
Risk and Protective Factors Experienced by Fathers of Refugee Background during the Early Years of Parenting: A Qualitative Study

 ,
, {kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Population and Recruitment
2.3. Data Collection
2.4. Data Analysis
2.5. Ethics
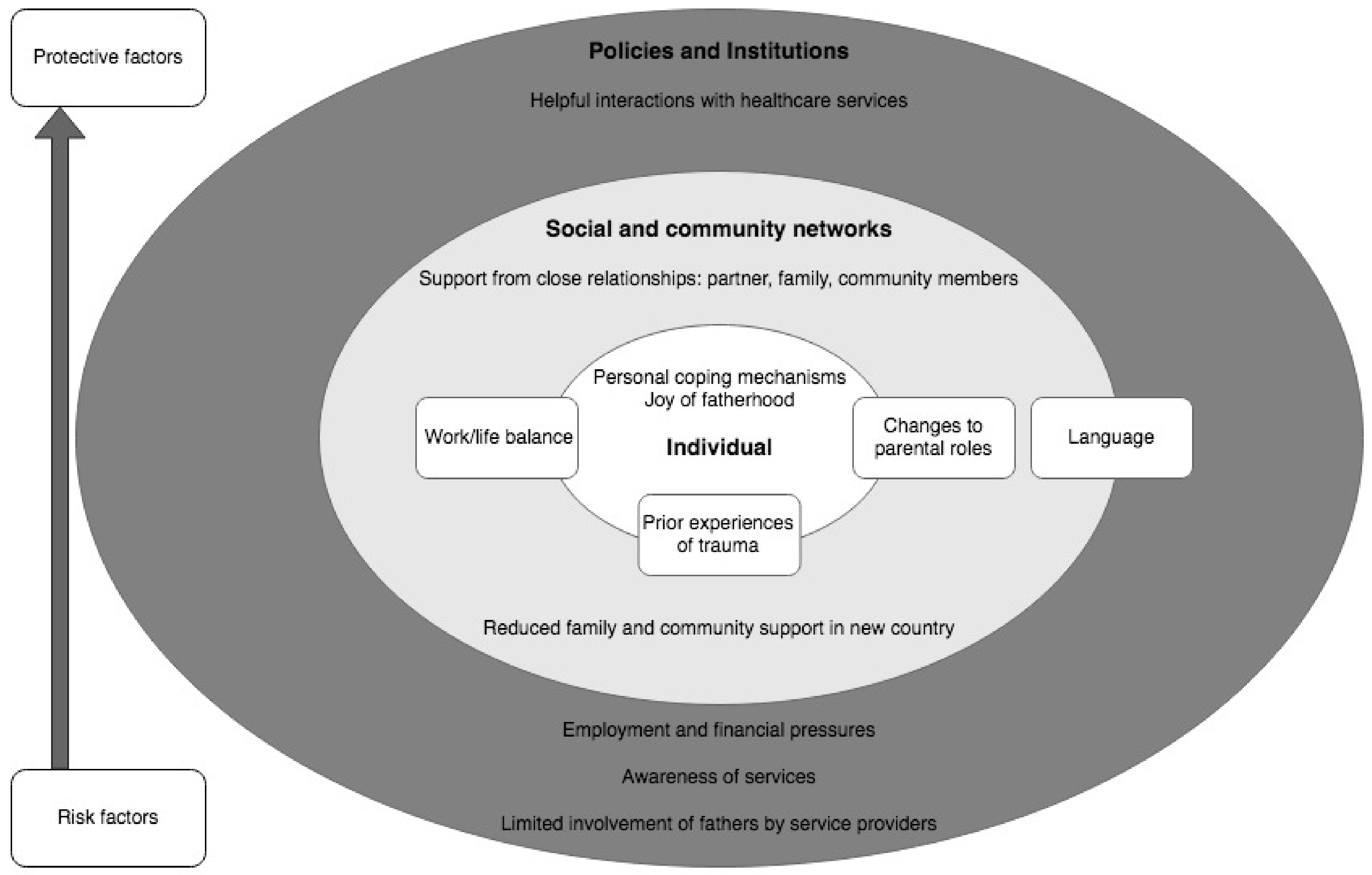
3. Results
3.1. Individual Factors
3.1.1. Joy of Fatherhood
“What I love about it, I think just the beauty of spending time with my son and hearing what he says. The person that he is, and as a two-year-old he’s got his own character, his own personality.”Afghan father.
“And, sometimes when you stressful, you worry, you come home and you play with the children, all the stress is gone. It’s like a medicine, you know? It works.”Afghan father.
3.1.2. Work/Life Balance
“… as fathers, we have a lot of obligations. We have to take our children and our wives to the appointment, to the doctors, to schools. We don’t have that time, enough time to go to school and learn the language”Assyrian father.
“As a refugee, if you want to be successful, you really need to compensate for the things that you’ve lost. So, the few years that I spent in detention and the time that I lost in Afghanistan as I couldn’t continue with my education, and then first four or five years of life here, I had to work in factory jobs to keep up supporting a big family back at home and also myself here. So, with all of those, I had to work really hard.”Afghan father.
“I could see that a lot of the Afghani fathers, especially coming from asylum seeker, refugee backgrounds, had issues… a lot of them would focus so much to get financially by that they would work, you know, 60 h, and wouldn’t be there for the kids. And, I think I really could see the need for services to communicate to these people that, you know, your ultimate goal is a better future for your children, isn’t that? And, they would be, “Yes. Absolutely.” “And, how do you see achieving that, is by working 60 h?”Afghan father.
3.1.3. Personal Coping Mechanisms
“If I notice, for instance, that becoming somehow depressed about something, one way is to take my book, play my music—I’ve got some very special songs.”Sierra Leonean father.
3.1.4. Prior Experiences of Trauma
“As a father in the camp in Burma, we have a lot of trauma experience and hardship going through in our life. It’s good not to share our trauma and hardship to the children because the children grow up in this country, better grow in the future…although we have very painful experience, we better not show the children about our painful experience, only encourage the children for the better future.”Karen father.
3.1.5. Changes to Parental Roles
“I can say it’s shame in Syria as a dad to take care of a child, changing her or him…the nappies, yeah… but here, I can see that there’s no difference or it’s okay for the dad to take care of the baby.”Assyrian father.
“It’s good in the new country, you can better learn the new way of nurturing the children, because you can’t do it all in the traditional way because the children grew up in a new environment, so the father needs to learn the new way.”Karen father.
3.2. Social and Community Network Factors
3.2.1. Support from Close Relationships: Partner, Family, Community Members
“After having the first child the relationship is strengthened more and more. Everything—I think it’s love is increased and we link to each other more and our relationship is turned to like iron relationship.”Assyrian father.
“Especially with the kids, when the kids have some issue, we ask our parents, especially my mum, yeah, we have this situation, how to cope with this one, what to do.”Afghan father.
“It is helpful because I think every parent has its own sort of experience…when you do talk with them, also it’s a good opportunity for exchange experience, perhaps the way they do things, the way they solve the problem, I think it’s good to have that sort of conversation.”Afghan father.
“This is how it works here, because if it comes from us that have lived here for long, telling our African brothers, they would tend to believe us more. Because, we have gone through and we should be able to share our experiences with them.”Sierra Leonean father.
“So, for example, there are sometimes I might not tell them details about how I manage something, you know, some difficulty. Because, I just feel vulnerable in some ways, you know? I don’t want to be judged too much.”Afghan father.
3.2.2. Reduced Family and Community Support in New Country
“From my experience, becoming a parent for the very first time in the western world, it’s very hard, compared to in Africa. In Africa you have so many help.”Sierra Leonean father.
3.3. Policy and Institutional Level Factors
3.3.1. Employment and Financial Pressures
“Basically, as the father, I feel the pressure of… I need to make sure that we are financially okay.”Afghan father.
“Yeah, it’s very stressful looking for the job, because of the language problem and also—don’t know how to use the online job applications and online sites”Karen father.
3.3.2. Language
“Without having language it’s very difficult to find a job and to find employment. We feel that they pressure, pressuring…It’s during a small period of time and they’re asking us to find a job. We are not able just to say ‘Hi’ in English. How can we find a job without having this language?”Assyrian father.
“If you can’t communicate, you cannot appropriately address your needs… main barrier would be language, otherwise if you know the language, then you know about the services available.”Afghan father.
“For the first appointment I did not have an interpreter. But I asked for the telephone interpreter. And, then the next follow up appointment no interpreter. So I accompany with a friend or relative to go interpreter for me.”Karen father.
3.3.3. Awareness of Services
“The other family told us that when we talked about a stressful time, and they told, “Why you didn’t use this service?” And we told that we didn’t know about that one.”Afghan father.
3.3.4. Helpful Interactions with Healthcare Services
“Thanks to our new home, Australia, because we have one of the best health systems in the world. I’m very proud of that. And we did get good advice from our doctors and GPs.”Afghan father.
3.3.5. Limited Involvement of Fathers by Service Providers
“…most times I’ll be there just observing. They’ll be talking. Actually, they’ll mostly be asking my wife questions, she’ll be answering, and I’ll be just there.”Sierra Leonean father.
“They weigh the baby and they check some movements and that’s all basically about it…I think this maternal child health should be more than a GP role to see the wellbeing of the mother, wellbeing of the baby, and the whole family—the father, mother, parents and the baby”Tamil father.
4. Discussion
4.1. Strengths and Limitations
4.2. Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Black, M.M.; Walker, S.P.; Fernald, L.C.; Andersen, C.T.; DiGirolamo, A.M.; Lu, C.; McCoy, D.C.; Fink, G.; Shawar, Y.R.; Shiffman, J.; et al. Early childhood development coming of age: Science through the life course. Lancet 2017, 389, 77–90. [Google Scholar] [CrossRef] [Green Version]
- Britto, P.R.; Lye, S.J.; Proulx, K.; Yousafzai, A.K.; Matthews, S.G.; Vaivada, T.; Perez-Escamilla, R.; Rao, N.; Ip, P.; Fernald, L.C.H.; et al. Nurturing care: Promoting early childhood development. Lancet 2017, 389, 91–102. [Google Scholar] [CrossRef] [Green Version]
- Leach, L.S.; Poyser, C.; Cooklin, A.R.; Giallo, R. Prevalence and course of anxiety disorders (and symptom levels) in men across the perinatal period: A systematic review. J. Affect. Disord. 2016, 190, 675–686. [Google Scholar] [CrossRef]
- Garfield, C.F.; Duncan, G.; Rutsohn, J.; McDade, T.W.; Adam, E.K.; Coley, R.L.; Chase-Lansdale, P.L. A longitudinal study of paternal mental health during transition to fatherhood as young adults. Pediatrics 2014, 133, 836–843. [Google Scholar] [CrossRef] [Green Version]
- Paulson, J.F.; Bazemore, S.D. Prenatal and postpartum depression in fathers and its association with maternal depression: A meta-analysis. JAMA 2010, 303, 1961–1969. [Google Scholar] [CrossRef] [PubMed]
- Giallo, R.; D’Esposito, F.; Christensen, D.; Mensah, F.; Cooklin, A.; Wade, C.; Lucas, N.; Canterford, L.; Nicholson, J. Father mental health during the early parenting period: Results of an Australian population based longitudinal study. Soc. Psychiatry Psychiatr. Epidemiol. 2012, 47, 1907–1916. [Google Scholar] [CrossRef] [PubMed]
- Ramchandani, P.; Stein, A.; Evans, J.; O’Connor, T.G.; Team, A.S. Paternal depression in the postnatal period and child development: A prospective population study. Lancet 2005, 365, 2201–2205. [Google Scholar] [CrossRef]
- Mensah, F.K.; Kiernan, K.E. Parents’ mental health and children’s cognitive and social development. Soc. Psychiatry Psychiatr. Epidemiol. 2010, 45, 1023–1035. [Google Scholar] [CrossRef] [PubMed]
- Allotey, P.; Reidpath, D. The Health of Refugees: Public Health Perspectives from Crisis to Settlement; Oxford University Press: Oxford, UK, 2018. [Google Scholar]
- Akesson, B.; Sousa, C. Parental suffering and resilience among recently displaced Syrian refugees in Lebanon. J. Child Fam. Stud. 2020, 29, 1264–1273. [Google Scholar] [CrossRef]
- Berry, J.W. Acculturation: Living successfully in two cultures. Int. J. Intercult. Relat. 2005, 29, 697–712. [Google Scholar] [CrossRef]
- Milner, K.; Khawaja, N.G. Sudanese refugees in Australia: The impact of acculturation stress. J. Pac. Rim Psychol. 2010, 4, 19–29. [Google Scholar] [CrossRef] [Green Version]
- Lindert, J.; von Ehrenstein, O.S.; Priebe, S.; Mielck, A.; Brähler, E. Depression and anxiety in labor migrants and refugees—A systematic review and meta-analysis. Soc. Sci. Med. 2009, 69, 246–257. [Google Scholar] [CrossRef]
- Porter, M.; Haslam, N. Predisplacement and postdisplacement factors associated with mental health of refugees and internally displaced persons: A meta-analysis. JAMA 2005, 294, 602–612. [Google Scholar] [CrossRef]
- Schweitzer, R.D.; Brough, M.; Vromans, L.; Asic-Kobe, M. Mental health of newly arrived Burmese refugees in Australia: Contributions of pre-migration and post-migration experience. Aust. N. Z. J. Psychiatry 2011, 45, 299–307. [Google Scholar] [CrossRef] [Green Version]
- Hamrah, M.S.; Hoang, H.; Mond, J.; Pahlavanzade, B.; Charkazi, A.; Auckland, S. The prevalence and correlates of symptoms of post-traumatic stress disorder (PTSD) among resettled Afghan refugees in a regional area of Australia. J. Ment. Health 2020, 30, 674–680. [Google Scholar] [CrossRef]
- Shawyer, F.; Enticott, J.C.; Block, A.A.; Cheng, I.-H.; Meadows, G.N. The mental health status of refugees and asylum seekers attending a refugee health clinic including comparisons with a matched sample of Australian-born residents. BMC Psychiatry 2017, 17, 76. [Google Scholar] [CrossRef] [Green Version]
- Vaage, A.B.; Thomsen, P.H.; Silove, D.; Wentzel-Larsen, T.; Van Ta, T.; Hauff, E. Long-term mental health of Vietnamese refugees in the aftermath of trauma. Br. J. Psychiatry 2010, 196, 122–125. [Google Scholar] [CrossRef]
- Giallo, R.; Riggs, E.; Lynch, C.; Vanpraag, D.; Yelland, J.; Szwarc, J.; Duell-Piening, P.; Tyrell, L.; Casey, S.; Brown, S.J. The physical and mental health problems of refugee and migrant fathers: Findings from an Australian population-based study of children and their families. BMJ Open 2017, 7, e015603. [Google Scholar] [CrossRef] [PubMed]
- Scharpf, F.; Kyaruzi, E.; Landolt, M.A.; Hecker, T. Prevalence and co-existence of morbidity of posttraumatic stress and functional impairment among Burundian refugee children and their parents. Eur. J. Psychotraumatol. 2019, 10, 1676005. [Google Scholar] [CrossRef] [Green Version]
- Vaage, A.B.; Thomsen, P.H.; Rousseau, C.; Wentzel-Larsen, T.; Ta, T.V.; Hauff, E. Paternal predictors of the mental health of children of Vietnamese refugees. Child Adolesc. Psychiatry Ment. Health 2011, 5, 2. [Google Scholar] [CrossRef] [Green Version]
- Van Ee, E.; Sleijpen, M.; Kleber, R.J.; Jongmans, M.J. Father-involvement in a refugee sample: Relations between posttraumatic stress and caregiving. Fam. Process 2013, 52, 723–735. [Google Scholar] [CrossRef] [PubMed]
- Javanbakht, A.; Rosenberg, D.; Haddad, L.; Arfken, C.L. Mental Health in Syrian refugee children resettling in the United States: War trauma, migration, and the role of parental stress. J. Am. Acad. Child Adolesc. Psychiatry 2018, 57, 209–211. [Google Scholar] [CrossRef] [PubMed]
- Bryant, R.A.; Edwards, B.; Creamer, M.; O’Donnell, M.; Forbes, D.; Felmingham, K.L.; Silove, D.; Steel, Z.; Nickerson, A.; McFarlane, A.C.; et al. The effect of post-traumatic stress disorder on refugees’ parenting and their children’s mental health: A cohort study. Lancet Public Health 2018, 3, e249–e258. [Google Scholar] [CrossRef] [Green Version]
- Riggs, E.; Yelland, J.; Szwarc, J.; Wahidi, S.; Casey, S.; Chesters, D.; Fouladi, F.; Duell-Piening, P.; Giallo, R.; Brown, S.; et al. Fatherhood in a new country: A qualitative study exploring the experiences of Afghan men and implications for health services. Birth 2016, 43, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Forget, G.; Correa-Velez, I.; Dee, M. Being a father in my new society: A qualitative study of the fathering experiences of men from refugee backgrounds resettled in Australia. J. Refug. Stud. 2019, 32, 322–339. [Google Scholar] [CrossRef] [Green Version]
- Este, D.C.; Tachble, A. Fatherhood in the Canadian context: Perceptions and experiences of Sudanese refugee men. Sex Roles 2009, 60, 456–466. [Google Scholar] [CrossRef]
- Stewart, M.; Dennis, C.-L.; Kariwo, M.; Kushner, K.E.; Letourneau, N.; Makumbe, K.; Makwarimba, E.; Shizha, E. Challenges faced by refugee new parents from Africa in Canada. J. Immigr. Minority Health 2015, 17, 1146–1156. [Google Scholar] [CrossRef]
- Mangrio, E.; Carlson, E.; Zdravkovic, S. Newly arrived refugee parents in Sweden and their experience of the resettlement process: A qualitative study. Scand. J. Public Health 2020, 48, 699–706. [Google Scholar] [CrossRef] [PubMed]
- Merry, L.; Pelaez, S.; Edwards, N.C. Refugees, asylum-seekers and undocumented migrants and the experience of parenthood: A synthesis of the qualitative literature. Glob. Health 2017, 13, 75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bronfenbrenner, U. Toward an experimental ecology of human development. Am. Psychol. 1977, 32, 513. [Google Scholar] [CrossRef]
- Göran, D.; Whitehead, M. Policies and strategies to promote social equity in health. In Background Document to WHO-Strategy Paper for Europe; Institute for Futures Studies: Stockholm, Sweden, 1991. [Google Scholar]
- The Victorian Foundation for Survivors of Torture Inc. Foundation House: About Us. 2020. Available online: https://foundationhouse.org.au/about-us/ (accessed on 1 April 2022).
- Riggs, E.; Yelland, J.; Szwarc, J.; Casey, S.; Chesters, D.; Duell-Piening, P.; Wahidi, S.; Fouladi, F.; Brown, S. Promoting the inclusion of Afghan women and men in research: Reflections from research and community partners involved in implementing a ‘proof of concept’ project. Int. J. Equity Health 2015, 14, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- QSR International. NVivo Qualitative Data Analysis Software, Version 12; QSR International Pty Ltd.: Melbourne, Australia, 2018. [Google Scholar]
- Green, J.; Willis, K.; Hughes, E.; Small, R.; Welch, N.; Gibbs, L.; Daly, J. Generating best evidence from qualitative research: The role of data analysis. Aust. N. Z. J. Public Health 2007, 31, 545–550. [Google Scholar] [CrossRef]
- Liamputtong, P. Moral and ethical perspectives. In Performing Qualitative Cross-Cultural Research; Cambridge University Press: Cambridge, UK, 2010; pp. 31–57. [Google Scholar]
- Correa-Velez, I.; Barnett, A.G.; Gifford, S. Working for a better life: Longitudinal evidence on the predictors of employment among recently arrived refugee migrant men living in Australia. Int. Migr. 2015, 53, 321–337. [Google Scholar] [CrossRef] [Green Version]
- Poppitt, G.; Frey, R. Sudanese adolescent refugees: Acculturation and acculturative stress. J. Psychol. Couns. Sch. 2007, 17, 160–181. [Google Scholar] [CrossRef]
- Magruder, K.M.; McLaughlin, K.A.; Elmore Borbon, D.L. Trauma is a public health issue. Eur. J. Psychotraumatol. 2017, 8, 1375338. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, I. Rebuilding Shattered Lives—Integrated Trauma Recovery for People of Refugee Background; The Victorian Foundation for Survivors of Torture Inc.: Brunswick, Australia, 2020. [Google Scholar]
- Substance Abuse and Mental Health Services Administration. SAMHSA’s Concept of Trauma and Guidance for a Trauma-Informed Approach; Report no.: SMA14-4884; Substance Abuse and Mental Health Services Administration: Rockville, MD, USA, 2014.
- Hopper, E.K.; Bassuk, E.L.; Olivet, J. Shelter from the storm: Trauma-informed care in homelessness services settings. Open Health Serv. Policy J. 2010, 3, 80–100. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bulford, E.; Fogarty, A.; Giallo, R.; Brown, S.; Szwarc, J.; Riggs, E. Risk and Protective Factors Experienced by Fathers of Refugee Background during the Early Years of Parenting: A Qualitative Study. Int. J. Environ. Res. Public Health 2022, 19, 6940. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19116940
Bulford E, Fogarty A, Giallo R, Brown S, Szwarc J, Riggs E. Risk and Protective Factors Experienced by Fathers of Refugee Background during the Early Years of Parenting: A Qualitative Study. International Journal of Environmental Research and Public Health. 2022; 19(11):6940. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19116940
Chicago/Turabian StyleBulford, Eleanor, Alison Fogarty, Rebecca Giallo, Stephanie Brown, Josef Szwarc, and Elisha Riggs. 2022. "Risk and Protective Factors Experienced by Fathers of Refugee Background during the Early Years of Parenting: A Qualitative Study" International Journal of Environmental Research and Public Health 19, no. 11: 6940. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19116940