
Israeli Medical Experts’ Knowledge, Attitudes, and Preferences in Allocating Donor Organs for Transplantation


Abstract
:1. Introduction
1.1. Public Preferences regarding Organ Allocation
1.2. Health Care Professionals’ Preferences regarding Organ Allocation
2. Materials and Methods
2.1. Study Design
2.2. Participants and Eligible Criteria
2.3. Interview and Questionnaire
2.4. Statistical Analysis
3. Results
3.1. Demographic Distribution and Organ Donation Status
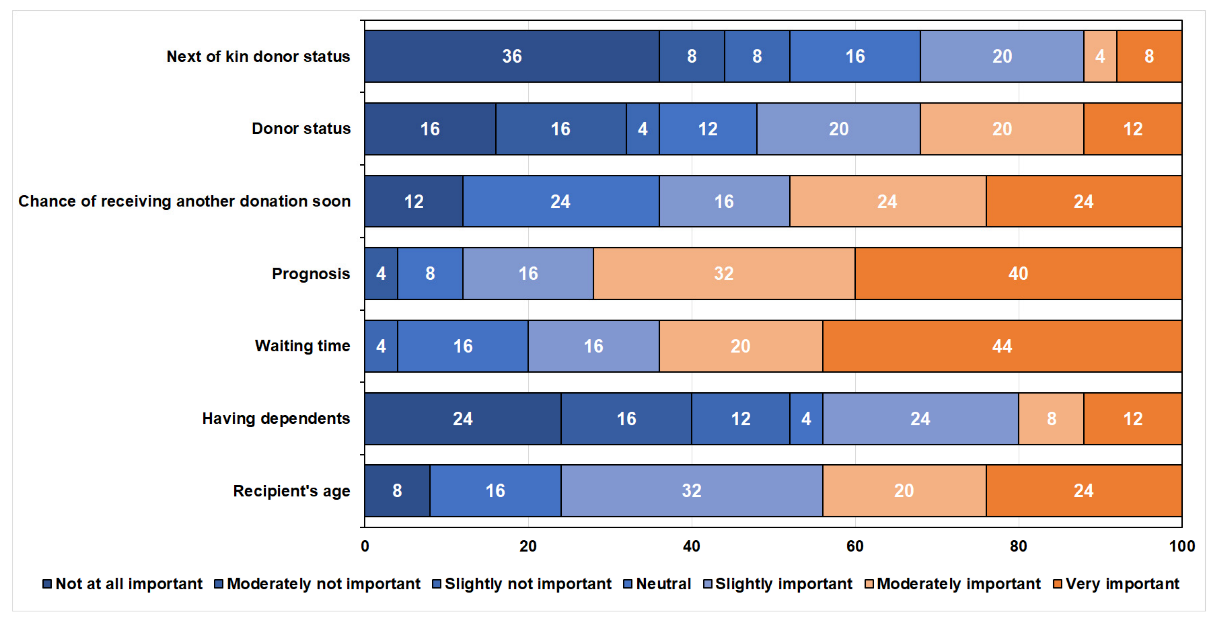
3.2. Declared Preferences for Organ Allocation Criteria
3.3. Experts’ Hypothesis about the General Public Preferences
3.4. Comparison among Experts’ Preferences, Public Preferences, and Declared Preferences
3.5. Willingness to Be an Organ Donor
4. Discussion
5. Limitations and Future-Prospects
6. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Grinyó, J.M. Why Is Organ Transplantation Clinically Important? Cold Spring Harb. Perspect. Med. 2013, 3, 485–496. [Google Scholar] [CrossRef] [Green Version]
- Organ Donation Statistics Organ Donation Statistics. Available online: https://www.organdonor.gov/learn/organ-donation-statistics (accessed on 5 October 2021).
- Elalouf, A. Immune response against the biomaterials used in 3D bioprinting of organs. Transpl. Immunol. 2021, 69, 101446. [Google Scholar] [CrossRef] [PubMed]
- Wu, D.A.; Watson, C.J.; Bradley, J.A.; Johnson, R.J.; Forsythe, J.L.; Oniscu, G.C. Global trends and challenges in deceased donor kidney allocation. Kidney Int. 2017, 91, 1287–1299. [Google Scholar] [CrossRef] [Green Version]
- Freeman, R.B.; Matas, A.T.; Henry, M.; Segev, D.L.; Kaufman, D.B.; Roberts, J.P. Moving kidney allocation forward: The ASTS perspective. Am. J. Transplant. 2009, 9, 1501–1506. [Google Scholar] [CrossRef] [PubMed]
- Stegall, M.D. Developing a new kidney allocation policy: The rationale for including life years from transplant: Personal viewpoint. Am. J. Transplant. 2009, 9, 1528–1532. [Google Scholar] [CrossRef]
- Robinson, C. POLICY POL200/4.1—Introduction to Patient Selection and Organ Allocation Policies; NHSBT: Bristol, UK, 2018; pp. 1–23. [Google Scholar]
- Leichtman, A.B.; McCullough, K.P.; Wolfe, R.A. Improving the Allocation System for Deceased-Donor Kidneys. N. Engl. J. Med. 2011, 364, 1287–1289. [Google Scholar] [CrossRef]
- Taherkhani, N.; Sepehri, M.M.; Shafaghi, S.; Khatibi, T. Identification and weighting of kidney allocation criteria: A novel multi-expert fuzzy method. BMC Med. Inform. Decis. Mak. 2019, 19, 182. [Google Scholar] [CrossRef] [Green Version]
- Ashkenazi, T.; Lavee, J.; Mor, E. Organ donation in Israel-Achievements and challenges. Transplantation 2015, 99, 265–266. [Google Scholar] [CrossRef]
- David, I.; Yechiali, U. Sequential assignment match processes with arrivals of candidates and offers. Probab. Eng. Inf. Sci. 1990, 4, 413–430. [Google Scholar] [CrossRef]
- Yuan, Y.; Feldhamer, S.; Gafni, A.; Fyfe, F.; Ludwin, D. An internet-based fuzzy logic expert system for organ transplantation assignment. Int. J. Healthc. Technol. Manag. 2001, 3, 386–405. [Google Scholar] [CrossRef]
- Gundogar, E.; Duran, F.M.; Canbolat, Y.B.; Turkmen, A. Fuzzy organ allocation system for cadaveric kidney transplantation. Transplantation 2005, 80, 1648–1653. [Google Scholar] [CrossRef]
- Baskin-Bey, E.S.; Nyberg, S.L. Matching graft to recipient by predicted survival: Can this be an acceptable strategy to improve utilization of deceased donor kidneys? Transplant. Rev. 2008, 22, 167–170. [Google Scholar] [CrossRef]
- Cruz-Ramírez, M.; Hervás-Martínez, C.; Fernández, J.C.; Briceño, J.; de la Mata, M. Predicting patient survival after liver transplantation using evolutionary multi-objective artificial neural networks. Artif. Intell. Med. 2013, 58, 37–49. [Google Scholar] [CrossRef] [PubMed]
- Bertsimas, D.; Farias, V.F.; Trichakis, N. Fairness, efficiency, and flexibility in organ allocation for kidney transplantation. Oper. Res. 2013, 61, 73–87. [Google Scholar] [CrossRef] [Green Version]
- Al-Ebbini, L.; Oztekin, A.; Chen, Y. FLAS: Fuzzy lung allocation system for US-based transplantations. Eur. J. Oper. Res. 2016, 248, 1051–1065. [Google Scholar] [CrossRef]
- Ahmadvand, S.; Pishvaee, M.S. An efficient method for kidney allocation problem: A credibility-based fuzzy common weights data envelopment analysis approach. Health Care Manag. Sci. 2018, 21, 587–603. [Google Scholar] [CrossRef]
- Tavana, M.; Zareinejad, M.; Di Caprio, D.; Kaviani, M.A. An integrated intuitionistic fuzzy AHP and SWOT method for outsourcing reverse logistics. Appl. Soft Comput. J. 2016, 40, 544–557. [Google Scholar] [CrossRef]
- Singh, A.; Prasher, A. Measuring healthcare service quality from patients’ perspective: Using Fuzzy AHP application. Total Qual. Manag. Bus. Excell. 2019, 30, 284–300. [Google Scholar] [CrossRef]
- Huang, Y.P.; Basanta, H.; Kuo, H.C.; Huang, A. Health symptom checking system for elderly people using fuzzy analytic hierarchy process. Appl. Syst. Innov. 2018, 1, 10. [Google Scholar] [CrossRef] [Green Version]
- Saha, C.; Zhang, J.; Yoon, S.W.; Khasawneh, M.T.; Srihari, K. Selection and matching of kidney donor and recipient using fuzzy techniques and analytic hierarchy process. In Proceedings of the 62nd IIE Annual Conference and Expo 2012, Orlando, FL, USA, 19–23 May 2012; pp. 2834–2843. [Google Scholar]
- Tong, A.; Jan, S.; Wong, G.; Craig, J.C.; Irving, M.; Chadban, S.; Cass, A.; Howard, K. Rationing scarce organs for transplantation: Healthcare provider perspectives on waitlisting and organ allocation. Clin. Transplant. 2013, 27, 60–71. [Google Scholar] [CrossRef] [PubMed]
- Tong, A.; Hanson, C.S.; Chapman, J.R.; Halleck, F.; Budde, K.; Papachristou, C.; Craig, J.C. The preferences and perspectives of nephrologists on patients’ access to kidney transplantation: A systematic review. Transplantation 2014, 98, 682–691. [Google Scholar] [CrossRef]
- Oedingen, C.; Bartling, T.; Krauth, C. Public, medical professionals’ and patients’ preferences for the allocation of donor organs for transplantation: Study protocol for discrete choice experiments. BMJ Open 2018, 8, e026040. [Google Scholar] [CrossRef] [Green Version]
- Johri, M.; Ubel, P.A. Setting organ allocation priorities: Should we care what the public cares about? Liver Transplant. 2003, 9, 878–880. [Google Scholar] [CrossRef] [PubMed]
- Oedingen, C.; Bartling, T.; Dierks, M.L.; Mühlbacher, A.C.; Schrem, H.; Krauth, C. Public preferences for the allocation of donor organs for transplantation: Focus group discussions. Heal. Expect. 2020, 23, 670–680. [Google Scholar] [CrossRef]
- Dolan, P.; Shaw, R. A note on a discussion group study of public preferences regarding priorities in the allocation of donor kidneys. Health Policy 2004, 68, 31–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elalouf, A.; Pliskin, J.S.; Kogut, T. Attitudes, knowledge, and preferences of the Israeli public regarding the allocation of donor organs for transplantation. Isr. J. Health Policy Res. 2020, 9, 25. [Google Scholar] [CrossRef] [PubMed]
- Ratcliffe, J. Public preferences for the allocation of donor liver grafts for transplantation. Health Econ. 2000, 9, 137–148. [Google Scholar] [CrossRef]
- Tong, A.; Howard, K.; Jan, S.; Cass, A.; Rose, J.; Chadban, S.; Allen, R.D.; Craig, J.C. Community preferences for the allocation of solid organs for transplantation: A systematic review. Transplantation 2010, 89, 796–805. [Google Scholar] [CrossRef]
- Wilmot, S.; Ratcliffe, J. Principles of distributive justice used by members of the general public in the allocation of donor liver grafts for transplantation: A qualitative study. Heal. Expect. 2002, 5, 199–209. [Google Scholar] [CrossRef] [Green Version]
- Howard, K.; Jan, S.; Rose, J.M.; Wong, G.; Irving, M.; Tong, A.; Craig, J.C.; Chadban, S.; Allen, R.D.; Cass, A. Community preferences for the allocation of donor organs for transplantation: A discrete choice study. Transplantation 2015, 99, 560–567. [Google Scholar] [CrossRef] [Green Version]
- Stahl, J.E.; Tramontano, A.C.; Swan, J.S.; Cohen, B.J. Balancing urgency, age and quality of life in organ allocation decisions-What would you do?: A survey. J. Med. Ethics 2008, 34, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Browning, C.J.; Thomas, S.A. Community values and preferences in transplantation organ allocation decisions. Soc. Sci. Med. 2001, 52, 853–861. [Google Scholar] [CrossRef]
- Sears, S.F.; Marhefka, S.L.; Rodrigue, J.R.; Campbell, C. The role of patients’ ability to pay, gender, and smoking history on public attitudes toward cardiac transplant allocation: An experimental investigation. Health Psychol. 2000, 19, 192–196. [Google Scholar] [CrossRef]
- Clark, M.D.; Gumber, A.; Leech, D.; Moro, D.; Szczepura, A.K.; West, N.; Higgins, R.M. Prioritising patients for renal transplantation? Analysis of patient preferences for kidney allocation according to ethnicity and gender. Divers. Equal. Health Care 2009, 6, 181–191. [Google Scholar] [CrossRef]
- Rose, C.; Nickerson, P.; Delmonico, F.; Randhawa, G.; Gill, J.; Gill, J.S. Estimation of potential deceased organ donors in Canada. Transplantation 2016, 100, 1558–1563. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cass, A.; Cunningham, J.; Anderson, K.; Snelling, P.; Colman, S.; Devitt, J.; Preece, C.; Eris, J. Decision-making about suitability for kidney transplantation: Results of a national survey of Australian nephrologists. Nephrology 2007, 12, 299–304. [Google Scholar] [CrossRef] [PubMed]
- Almeida, N.; Almeida, R.F.; Almeida, K.; Almeida, A. Attitude of medical professionals regarding controversial issues in kidney donation/transplantation. Indian J. Nephrol. 2016, 26, 393–397. [Google Scholar] [CrossRef]
- Thamer, M.; Hwang, W.; Fink, N.E.; Sadler, J.H.; Bass, E.B.; Levey, A.S.; Brookmeyer, R.; Powe, N.R. U.S. nephrologists’ attitudes towards renal transplantation: Results from a national survey. Transplantation 2001, 71, 281–288. [Google Scholar] [CrossRef] [Green Version]
- Tong, A.; Howard, K.; Wong, G.; Cass, A.; Jan, S.; Irving, M.; Craig, J.C. Nephrologists’ perspectives on waitlisting and allocation of deceased donor kidneys for transplant. Am. J. Kidney Dis. 2011, 58, 704–716. [Google Scholar] [CrossRef]
- Omar, F.; TinghÖg, G.; Carlsson, P.; Omnell-Persson, M.; Welin, S. Priority setting in kidney transplantation: A qualitative study evaluating Swedish practices. Scand. J. Public Health 2013, 41, 206–215. [Google Scholar] [CrossRef]
- Davison, S.N.; Kromm, S.K.; Currie, G.R. Patient and health professional preferences for organ allocation and procurement, end-of-life care and organization of care for patients with chronic kidney disease using a discrete choice experiment. Nephrol. Dial. Transplant. 2010, 25, 2334–2341. [Google Scholar] [CrossRef] [Green Version]
- Neuberger, J.; Adams, D.; MacMaster, P.; Maidment, A.; Speed, M. Assessing priorities for allocation of donor liver grafts: Survey of public and clinicians. Br. Med. J. 1998, 317, 172–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bedenko, R.C.; Nisihara, R.; Yokoi, D.S.; De Mello Candido, V.; Galina, I.; Moriguchi, R.M.; Ceulemans, N.; Salvalaggio, P. Analysis of knowledge of the general population and health professionals on organ donation after cardiac death. Rev. Bras. Ter. Intensiva 2016, 28, 285–293. [Google Scholar] [CrossRef] [PubMed]
- Söffker, G.; Bhattarai, M.; Welte, T.; Quintel, M.; Kluge, S. Attitude of intensive care specialists toward deceased organ donation in Germany: Results of a questionnaire at the 12th Congress of the German Interdisciplinary Association for Intensive and Emergency Medicine. Med. Klin. Intensivmed. Notfmed. 2014, 109, 41–417. [Google Scholar] [CrossRef]
- State of Israel Ministry of Health Kidney Allocation, Ministry of Health. Available online: https://www.health.gov.il/Subjects/Organ_transplant/transplant/allocation_general/Pages/kidneys_allocation.aspx (accessed on 30 December 2021).
- Sung, R.S.; Guidinger, M.K.; Lake, C.D.; McBride, M.A.; Greenstein, S.M.; Delmonico, F.L.; Port, F.K.; Merion, R.M.; Leichtman, A.B. Impact of the expanded criteria donor allocation system on the use of expanded criteria donor kidneys. Transplantation 2005, 79, 1257–1261. [Google Scholar] [CrossRef] [PubMed]
- Meier-Kriesche, H.U.; Schold, J.D.; Gaston, R.S.; Wadstrom, J.; Kaplan, B. Kidneys from deceased donors: Maximizing the value of a scarce resource. Am. J. Transplant. 2005, 5, 1725–1730. [Google Scholar] [CrossRef] [PubMed]
- Giessing, M.; Budde, K.; Fritsche, L.; Slowinski, T.; Tuerk, I.; Schoenberger, B.; Neumayer, H.H.; Loening, S.A. “Old-for-Old” Cadaveric Renal Transplantation: Surgical Findings, Perioperative Complications and Outcome. Eur. Urol. 2003, 44, 701–708. [Google Scholar] [CrossRef]
- Smits, J.M.A.; Persijn, G.G.; Van Houwelingen, H.C.; Claas, F.H.J.; Frei, U. Evaluation of the Eurotransplant Senior Program. The results of the first year. Am. J. Transplant. 2002, 2, 664–670. [Google Scholar] [CrossRef]
- Hippen, B.E.; Thistlethwaite, J.R.; Ross, L.F. Risk, Prognosis, and Unintended Consequences in Kidney Allocation. N. Engl. J. Med. 2011, 364, 1285–1287. [Google Scholar] [CrossRef] [PubMed]
- Cotter, T.G.; Wang, J.; Lieber, S.R.; Odenwald, M.A.; Rich, N.E.; Marrero, J.A.; Singal, A.G.; Mitchell, M.C.; Aronsohn, A.; Charlton, M.; et al. Raising HOPE: Improved Outcomes for HIV/HCV-coinfected Liver Transplant Recipients in the Direct-acting Antiviral Era. Transplant. Direct 2021, 7, e707. [Google Scholar] [CrossRef]
- Halpern, S.D.; Asch, D.A.; Shaked, A.; Stock, P.G.; Blumberg, E. Determinants of transplant surgeons’ willingness to provide organs to patients infected with HBV, HCV or HIV. Am. J. Transplant. 2005, 5, 1319–1325. [Google Scholar] [CrossRef]
- Asghari, F.; Broumand, M.; Heidari, A. Public preferences for donor kidney allocation: A study in Iran. Clin. Transplant. 2013, 27, 718–723. [Google Scholar] [CrossRef]
- Stewart, D.E.; Wood, D.W.; Alcorn, J.B.; Lease, E.D.; Hayes, M.; Hauber, B.; Goff, R.E. A revealed preference analysis to develop composite scores approximating lung allocation policy in the U.S. BMC Med. Inform. Decis. Mak. 2021, 21, 8. [Google Scholar] [CrossRef] [PubMed]
- Hanson, C.S.; Chadban, S.J.; Chapman, J.R.; Craig, J.C.; Wong, G.; Tong, A. Nephrologists’ perspectives on recipient eligibility and access to living kidney donor transplantation. Transplantation 2016, 100, 943–953. [Google Scholar] [CrossRef]
- Oedingen, C.; Bartling, T.; Mühlbacher, A.C.; Schrem, H.; Krauth, C. Systematic Review of Public Preferences for the Allocation of Donor Organs for Transplantation: Principles of Distributive Justice. Patient 2019, 12, 475–489. [Google Scholar] [CrossRef] [PubMed]
- Ralph, A.F.; Alyami, A.; Allen, R.D.M.; Howard, K.; Craig, J.C.; Chadban, S.J.; Irving, M.; Tong, A. Attitudes and beliefs about deceased organ donation in the Arabic-speaking community in Australia: A focus group study. BMJ Open 2016, 6, e010138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Günterberg, K. Health services. Dtsch. Arztebl. Int. 2013, 110, A1915. [Google Scholar]
- Jewish Virtual Library Latest Population Statistics for Israel | Jewish Virtual Library. Available online: https://www.jewishvirtuallibrary.org/latest-population-statistics-for-israel (accessed on 30 December 2021).



{kind=link}
{kind=link}
| Demographic Characteristics | Number | Percentage | |
|---|---|---|---|
| Gender | Male | 12 | 48 |
| Female | 13 | 52 | |
| Profession | Nephrologists | 14 | 56 |
| Surgeons | 3 | 12 | |
| Physicians | 2 | 8 | |
| Others | 6 | 24 | |
| Role in organ allocation | Health care professionals | 19 | 76 |
| Organ allocation managers | 6 | 24 | |
| Religion | Secular | 18 | 72 |
| Traditional | 4 | 16 | |
| Orthodox | 1 | 4 | |
| Religious | 2 | 8 | |
| Financial status | Average | 3 | 12 |
| Above-average | 16 | 64 | |
| Slightly above average | 6 | 24 | |
| Demographic Characteristics | Yes N (%) | No N (%) | Chi-Square Value | p-Value | |
|---|---|---|---|---|---|
| Gender | |||||
| Male | 11 (44) | 1 (4) | 0.294 | 0.58 | |
| Female | 11 (44) | 2 (8) | |||
| Age (y) | |||||
| 35–50 | 12 (48) | 2 (8) | 349 | 0.84 | |
| 51–65 | 8 (32) | 1 (4) | |||
| >65 | 2 (8) | 0 (0) | |||
| Profession | |||||
| Surgeons | 3 (12) | 0 (0) | 2.679 | 0.95 | |
| Nephrologists | 11 (44) | 3 (12) | |||
| Human resource coordinator | 1 (4) | 0 (0) | |||
| Chairman of association of kidney patients and their families | 1 (4) | 0 (0) | |||
| Physicians | 2 (8) | 0 (0) | |||
| Nutritionist | 1 (4) | 0 (0) | |||
| Nephrology nurse | 1 (4) | 0 (0) | |||
| Transplant coordinators | 1 (4) | 0 (0) | |||
| Ethical professor | 1 (4) | 0 (0) | |||
| Role in organ allocation | Health care professionals | 16 (64) | 3 (12) | 1.077 | 0.299 |
| Organ allocation managers | 6 (24) | 0 (0) | |||
| Health status | |||||
| Excellent | 8 (32) | 1 (4) | 2.694 | 0.61 | |
| Very good | 6 (24) | 0 (0) | |||
| Good | 4 (16) | 1 (4) | |||
| Fair | 2 (8) | 1 (4) | |||
| Poor | 2 (8) | 0 (0) | |||
| Marital status | |||||
| Married | 19 (76) | 3 (12) | 0.465 | 0.49 | |
| Unmarried | 2 (8) | 0 (0) | |||
| Children | |||||
| 0 | 7 (28) | 1 (4) | 7.244 | 0.203 | |
| 1 | 1 (4) | 1 (4) | |||
| 2 | 4 (16) | 0 (0) | |||
| 3 | 8 (32) | 0 (0) | |||
| 4 | 1 (4) | 1 (4) | |||
| 5 | 1 (4) | 0 (0) | |||
| Birthplace | |||||
| Israel | 16 (64) | 1 (4) | 9.774 | 0.008 | |
| America | 5 (20) | 0 (0) | |||
| USSR | 1 (4) | 2 (8) | |||
| Immigrant | |||||
| Parents | 8 (32) | 0 (0) | 2.286 | 0.131 | |
| Self | 6 (24) | 2 (8) | |||
| Religion | |||||
| Jewish | 21 (84) | 3 (12) | 0.142 | 0.706 | |
| Christian | 1 (4) | 0 (0) | |||
| Religiosity | |||||
| Secular | 16 (64) | 2 (8) | 1.741 | 0.783 | |
| Religious | 2 (8) | 0 (0) | |||
| Traditional | 3 (12) | 1 (4) | |||
| Orthodox | 1 (4) | 0 (0) | |||
| Financial status | |||||
| Above average | 15 (60) | 1 (4) | 9.809 | 0.007 | |
| Average | 1 (4) | 2 (8) | |||
| Slightly above average | 6 (24) | 0 (0) | |||
| Mean ± SD | Median | Chi-Square Test | p-Value | Pearson Correlation | |
|---|---|---|---|---|---|
| 1 Recipient’s age | 5.2 ± 1.63 | 5 | 4 | 0.40 | |
| 2 Having dependents | 3.6 ± 2.14 | 3 | 6.08 | 0.41 | 2 vs. 6 (p = 0.04) |
| 3 Waiting time | 5.84 ± 1.28 | 6 | 10.8 | 0.03 | 3 vs. 5 (p = 0.01) |
| 4 Prognosis | 5.92 ± 1.26 | 6 | 12 | 0.01 | |
| 5 Chance of receiving another donation soon | 5 ± 1.87 | 5 | 1.6 | 0.8 | |
| 6 Donor status | 4.12 ± 2.09 | 5 | 3.28 | 0.77 | 6 vs. 7 (p = 0.001) |
| 7 Next of kin donor status | 3.2 ± 2.06 | 3 | 12.8 | 0.04 |
| Chance of Receiving Another Donor N (%) | Waiting Time N (%) | Prognosis N (%) | Age N (%) | Donor Status N (%) | Chi-Square | p-Value | |
|---|---|---|---|---|---|---|---|
| Most Important | 3 (12) | 6 (24) | 13 (52) | 3 (12) | 0 | 10.68 | 0.01 |
| Least Important | 4 (16) | 1 (4) | 0 | 5 (20) | 15 (60) | 17.72 | 0.001 |
| Chance of Receiving Another Organ N (%) | Waiting Time N (%) | Prognosis N (%) | Recipient’s Age N (%) | Donor Status N (%) | Don’t Know N (%) | Chi-Square | p-Value | Pearson Correlation | |
|---|---|---|---|---|---|---|---|---|---|
| 1 Most Important | 1 (4) | 13 (52) | 2 (8) | 3 (12) | 1 (4) | 5 (20) | 25.16 | 0.00 | 1 vs. 2 (p = 0.02) |
| 2 Runner-up | 3 (12) | 4 (16) | 5 (20) | 7 (28) | 1 (4) | 5 (20) | 5 | 0.41 | 2 vs. 3 (p = 0.01) |
| 3 Least Important | 7 (28) | 0 (0) | 1 (4) | 1 (4) | 11 (44) | 5 (20) | 14.4 | 0.006 | 3 vs. 1 (p = 0.01) |
| Scenario no. | Description | Experts’ Preferences | Public Preferences [29] | The Point System Decision [48] |
|---|---|---|---|---|
| 1 | Patient A is 30 years old. Patient B is 45 years old. | |||
| No Preference | 84% | 71.5% | Patient A 2.9 points | |
| Patient A | 8% | 20% | ||
| Patient B | 8% | 5% | Patient B 1.4 points | |
| 2 | Patient A has a 70% chance of a successful transplant and waiting for 4 years. Patient B has a 90% chance of a successful transplant and waiting for 1 year. | |||
| No Preference | 0 | 12% | Patient A 3.92 points | |
| Patient A | 60% | 39% | ||
| Patient B | 40% | 45% | Patient B 4.48 points | |
| 3 | Patient A is 45 years old and waiting for 2 years. Patient B is 35 years old and waiting for the last 6 months. | |||
| No Preference | 12% | Patient A 2.46 points | ||
| Patient A | 80% | |||
| Patient B | 8% | Patient B 2.7 points | ||
| 4 | Patient A has a 90% chance of a successful transplant. The odds of finding another suitable kidney shortly (if he does not receive the kidney now) are 70%. Patient B has an 80% chance of a successful transplant. The odds of finding another suitable kidney soon (if he does not receive the kidney now) are 30%. | |||
| No Preference | 4% | |||
| Patient A | 8% | |||
| Patient B | 88% | |||
| 5 | Patient A is 40 years old and signed an organ donor card. Patient B is 20 years old and had not signed an organ donor | |||
| No Preference | 40% | 41% | Patient A 3.9 points | |
| Patient A | 44% | 36% | ||
| Patient B | 16% | 20% | Patient B 3.9 points | |
| 6 | Patient A is a registered donor and has a 70% chance to obtain another suitable kidney shortly if he does not receive the kidney now. Patient B is not a registered donor and has a 30% chance to obtain another suitable kidney shortly if he does not receive the kidney now. | |||
| No Preference | 4% | 21% | Patient A 4 points | |
| Patient A | 20% | 40% | ||
| Patient B | 76% | 36% | Patient B 4 points | |
| 7 | Patient A is 24 years old. He has a 70% chance of a successful transplant. Patient B is 50 years old. He has a 90% chance of a successful transplant. | |||
| No Preference | 24% | Patient A 3.5 points | ||
| Patient A | 20% | |||
| Patient B | 56% | Patient B 1.04 points | ||
| 8 | Patient A is an organ donor and waiting for 1 year. Patient B is not an organ donor and waiting for 4 years. | |||
| No Preference | 0 | 21% | Patient A 2.48 points | |
| Patient A | 24% | 23% | ||
| Patient B | 76% | 53% | Patient B 1.92 points | |
| 9 | Patient A is 40 years old. If he does not receive a kidney now, there is an 80% chance of finding another suitable kidney soon. Patient B is 55 years old. The odds of finding another suitable kidney shortly (if he does not receive the kidney now) are 40%. | |||
| No Preference | 12% | Patient A 1.99 points | ||
| Patient A | 12% | |||
| Patient B | 76% | Patient B 0.56 points | ||
| 10 | Patient A is a registered organ donor and has a 70% chance of a successful transplant. Patient B is not a registered organ donor and has a 90% chance of a successful transplant. | |||
| No Preference | 20% | 19% | Patient A 4 points | |
| Patient A | 32% | 27% | ||
| Patient B | 48% | 51% | Patient B 4 points | |
| 11 | Patient A has been waiting for a month. The odds of finding another suitable kidney soon (if he does not receive the kidney now) are 30%. Patient B has been on the waiting list for two years. The chances of finding another suitable kidney shortly (if he does not receive the kidney now) are 60%. | |||
| No Preference | 4% | Patient A 0.04 points | ||
| Patient A | 52% | |||
| Patient B | 44% | Patient B 0.96 points | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elalouf, A. Israeli Medical Experts’ Knowledge, Attitudes, and Preferences in Allocating Donor Organs for Transplantation. Int. J. Environ. Res. Public Health 2022, 19, 6945. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19116945
Elalouf A. Israeli Medical Experts’ Knowledge, Attitudes, and Preferences in Allocating Donor Organs for Transplantation. International Journal of Environmental Research and Public Health. 2022; 19(11):6945. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19116945
Chicago/Turabian StyleElalouf, Amir. 2022. "Israeli Medical Experts’ Knowledge, Attitudes, and Preferences in Allocating Donor Organs for Transplantation" International Journal of Environmental Research and Public Health 19, no. 11: 6945. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19116945