3. Settings | |||||||||
| -School-based (6) | 0.69 | 0.49–0.95 | 0.025 | 31 | 64.46 | 0.00 | 89.19 | ||
| -Non School-based (9) | 0.61 | 0.54–0.70 | 0.000 | 39 | 0.36 | 0.55 | 14.29 | 0.00 | 56.08 |
| 4. Level | |||||||||
| -Club (8) | 0.60 | 0.52–0.71 | 0.000 | 40 | 69.01 | 0.000 | 61.57 | ||
| -Amateur (7) | 0.68 | 0.52–0.91 | 0.008 | 32 | 0.55 | 0.46 | 9.73 | 0.002 | 88.19 |
| 5. WIP Type | |||||||||
| -Balance/Neuromuscular (5) | 0.59 | 0.43–0.82 | 0.001 | 41 | 78.60 | 0.000 | 84.62 | ||
| -Comprehensive (10) | 0.66 | 0.54–0.80 | 0.000 | 34 | 0.28 | 0.60 | 0.15 | 0.702 | 82.89 |
| 6. Injury Location | |||||||||
| -Upper and Lower EXT (6) | 0.61 | 0.46–0.81 | 0.001 | 39 | 78.57 | 0.000 | 85.33 | ||
| -Lower EXT (9) | 0.65 | 0.53–0.81 | 0.000 | 35 | 0.15 | 0.70 | 0.18 | 0.676 | 82.02 |
| 7. Compliance | |||||||||
| -<70% (5) | 0.81 | 0.65–1.01 | 0.064 | 19 | 50.40 | 0.000 | 82.48 | ||
| ->70% (10) | 0.56 | 0.48–0.67 | 0.000 | 44 | 6.24 | 0.01 | 28.34 | 0.000 | 67.35 |
| 8. Study quality | |||||||||
| -<60% (4) | 0.70 | 0.45–1.08 | 0.110 | 30 | 64.95 | 0.000 | 91.47 | ||
| ->60% (11) | 0.62 | 0.54–0.72 | 0.000 | 38 | 0.26 | 0.61 | 13.79 | 0.000 | 66.44 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ding, L.; Luo, J.; Smith, D.M.; Mackey, M.; Fu, H.; Davis, M.; Hu, Y. Effectiveness of Warm-Up Intervention Programs to Prevent Sports Injuries among Children and Adolescents: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 6336. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106336
Ding L, Luo J, Smith DM, Mackey M, Fu H, Davis M, Hu Y. Effectiveness of Warm-Up Intervention Programs to Prevent Sports Injuries among Children and Adolescents: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2022; 19(10):6336. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106336
Chicago/Turabian StyleDing, Liyi, Jianfeng Luo, Daniel M. Smith, Marcia Mackey, Haiqing Fu, Matthew Davis, and Yanping Hu. 2022. "Effectiveness of Warm-Up Intervention Programs to Prevent Sports Injuries among Children and Adolescents: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 19, no. 10: 6336. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106336