
Simple and Autonomous Sleep Signal Processing System for the Detection of Obstructive Sleep Apneas

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data
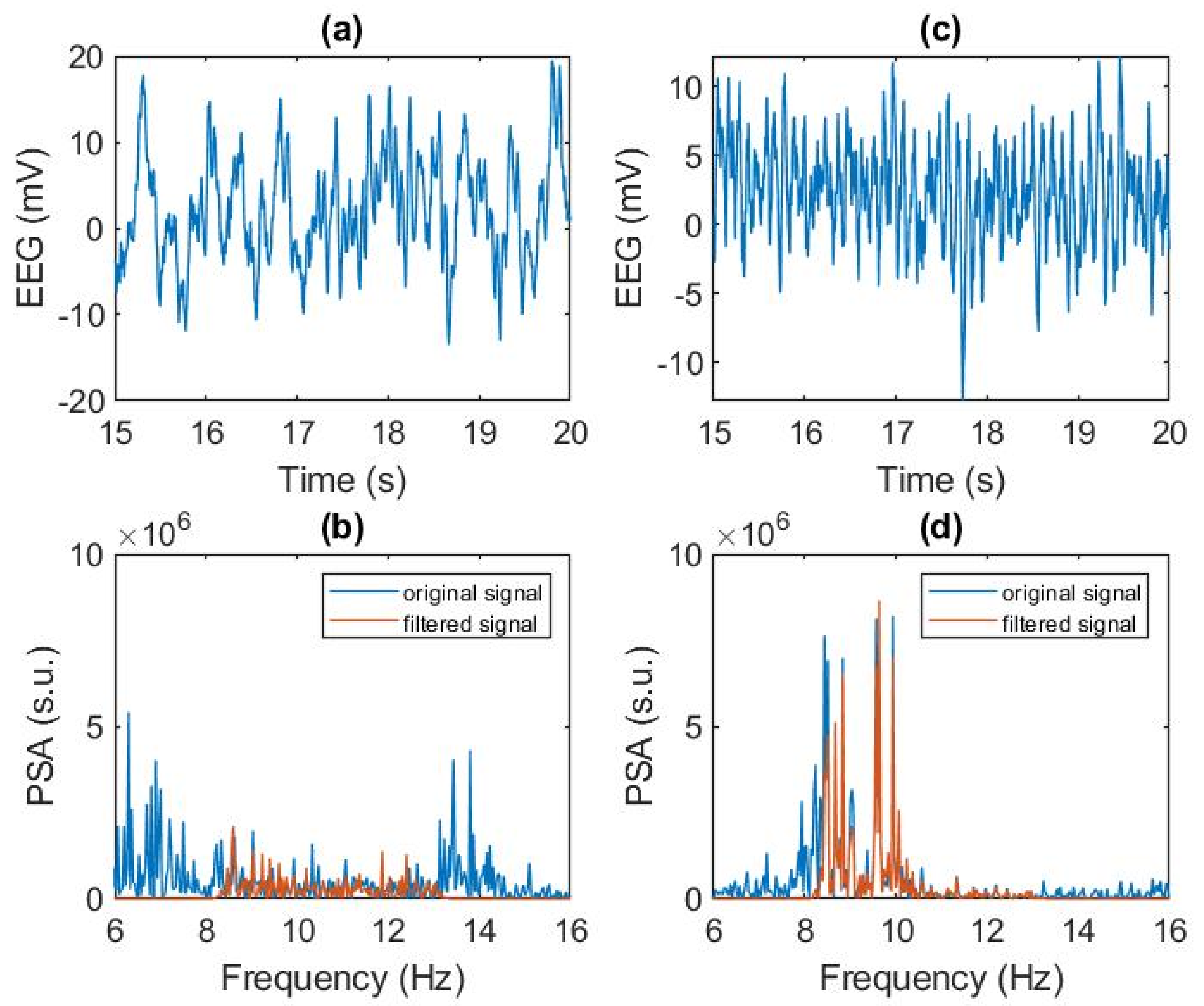
2.2. Signal Analysis
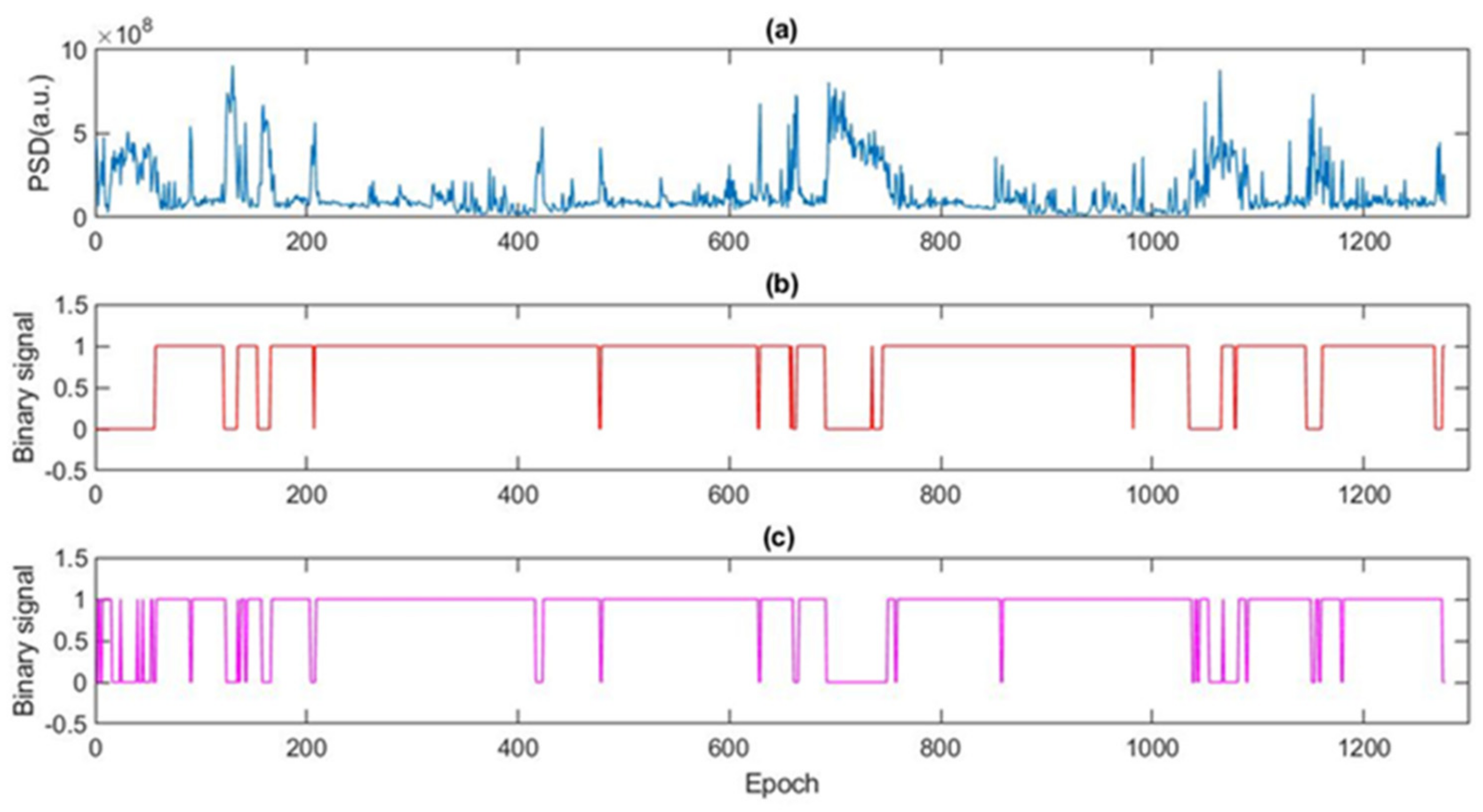
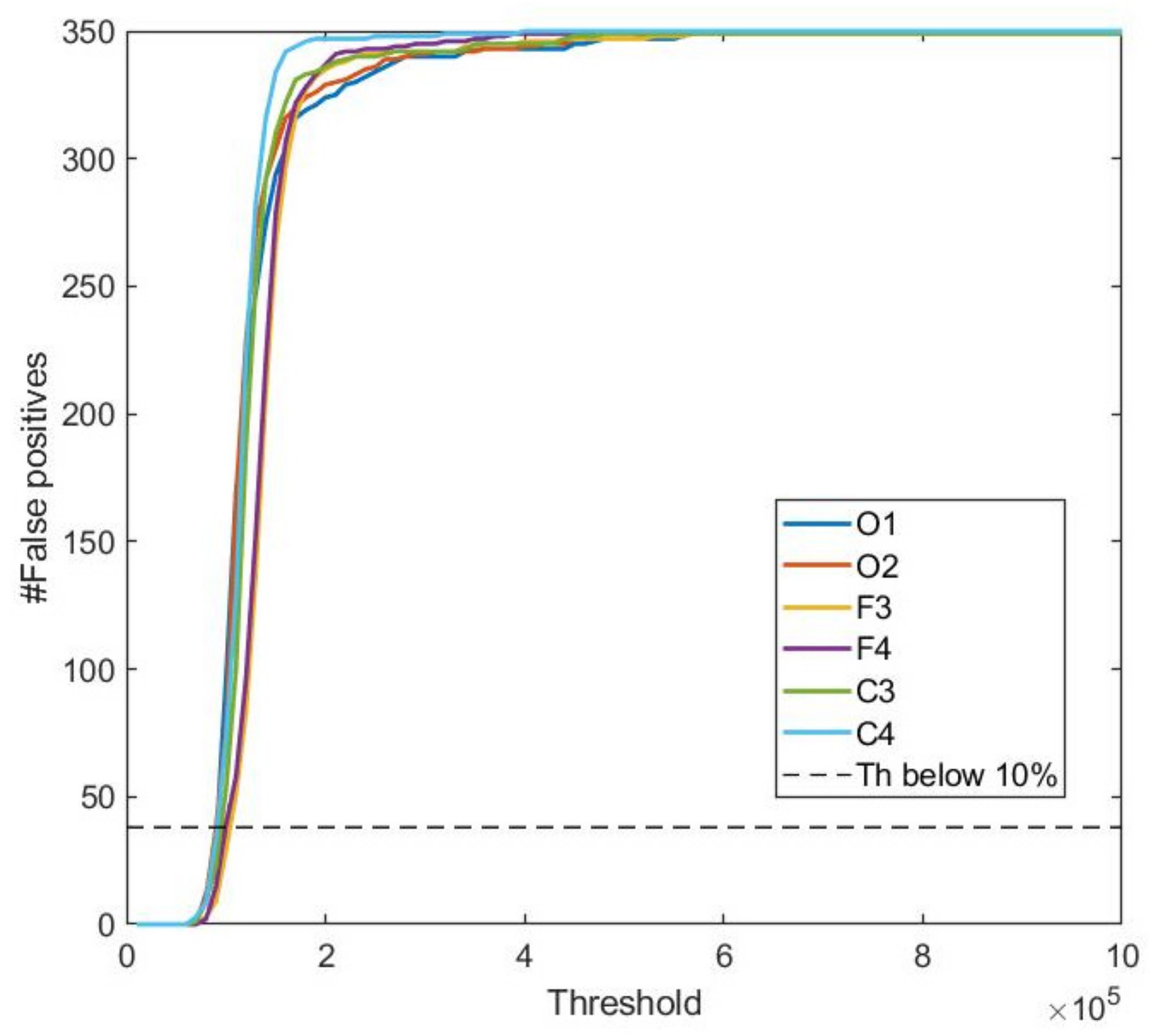
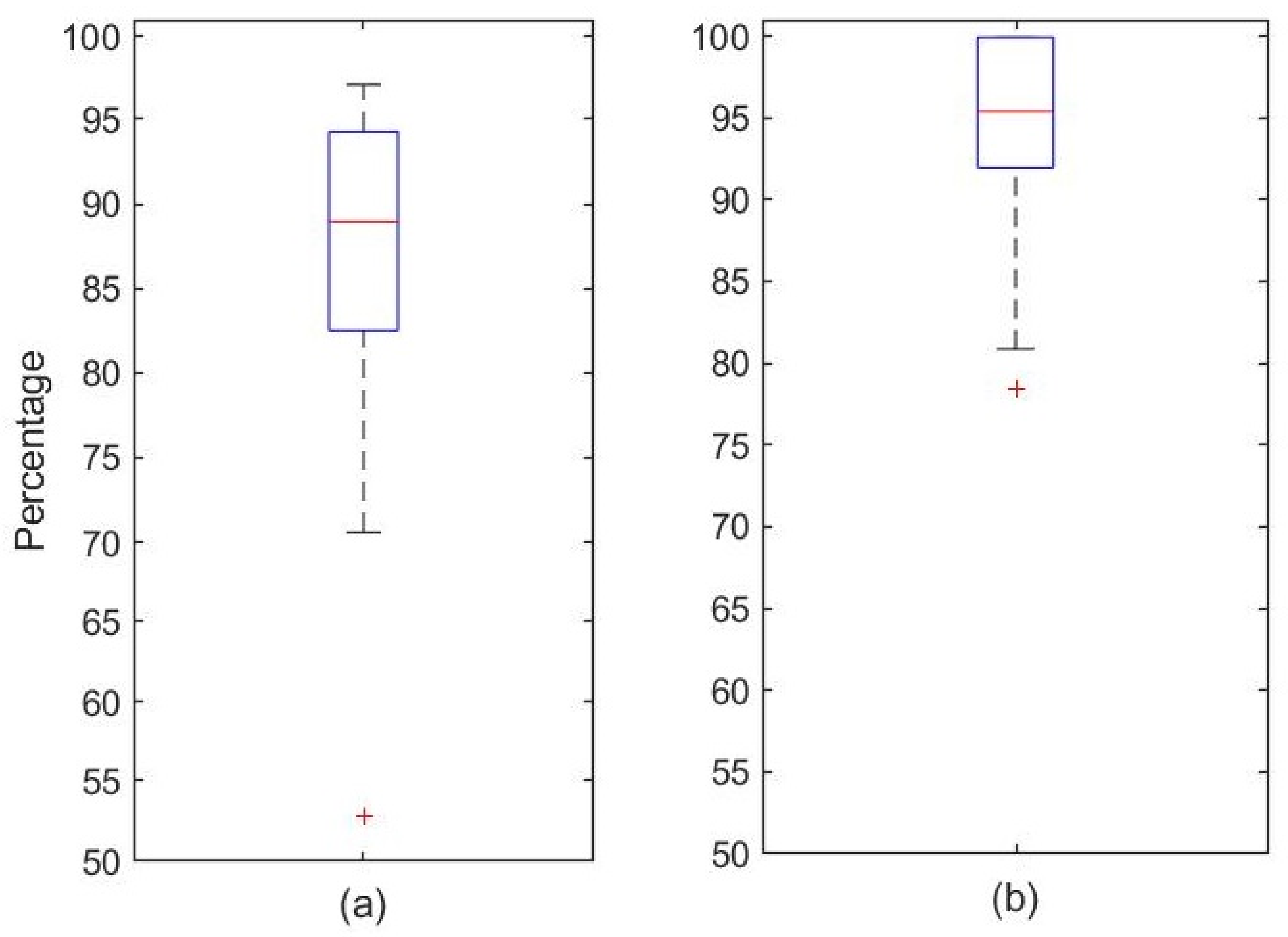
2.2.1. Detection of Awake/Sleep Stages
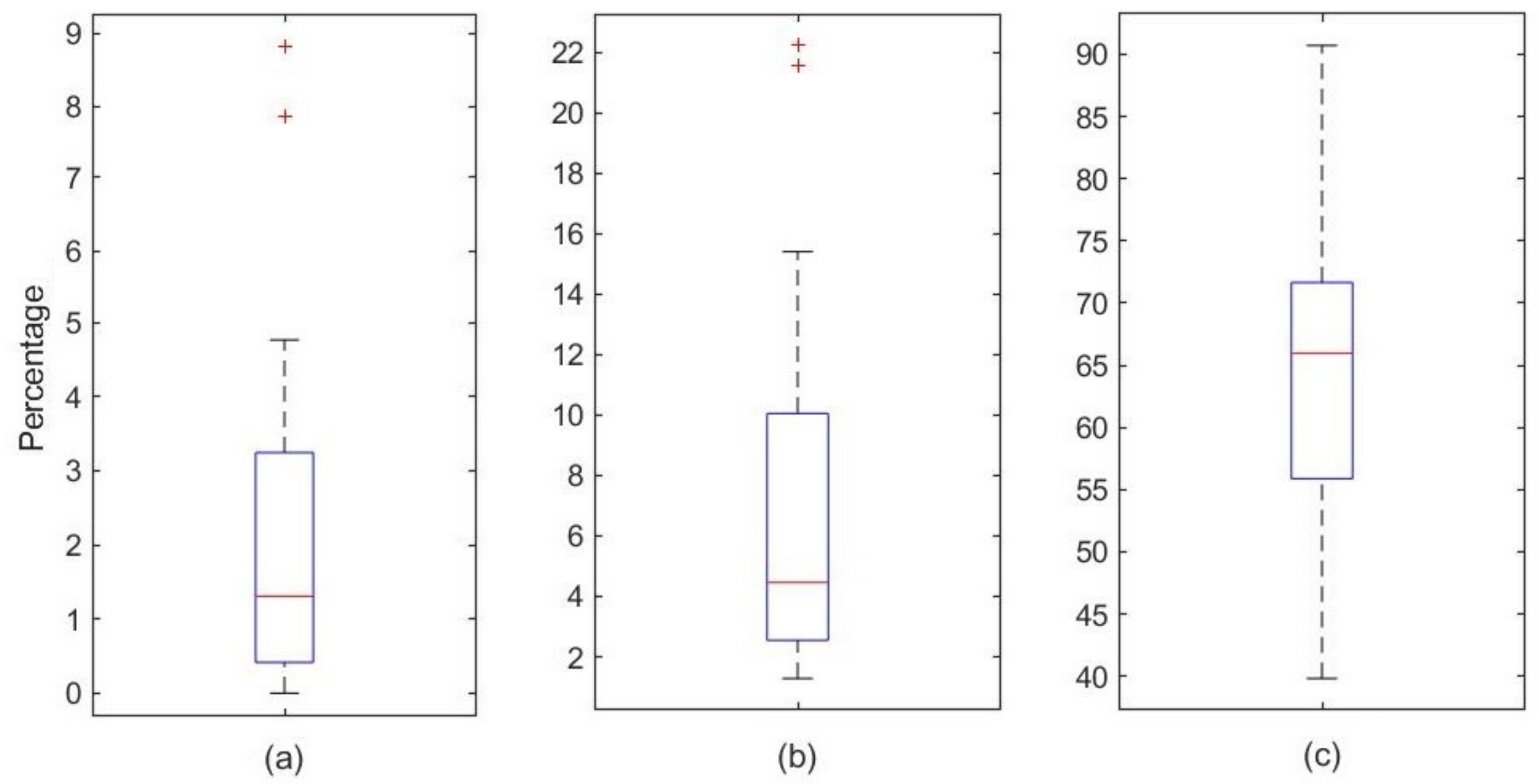
2.2.2. Detection of Sleep Apnea
- An apnea is scored when there is a drop in peak signal excursion by ≥90% of the amplitude signal of the oronasal pressure sensor RF2 compared to previous epochs amplitudes and that remains for ≥10 s.
- A hypopnea is scored when there is a reduction between ≥30% and <90% of the amplitude signal of the oronasal pressure sensor RF2 compared to previous epochs, during ≥10 s in association with ≥3% arterial oxygen desaturation.
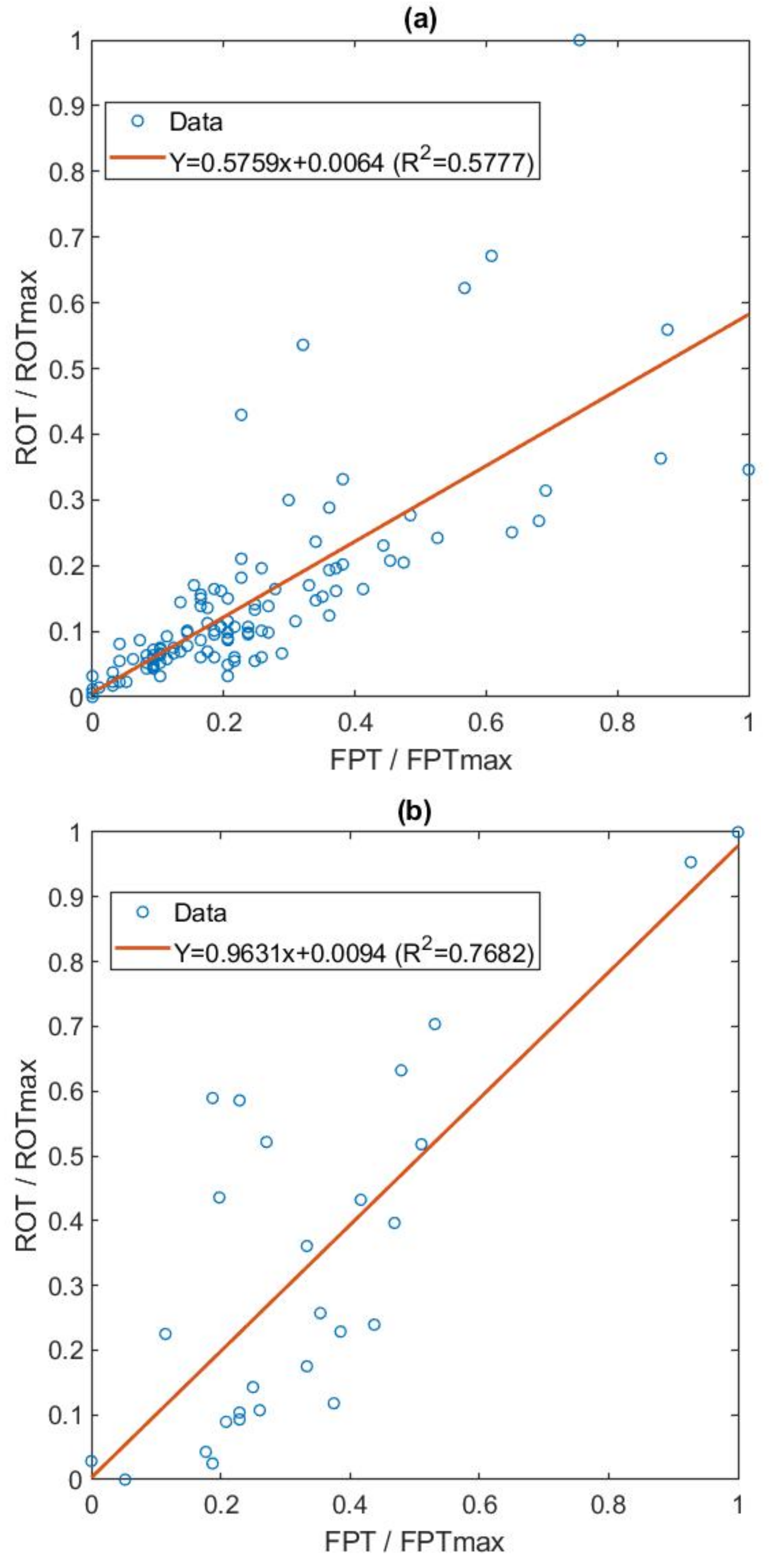
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Senaratna, C.V.; Perret, J.L.; Lodge, C.J.; Lowe, A.J.; Campbell, B.E.; Matheson, M.C.; Hamilton, G.S.; Dharmage, S.C. Prevalence of obstructive sleep apnea in the general population: A systematic review. Sleep Med. Rev. 2017, 34, 70–81. [Google Scholar] [CrossRef]
- Mediano, O.; González, N.; Montserrat, J.M.; Alonso-Álvarez, M.L.; Almendros, I.; Alonso-Fernández, A.; Barbé, F.; Borsini, E.; Caballero-Eraso, C.; Cano-Pumarega, I.; et al. Spanish Sleep Network. International consensus document on obstructive sleep apnea. Arch. Bronconeumol. 2022, 58, 52–68. [Google Scholar] [CrossRef] [PubMed]
- Apprill, M.; Weitzenblum, E.; Krieger, J.; Oswald, M.; Kurtz, D. Frequency and mechanism of daytime pulmonary hypertension in patients with obstructive sleep apnoea syndrome. Cor Vasa 1991, 33, 42–49. [Google Scholar] [PubMed]
- Peker, Y.; Kraiczi, H.; Hedner, J.; Loth, S.; Johansson, A.; Bende, M. An independent association between obstructive sleep apnoea and coronary artery disease. Eur. Respir. J. 1999, 14, 179–184. [Google Scholar] [CrossRef]
- Cepeda-Valery, B.; Acharjee, S.; Romero-Corral, A.; Pressman, G.S.; Gami, A.S. Obstructive sleep apnea and acute coronary syndromes: Etiology, risk, and management. Curr. Cardiol. Rep. 2014, 16, 535. [Google Scholar] [CrossRef]
- Arzt, M.; Young, T.; Peppard, P.E.; Finn, L.; Ryan, C.M.; Bayley, M.; Bradley, T.D. Dissociation of obstructive sleep apnea from hypersomnolence and obesity in patients with stroke. J. Cereb. Circ. 2010, 41, e129–e134. [Google Scholar] [CrossRef] [Green Version]
- Dyken, M.E.; Im, K.B. Obstructive sleep apnea and stroke. Chest 2009, 136, 1668–1677. [Google Scholar] [CrossRef] [PubMed]
- Gami, A.S.; Olson, E.J.; Shen, W.K.; Wright, R.S.; Ballman, K.V.; Hodge, D.O.; Herges, R.M.; Howard, D.E.; Somers, V.K. Obstructive sleep apnea and the risk of sudden cardiac death: A longitudinal study of 10,701 adults. J. Am. Coll. Cardiol. 2013, 62, 610–616. [Google Scholar] [CrossRef] [Green Version]
- Patil, S.P.; Ayappa, I.A.; Caples, S.M.; Kimoff, R.J.; Patel, S.R.; Harrod, C.G. Treatment of Adult Obstructive Sleep Apnea with Positive Airway Pressure: An American Academy of Sleep Medicine Clinical Practice Guideline. J. Clin. Sleep Med. 2019, 15, 335–343. [Google Scholar] [CrossRef] [Green Version]
- Rotenberg, B.W.; Murariu, D.; Pang, K.P. Trends in CPAP adherence over twenty years of data collection: A flattened curve. J. Otolaryngol. Head Neck Surg. = Le J. D’oto-Rhino-Laryngol. Et De Chir. Cervico-Faciale 2016, 45, 43. [Google Scholar] [CrossRef] [Green Version]
- Maurer, J.T.; Van de Heyning, P.; Lin, H.S.; Baskin, J.; Anders, C.; Hohenhorst, W.; Woodson, B.T. Operative technique of upper airway stimulation: An implantable treatment of obstructive sleep apnea. Oper. Tech. Otolaryngol. Head Neck Surg. 2012, 23, 227–233. [Google Scholar] [CrossRef]
- Kezirian, E.J.; Boudewyns, A.; Eisele, D.W.; Schwartz, A.R.; Smith, P.L.; Van de Heyning, P.H.; De Backer, W.A. Electrical stimulation of the hypoglossal nerve in the treatment of obstructive sleep apnea. Sleep Med Rev. 2010, 14, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Lorenzi-Filho, G.; Almeida, F.R.; Strollo, P.J. Treating OSA: Current and emerging therapies beyond CPAP. Respirology 2017, 22, 1500–1507. [Google Scholar] [CrossRef] [Green Version]
- Rangel-León, Y.J.; Rengifo-Varona, M.L.; Gálvis-Gómez, A.M.; Sarmiento-González, M.C.; Giraldo-Cadavid, L.F. Rehabilitation of oropharyngeal muscles with exercises and electrotherapy for obstructive sleep apnea-hypopnea syndrome. Rehabilitation 2015, 49, 4–9. [Google Scholar]
- Steier, J.; Seymour, J.; Rafferty, G.F.; Jolley, C.J.; Solomon, E.; Luo, Y.; Man, W.D.-C.; Polkey, M.I.; Moxham, J. Continuous Transcutaneous Submental Electrical Stimulation in Obstructive Sleep Apnea: A Feasibility Study. Chest 2011, 140, 998–1007. [Google Scholar] [CrossRef] [PubMed]
- Pengo, M.F.; Steier, J. Emerging technology: Electrical stimulation in obstructive sleep apnoea. J. Thorac. Dis. 2015, 7, 1286–1297. [Google Scholar]
- De Lucas Ramos, L.; Rodríguez, J.M.; De Miguel Diez, J. Sleep-disordered breathing. Neumomadrid Monographs. 2004, VI, 45–57. [Google Scholar]
- Wessolleck, E.; Bernd, E.; Dockter, S.; Lang, S.; Sama, A.; Stuck, B.A. Intraoral electrical muscle stimulation in the treatment of snoring. Somnologie 2018, 22 (Suppl. S2), 47–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ratneswaran, D.; Guni, A.; Pengo, M.F.; Al-Sherif, M.; He, B.; Cheng, M.C.; Steier, J.; Schwarz, E.I. Electrical stimulation as a therapeutic approach in obstructive sleep apnea—A meta-analysis. Sleep Breath. Int. J. Sci. Pract. Sleep Med. 2021, 25, 207–218. [Google Scholar] [CrossRef]
- Berry, R.B.; Brooks, R.; Gamaldo, C.E.; Harding, S.M.; Lloyd, R.M.; Quan, S.F.; Troester, M.T.; Vaughn, B.V. For the American Academy of Sleep Medicine. In The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications; American Academy of Sleep Medicine: Downers Grove Township, IL, USA, 2016; Version 2.3. [Google Scholar]
- Kapur, V.K.; Auckley, D.H.; Chowdhuri, S.; Kuhlmann, D.C.; Mehra, R.; Ramar, K.; Harrod, C.G. Clinical Practice Guideline for Diagnostic Testing for Adult Obstructive Sleep Apnea: An American Academy of Sleep Medicine Clinical Practice Guideline. J. Clin. Sleep Med. 2017, 13, 479–504. [Google Scholar] [CrossRef]
- Oshana, R. DSP Software Development Techniques for Embedded and Real-Time Systems. Chapter 4–Overview of Digital Signal Processing Algorithms; Elsevier: Amsterdam, The Netherlands, 2006; pp. 59–121. [Google Scholar]
- Hussin, S.; Sudirman, R. Sensory Response through EEG Interpretation on Alpha Wave and Power Spectrum. Malays. Tech. Univ. Conf. Eng. Technol. 2013, 53, 288–293. [Google Scholar] [CrossRef] [Green Version]
- Okura, K.; Kato, T.; Montplaisir, J.Y.; Sessle, B.J.; Lavigne, G.J. Quantitative analysis of surface EMG activity of cranial and leg muscles across sleep stages in human. Clin. Neurophysiol. 2006, 117, 269–278. [Google Scholar] [CrossRef] [PubMed]
- Sugi, T.; Kawana, F.; Nakamura, M. Automatic EEG arousal detection for sleep apnea syndrome. Biomed. Signal Process. Control 2009, 4, 329–337. [Google Scholar] [CrossRef]
- Dumont, M.; Jurysta, F.; Lanquart, J.; Noseda, A.; Van de Borne, P.; Linkowski, P. Scale-free dynamics of the synchronization between sleep EEG power bands and the high frequency component of heart rate variability in normal men and patients with sleep apnea–hypopnea syndrome. Clin. Neurophysiol. 2007, 118, 2752–2764. [Google Scholar] [CrossRef]
- Imtiaz, S.A.; Rodriguez-Villegas, E. A Low Computational Cost Algorithm for REM Sleep Detection Using Single Channel EEG. Ann. Biomed. Eng. 2014, 42, 2344–2359. [Google Scholar] [CrossRef] [Green Version]
- Aboalayon, K.A.; Ocbagabir, H.T.; Faezipour, M. Efficient sleep stage classification based on EEG signals. In Proceedings of the IEEE Long Island Systems, Applications and Technology (LISAT) Conference 2014, Farmingdale, NY, USA, 2 May 2014. [Google Scholar]
- Wei, R.; Zhang, X.; Wang, J.; Dang, X. The research of sleep staging based on single-lead electrocardiogram and deep neural network. Biomed. Eng. Lett. 2017, 8, 87–93. [Google Scholar] [CrossRef]
- Lucey, B.P.; Mcleland, J.S.; Toedebusch, C.D.; Boyd, J.; Morris, J.C.; Landsness, E.C.; Yamada, K.; Holtzman, D.M. Comparison of a single-channel EEG sleep study to polysomnography. J. Sleep Res. 2016, 25, 625–635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Imtiaz, S.A.; Jiang, Z.; Rodriguez-Villegas, E. An Ultralow Power System on Chip for Automatic Sleep Staging. IEEE J. Solid-State Circuits 2017, 52, 822–833. [Google Scholar] [CrossRef]
- Shen, H.; Xu, M.; Guez, A.; Li, A.; Ran, F. An accurate sleep stages classification method based on state space model. IEEE Access 2019, 7, 125268–125279. [Google Scholar] [CrossRef]
- Nakamura, T.; Alqurashi, Y.D.; Morrell, M.J.; Mandic, D.P. Hearables: Automatic Overnight Sleep Monitoring with Standardized In-Ear EEG Sensor. IEEE Trans. Biomed. Eng. 2020, 67, 203–212. [Google Scholar] [CrossRef] [Green Version]
- Da Silveira, T.; Kozakevicius, A.; Rodrigues, C. Single-channel EEG sleep stage classification based on a streamlined set of statistical features in wavelet domain. Med. Biol. Eng. Comput. 2017, 55, 343–352. [Google Scholar] [CrossRef]
- Abou Jaoude, M.; Sun, H.; Pellerin, K.R.; Pavlova, M.; Sarkis, R.A.; Cash, S.S.; Westover, M.B.; Lam, A.D. Expert-level automated sleep staging of long-term scalp electroencephalography recordings using deep learning. Sleep 2020, 43, zsaa112. [Google Scholar] [CrossRef]
- Chang, S.; Wu, B.; Liou, Y.; Zheng, R.; Lee, P.; Chiueh, T.; Liu, T. An Ultra-Low-Power Dual-Mode Automatic Sleep Staging Processor Using Neural-Network-Based Decision Tree. IEEE Trans. Circuits Syst. I Regul. Pap. 2019, 66, 3504–3516. [Google Scholar] [CrossRef]
- Imtiaz, S.A. A Systematic Review of Sensing Technologies for Wearable Sleep Staging. Sensors 2021, 21, 1562. [Google Scholar] [CrossRef]
- Burgos, A.; Gõni, A.; Illarramendi, A.; Bermúdez, J. Real-time detection of apneas on a PDA. IEEE Trans. Inf. Technol. Biomed. 2010, 14, 995–1002. [Google Scholar] [CrossRef] [PubMed]
- Garde, A.; Dehkordi, P.; Wensley, D.; Ansermino, J.; Dumont, G. Pulse oximetry recorded from the phone oximeter for detection of obstructive sleep apnea events with and without oxygen desaturation in children. In Proceedings of the 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Milano, Italy, 25–29 August 2015. [Google Scholar]
- Mendonça, F.; Mostafa, S.S.; Ravelo-García, A.G.; Morgado-Dias, F.; Penzel, T. Devices for home detection of obstructive sleep apnea: A review. Sleep Med. Rev. 2018, 41, 149–160. [Google Scholar] [CrossRef]
- Sharma, M.; Kumbhani, D.; Tiwari, J.; Kumar, T.S.; Acharya, U.R. Automated detection of obstructive sleep apnea in more than 8000 subjects using frequency optimized orthogonal wavelet filter bank with respiratory and oximetry signals. Comput. Biol. Med. 2022, 144, 105364. [Google Scholar] [CrossRef]
- Koley, B.L.; Dey, D. Automatic detection of sleep apnea and hypopnea events from single channel measurement of respiration signal employing ensemble binary SVM classifiers. Measurement 2013, 46, 2082–2092. [Google Scholar] [CrossRef]
- Moscoso-Barrera, W.D.; Carreño-Pérez, I.S.; Agudelo-Otalora, L.M.; Giraldo-Cadavid, L.F.; Burguete, J. Design of an electronic device for the measurement of respiratory signals. In Proceedings of the 2021 4th International Conference on Bio-Engineering for Smart Technologies (BioSMART), Paris, France, 8–10 December 2021; pp. 1–5. [Google Scholar] [CrossRef]
- Tsouti, V.; Kanaris, A.I.; Tsoutis, K.; Chatzandroulis, S. Development of an automated system for obstructive sleep apnea treatment based on machine learning and breath effort monitoring. Microelectron. Eng. 2020, 231, 111376. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Real (Expert) | ||||
|---|---|---|---|---|
| Awake | Sleep | |||
| Algorithm | Awake | 292 | 70 | 362 |
| Sleep | 58 | 802 | 860 | |
| 350 | 872 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moscoso-Barrera, W.D.; Urrestarazu, E.; Alegre, M.; Horrillo-Maysonnial, A.; Urrea, L.F.; Agudelo-Otalora, L.M.; Giraldo-Cadavid, L.F.; Fernández, S.; Burguete, J. Simple and Autonomous Sleep Signal Processing System for the Detection of Obstructive Sleep Apneas. Int. J. Environ. Res. Public Health 2022, 19, 6934. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19116934
Moscoso-Barrera WD, Urrestarazu E, Alegre M, Horrillo-Maysonnial A, Urrea LF, Agudelo-Otalora LM, Giraldo-Cadavid LF, Fernández S, Burguete J. Simple and Autonomous Sleep Signal Processing System for the Detection of Obstructive Sleep Apneas. International Journal of Environmental Research and Public Health. 2022; 19(11):6934. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19116934
Chicago/Turabian StyleMoscoso-Barrera, William D., Elena Urrestarazu, Manuel Alegre, Alejandro Horrillo-Maysonnial, Luis Fernando Urrea, Luis Mauricio Agudelo-Otalora, Luis F. Giraldo-Cadavid, Secundino Fernández, and Javier Burguete. 2022. "Simple and Autonomous Sleep Signal Processing System for the Detection of Obstructive Sleep Apneas" International Journal of Environmental Research and Public Health 19, no. 11: 6934. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19116934