
Validation of PARADISE 24 and Development of PARADISE-EDEN 36 in Patients with Dementia

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Samples
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Item | Option | All | PARADISE 24 Data | EDEN18 Data | p-Value |
|---|---|---|---|---|---|
| Item 1 | None | 40 (19.9) | 13 (16.2) | 27 (22.3) | <0.001 |
| Mild to moderate | 93 (46.3) | 55 (68.8) | 38 (31.4) | ||
| Severe to extreme | 68 (33.8) | 12 (15.0) | 56 (46.3) | ||
| Item 2 | None | 68 (33.8) | 25 (31.2) | 43 (35.5) | 0.001 |
| Mild to moderate | 85 (42.3) | 46 (57.5) | 39 (32.2) | ||
| Severe to extreme | 46 (22.9) | 8 (10.0) | 38 (31.4) | ||
| Missing | 2 (1.0) | 1 (1.2) | 1 (0.8) | ||
| Item 3 | None | 115 (57.2) | 48 (60.0) | 67 (55.4) | 0.043 |
| Mild to moderate | 62 (30.8) | 28 (35.0) | 34 (28.1) | ||
| Severe to extreme | 24 (11.9) | 4 (5.0) | 20 (16.5) | ||
| Item 4 | None | 64 (31.8) | 34 (42.5) | 30 (24.8) | 0.004 |
| Mild to moderate | 75 (37.3) | 31 (38.8) | 44 (36.4) | ||
| Severe to extreme | 62 (30.8) | 15 (18.8) | 47 (38.8) | ||
| Item 5 | None | 88 (43.8) | 37 (46.2) | 51 (42.1) | 0.074 |
| Mild to moderate | 78 (38.8) | 35 (43.8) | 43 (35.5) | ||
| Severe to extreme | 35 (17.4) | 8 (10.0) | 27 (22.3) | ||
| Item 6 | None | 58 (28.9) | 21 (26.2) | 37 (30.6) | 0.026 |
| Mild to moderate | 97 (48.3) | 47 (58.8) | 50 (41.3) | ||
| Severe to extreme | 45 (22.4) | 11 (13.8) | 34 (28.1) | ||
| Missing | 1 (0.5) | 1 (1.2) | 0 (0.0) | ||
| Item 7 | None | 44 (21.9) | 19 (23.8) | 25 (20.7) | 0.001 |
| Mild to moderate | 97 (48.3) | 50 (62.5) | 47 (38.8) | ||
| Severe to extreme | 59 (29.4) | 11 (13.8) | 48 (39.7) | ||
| Missing | 1 (0.5) | 0 (0.0) | 1 (0.8) | ||
| Item 8 | None | 63 (31.3) | 28 (35.0) | 35 (28.9) | <0.001 |
| Mild to moderate | 74 (36.8) | 43 (53.8) | 31 (25.6) | ||
| Severe to extreme | 64 (31.8) | 9 (11.2) | 55 (45.5) | ||
| Item 9 | None | 56 (27.9) | 26 (32.5) | 30 (24.8) | 0.017 |
| Mild to moderate | 79 (39.3) | 38 (47.5) | 41 (33.9) | ||
| Severe to extreme | 65 (32.3) | 16 (20.0) | 49 (40.5) | ||
| Missing | 1 (0.5) | 0 (0.0) | 1 (0.8) | ||
| Item 10 | None | 64 (31.8) | 25 (31.2) | 39 (32.2) | 0.064 |
| Mild to moderate | 86 (42.8) | 41 (51.2) | 45 (37.2) | ||
| Severe to extreme | 51 (25.4) | 14 (17.5) | 37 (30.6) | ||
| Item 11 | None | 82 (40.8) | 46 (57.5) | 36 (29.8) | <0.001 |
| Mild to moderate | 65 (32.3) | 28 (35.0) | 37 (30.6) | ||
| Severe to extreme | 53 (26.4) | 5 (6.2) | 48 (39.7) | ||
| Missing | 1 (0.5) | 1 (1.2) | 0 (0.0) | ||
| Item 12 | None | 36 (17.9) | 7 (8.8) | 29 (24.0) | <0.001 |
| Mild to moderate | 91 (45.3) | 49 (61.3) | 42 (34.7) | ||
| Severe to extreme | 74 (36.8) | 24 (30.0) | 50 (41.3) | ||
| Item 13 | None | 60 (29.9) | 21 (26.2) | 39 (32.2) | 0.005 |
| Mild to moderate | 86 (42.8) | 40 (50.0) | 46 (38.0) | ||
| Severe to extreme | 50 (24.9) | 14 (17.5) | 36 (29.8) | ||
| Missing | 5 (2.5) | 5 (6.2) | 0 (0.0) | ||
| Item 14 | None | 84 (41.8) | 25 (31.2) | 59 (48.8) | <0.001 |
| Mild to moderate | 79 (39.3) | 46 (57.5) | 33 (27.3) | ||
| Severe to extreme | 37 (18.4) | 8 (10.0) | 29 (24.0) | ||
| Missing | 1 (0.5) | 1 (1.2) | 0 (0.0) | ||
| Item 15 | None | 46 (22.9) | 27 (33.8) | 19 (15.7) | <0.001 |
| Mild to moderate | 53 (26.4) | 30 (37.5) | 23 (19.0) | ||
| Severe to extreme | 94 (46.8) | 22 (27.5) | 72 (59.5) | ||
| Missing | 8 (4.0) | 1 (1.2) | 7 (5.8) | ||
| Item 16 | None | 74 (36.8) | 45 (56.2) | 29 (24.0) | <0.001 |
| Mild to moderate | 52 (25.9) | 24 (30.0) | 28 (23.1) | ||
| Severe to extreme | 75 (37.3) | 11 (13.8) | 64 (52.9) | ||
| Item 17 | None | 63 (31.3) | 6 (7.5) | 57 (47.1) | <0.001 |
| Mild to moderate | 24 (11.9) | 5 (6.2) | 19 (15.7) | ||
| Severe to extreme | 21 (10.4) | 1 (1.2) | 20 (16.5) | ||
| Missing | 93 (46.3) | 68 (85.0) | 25 (20.7) | ||
| Item 18 | None | 48 (23.9) | 17 (21.2) | 31 (25.6) | <0.001 |
| Mild to moderate | 42 (20.9) | 26 (32.5) | 16 (13.2) | ||
| Severe to extreme | 79 (39.3) | 19 (23.8) | 60 (49.6) | ||
| Missing | 32 (15.9) | 18 (22.5) | 14 (11.6) | ||
| Item 19 | None | 56 (27.9) | 23 (28.7) | 33 (27.3) | 0.010 |
| Mild to moderate | 74 (36.8) | 38 (47.5) | 36 (29.8) | ||
| Severe to extreme | 71 (35.3) | 19 (23.8) | 52 (43.0) | ||
| Item 20 | None | 107 (53.2) | 38 (47.5) | 69 (57.0) | 0.006 |
| Mild to moderate | 58 (28.9) | 31 (38.8) | 27 (22.3) | ||
| Severe to extreme | 31 (15.4) | 7 (8.8) | 24 (19.8) | ||
| Missing | 5 (2.5) | 4 (5.0) | 1 (0.8) | ||
| Item 21 | None | 118 (58.7) | 41 (51.2) | 77 (63.6) | <0.001 |
| Mild to moderate | 68 (33.8) | 39 (48.8) | 29 (24.0) | ||
| Severe to extreme | 15 (7.5) | 0 (0.0) | 15 (12.4) | ||
| Item 22 | None | 29 (14.4) | 6 (7.5) | 23 (19.0) | <0.001 |
| Mild to moderate | 49 (24.4) | 20 (25.0) | 29 (24.0) | ||
| Severe to extreme | 46 (22.9) | 0 (0.0) | 46 (38.0) | ||
| Missing | 77 (38.3) | 54 (67.5) | 23 (19.0) | ||
| Item 23 | None | 62 (30.8) | 29 (36.2) | 33 (27.3) | <0.001 |
| Mild to moderate | 61 (30.3) | 31 (38.8) | 30 (24.8) | ||
| Severe to extreme | 60 (29.9) | 9 (11.2) | 51 (42.1) | ||
| Missing | 18 (9.0) | 11 (13.8) | 7 (5.8) | ||
| Item 24 | None | 94 (46.8) | 37 (46.2) | 57 (47.1) | 0.474 |
| Mild to moderate | 55 (27.4) | 26 (32.5) | 29 (24.0) | ||
| Severe to extreme | 47 (23.4) | 15 (18.8) | 32 (26.4) | ||
| Missing | 5 (2.5) | 2 (2.5) | 3 (2.5) | ||
| Item 25 | None | 102 (50.7) | 50 (62.5) | 52 (43.0) | 0.004 |
| Mild to moderate | 72 (35.8) | 27 (33.8) | 45 (37.2) | ||
| Severe to extreme | 26 (12.9) | 3 (3.8) | 23 (19.0) | ||
| Missing | 1 (0.5) | 0 (0.0) | 1 (0.8) | ||
| Item 26 | None | 83 (41.3) | 41 (51.2) | 42 (34.7) | 0.007 |
| Mild to moderate | 77 (38.3) | 32 (40.0) | 45 (37.2) | ||
| Severe to extreme | 40 (19.9) | 7 (8.8) | 33 (27.3) | ||
| Missing | 1 (0.5) | 0 (0.0) | 1 (0.8) | ||
| Item 27 | None | 64 (31.8) | 26 (32.5) | 38 (31.4) | 0.008 |
| Mild to moderate | 88 (43.8) | 43 (53.8) | 45 (37.2) | ||
| Severe to extreme | 48 (23.9) | 10 (12.5) | 38 (31.4) | ||
| Missing | 1 (0.5) | 1 (1.2) | 0 (0.0) | ||
| Item 28 | None | 79 (39.3) | 39 (48.8) | 40 (33.1) | 0.001 |
| Mild to moderate | 80 (39.8) | 33 (41.2) | 47 (38.8) | ||
| Severe to extreme | 40 (19.9) | 6 (7.5) | 34 (28.1) | ||
| Missing | 2 (1.0) | 2 (2.5) | 0 (0.0) | ||
| Item 29 | None | 49 (24.4) | 18 (22.5) | 31 (25.6) | 0.096 |
| Mild to moderate | 86 (42.8) | 39 (48.8) | 47 (38.8) | ||
| Severe to extreme | 59 (29.4) | 18 (22.5) | 41 (33.9) | ||
| Missing | 7 (3.5) | 5 (6.2) | 2 (1.7) | ||
| Item 30 | None | 88 (43.8) | 51 (63.7) | 37 (30.6) | <0.001 |
| Mild to moderate | 57 (28.4) | 26 (32.5) | 31 (25.6) | ||
| Severe to extreme | 54 (26.9) | 3 (3.8) | 51 (42.1) | ||
| Missing | 2 (1.0) | 0 (0.0) | 2 (1.7) | ||
| Item 31 | None | 70 (34.8) | 37 (46.2) | 33 (27.3) | <0.001 |
| Mild to moderate | 75 (37.3) | 40 (50.0) | 35 (28.9) | ||
| Severe to extreme | 54 (26.9) | 3 (3.8) | 51 (42.1) | ||
| Missing | 2 (1.0) | 0 (0.0) | 2 (1.7) | ||
| Item 32 | None | 42 (20.9) | 11 (13.8) | 31 (25.6) | 0.008 |
| Mild to moderate | 80 (39.8) | 36 (45.0) | 44 (36.4) | ||
| Severe to extreme | 74 (36.8) | 28 (35.0) | 46 (38.0) | ||
| Missing | 5 (2.5) | 5 (6.2) | 0 (0.0) | ||
| Item 33 | None | 48 (23.9) | 27 (33.8) | 21 (17.4) | <0.001 |
| Mild to moderate | 64 (31.8) | 35 (43.8) | 29 (24.0) | ||
| Severe to extreme | 81 (40.3) | 18 (22.5) | 63 (52.1) | ||
| Missing | 8 (4.0) | 0 (0.0) | 8 (6.6) | ||
| Item 34 | None | 54 (26.9) | 22 (27.5) | 32 (26.4) | 0.001 |
| Mild to moderate | 81 (40.3) | 43 (53.8) | 38 (31.4) | ||
| Severe to extreme | 66 (32.8) | 15 (18.8) | 51 (42.1) | ||
| Item 35 | None | 76 (37.8) | 31 (38.8) | 45 (37.2) | 0.033 |
| Mild to moderate | 94 (46.8) | 43 (53.8) | 51 (42.1) | ||
| Severe to extreme | 31 (15.4) | 6 (7.5) | 25 (20.7) | ||
| Item 36 | None | 52 (25.9) | 20 (25.0) | 32 (26.4) | 0.012 |
| Mild to moderate | 71 (35.3) | 38 (47.5) | 33 (27.3) | ||
| Severe to extreme | 75 (37.3) | 22 (27.5) | 53 (43.8) | ||
| Missing | 3 (1.5) | 0 (0.0) | 3 (2.5) | ||
| Item 37 | None | 62 (30.8) | 43 (53.8) | 19 (15.7) | <0.001 |
| Mild to moderate | 65 (32.3) | 32 (40.0) | 33 (27.3) | ||
| Severe to extreme | 70 (34.8) | 5 (6.2) | 65 (53.7) | ||
| Missing | 4 (2.0) | 0 (0.0) | 4 (3.3) | ||
| Item 38 | None | 47 (23.4) | 16 (20.0) | 31 (25.6) | <0.001 |
| Mild to moderate | 80 (39.8) | 49 (61.3) | 31 (25.6) | ||
| Severe to extreme | 66 (32.8) | 13 (16.2) | 53 (43.8) | ||
| Missing | 8 (4.0) | 2 (2.5) | 6 (5.0) | ||
| Item 39 | None | 87 (43.3) | 39 (48.8) | 48 (39.7) | 0.007 |
| Mild to moderate | 69 (34.3) | 32 (40.0) | 37 (30.6) | ||
| Severe to extreme | 44 (21.9) | 8 (10.0) | 36 (29.8) | ||
| Missing | 1 (0.5) | 1 (1.2) | 0 (0.0) | ||
| Item 40 | None | 64 (31.8) | 19 (23.8) | 45 (37.2) | <0.001 |
| Mild to moderate | 66 (32.8) | 27 (33.8) | 39 (32.2) | ||
| Severe to extreme | 56 (27.9) | 19 (23.8) | 37 (30.6) | ||
| Missing | 15 (7.5) | 15 (18.8) | 0 (0.0) | ||
| Item 41 | None | 89 (44.3) | 31 (38.8) | 58 (47.9) | 0.041 |
| Mild to moderate | 87 (43.3) | 40 (50.0) | 47 (38.8) | ||
| Severe to extreme | 22 (10.9) | 6 (7.5) | 16 (13.2) | ||
| Missing | 3 (1.5) | 3 (3.8) | 0 (0.0) | ||
| Item 42 | None | 83 (41.3) | 35 (43.8) | 48 (39.7) | <0.001 |
| Mild to moderate | 67 (33.3) | 37 (46.2) | 30 (24.8) | ||
| Severe to extreme | 49 (24.4) | 6 (7.5) | 43 (35.5) | ||
| Missing | 2 (1.0) | 2 (2.5) | 0 (0.0) |
References
- World Health Organization. The Global Dementia Observatory Reference Guide (CC BY-NC-SA 3.0 IGO); World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- World Health Organization. The Global Action Plan on the Public Health Response to Dementia 2017–2025; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Jakob, R.; Üstün, B.; Madden, R.; Sykes, C. The WHO Family of International Classifications. Bundesgesundheitsblatt Gesundh. Gesundh. 2007, 50, 924–931. [Google Scholar] [CrossRef]
- Cipriani, G.; Danti, S.; Picchi, L.; Nuti, A.; Fiorino, M. Daily functioning and dementia. Dement. Neuropsychol. 2020, 14, 93–102. [Google Scholar] [CrossRef]
- Gitlin, L.N.; Marx, K.A.; Stanley, I.H.; Hansen, B.R.; van Haitsma, K.S. Assessing neuropsychiatric symptoms in people with dementia: A systematic review of measures. Int. Psychogeriatr. 2014, 26, 1805–1848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, S.T.S.; Yu, M.-L.; Brown, T.; Andrews, H. Association between older adults’ functional performance and their scores on the Mini Mental State Examination (MMSE) and Montreal Cognitive Assessment (MoCA). Ir. J. Occup. Ther. 2018, 46, 4–23. [Google Scholar] [CrossRef] [Green Version]
- Krein, L.; Jeon, Y.H.; Amberber, A.M.; Fethney, J. The Assessment of Language and Communication in Dementia: A Synthesis of Evidence. Am. J. Geriatr. Psychiatry 2019, 27, 363–377. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.S.; O’Connor, E.; Rossom, R.C.; Perdue, L.A.; Burda, B.U.; Thompson, M.; Eckstrom, E. Screening for Cognitive Impairment in Older Adults: An Evidence Update for the U.S. Preventive Services Task Force [Internet]; Evidence Synthesis, No. 189; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2020. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/books/NBK554654/ (accessed on 1 March 2022).
- Malara, A.; Sgrò, G.; Ceravolo, F.; Curinga, G.; Renda, G.F.; Spadea, F.; Rispoli, V. Profiles of ICF disability in Alzheimer and Vascular dementia. J. Aging Res. Clin. Pract. 2015, 4, 154–158. [Google Scholar] [CrossRef]
- Cieza, A.; Anczewska, M.; Ayuso-Mateos, J.L.; Baker, M.; Bickenbach, J.; Chatterji, S.; Consortium, P. Understanding the Impact of Brain Disorders: Towards a ‘Horizontal Epidemiology’ of Psychosocial Difficulties and Their Determinants. PLoS ONE 2015, 10, e0136271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cieza, A.; Sabariego, C.; Anczewska, M.; Ballert, C.; Bickenbach, J.; Cabello, M.; et Consortium, P. PARADISE 24: A Measure to Assess the Impact of Brain Disorders on People’s Lives. PLoS ONE 2015, 10, e0132410. [Google Scholar] [CrossRef]
- World Health Organization. ICF: International Classification of Functioning, Disability and Health; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- Rasch, G.W. Probabilistic Models for some Intelligence and Attainment Tests Copenhagen; MESA Press: San Diego, CA, USA, 1960. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-IV, 4th ed.; American Psychiatric Association: Washington, DC, USA, 1995. [Google Scholar]
- Roman, G.C.; Tatemichi, T.K.; Erkinjuntti, T.; Cummings, J.L.; Masdeu, J.C.; Garcia, J.H.; Amaducci, L.; Orgogozo, J.-M.; Brun, A.; Hofman, A.; et al. Vascular dementia: Diagnostic criteria for research studies: Report of the NINDS-AIREN International Workshop. Neurology 1993, 43, 250–260. [Google Scholar] [CrossRef]
- McKhann, G.; Drachman, D.; Folstein, M.; Katzman, R.; Price, D.; Stadlan, E.M. Clinical diagnosis of Alzheimer’s disease: Report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer’s Disease. Neurology 1984, 34, 939–944. [Google Scholar] [CrossRef] [Green Version]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”: A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Katz, S. Assessing self-maintenance: Activities of daily living, mobility, and instrumental activities of daily living. J. Am. Geriatr. Soc. 1983, 31, 721–727. [Google Scholar] [CrossRef] [PubMed]
- Masters, G.N. A rasch model for partial credit scoring. Psychometrika 1982, 47, 149–174. [Google Scholar] [CrossRef]
- Tennant, A.; Conaghan, P.G. The Rasch measurement model in rheumatology: What is it and why use it? When should it be applied, and what should one look for in a Rasch paper? Arthritis Rheum. 2007, 57, 1358–1362. [Google Scholar] [CrossRef] [PubMed]
- Wright, B.D.; Linacre, J.M.; Gustafson, J.E.; Martin-Loef, P. Reasonable Mean-Square Fit Values. Rasch Meas. Trans. 1994, 8, 370. [Google Scholar]
- Colton, D.A.; Gao, X.; Harris, D.J.; Kolen, M.J.; Martinovich-Barhite, D.; Wang, T.; Welch, C.J. Reliability Issues with Performance Assessments: A Collection of Papers; ACT Research Report Series 97-3; ACT, Inc.: Iowa City, IA, USA, 1997; pp. 1–137. [Google Scholar]
- Nunnally, J.C. Psychometric Theory, 2nd ed.; McGraw-Hill: New York, NY, USA, 1978. [Google Scholar]
- Wright, B.D. Reliability and separation. Rasch Meas. Trans. 1996, 9, 472. [Google Scholar]
- Smith, R.M.; Schumacker, R.E.; Bush, M.J. Using item mean squares to evaluate fit to the Rasch model. J. Outcome Meas. 1998, 2, 66–78. [Google Scholar] [PubMed]
- Andrich, D.; Luo, G. Conditional Pairwise Estimation in the Rasch Model for Ordered Response Categories Using Principal Components. J. Appl. Meas. 2003, 4, 205–221. [Google Scholar]
- Andrich, D.; Marais, I. A Course in Rasch Measurement Theory: Measuring in the Educational, Social and Health Sciences; Springer: Singapore, 2019. [Google Scholar]
- Yen, W.M. Effects of Local Item Dependence on the Fit and Equating Performance of the Three-Parameter Logistic Model. Appl. Psychol. Meas. 1984, 8, 125–145. [Google Scholar] [CrossRef]
- Baghaei, P. Local Dependency and Rasch Measures. Rasch Meas. Trans. 2008, 21, 1105–1106. [Google Scholar]
- Marais, I. Local dependence. In Rasch Models in Health; John Wiley & Sons: Hoboken, NJ, USA, 2012; pp. 111–130. [Google Scholar]
- Smith, E.V.J. Detecting and Evaluating the Impact of Multidimensionality Using Item Fit Statistics and Principal Component Analysis of Residuals. J. Appl. Meas. 2002, 3, 205–231. [Google Scholar]
- Holland, P.W.; Wainger, H. Differential Item Functioning; Erlbaum: Hillsdale, NJ, USA, 1993. [Google Scholar]
- Benjamini, Y.; Hochberg, Y. Controlling the False Discovery Rate: A Practical and Powerful Approach to Multiple Testing. J. R. Stat. Soc. Ser. B 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Stekhoven, D.J.; Bühlmann, P. MissForest—Non-parametric missing value imputation for mixed-type data. Bioinformatics 2011, 28, 112–118. [Google Scholar] [CrossRef] [Green Version]
- Yoshida, K.; Bartel, A. Tableone: Create ’Table 1’ to Describe Baseline Characteristics with or without Propensity Score Weights. 2021. Available online: https://CRAN.R-project.org/package=tableone (accessed on 1 June 2022).
- Kuan, Y.-C.; Huang, L.-K.; Wang, Y.-H.; Hu, C.-J.; Tseng, I.-J.; Chen, H.-C.; Lin, L.-F. Balance and gait performance in older adults with early-stage cognitive impairment. Eur. J. Phys. Rehabil. Med. 2021, 57, 560–567. [Google Scholar] [CrossRef]
- Thom, R.P.; Grudzinskas, A.J., Jr.; Saleh, F.M. Sexual Behavior Among Persons with Cognitive Impairments. Curr. Psychiatry Rep. 2017, 19, 25. [Google Scholar] [CrossRef]
- Srinivasan, S.; Glover, J.; Tampi, R.R.; Tampi, D.J.; Sewell, D.D. Sexuality and the Older Adult. Curr. Psychiatry Rep. 2019, 21, 97. [Google Scholar] [CrossRef]
- Malara, A.; Sgrò, G.; Caruso, C.; Ceravolo, F.; Curinga, G.; Renda, G.F.; Rispoli, V. Relationship between cognitive impairment and nutritional assessment on functional status in Calabrian long-term-care. Clin. Int. Aging 2014, 9, 105–110. [Google Scholar] [CrossRef] [Green Version]
- Sharp, E.S.; Gatz, M. Relationship between education and dementia: An updated systematic review. Alzheimer Dis. Assoc. Disord. 2011, 25, 289–304. [Google Scholar] [CrossRef] [Green Version]
- Jackson, C.A.; Sudlow, C.L.M.; Mishra, G.D. Education, sex and risk of stroke: A prospective cohort study in New South Wales, Australia. BMJ Open 2018, 8, e024070. [Google Scholar] [CrossRef] [PubMed] [Green Version]




| PARADISE | EDEN | All | |||||
|---|---|---|---|---|---|---|---|
| Item | Question | In/Outfit | DIF | In/Outfit | DIF | In/Outfit | DIF |
| Item 1 | Problem due to not feeling rested and refreshed during the day? | 0.79/0.8 | 0.87/0.85 | ||||
| Item 2 | Problem with loss of interest? | 0.86/0.89 | 0.96/0.98 | ||||
| Item 3 | Problem with your appetite? | 1.23/1.33 | 1.44/1.41 | ||||
| Item 4 | Problem with sleeping, such as falling asleep, waking up frequently during the night or waking up too early in the morning? | 1.14/1.02 | 1.35/1.09 | ||||
| Item 5 | Problem being so irritable that you started arguments, shouted at people or even hit people? | 1.11/1.11 | 1.11/1.11 | ||||
| Item 6 | Problem with being slowed down or feeling as if things were moving too fast around you? | 0.89/0.89 | 0.98/0.96 | ||||
| Item 7 | Problem with feeling sad, low or depressed? | 0.88/0.91 | 0.96/0.99 | ||||
| Item 8 | Problem with worry or anxiety? | 0.91/0.97 | 0.96/1.02 | ||||
| Item 9 | Problem with not being able to cope with all the things that you had to do? | 0.77/0.8 | 0.83/0.88 | ||||
| Item 10 | How much bodily ache or pain did you have? | 1.12/1.13 | 1.22/1.19 | ||||
| Item 11 | Difficulty in concentrating on doing something for ten minutes? | 0.84/0.87 | S | 0.96/0.95 | S | ||
| Item 12 | Difficulty in remembering to do important things? | 1.17/1.09 | 1.24/1.15 | ||||
| Item 13 | Difficulty in making decisions? | 0.88/0.88 | 0.96/0.94 | ||||
| Item 14 | Difficulty in starting and maintaining a conversation? | 1.07/1.07 | 1.11/1.11 | ||||
| Item 15 | Difficulty in walking a long distance such as a kilometer (or equivalent)? | 1.28/1.25 | 1.24/1.23 | ||||
| Item 16 | Difficulty in grooming or dressing, toileting or eating? | 0.94/0.98 | R; S | 0.85/0.9 | R; S | ||
| Item 17 | Difficulty in sexual activities? | 1.1/1.06 | 1.21/1.19 | ||||
| Item 18 | Difficulty in staying by yourself for a few days? | 0.79/0.84 | 0.88/0.9 | ||||
| Item 19 | Difficulty with looking after your health, such as eating well, exercising and taking your medicines? | 0.87/0.88 | 0.94/0.92 | ||||
| Item 20 | Difficulty in initiating and maintaining a friendship? | 1.04/0.97 | 1.12/1.02 | ||||
| Item 21 | Difficulty in getting along with people who are close to you? | 0.85/0.86 | 0.89/0.89 | ||||
| Item 22 | Difficulty in your day-to-day work or school? | 0.75/0.77 | 0.73/0.76 | ||||
| Item 23 | Difficulty with managing your money? | 1.28/1.05 | 1.27/1.07 | ||||
| Item 24 | Difficulty in joining in community activities (for example, festivities, religious or other activities) in the same way as anyone else can? | 1.12/1.08 | 1.19/1.1 | ||||
| Item 25 | Problem resisting doing or saying things in ways you would normally think were inappropriate? | 1.1/1.08 | 0.97/0.98 | ||||
| Item 26 | Problem with feeling lonely even when with people? | 0.93/0.98 | 0.91/0.97 | ||||
| Item 27 | Problem in finding the words you wanted to say or understanding words said to you? | 0.96/1 | 0.91/0.96 | ||||
| Item 28 | Problem with feeling that your thoughts were too slow or that you could not think clearly? | 0.98/0.87 | 0.92/0.88 | ||||
| Item 29 | Difficulty in analyzing and finding solutions to problems in day-to-day life? | 0.8/0.83 | 0.78/0.82 | ||||
| Item 30 | Problem with passing water (urinating) or in controlling urine? | 0.87/0.89 | S | 0.85/0.9 | S | ||
| Item 31 | Problem with your balance? | 1.11/1.12 | R; S | 1.06/1.1 | R; S | ||
| Item 32 | Difficulty in learning a new task, for example, learning how to get to a new place? | 1.05/1.05 | R; S | 0.99/1.03 | R; S | ||
| Item 33 | Difficulty in reading books, instructions or newspapers? | 1.11/1.03 | 1.04/1.01 | ||||
| Item 34 | Difficulty in carrying out your day-to-day activities? | 0.71/0.7 | 0.67/0.7 | ||||
| Item 35 | Difficulty in generally understanding what people say? | 0.91/0.92 | 0.88/0.91 | ||||
| Item 36 | Difficulty in lifting and carrying things? | 1.16/1.09 | 1.04/1.05 | ||||
| Item 37 | Difficulty with moving around? | 1.21/1.13 | R; S | 1.15/1.11 | R; S | ||
| Item 38 | Difficulty in taking care of your household responsibilities? | 0.87/0.85 | 0.86/0.85 | ||||
| Item 39 | Difficulty in dealing with conflicts and tensions with others? | 0.96/0.97 | 0.88/0.93 | ||||
| Item 40 | Difficulty in providing for or supporting others? | 0.92/0.94 | R; S | 0.92/0.9 | R | ||
| Item 41 | Difficulty in dealing with people you do not know? | 1.16/1.14 | R; S | 1.08/1.07 | R | ||
| Item 42 | Difficulty in doing things by yourself for relaxation or pleasure? | 0.88/0.85 | 0.83/0.82 | ||||
| Overall | PARADISE-Data | EDEN-Data | p-Value | |
|---|---|---|---|---|
| N | 201 | 80 | 121 | |
| Age-mean (SD) | 82.55 (6.95) | 82.06 (5.51) | 82.88 (7.78) | 0.418 |
| Gender: Female (%) | 152 (76.0) | 63 (78.8) | 89 (74.2) | 0.566 |
| Marital Status | 0.078 | |||
| Married | 53 (26.4) | 25 (31.2) | 28 (23.1) | |
| Widowed | 114 (56.7) | 48 (60.0) | 66 (54.5) | |
| Divorced | 12 (6.0) | 2 (2.5) | 10 (8.3) | |
| Never Married | 22 (10.9) | 5 (6.2) | 17 (14.0) | |
| <0.001 | ||||
| Education (%) | ||||
| Less than primary school | 3 (3.8) | |||
| Primary school completed | 15 (18.8) | |||
| Secondary school completed | 3 (3.8) | |||
| High school (or equivalent) completed | 32 (40.0) | |||
| University completed | 22 (27.5) | |||
| Post graduate degree completed | 5 (6.2) | |||
| Education (%) | ||||
| Illiteracy | 33 (27.3) | |||
| Primary School | 67 (55.4) | |||
| High School | 16 (13.2) | |||
| Degree | 5 (4.1) | |||
| Residency: Home (%) | 103 (51.2) | 70 (87.5) | 33 (27.3) | <0.001 |
| Diagnosis (%) | <0.001 | |||
| Alzheimer Disease | 86 (44.3) | 49 (61.3) | 37 (32.5) | |
| Vascular Dementia | 92 (47.4) | 27 (33.8) | 65 (57.0) | |
| Other | 16 (8.2) | 4 (5.0) | 12 (10.5) | |
| MMSE-mean (SD) | 19.26 (3.79) | 21.10 (2.89) | 18.03 (3.83) | <0.001 |
| Satisfaction in ADL (%) | <0.001 | |||
| Very satisfied | 3 (3.8) | |||
| Satisfied | 27 (33.8) | |||
| Neither satisfied nor dissatisfied | 33 (41.2) | |||
| Dissatisfied | 17 (21.2) | |||
| Independence in ADL (%) | ||||
| Independence | 14 (11.7) | |||
| Mild dependence | 23 (19.2) | |||
| Moderate dependence | 33 (27.5) | |||
| Severe dependence | 50 (41.7) |
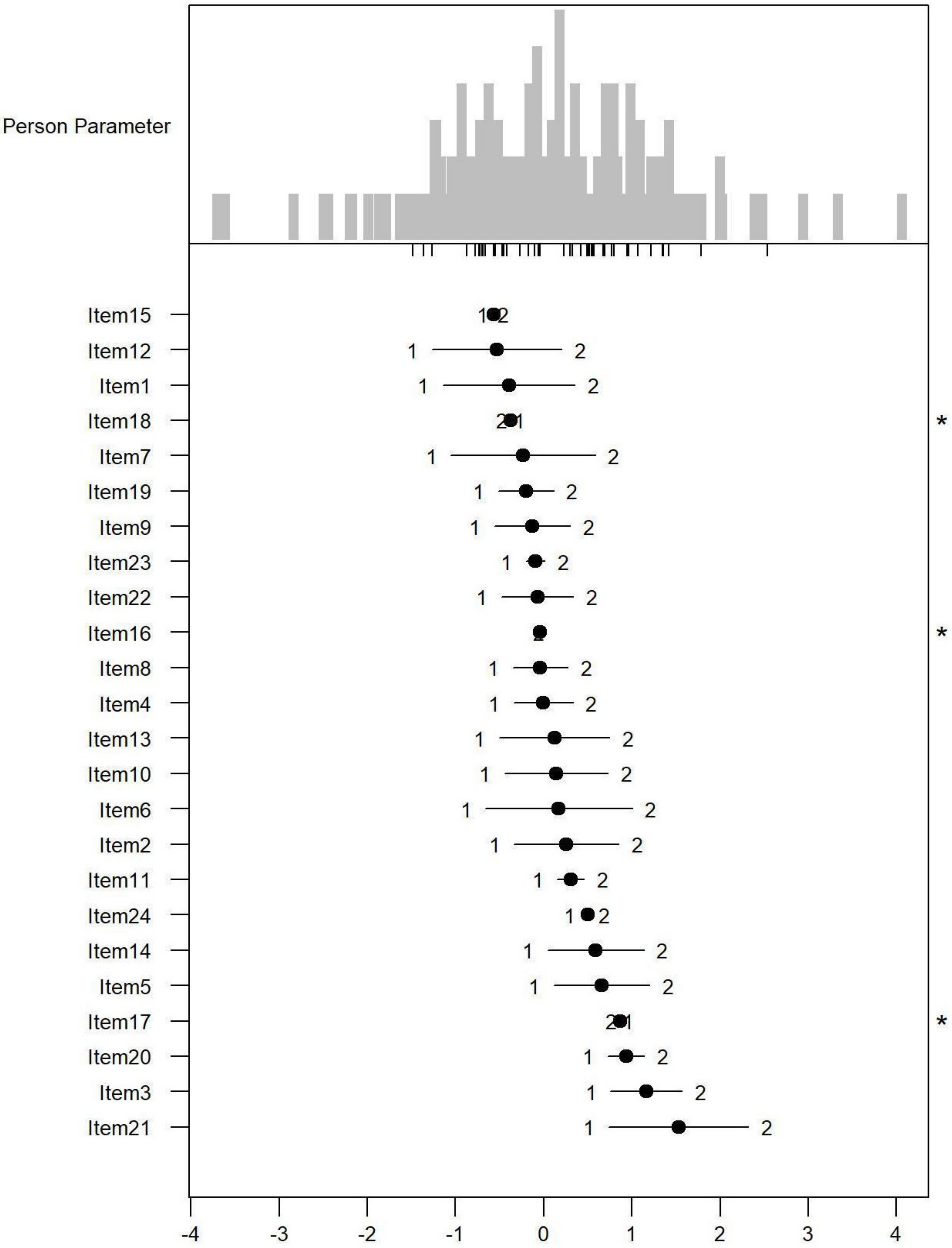
| Mean | SD | (Min; Max) | Mean Residuals | SD Residuals | |||
|---|---|---|---|---|---|---|---|
| Paradise Items | Targeting | Difficulty | 0.19 | 0.86 | (−1.48; 2.54) | 0.2 | 0.04 |
| Ability | 0.11 | 0.97 | (−3.71; 4.06) | 0.33 | 0.08 | ||
| Index | Coefficient | Strata | |||||
| Reliability | Difficulty | 0.94 | 4.17 | 5.89 | |||
| Ability | 0.9 | 3.07 | 4.43 | ||||
| Alpha | |||||||
| Test | 0.91 | ||||||
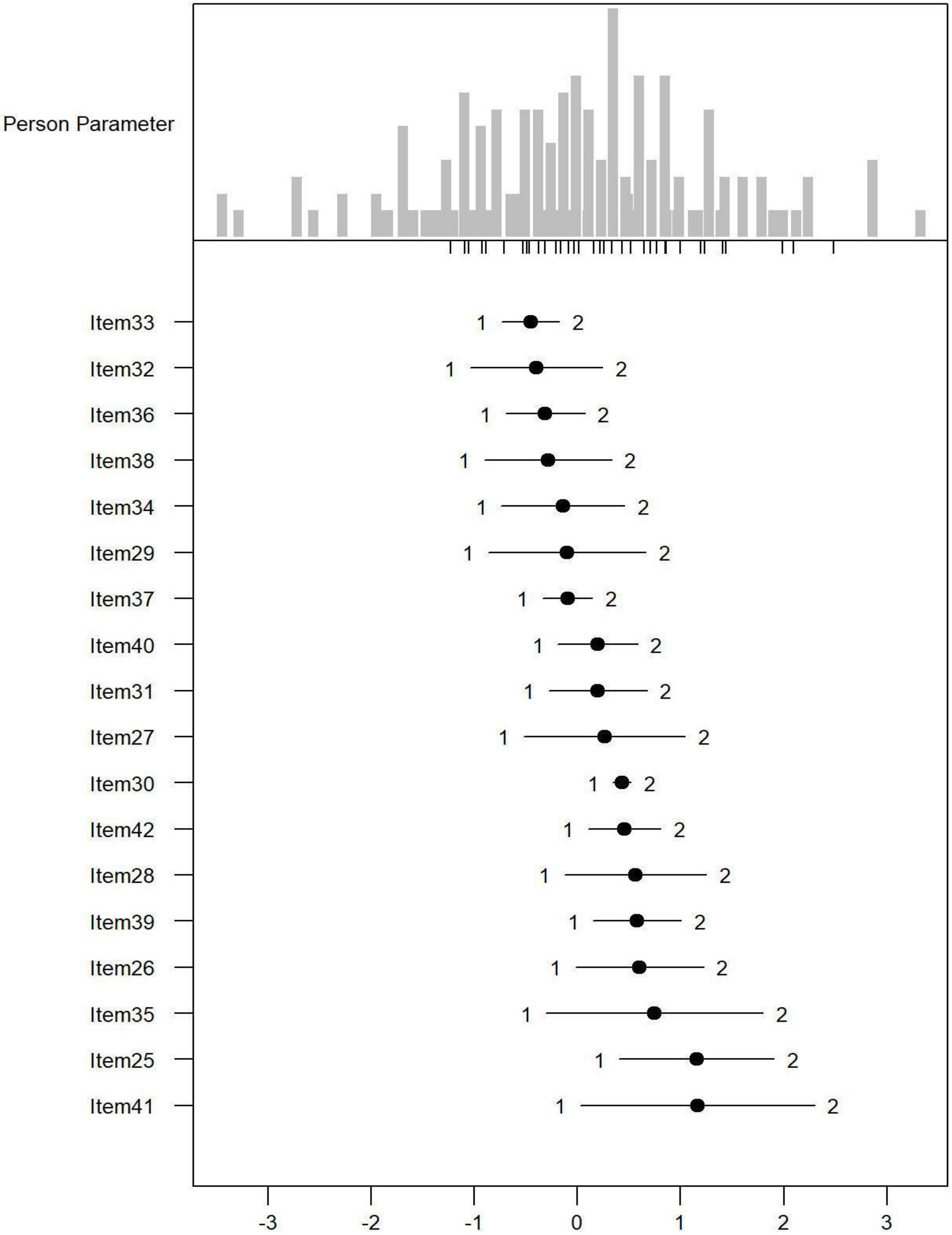
| Mean | SD | (Min; Max) | Mean Residuals | SD Residuals | |||
| Eden Items | Targeting | Difficulty | 0.25 | 0.95 | (−1.23; 2.49) | 0.2 | 0.03 |
| Ability | 0.02 | 1.21 | (−4.25; 4.3) | 0.41 | 0.11 | ||
| Index | Coefficient | Strata | |||||
| Reliability | Difficulty | 0.88 | 4.69 | 6.58 | |||
| Ability | 0.96 | 2.8 | 4.07 | ||||
| Alpha | |||||||
| Test | 0.91 | ||||||
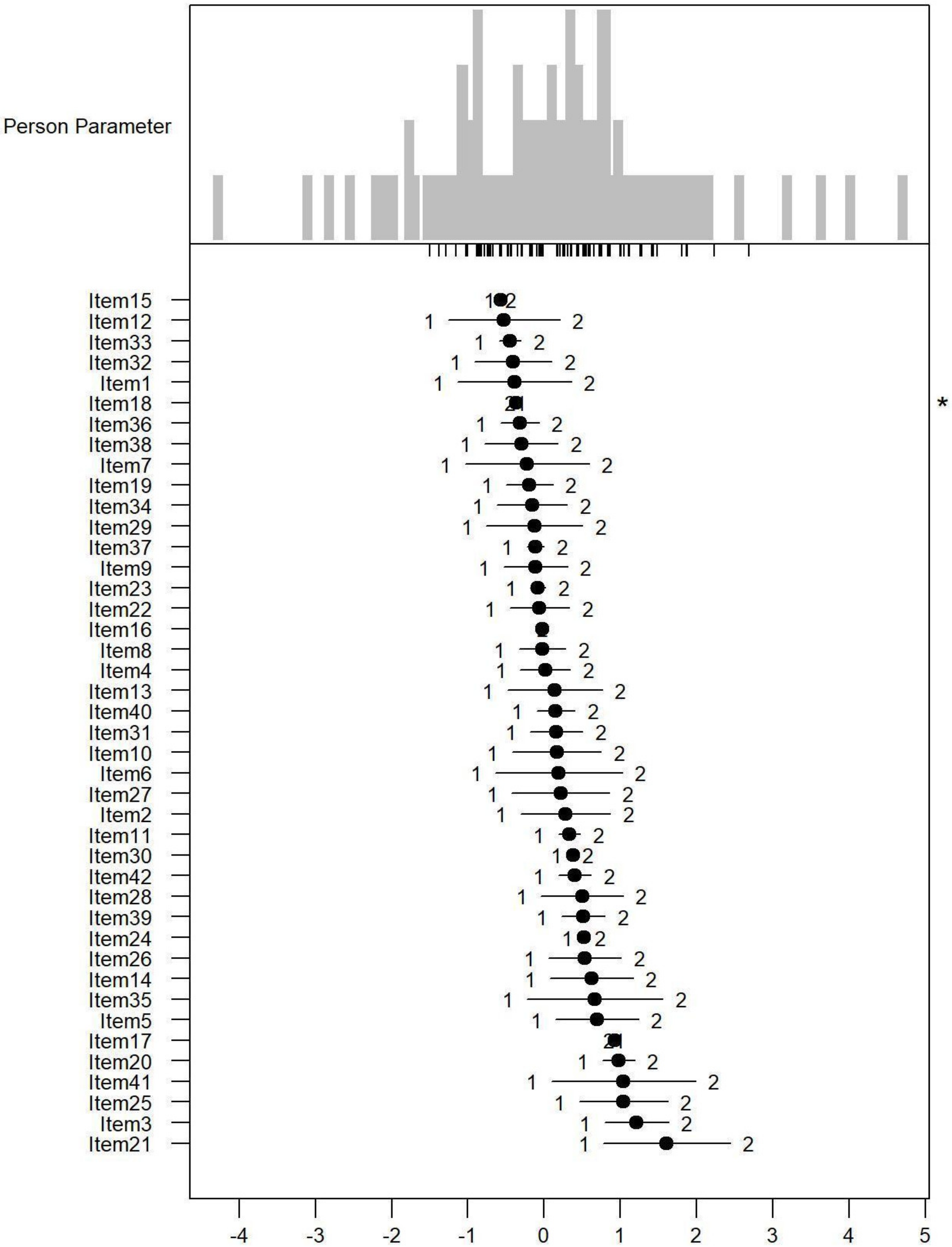
| Mean | SD | (Min; Max) | Mean Residuals | SD Residuals | |||
| All Items | Targeting | Difficulty | 0.21 | 0.88 | (−1.5; 2.69) | 0.2 | 0.03 |
| Ability | 0.16 | 0.98 | (−4.28; 4.7) | 0.25 | 0.09 | ||
| Index | Coefficient | Strata | |||||
| Reliability | Difficulty | 0.95 | 4.29 | 6.05 | |||
| Ability | 0.94 | 4.31 | 6.08 | ||||
| Alpha | |||||||
| Test | 0.95 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Talarico, F.; Fellinghauer, C.; De Biase, G.A.; Gareri, P.; Capurso, S.; Moneti, P.; Caruso, A.; Chiatante, V.; Gentile, E.; Malerba, M.; et al. Validation of PARADISE 24 and Development of PARADISE-EDEN 36 in Patients with Dementia. Int. J. Environ. Res. Public Health 2022, 19, 6949. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19116949
Talarico F, Fellinghauer C, De Biase GA, Gareri P, Capurso S, Moneti P, Caruso A, Chiatante V, Gentile E, Malerba M, et al. Validation of PARADISE 24 and Development of PARADISE-EDEN 36 in Patients with Dementia. International Journal of Environmental Research and Public Health. 2022; 19(11):6949. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19116949
Chicago/Turabian StyleTalarico, Francesco, Carolina Fellinghauer, Giuseppe Andrea De Biase, Pietro Gareri, Sebastiano Capurso, Paolo Moneti, Angela Caruso, Valentina Chiatante, Emanuela Gentile, Monica Malerba, and et al. 2022. "Validation of PARADISE 24 and Development of PARADISE-EDEN 36 in Patients with Dementia" International Journal of Environmental Research and Public Health 19, no. 11: 6949. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19116949