
Evaluation of Infant Injury Prevention Education Provided during Antenatal Classes after Two Years: A Pilot Prospective Cohort Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
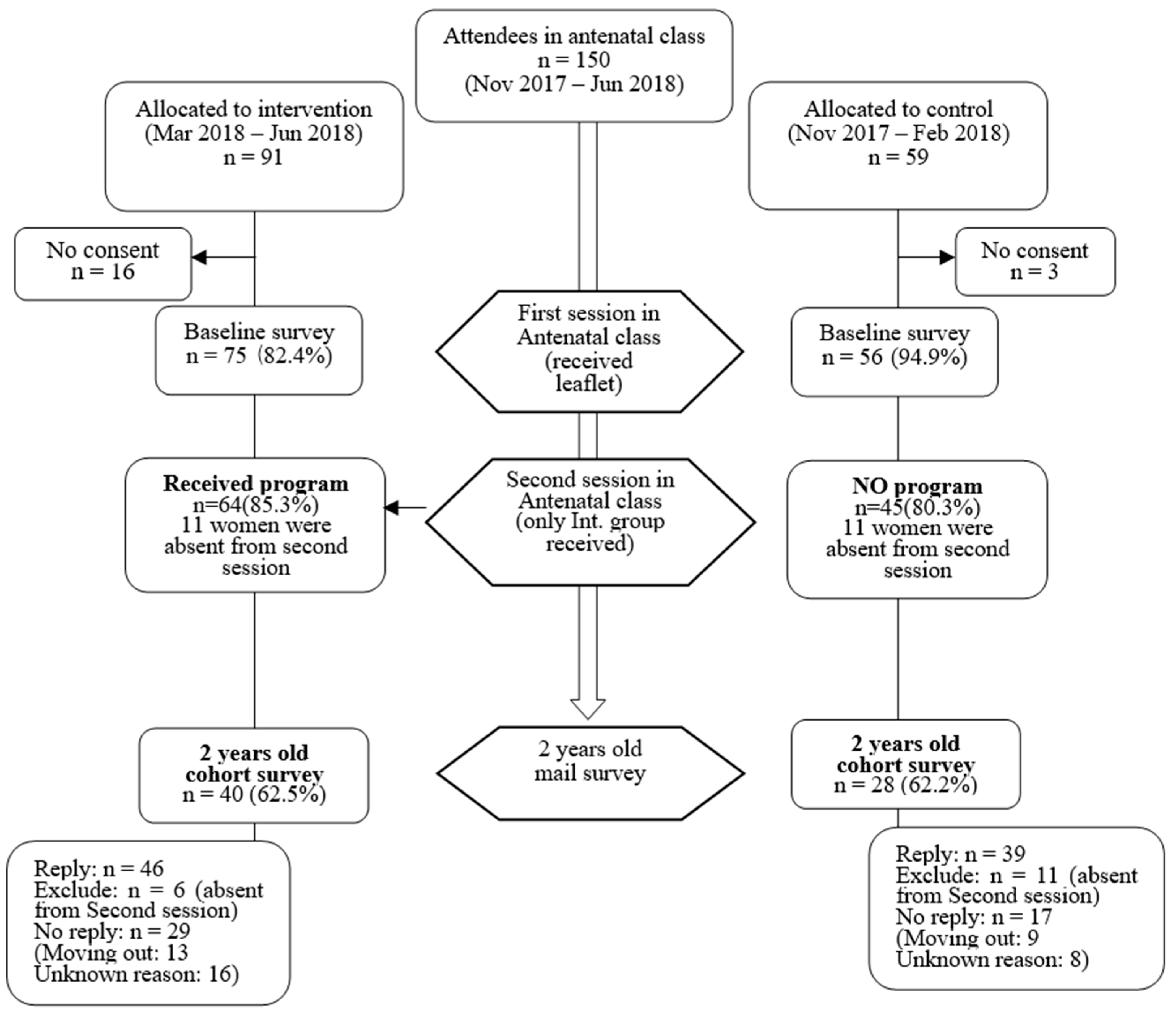
2.1. Study Design and Setting
2.2. Eligibility and Enrollment
2.3. Study Outcomes
2.4. Ethical Considerations
2.5. Statistical Analysis
3. Results
3.1. Participant Characteristics and Injury Status up to 24 Months of Age
3.2. Mothers’ Perceptions of Injury Prevention
3.3. Implementation Status of SPs and Active Attitudes toward Injury Prevention
3.4. Injury Risk Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. World Report on Child Injury Prevention; WHO: Geneva, Switzerland, 2008. [Google Scholar]
- Kendrick, D.; Mulvaney, C.A.; Ye, L.; Stevens, T.; Mytton, J.A.; Stewart-Brown, S. Parenting interventions for the prevention of unintentional injuries in childhood. Cochrane Database Syst. Rev. 2013, 2013, CD006020. [Google Scholar] [CrossRef] [PubMed]
- Culp, A.M.; Culp, R.E.; Anderson, J.W.; Carter, S. Health and safety intervention with first-time mothers. Health Educ. Res. 2007, 22, 285–294. [Google Scholar] [CrossRef]
- Kitzman, H.; Olds, D.L.; Henderson, C.R.; Hanks, C.; Cole, R.; Tatelbaum, R.; McConnochie, K.M.; Sidora, K.; Luckey, D.W.; Shaver, D.; et al. Effect of Prenatal and Infancy Home Visitation by Nurses on Pregnancy Outcomes, Childhood Injuries, and Repeated Childbearing:A Randomized Controlled Trial. JAMA 1997, 278, 644–652. [Google Scholar] [CrossRef] [PubMed]
- Flavin, M.P.; Dostaler, S.M.; Simpson, K.; Brison, R.J.; Pickett, W. Stages of Development and Injury Patterns in the Early Years: A Population-Based Analysis. BMC Public Health 2006, 6, 187. [Google Scholar] [CrossRef] [PubMed]
- Osawa, E.; Akiyama, Y.; Yamagata, Z.; Ojima, T. National Campaign to Promote Maternal and Child Health in 21st-century Japan: Healthy Parents and Children 21. J. Natl. Inst. Public Health 2019, 68, 2–7. [Google Scholar] [CrossRef]
- Ministry of Health, Labour and Welfare. Percentage of Municipalities Implementing Injury Prevention Measures. Final Report of Healthy Parents and Children 21. 2013. 126p. Available online: https://rhino.med.yamanashi.ac.jp/sukoyaka/pdf/saisyuuhyouka5.pdf (accessed on 27 March 2022).
- Honda, C.; Yamana, H.; Matsui, H.; Nagata, S.; Yasunaga, H.; Naruse, T. Age in Months and Birth Order in Infant Nonfatal Injuries: A Retrospective Cohort Study. Public Health Pract. 2020, 1, 100005. [Google Scholar] [CrossRef]
- Johnston, B.D.; Huebner, C.E.; Anderson, M.L.; Tyll, L.T.; Thompson, R.S. Healthy Steps in an Integrated Delivery System: Child and Parent Outcomes at 30 Months. Arch. Pediatr. Adolesc. Med. 2006, 160, 793–800. [Google Scholar] [CrossRef]
- Honda, C.; Naruse, T.; Yamana, H.; Yamamoto-Mitani, N. Infant Injury Prevention Education for Pregnant Women Attending Antenatal Class: A quasi-Experimental Study. Int. J. Environ. Res. Public Health 2021, 18, 9393. [Google Scholar] [CrossRef]
- Tokyo Fire Department. KyuKyu Hansou Data Kara Miru Nichijyou Seikatsu Jiko No Jittai [Emergency Transport Data Concerning Daily Life Accidents]. 2018. Available online: https://www.tfd.metro.tokyo.lg.jp/lfe/topics/201910/nichijoujiko/data/all.pdf (accessed on 27 March 2022).
- Rogers, R.W. A Protection Motivation Theory of Fear Appeals and Attitude Change. J. Psychol. 1975, 1, 93–114. [Google Scholar] [CrossRef]
- Ajzen, I. The Theory of Planned Behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- McBride, C.M.; Emmons, K.M.; Lipkus, I.M. Understanding the Potential of Teachable Moments: The Case of Smoking cessation. Health Educ. Res. 2003, 18, 156–170. [Google Scholar] [CrossRef]
- Phelan, S. Pregnancy: A “Teachable Moment” for Weight Control and Obesity Prevention. Am. J. Obstet. Gynecol. 2010, 202, 135.e1–135.e8. [Google Scholar] [CrossRef]
- Mack, K.A.; Gilchrist, J.; Ballesteros, M.F. Injuries among Infants Treated in Emergency Departments in the United States, 2001–2004. Pediatrics 2008, 121, 930–937. [Google Scholar] [CrossRef] [PubMed]
- Powell, E.C.; Tanz, R.R. Adjusting Our View of Injury Risk: The Burden of Nonfatal Injuries in Infancy. Pediatrics 2002, 110, 792–796. [Google Scholar] [CrossRef] [PubMed]
- Honda, C.; Naruse, T.; Yamamoto-Mitani, N. Pregnant Women’s Intentions to Implement Safety Practices for Preventing Infant Injury: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2020, 18, 24. [Google Scholar] [CrossRef] [PubMed]
- Rosen, B.N.; Peterson, L. Gender Differences in Children’s Outdoor Play Injuries: A Review and an Integration. Clin. Psychol. Rev. 1990, 10, 187–205. [Google Scholar] [CrossRef]
- Morrongiello, B.A.; Rennie, H. Why Do Boys Engage in More Risk Taking than Girls? The Role of Attributions, Beliefs, and Risk Appraisals. J. Pediatr. Psychol. 1998, 23, 33–43. [Google Scholar] [CrossRef]
- Block, J.H. Differential Premises Arising from Differential Socialization of the Sexes: Some Conjectures. Child Dev. 1983, 54, 1335–1354. [Google Scholar] [CrossRef]
- Fagot, B.I. The Influence of Sex of Child on Parental Reactions to Toddler Children. Child Dev. 1978, 49, 459–465. [Google Scholar] [CrossRef]
- Khanom, A.; Hill, R.A.; Brophy, S.; Morgan, K.; Rapport, F.; Lyons, R. Mothers’ Perspectives on the Delivery of Childhood Injury Messages: A Qualitative Study from the Growing up in Wales, Environments for Healthy Living Study (EHL). BMC Public Health 2013, 13, 806. [Google Scholar] [CrossRef]
- Honda, C.; Yoshioka-Maeda, K.; Iwasaki-Motegi, R. Child Abuse and Neglect Prevention by Public Health Nurses during the COVID-19 Pandemic in Japan. J. Adv. Nurs. 2020, 76, 2792–2793. [Google Scholar] [CrossRef] [PubMed]
- Gielen, A.C.; Bishai, D.M.; Omaki, E.; Shields, W.C.; McDonald, E.M.; Rizzutti, N.C.; Case, J.; Stevens, M.W.; Aitken, M.E. Results of an RCT in Two Pediatric Emergency Departments to Evaluate the Efficacy of an M-Health Educational App on Car Seat Use. Am. J. Prev. Med. 2018, 54, 746–755. [Google Scholar] [CrossRef] [PubMed]
- World health Organization. Japan Health System Review; Health Systems in Transition Vol. 8 No. 1; World Health Organization. Regional Office for South-East Asia: New Delhi, India, 2018; Available online: https://apps.who.int/iris/handle/10665/259941 (accessed on 27 March 2022).
- Cummings, P.; Rivara, F.P.; Thompson, R.S.; Reid, R.J. Ability of Parents to Recall the Injuries of Their Young Children. Inj. Prev. 2005, 11, 43–47. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Total (N = 68) | Intervention (N = 40) | Control (N = 28) | Regression | |||
|---|---|---|---|---|---|---|
| Variables | n(%) | n(%) | n(%) | OR | (95% CI) | p |
| Infant characteristics | ||||||
| Sex (male) | 30 (49.2) | 21 (56.8) | 9 (37.5) | 0.46 | (0.16–1.31) | 0.145 |
| Birth weight ≥ 2900 g | 34 (54.8) | 19 (50.0) | 15 (62.5) | 0.60 | (0.21–1.70) | 0.337 |
| Health condition requiring a hospital visit | 5 (7.4) | 3 (7.7) | 2 (7.1) | 0.95 | (0.15–6.08) | 0.956 |
| Mothers’ characteristics | ||||||
| Health condition requiring a hospital visit | 9 (13.2) | 4 (10.0) | 5 (17.9) | 1.96 | (0.48–8.05) | 0.353 |
| Subsequent children | 8 (11.8) | 2 (5.0) | 6 (21.4) | 0.19 | (0.036–1.04) | 0.056 |
| University or graduate school | 42 (61.8) | 23 (57.5) | 19 (67.9) | 0.64 | (0.23–1.76) | 0.388 |
| Full or part-time job | 36 (52.9) | 21 (52.5) | 15 (53.6) | 0.96 | (0.36–2.52) | 0.931 |
| Home environment | ||||||
| Annual household income (thousands of yen) ≥ 7000 | 43 (64.2) | 24 (61.5) | 19 (67.9) | 0.76 | (0.27–2.11) | 0.595 |
| Moved after child’s birth | 9 (13.2) | 5 (12.8) | 4 (14.3) | 1.17 | (0.28–4.77) | 0.831 |
| Smoking within the family | 14 (20.6) | 9 (22.5) | 5 (17.9) | 0.75 | (0.22–2.53) | 0.642 |
| All types of injury (0–24 months) | ||||||
| Medically attended | 24 (35.3) | 13 (32.5) | 11 (39.3) | 0.74 | (0.27–2.04) | 0.565 |
| Home-care | 55 (80.9) | 29 (72.5) | 26 (92.9) | 0.20 | (0.04–1.00) | 0.050 |
| Types of injury (0–24 months) | ||||||
| Fall | ||||||
| Medically attended | 9 (13.3) | 4 (10.0) | 5 (17.9) | 0.51 | (0.12–2.10) | 0.353 |
| Home-care | 36 (52.9) | 20 (50.0) | 16 (57.2) | 0.75 | (0.28–1.98) | 0.562 |
| Trip over | ||||||
| Medically attended | 5 (7.4) | 3 (7.5) | 2 (7.1) | 1.05 | (0.16–6.76) | 0.956 |
| Home-care | 21 (30.9) | 11 (27.5) | 10 (35.7) | 0.68 | (0.24–1.93) | 0.472 |
| Accidental ingestion/foreign body | ||||||
| Medically attended | 7(10.3) | 2 (5.0) | 5 (17.9) | 0.24 | (0.04–1.35) | 0.106 |
| Home-care | 8 (11.8) | 6 (15.0) | 2 (7.1) | 2.29 | (0.43–12.31) | 0.333 |
| Struck | ||||||
| Medically attended | 5 (7.4) | 3 (7.5) | 2 (7.1) | 1.05 | (0.16–6.76) | 0.956 |
| Home-care | 18 (26.5) | 11 (27.5) | 7 (25.0) | 1.14 | (0.38–3.42) | 0.818 |
| Caught between (objects) | ||||||
| Medically attended † | 2 (2.9) | 2 (5.0) | 0 (0.0) | - | - | - |
| Home-care | 16 (23.5) | 5 (12.5) | 11 (39.3) | 0.22 | (0.07–0.73) | 0.014 |
| Burn or scald | ||||||
| Medically attended † | 3 (4.4) | 3 (7.5) | 0 (0.0) | - | - | - |
| Home-care † | 2 (2.9) | 0 (0.0) | 2 (7.1) | - | - | - |
| Cut or pierce | ||||||
| Medically attended † | 1 (1.5) | 0 (0.0) | 1 (3.6) | - | - | - |
| Home-care | 9 (13.3) | 5 (12.5) | 4 (14.3) | 0.86 | (0.21–3.52) | 0.831 |
| Drowning | ||||||
| Medically attended † | 0 (0.0) | 0 (0.0) | 0 (0.0) | - | - | - |
| Home-care | 8 (11.8) | 3 (7.5) | 5 (17.9) | 0.37 | (0.08–1.71) | 0.204 |
| Suffocation | ||||||
| Medically attended † | 0 (0.0) | 0 (0.0) | 0 (0.0) | - | - | - |
| Home-care † | 0 (0.0) | 0 (0.0) | 0 (0.0) | - | - | - |
| Other | ||||||
| Medically attended † | 2 (2.9) | 0 0.0 | 2 (7.1) | - | - | - |
| Home-care † | 0 (0.0) | 0 (0.0) | 0 (0.0) | - | - | - |
| Total (N = 68) | Intervention (N = 40) | Control (N = 28) | Regression | |||
|---|---|---|---|---|---|---|
| Mean (SD) | Mean (SD) | Mean (SD) | Β | β | p | |
| Severity and probability of occurrence | 4.04 (1.17) | 4.25 (1.03) | 3.75 (1.29) | 0.500 | 0.213 | 0.081 |
| Parental responsibility | 4.34 (0.78) | 4.40 (0.67) | 4.25 (0.93) | 0.150 | 0.095 | 0.442 |
| Perceived behavioral control | 4.69 (0.62) | 4.75 (0.44) | 4.61 (0.83) | 0.143 | 0.113 | 0.361 |
| Intention to implement safety practice | 4.25 (0.76) | 4.35 (0.62) | 4.11 (0.92) | 0.243 | 0.158 | 0.197 |
| Total score (4–20) | 17.38 (2.18) | 17.85 (1.4) | 16.71 (2.85) | 1.136 | 0.258 | 0.033 |
| Total (N = 68) n (%) | Intervention (N = 40) n (%) | Control (N = 28) n (%) | Regression | |||
|---|---|---|---|---|---|---|
| OR | (95%CI) | p | ||||
| Safety practices | ||||||
| Fall prevention | 38 (55.9) | 19 (47.5) | 19 (67.9) | 0.43 | (0.16–1.17) | 0.099 |
| Trip prevention | 18 (26.5) | 12 (30.0) | 6 (21.4) | 1.57 | (0.52–4.85) | 0.432 |
| Accidental-ingestion prevention | 36 (52.9) | 20 (50.0) | 16 (57.1) | 0.75 | (0.28–1.98) | 0.562 |
| Burn prevention | 49 (72.1) | 31 (77.5) | 18 (64.3) | 1.91 | (0.66–5.59) | 0.235 |
| Pierce prevention | 41 (60.3) | 25 (62.5) | 16 (57.1) | 1.25 | (0.47–3.35) | 0.657 |
| Drowning prevention † | 63 (92.6) | 40 (100.0) | 23 (82.1) | - | - | - |
| Active attitudes toward injury prevention | ||||||
| Talked with family or friends | 53 (77.9) | 33 (82.5) | 20 (71.4) | 1.89 | (0.59–5.99) | 0.282 |
| Attended a lecture or study session | 18 (26.5) | 12 (30.0) | 6 (21.4) | 1.57 | (0.51–4.85) | 0.432 |
| Sent messages on social networking sites | 3 (4.4) | 1 (2.5) | 2 (7.1) | 0.33 | (0.29–3.87) | 0.380 |
| Medically Attended | Home-Care | |||||
|---|---|---|---|---|---|---|
| OR | (95% CI) | p | OR | (95% CI) | p | |
| Sex: Female (Male) | 4.68 | (1.34–16.30) | 0.015 | 1.44 | (0.35–5.88) | 0.616 |
| Mother’s educational level: University or Graduate School (Middle or high school) | 0.98 | (0.28–3.47) | 0.976 | 0.93 | (0.21–4.05) | 0.920 |
| Household annual income: ≥7000 (<7000) | 0.32 | (0.09–1.12) | 0.075 | 0.81 | (0.17–3.82) | 0.794 |
| Perception score | 1.17 | (0.79–1.73) | 0.442 | 0.55 | (0.31–0.96) | 0.035 |
| Intervention (control) | 0.69 | (0.20–2.47) | 0.573 | 0.24 | (0.04–1.28) | 0.094 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Honda, C.; Yoshioka-Maeda, K.; Fujii, H.; Iwasaki-Motegi, R.; Yamamoto-Mitani, N. Evaluation of Infant Injury Prevention Education Provided during Antenatal Classes after Two Years: A Pilot Prospective Cohort Study. Int. J. Environ. Res. Public Health 2022, 19, 7195. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19127195
Honda C, Yoshioka-Maeda K, Fujii H, Iwasaki-Motegi R, Yamamoto-Mitani N. Evaluation of Infant Injury Prevention Education Provided during Antenatal Classes after Two Years: A Pilot Prospective Cohort Study. International Journal of Environmental Research and Public Health. 2022; 19(12):7195. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19127195
Chicago/Turabian StyleHonda, Chikako, Kyoko Yoshioka-Maeda, Hitoshi Fujii, Riho Iwasaki-Motegi, and Noriko Yamamoto-Mitani. 2022. "Evaluation of Infant Injury Prevention Education Provided during Antenatal Classes after Two Years: A Pilot Prospective Cohort Study" International Journal of Environmental Research and Public Health 19, no. 12: 7195. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19127195