
Infant Care Practices, Caregiver Awareness of Safe Sleep Advice and Barriers to Implementation: A Scoping Review


Abstract
:1. Introduction
2. Review Methodology
3. Review Aim
4. Search Strategy
Eligibility Criteria
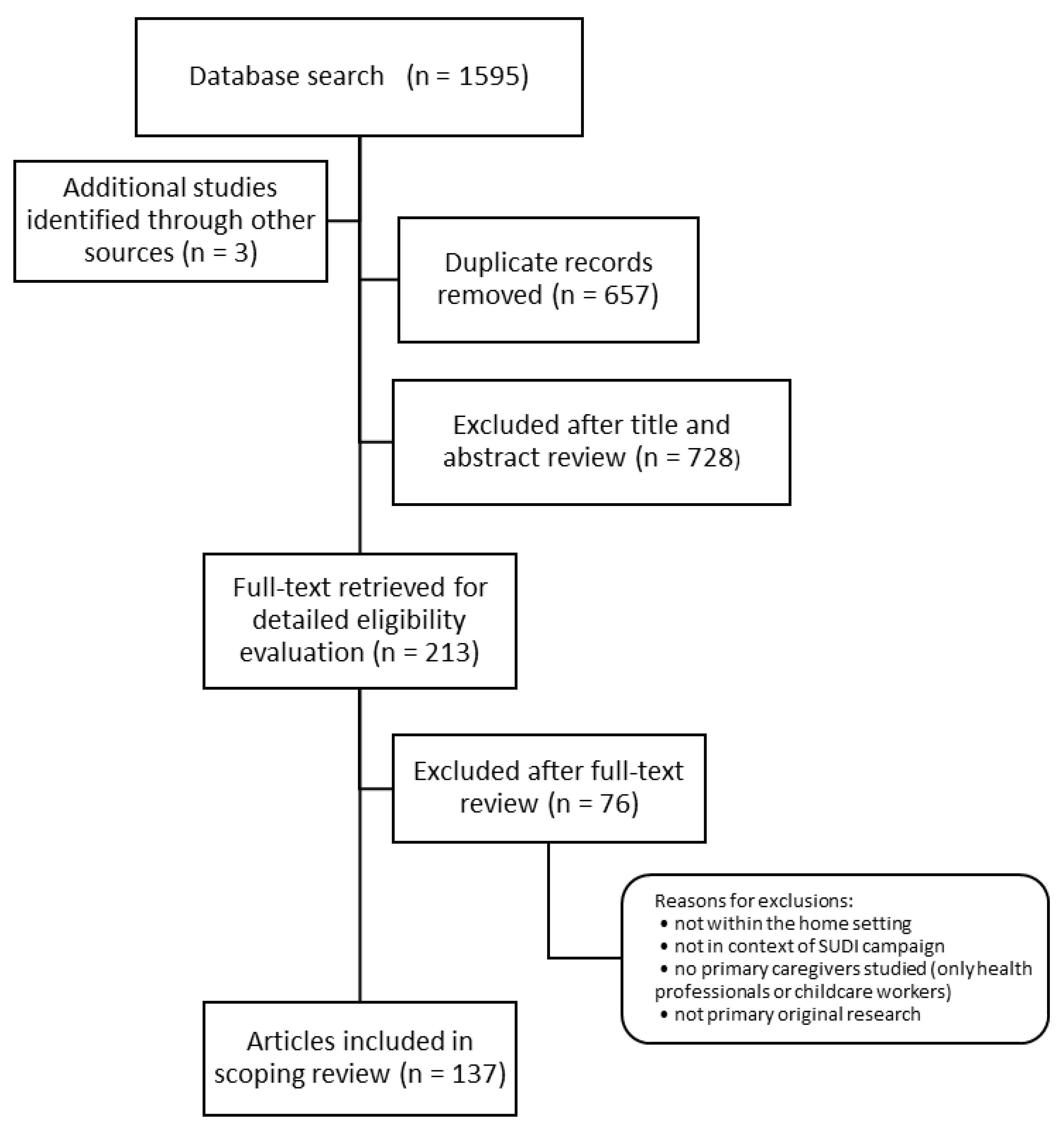
5. Screening and Source Selection
6. Data Extraction and Charting
7. Findings and Analysis
7.1. Eligible Study Characteristics
7.1.1. Study Designs
7.1.2. Study Country of Origins
7.1.3. Study Data Collection Periods
7.1.4. Study Participants
7.2. Analysis and Discussion of Target Outcome Measures
7.3. Prevalence of Key Modifiable Practices
7.3.1. Position Infant Placed to Sleep
7.3.2. Infant Smoke Exposure
7.3.3. Items in an Infant’s Sleeping Space
7.3.4. Infant’s Bed Type or Sleeping Surface
7.3.5. Infant Sleep Location: Room-Sharing and Surface Sharing
7.3.6. Breastfeeding
7.3.7. Summary of Prevalence Findings
7.4. Awareness of Infant Safe Sleep Messages
7.5. Challenges Implementing Safe Sleep Advice
8. Discussion of Review Findings
Limitations
9. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Organisation for Economic Co-Operation and Development (OECD). CO1.1: Infant Mortality. Available online: https://www.oecd.org/els/family/CO_1_1_Infant_mortality.pdf (accessed on 9 September 2021).
- Müller-Nordhorn, J.; Schneider, A.; Grittner, U.; Neumann, K.; Keil, T.; Willich, S.N.; Binting, S. International time trends in sudden unexpected infant death, 1969-2012. BMC Pediatr. 2020, 20, 377. [Google Scholar] [CrossRef] [PubMed]
- McEniery, J.; Cruice, D.; QPQC Members. Sudden Unexpected Death in Infancy. Available online: https://www.childrens.health.qld.gov.au/wp-content/uploads/PDF/qpqc/Sudden-unexpected-Death-in-infancy.pdf (accessed on 26 March 2019).
- Australian Bureau of Statistics. 3302.0—Deaths, Australia, 2016. Available online: http://www.abs.gov.au/AUSSTATS/[email protected]/DetailsPage/3302.02016?OpenDocument (accessed on 26 March 2019).
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Munn, Z.; Peters, M.D.J.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med. Res. Methodol. 2018, 18, 143. [Google Scholar] [CrossRef] [PubMed]
- Peters, M.D.J.; Marnie, C.; Tricco, A.C.; Pollock, D.; Munn, Z.; Alexander, L.; McInerney, P.; Godfrey, C.M.; Khalil, H. Updated methodological guidance for the conduct of scoping reviews. JBI Evid. Synth. 2020, 18, 2119–2126. [Google Scholar] [CrossRef] [PubMed]
- Bradbury-Jones, C.; Isham, L.; Morris, A.J.; Taylor, J. The “Neglected” Relationship Between Child Maltreatment and Oral Health? An International Scoping Review of Research. Trauma Violence Abus. 2019, 22, 265–276. [Google Scholar] [CrossRef] [Green Version]
- Buckley, L.; Berta, W.; Cleverley, K.; Medeiros, C.; Widger, K. What is known about paediatric nurse burnout: A scoping review. Hum. Resour. Health 2020, 18, 9. [Google Scholar] [CrossRef]
- Gjærde, L.K.; Hybschmann, J.; Dybdal, D.; Topperzer, M.K.; Schrøder, M.A.; Gibson, J.L.; Ramchandani, P.; Ginsberg, E.I.; Ottesen, B.; Frandsen, T.L.; et al. Play interventions for paediatric patients in hospital: A scoping review. BMJ Open 2021, 11, e051957. [Google Scholar] [CrossRef]
- Alahmadi, T.S.; Sobaihi, M.; Banjari, M.A.; Bakheet, K.M.A.; Modan Alghamdi, S.A.; Alharbi, A.S. Are Safe Sleep Practice Recommendations For Infants Being Applied Among Caregivers? Cureus 2020, 12, e12133. [Google Scholar] [CrossRef]
- Ball, H.L.; Moya, E.; Fairley, L.; Westman, J.; Oddie, S.; Wright, J. Infant care practices related to sudden infant death syndrome in South Asian and White British families in the UK. Paediatr. Perinat. Epidemiol. 2012, 26, 3–12. [Google Scholar] [CrossRef]
- Damato, E.G.; Haas, M.C.; Czeck, P.; Dowling, D.A.; Barsman, S.G. Safe Sleep Infant Care Practices Reported by Mothers of Twins. Adv. Neonatal Care 2016, 16, E3–E14. [Google Scholar] [CrossRef]
- Schluter, P.J.; Paterson, J.; Percival, T. Infant care practices associated with sudden infant death syndrome: Findings from the Pacific Islands Families study. J. Paediatr. Child Health 2007, 43, 388–393. [Google Scholar] [CrossRef] [PubMed]
- Schluter, P.J.; Young, J. Reducing the risk of SIDS: What infant care practices are being used by primary caregivers in Queensland? Neonatal Paediatr. Child Health Nurs. 2002, 5, 26–33. [Google Scholar]
- Cole, R.; Young, J.; Kearney, L.; Thompson, J.M.D. Infant care practices and parent uptake of safe sleep messages: A cross-sectional survey in Queensland, Australia. BMC Pediatrics 2020, 20, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baeis, M.G.; Miladinia, M.; Talayian, M.; Vahedi, M.; Vafayi, S.; Tashvighi, M. Prevalence and the relationship between characteristics and parental conditions with risk factors for Sudden Infant Death Syndrome (SIDS). Int. J. Pediatrics 2015, 3, 1135–1143. [Google Scholar] [CrossRef]
- Haas, M.C.; Dowling, D.; Damato, E.G. Adherence to Safe Sleep Recommendations by Families With Higher-order Multiples. Adv. Neonatal Care 2017, 17, 407–416. [Google Scholar] [CrossRef]
- Hutchison, L.; Thompson, J.M.D.; Mitchell, E.A. Infant care practices related to sudden unexpected death in infancy: A 2013 survey. N. Z. Med. J. 2015, 128, 15–22. [Google Scholar]
- Sawaguchi, T.; Nishida, H.; Fukui, F.; Horiuchi, T.; Nelson, E.A.S. Study on social responses (encouraging public awareness) to sudden infant death syndrome: Evaluation of SIDS prevention campaigns. Forensic Sci. Int. 2002, 130, S78–S80. [Google Scholar] [CrossRef]
- Shields, L.B.E.; Hunsaker, D.M.; Muldoon, S.; Corey, T.S.; Spivack, B.S. Risk factors associated with sudden unexplained infant death: A prospective study of infant care practices in Kentucky. Pediatrics 2005, 116, e13–e20. [Google Scholar] [CrossRef] [Green Version]
- Wilson, C.E. Cree infant care practices and sudden infant death syndrome. Can. J. Public Health 2000, 91, 133–136. [Google Scholar] [CrossRef]
- Specker, B.L.; Minett, M.; Beare, T.; Poppinga, N.; Carpenter, M.; Munger, J.; Strasser, K.; Ahrendt, L. Safe Sleep Behaviors Among South Dakota Mothers and the Role of the Healthcare Provider. S. D. Med. 2020, 73, 152–162. [Google Scholar]
- Cole, R.; Young, J.; Kearney, L.; Thompson, J.M.D. Awareness of infant safe sleep messages and associated care practices: Findings from an Australian cohort of families with young infants. BMJ Paediatr. Open 2021, 5, e000972. [Google Scholar] [CrossRef] [PubMed]
- Cole, R.; Young, J.; Kearney, L.; Thompson, J.M.D. Challenges parents encounter when implementing infant safe sleep advice. Acta Paediatr. 2021, 110, 3083–3093. [Google Scholar] [CrossRef] [PubMed]
- Ajao, T.I.; Oden, R.P.; Joyner, B.L.; Moon, R.Y. Decisions of black parents about infant bedding and sleep surfaces: A qualitative study. Pediatrics 2011, 128, 494–502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alzahrani, R.M.; Algethami, N.E.; Alharbi, A.; Alharbi, N.; Abbas, R.; Alqthami, L.M.; Alshardi, I.; Aljaid, M. Awareness of Sudden Infant Death Syndrome Among Saudi Arabian Women in 2019: A Cross-Sectional Study. Cureus 2020, 12, e9768. [Google Scholar] [CrossRef]
- Fernandes, S.C.; de Luca, F.; Fonseca, S.; Oliveira, F.; Areias, M. Sudden Infant Death Syndrome: What Healthcare Professionals and Parents Know About How to Prevent it in Portugal. Yale J. Biol. Med. 2020, 93, 475–485. [Google Scholar]
- Kuhlmann, Z.; Kuhlmann, S.; Schunn, C.; Klug, B.F.; Greaves, T.; Foster, M.; Ahlers-Schmidt, C.R. Collaborating with obstetrical providers to promote infant safe sleep guidelines. Sleep Health 2016, 2, 219–224. [Google Scholar] [CrossRef]
- Lau, A.; Hall, W. Safe sleep, day and night: Mothers’ experiences regarding infant sleep safety. J. Clin. Nurs. 2016, 25, 2816–2826. [Google Scholar] [CrossRef]
- Moon, R.Y.; Carlin, R.F.; Cornwell, B.; Mathews, A.; Oden, R.P.; Cheng, Y.I.; Fu, L.Y.; Wang, J. Implications of Mothers’ Social Networks for Risky Infant Sleep Practices. J. Pediatrics 2019, 212, 151–158.e152. [Google Scholar] [CrossRef]
- Pretorius, K.; Choi, E.; Kang, S.; Mackert, M. Sudden Infant Death Syndrome on Facebook: Qualitative Descriptive Content Analysis to Guide Prevention Efforts. J. Med. Internet Res. 2020, 22, e18474. [Google Scholar] [CrossRef]
- Raines, D.A. Factors That Influence Parents’ Adherence to Safe Sleep Guidelines. JOGNN-J. Obstet. Gynecol. Neonatal Nurs. 2018, 47, 316–323. [Google Scholar] [CrossRef]
- Varghese, S.; Gasalberti, D.; Ahern, K.; Chang, J.C. An analysis of attitude toward infant sleep safety and SIDS risk reduction behavior among caregivers of newborns and infants. J. Perinatol. 2015, 35, 970–973. [Google Scholar] [CrossRef] [PubMed]
- Kihlström, L.; Agu, N.; Dorjulus, B.; Prieto, C.; Chandran, V.; Alastre, S.; Rojas, D.; Birriel, P.C.; Marshall, J. Using Photovoice to Understand Perspectives on Safe Infant Sleep Practices among Caregivers Enrolled in Perinatal Home Visiting. J. Soc. Serv. Res. 2020, 47, 357–368. [Google Scholar] [CrossRef]
- Abdulrazzaq, Y.M.; Kendi, A.A.; Nagelkerke, N. Child care practice in the United Arab Emirates: The ESACCIPS study. Acta Paediatr. 2008, 97, 590–595. [Google Scholar] [CrossRef] [PubMed]
- Aitken, M.E.; Rose, A.; Mullins, S.H.; Miller, B.K.; Nick, T.; Rettiganti, M.; Nabaweesi, R.; Whiteside-Mansell, L. Grandmothers’ Beliefs and Practices in Infant Safe Sleep. Matern. Child Health J. 2016, 20, 1464–1471. [Google Scholar] [CrossRef] [Green Version]
- Anderson, E.S.; Jackson, A.; Wailoo, M.P.; Petersen, S.A. Child care decisions: Parental choice or chance? Child Care Health Dev. 2002, 28, 391–401. [Google Scholar] [CrossRef]
- Anuntaseree, W.; Mo-Suwan, L.; Vasiknanonte, P.; Kuasirikul, S.; Ma-a-Lee, A.; Choprapawon, C. Factors associated with bed sharing and sleep position in Thai neonates. Child Care Health Dev. 2008, 34, 482–490. [Google Scholar] [CrossRef]
- Ateah, C.A.; Hamelin, K.J. Maternal bedsharing practices, experiences, and awareness of risks. JOGNN J. Obstet. Gynecol. Neonatal Nurs. 2008, 37, 274–281. [Google Scholar] [CrossRef]
- Austin, J.E.; Nashban, C.J.; Doering, J.J.; Davies, W.H. Prevention Messages in Parent-Infant Bed-Sharing: Message Source, Credibility, and Effectiveness. Glob. Pediatric Health 2017, 4, 2333794x17743403. [Google Scholar] [CrossRef] [Green Version]
- Bailey, C. Breastfeeding mothers’ experiences of bedsharing: A qualitative study. Breastfeed. Rev. 2016, 24, 33–40. [Google Scholar]
- Bailey, C.; Tawia, S.; McGuire, E. Breastfeeding Duration and Infant Sleep Location in a Cohort of Volunteer Breastfeeding Counselors. J. Hum. Lact. 2020, 36, 354–364. [Google Scholar] [CrossRef]
- Ball, H.L.; Moya, E.; Fairley, L.; Westman, J.; Oddie, S.; Wright, J. Bed- and sofa-sharing practices in a UK biethnic population. Pediatrics 2012, 129, e673–e681. [Google Scholar] [CrossRef] [PubMed]
- Barbir, I.; Ball, H.L.; Zakarija-Grković, I. Parental knowledge of safe infant sleep and sudden infant death syndrome is inadequate in Croatia. Acta Paediatr. Int. J. Paediatr. 2020, 109, 1887–1888. [Google Scholar] [CrossRef] [PubMed]
- Beck, L.F.; Morrow, B.; Lipscomb, L.E.; Johnson, C.H.; Gaffield, M.E.; Rogers, M.; Gilbert, B.C. Prevalence of selected maternal behaviors and experiences, pregnancy risk assessment monitoring system (PRAMS), 1999. Morb. Mortal. Wkly. Rep. 2002, 51, 1–29. [Google Scholar]
- Bombard, J.M.; Kortsmit, K.; Warner, L.; Shapiro-Mendoza, C.K.; Cox, S.; Kroelinger, C.D.; Parks, S.E.; Dee, D.L.; D’Angelo, D.V.; Smith, R.A.; et al. Vital Signs: Trends and Disparities in Infant Safe Sleep Practices—United States, 2009–2015. Morb. Mortal. Wkly. Rep. 2018, 67, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Brenner, R.A.; Simons-Morton, B.G.; Bhaskar, B.; Revenis, M.; Das, A.; Clemens, J.D. Infant-parent bed sharing in an inner-city population. Arch. Pediatrics Adolesc. Med. 2003, 157, 33–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Broussard, D.; Sappenfield, W.; Goodman, D. The Black and White of Infant Back Sleeping and Infant Bed Sharing in Florida, 2004-2005. Matern. Child Health J. 2012, 16, 713–724. [Google Scholar] [CrossRef]
- Caraballo, M.; Shimasaki, S.; Johnston, K.; Tung, G.; Albright, K.; Halbower, A.C. Knowledge, Attitudes, and Risk for Sudden Unexpected Infant Death in Children of Adolescent Mothers: A Qualitative Study. J. Pediatrics 2016, 174, 78–83.e72. [Google Scholar] [CrossRef] [Green Version]
- Cesar, J.A.; Acevedo, J.D.; Kaczan, C.R.; Venzo, J.C.P.; Costa, L.R.; da Silva, L.C.M.; Neumann, N.A. Identifying mothers’ intention to place infant in supine sleep position: A population-based study. Cienc. E Saude Coletiva 2018, 23, 501–508. [Google Scholar] [CrossRef] [Green Version]
- Cesar, J.A.; Marmitt, L.P.; Carpena, M.X.; Pereira, F.G.; Neto, J.D.M.; Neumann, N.A.; Acevedo, J.D. Maternal Knowledge and Unsafe Baby Sleep Position: A Cross-Sectional Survey in Southern Brazil. Matern. Child Health J. 2019, 23, 183–190. [Google Scholar] [CrossRef]
- Chung, E.K.; Hung, Y.Y.; Marchi, K.; Chavez, G.F.; Braveman, P. Infant sleep position: Associated maternal and infant factors. Ambul. Pediatr. 2003, 3, 234–239. [Google Scholar] [CrossRef]
- Chung-Park, C.M.S. Knowledge, opinions, and practices of infant sleep position among parents. Mil. Med. 2012, 177, 235–239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cole, R.; Young, J.; Kearney, L.; Thompson, J.M.D. Reducing sleep-related infant mortality through understanding factors associated with breastfeeding duration: A cross-sectional survey. Breastfeed. Rev. 2020, 28, 7–19. [Google Scholar]
- Colson, E.R.; Stille, C.J.; Payton, J.; Bernstein, B.; Dworkin, P. Not yet ‘Back to Sleep’: Sleep position for infants in two inner-city clinics. Ambul. Child Health 2000, 6, 269–275. [Google Scholar] [CrossRef]
- Colson, E.R.; Bergman, D.M.; Shapiro, E.; Leventhal, J.H. Position for newborn sleep: Associations with parents’ perceptions of their nursery experience. Birth 2001, 28, 249–253. [Google Scholar] [CrossRef]
- Colson, E.R.; Levenson, S.; Rybin, D.; Calianos, C.; Margolis, A.; Colton, T.; Lister, G.; Corwin, M.J. Barriers to following the supine sleep recommendation among mothers at four centers for the Women, Infants, and Children Program. Pediatrics 2006, 118, e243–e250. [Google Scholar] [CrossRef]
- Colson, E.R.; Rybin, D.; Smith, L.A.; Colton, T.; Lister, G.; Corwin, M.J. Trends and factors associated with infant sleeping position: The national infant sleep position study, 1993–2007. Arch. Pediatrics Adolesc. Med. 2009, 163, 1122–1128. [Google Scholar] [CrossRef] [Green Version]
- Colson, E.R.; Willinger, M.; Rybin, D.; Heeren, T.; Smith, L.A.; Lister, G.; Corwin, M.J. Trends and factors associated with infant bed sharing, 1993-2010: The national infant sleep position study. JAMA Pediatr. 2013, 167, 1032–1037. [Google Scholar] [CrossRef] [Green Version]
- Colson, E.R.; Geller, N.L.; Heeren, T.; Corwin, M.J. Factors Associated With Choice of Infant Sleep Position. Pediatrics 2017, 140, e20170596. [Google Scholar] [CrossRef] [Green Version]
- Cornwell, B.; Yan, X.; Carlin, R.F.; Fu, L.; Wang, J.; Moon, R.Y. Social network influences on new mothers’ infant sleep adjustments. Soc. Sci. Med. 2021, 269, 113585. [Google Scholar] [CrossRef]
- Corwin, M.J.; Lesko, S.M.; Heeren, T.; Vezina, R.M.; Hunt, C.E.; Mandell, F.; McClain, M.; Mitchell, A.A. Secular changes in sleep position during infancy: 1995-1998. Pediatrics 2003, 111, 52–60. [Google Scholar] [CrossRef]
- Crane, D.; Ball, H.L. A qualitative study in parental perceptions and understanding of SIDS-reduction guidance in a UK bi-cultural urban community. BMC Pediatrics 2016, 16, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cullen, A.; Kiberd, B.; McDonnell, M.; Mehanni, M.; Matthews, T.G.; O’Regan, M. Sudden infant death syndrome—Are parents getting the message? Ir. J. Med. Sci. 2000, 169, 40–43. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, H.M.; Vally, H.; Bugeja, L. Bed-Sharing in the First 8 Weeks of Life: An Australian Study. Matern. Child Health J. 2018, 22, 556–564. [Google Scholar] [CrossRef] [PubMed]
- da Silva, B.G.C.; da Silveira, M.F.; de Oliveira, P.D.; Domingues, M.R.; Neumann, N.A.; Barros, F.C.; Bertoldi, A.D. Prevalence and associated factors of supine sleep position in 3-month-old infants: Findings from the 2015 Pelotas (Brazil) Birth Cohort. BMC Pediatrics 2019, 19, 165. [Google Scholar] [CrossRef]
- Douglas, T.A.; Buettner, P.G.; Whitehall, J. Maternal awareness of sudden infant death syndrome in North Queensland, Australia: An analysis of infant care practices. J. Paediatr. Child Health 2001, 37, 441–445. [Google Scholar] [CrossRef] [PubMed]
- Duzinski, S.V.; Yuma-Guerrero, P.J.; Fung, A.; Brown, J.M.; Wheeler, T.; Barczyk, A.N.; Lawson, K.A. Sleep behaviors of infants and young children: Associated demographic and acculturation characteristics among Hispanic teen mothers. J. Trauma Nurs. 2013, 20, 189–198. [Google Scholar] [CrossRef]
- Efe, E.; Ak, G. Turkish mothers’ who have preterm ınfants knowledge about risk factors of sudden ınfant death sendrome. HealthMED 2012, 6, 1137–1146. [Google Scholar]
- Eisenberg, S.R.; Bair-Merritt, M.H.; Colson, E.R.; Heeren, T.C.; Geller, N.L.; Corwin, M.J. Maternal Report of Advice Received for Infant Care. Pediatrics 2015, 136, E315–E322. [Google Scholar] [CrossRef] [Green Version]
- Epstein, J.; Jolly, C. Credibility gap? Parents’ beliefs about reducing the risk of cot death. Community Pr. 2009, 82, 21–24. [Google Scholar]
- Erdoğan, Ç.; Turan, T. Risky Behaviors of Mothers with Infants on Sudden Infant Death Syndrome in Turkey. J. Pediatr. Nurs. 2018, 38, e2–e6. [Google Scholar] [CrossRef]
- Erick-Peleti, S.; Paterson, J.; Williams, M. Pacific Islands Families Study: Maternal factors associated with cigarette smoking amongst a cohort of Pacific mothers with infants. N. Z. Med. J. 2007, 120, 113585. [Google Scholar]
- Ford, R.P.K.; Schluter, P.J.; Cowan, S. Changes to infant sleep practices in Canterbury. N. Z. Med. J. 2000, 113, 8–10. [Google Scholar] [PubMed]
- Fowler, A.J.; Evans, P.W.; Etchegaray, J.M.; Ottenbacher, A.; Arnold, C. Safe sleep practices and sudden infant death syndrome risk reduction: NICU and well-baby nursery graduates. Clin. Pediatrics 2013, 52, 1044–1053. [Google Scholar] [CrossRef] [PubMed]
- Galland, B.C.; Gray, A.; Sayers, R.M.; Heath, A.-L.M.; Lawrence, J.; Taylor, R.; Taylor, B.J. Safe sleep practices in a New Zealand community and development of a Sudden Unexpected Death in Infancy (SUDI) risk assessment instrument. BMC Pediatrics 2014, 14, 263. [Google Scholar] [CrossRef] [Green Version]
- Gaydos, L.M.; Blake, S.C.; Gazmararian, J.A.; Woodruff, W.; Thompson, W.W.; Dalmida, S.G. Revisiting Safe Sleep Recommendations for African-American Infants: Why Current Counseling is Insufficient. Matern. Child Health J. 2015, 19, 496–503. [Google Scholar] [CrossRef]
- Gibson, E.; Greenspan, J.S.; Rubin, S.; Dembofsky, C.A. Infant Sleep Position Practices 2 Years Into the “Back to Sleep” Campaign. Clin. Pediatrics 2000, 39, 285–289. [Google Scholar] [CrossRef]
- Goodstein, M.H.; Bell, T.; Krugman, S.D. Improving infant sleep safety through a comprehensive hospital-based program. Clin. Pediatrics 2015, 54, 212–221. [Google Scholar] [CrossRef]
- Hamadneh, S.; Kassab, M.; Hamadneh, J.; Amarin, Z. Sudden unexpected infant death in Jordan and the home environment. Pediatr. Int. 2016, 58, 1333–1336. [Google Scholar] [CrossRef]
- Hannan, K.E.; Smith, R.A.; Barfield, W.D.; Hwang, S.S. Association between Neonatal Intensive Care Unit Admission and Supine Sleep Positioning, Breastfeeding, and Postnatal Smoking among Mothers of Late Preterm Infants. J. Pediatrics 2020, 227, 114–120.e111. [Google Scholar] [CrossRef]
- Hauck, F.R.; Signore, C.; Fein, S.B.; Raju, T.N.K. Infant sleeping arrangements and practices during the first year of life. Pediatrics 2008, 122, S113–S120. [Google Scholar] [CrossRef] [Green Version]
- Hauck, F.R.; Tanabe, K.O.; McMurry, T.; Moon, R.Y. Evaluation of bedtime basics for babies: A national crib distribution program to reduce the risk of sleep-related sudden infant deaths. J. Community Health 2015, 40, 457–463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hirabayashi, M.; Yoshinaga, M.; Nomura, Y.; Ushinohama, H.; Sato, S.; Tauchi, N.; Horigome, H.; Takahashi, H.; Sumitomo, N.; Shiraishi, H.; et al. Environmental risk factors for sudden infant death syndrome in Japan. Eur. J. Pediatr. 2016, 175, 1921–1926. [Google Scholar] [CrossRef] [PubMed]
- Homer, C.; Armari, E.; Fowler, C. Bed-sharing with infants in a time of SIDS awareness. Neonatal Paediatr. Child Health Nurs. 2012, 15, 3–7. [Google Scholar]
- Hussain, S.; Lowell, G.S.; Roehler, D.R.; Quinlan, K.P.; Tandon, S.D.; Schwartz, L. You can have your breastmilk and safe sleep too: A preliminary analysis of infant safe sleep data in a Midwestern home visiting program. Inj. Epidemiol. 2018, 5, 14. [Google Scholar] [CrossRef] [PubMed]
- Hutchison, L.; Stewart, A.W.; Mitchell, E.A. SIDS-protective infant care practices among Auckland, New Zealand mothers. N. Z. Med. J. 2006, 119, U2365. [Google Scholar]
- Hutchison, L.; Stewart, A.; Mitchell, E. Infant sleep position, head shape concerns, and sleep positioning devices. J. Paediatr. Child Health 2007, 43, 243–248. [Google Scholar] [CrossRef]
- Hutchison, B.L.; Stewart, A.W.; Mitchell, E.A. The prevalence of cobedding and SIDS-related child care practices in twins. Eur. J. Pediatr. 2010, 169, 1477–1485. [Google Scholar] [CrossRef]
- Hwang, S.S.; Barfield, W.D.; Smith, R.A.; Morrow, B.; Shapiro-Mendoza, C.K.; Prince, C.B.; Smith, V.C.; McCormick, M.C. Discharge timing, outpatient follow-up, and home care of late-preterm and early-term infants. Pediatrics 2013, 132, 101–108. [Google Scholar] [CrossRef] [Green Version]
- Hwang, S.S.; Smith, R.A.; Barfield, W.D.; Smith, V.C.; McCormick, M.C.; Williams, M.A. Supine sleep positioning in preterm and term infants after hospital discharge from 2000 to 2011. J. Perinatol. 2016, 36, 787–793. [Google Scholar] [CrossRef]
- Inbar, Z.; Meibar, R.; Shehada, S.; Irena, V.; Rubin, S.; Rishpon, S. ‘Back to sleep’: Parents compliance with the recommendation on the most appropriate sleeping position of infants, Haifa District, Israel, 2001. Prev. Med. 2005, 40, 765–768. [Google Scholar] [CrossRef]
- Joyner, B.L.; Oden, R.P.; Moon, R.Y. Reasons for Pacifier Use and Non-Use in African-Americans: Does Knowledge of Reduced SIDS Risk Change Parents’ Minds? J. Immigr. Minor. Health 2016, 18, 402–410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kelmanson, I. Swaddling: Maternal Option and Sleep Behaviour in Two-month-old Infants. Child Care Pract. 2013, 19, 36–48. [Google Scholar] [CrossRef]
- Konstat-Korzenny, E.; Cohen-Welch, A.; Fonseca-Portilla, R.; Morgenstern-Kaplan, D. Sudden Unexpected Infant Death: Review and Analysis of Adherence to Recommendations. Cureus 2019, 11, e6076. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krouse, A.; Craig, J.; Watson, U.; Matthews, Z.; Kolski, G.; Isola, K. Bed-sharing influences, attitudes, and practices: Implications for promoting safe infant sleep. J. Child Health Care 2012, 16, 274–283. [Google Scholar] [CrossRef]
- Lahr, M.B.; Rosenberg, K.D.; Lapidus, J.A. Health departments do it better: Prenatal care site and prone infant sleep position. Matern. Child Health J. 2005, 9, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Lahr, M.B.; Rosenberg, K.D.; Lapidus, J.A. Bedsharing and maternal smoking in a population-based survey of new mothers. Pediatrics 2005, 116, e530–e542. [Google Scholar] [CrossRef] [Green Version]
- Lahr, M.B.; Rosenberg, K.D.; Lapidus, J.A. Maternal-infant bedsharing: Risk factors for bedsharing in a population-based survey of new mothers and implications for SIDS risk reduction. Matern. Child Health J. 2007, 11, 277–286. [Google Scholar] [CrossRef]
- Martiniuk, A.; Jacob, J.; Faruqui, N.; Yu, W. Positional plagiocephaly reduces parental adherence to SIDS Guidelines and inundates the health system. Child Care Health Dev. 2016, 42, 941–950. [Google Scholar] [CrossRef]
- Mathews, A.; Joyner, B.; Oden, R.; Alamo, I.; Moon, R. Comparison of Infant Sleep Practices in African-American and US Hispanic Families: Implications for Sleep-Related Infant Death. J. Immigr. Minority Health 2015, 17, 834–842. [Google Scholar] [CrossRef] [Green Version]
- Miladinia, M.; Baraz, S.; Nouri, E.M. Sudden infant death syndrome: Risk factors and the relationship between them. Int. J. Pediatrics 2015, 3, 1103–1110. [Google Scholar] [CrossRef]
- Möllborg, P.; Wennergren, G.; Norvenius, S.G.; Alm, B. Bed-sharing among six-month-old infants in western Sweden. Acta Paediatr. Int. J. Paediatr. 2011, 100, 226–230. [Google Scholar] [CrossRef] [PubMed]
- Moon, R.Y.; Oden, R.P.; Joyner, B.L.; Ajao, T.I. Qualitative analysis of beliefs and perceptions about sudden infant death syndrome in African-American mothers: Implications for safe sleep recommendations. J. Pediatrics 2010, 157, 92–97. [Google Scholar] [CrossRef] [PubMed]
- Moon, R.Y.; Omron, R. Determinants of infant sleep position in an urban population. Clin. Pediatrics 2002, 41, 569–573. [Google Scholar] [CrossRef] [PubMed]
- Nelson, E.A.; Taylor, B.J.; ICCPS Study Group. International Child Care Practices Study: Infant sleep position and parental smoking. Early Hum. Dev. 2001, 64, 7–20. [Google Scholar] [CrossRef]
- Nelson, E.A.S.; Taylor, B.J.; Jenik, A.; Vance, J.; Walmsley, K.; Pollard, K.; Freemantle, M.; Ewing, D.; Einspieler, C.; Engele, H.; et al. International Child Care Practices Study: Infant sleeping environment. Early Hum. Dev. 2001, 62, 43–55. [Google Scholar] [CrossRef]
- Nelson, E.A.S.; Yu, L.; Williams, S. International Child Care Practices Study: Breastfeeding and pacifier use. J. Hum. Lact. 2005, 21, 289–295. [Google Scholar] [CrossRef]
- Norton, P.J.; Grellner, K.W. A Retrospective Study on Infant Bed-Sharing in a Clinical Practice Population. Matern. Child Health J. 2011, 15, 507–513. [Google Scholar] [CrossRef]
- Nongkynrih, R.; Cutinho, S.P.; D’Almeida, V. A Study on Knowledge and Practice on Maternal Bed sharing Among Mothers in A Selected Hospital at Mangalore. Nitte Univ. J. Health Sci. 2017, 7, 3–7. [Google Scholar] [CrossRef] [Green Version]
- Oden, R.P.; Powell, C.; Sims, A.; Weisman, J.; Joyner, B.L.; Moon, R.Y. Swaddling: Will it get babies onto their backs for sleep? Clin. Pediatrics 2012, 51, 254–259. [Google Scholar] [CrossRef]
- Osberg, S.; Kalstad, T.G.; Stray-Pedersen, A. Norwegian parents avoid placing infants in prone sleeping positions but frequently share beds in hazardous ways. Acta Paediatr. 2021, 110, 2119–2125. [Google Scholar] [CrossRef]
- Panaretto, K.S.; Smallwood, V.E.; Cole, P.; Elston, J.; Whitehall, J.S. Sudden infant death syndrome risk factors in north Queensland: A survey of infant-care practices in Indigenous and non-Indigenous women. J. Paediatr. Child Health 2002, 38, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Paterson, J.; Tukuitonga, C.; Butler, S.; Williams, M. Infant bed-sharing among Pacific families in New Zealand. N. Z. Med. J. 2002, 115, 241–243. [Google Scholar] [PubMed]
- Pease, A.; Ingram, J.; Blair, P.S.; Fleming, P.J. Factors influencing maternal decision-making for the infant sleep environment in families at higher risk of SIDS: A qualitative study. BMJ Paediatr. Open 2017, 1, e000133. [Google Scholar] [CrossRef] [PubMed]
- Pease, A.S.; Blair, P.S.; Ingram, J.; Fleming, P.J. Mothers’ knowledge and attitudes to sudden infant death syndrome risk reduction messages: Results from a UK survey. Arch. Dis. Child. 2018, 103, 33–38. [Google Scholar] [CrossRef] [Green Version]
- Phares, T.M.; Morrow, B.; Lansky, A.; Barfield, W.D.; Prince, C.B.; Marchi, K.S.; Braveman, P.A.; Williams, L.M.; Kinniburgh, B. Surveillance for disparities in maternal health-related behaviors-selected states, Pregnancy Risk Assessment Monitoring System (PRAMS), 2000–2001. Morb. Mortal. Wkly. Rep. 2004, 53, 1–13. [Google Scholar]
- Provini, L.E.; Corwin, M.J.; Geller, N.L.; Heeren, T.C.; Moon, R.Y.; Rybin, D.V.; Shapiro-Mendoza, C.K.; Colson, E.R. Differences in Infant Care Practices and Smoking among Hispanic Mothers Living in the United States. J. Pediatrics 2017, 182, 321–326.e321. [Google Scholar] [CrossRef] [Green Version]
- Roberts, H.; Upton, D. New mothers’ knowledge of sudden infant death syndrome. Br. J. Midwifery 2000, 8, 147–150. [Google Scholar] [CrossRef]
- Robida, D.; Moon, R.Y. Factors influencing infant sleep position: Decisions do not differ by SES in African-American families. Arch. Dis. Child. 2012, 97, 900–905. [Google Scholar] [CrossRef]
- Rohana, J.; Ishak, S.; Wan Nurulhuda, W.M.Z. Sudden infant death syndrome: Knowledge and practise in parents of preterm infants. Pediatr. Int. 2018, 60, 710–713. [Google Scholar] [CrossRef]
- Ruiz Botia, I.; Cassanello Peñarroya, P.; Díez Izquierdo, A.; Martínez Sánchez, J.M.; Balaguer Santamaria, A. Sudden infant death syndrome: Do the parents follow the recommendations? An. Pediatr. 2020, 92, 222–228. [Google Scholar] [CrossRef]
- Salm Ward, T.; Ngui, E. Factors Associated with Bed-Sharing for African American and White Mothers in Wisconsin. Matern. Child Health J. 2015, 19, 720–732. [Google Scholar] [CrossRef] [PubMed]
- Salm Ward, T.C.; Kanu, F.A.; Anderson, A.K. Trends and Factors Associated with Breastfeeding and Infant Sleep Practices in Georgia. J. Community Health 2018, 43, 496–507. [Google Scholar] [CrossRef] [PubMed]
- Salm Ward, T.C.; Robb, S.W.; Kanu, F.A. Prevalence and Characteristics of Bed-Sharing Among Black and White Infants in Georgia. Matern. Child Health J. 2016, 20, 347–362. [Google Scholar] [CrossRef] [PubMed]
- Shapiro-Mendoza, C.K.; Colson, E.R.; Willinger, M.; Rybin, D.V.; Camperlengo, L.; Corwin, M.J. Trends in infant bedding use: National Infant Sleep Position Study, 1993–2010. Pediatrics 2015, 135, 10–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sivan, Y.; Reisner, S.; Amitai, Y.; Wasser, J.; Nehama, H.; Tauman, R. Effect of religious observance on infants’ sleep position in the Jewish population. J. Paediatr. Child Health 2004, 40, 534–539. [Google Scholar] [CrossRef]
- Smith, M.G.; Liu, J.H.; Helms, K.H.; Wilkerson, K.L. Racial differences in trends and predictors of infant sleep positioning in South Carolina, 1996-2007. Matern. Child Health J. 2012, 16, 72–82. [Google Scholar] [CrossRef]
- Smith, L.A.; Geller, N.L.; Kellams, A.L.; Colson, E.R.; Rybin, D.V.; Heeren, T.; Corwin, M.J. Infant Sleep Location and Breastfeeding Practices in the United States, 2011-2014. Acad. Pediatr. 2016, 16, 540–549. [Google Scholar] [CrossRef]
- Smylie, J.; Fell, D.B.; Chalmers, B.; Sauve, R.; Royle, C.; Allan, B.; O’Campo, P.; Maternity Experiences Study, G. Socioeconomic Position and Factors Associated With Use of a Nonsupine Infant Sleep Position: Findings From the Canadian Maternity Experiences Survey. Am. J. Public Health 2014, 104, 539–547. [Google Scholar] [CrossRef]
- Sperhake, J.P.; Zimmermann, I.; Püschel, K. Current recommendations on infants’ sleeping position are being followed-initial results of a population-based sentinel study on risk factors for SIDS, 1996-2006, in Hamburg, Germany. Int. J. Leg. Med. 2009, 123, 41–45. [Google Scholar] [CrossRef]
- Strömberg Celind, F.; Wennergren, G.; Möllborg, P.; Goksör, E.; Alm, B. Area-based study shows most parents follow advice to reduce risk of sudden infant death syndrome. Acta Paediatr. 2017, 106, 579–585. [Google Scholar] [CrossRef] [Green Version]
- Tipene-Leach, D.; Hutchison, L.; Tangiora, A.; Rea, C.; White, R.; Stewart, A.; Mitchell, E. SIDS-related knowledge and infant care practices among Māori mothers. N. Z. Med. J. 2010, 123, 88–96. [Google Scholar] [PubMed]
- Tirosh, E.; Becker, T.; Mansour, Y.; Cohen, A.; Jaffe, M. Sleep position, bedding and heating practices in high- and low-risk ethnic groups for unexpected death in infancy (UDI). Eur. J. Epidemiol. 2000, 16, 281–286. [Google Scholar] [CrossRef] [PubMed]
- Tully, K.; Holditch-Davis, D.; Brandon, D. The Relationship Between Planned and Reported Home Infant Sleep Locations Among Mothers of Late Preterm and Term Infants. Matern. Child Health J. 2015, 19, 1616–1623. [Google Scholar] [CrossRef] [PubMed]
- van Sleuwen, B.E.; L’Hoir, M.P.; Engelberts, A.C.; Westers, P.; Schulpen, T.W.J. Infant care practices related to cot death in Turkish and Moroccan families in the Netherlands. Arch. Dis. Child. 2003, 88, 784–788. [Google Scholar] [CrossRef] [Green Version]
- Vernacchio, L.; Corwin, M.J.; Lesko, S.M.; Vezina, R.M.; Hunt, C.E.; Hoffman, H.J.; Willinger, M.; Mitchell, A.A. Sleep position of low birth weight infants. Pediatrics 2003, 111, 633–640. [Google Scholar] [CrossRef]
- Vilvens, H.L.; Vaughn, L.M.; Southworth, H.; Denny, S.A.; Gittelman, M.A. Personalising Safe Sleep Messaging for Infant Caregivers in the United States. Health Soc. Care Community 2020, 28, 891–902. [Google Scholar] [CrossRef]
- Von Kohorn, I.; Corwin, M.J.; Rybin, D.V.; Heeren, T.C.; Lister, G.; Colson, E.R. Influence of prior advice and beliefs of mothers on infant sleep position. Arch. Pediatrics Adolesc. Med. 2010, 164, 363–369. [Google Scholar] [CrossRef]
- Walcott, R.L.; Salm Ward, T.C.; Ingels, J.B.; Llewellyn, N.A.; Miller, T.J.; Corso, P.S. A Statewide Hospital-Based Safe Infant Sleep Initiative: Measurement of Parental Knowledge and Behavior. J. Community Health 2018, 43, 534–542. [Google Scholar] [CrossRef] [Green Version]
- Wennergren, G.; Strömberg Celind, F.; Goksör, E.; Alm, B. Swedish survey of infant sleep practices showed increased bed-sharing and positive associations with breastfeeding. Acta Paediatr. 2021, 110, 1835–1841. [Google Scholar] [CrossRef]
- Willinger, M.; Ko, C.W.; Hoffman, H.J.; Kessler, R.C.; Corwin, M.J. Factors associated with caregivers’ choice of infant sleep position, 1994-1998: The national infant sleep position study. J. Am. Med. Assoc. 2000, 283, 2135–2142. [Google Scholar] [CrossRef] [Green Version]
- Woods, N.K.; Ahlers-Schmidt, C.R.; Wipperman, J.; Williams, T. Comparing Self-Reported Infant Safe Sleep From Community- and Health Care-Based Settings. J. Prim. Care Community Health 2015, 6, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Wright, C.; Beard, H.; Cox, J.; Scott, P.; Miller, J. Parents’ choice of non-supine sleep position for newborns: A cross-sectional study. Br. J. Midwifery 2014, 22, 625–629. [Google Scholar] [CrossRef]
- Yikilkan, H.; Ünalan, P.C.; Cakir, E.; Ersu, R.H.; Cifcili, S.; Akman, M.; Uzuner, A.; Dagli, E. Sudden infant death syndrome: How much mothers and health professionals know. Pediatr. Int. 2011, 53, 24–28. [Google Scholar] [CrossRef] [PubMed]
- Zoucha, R.; Walters, C.A.; Colbert, A.M.; Carlins, E.; Smith, E. Exploring Safe Sleep and SIDS Risk Perception in an African-American Community: Focused Ethnography. Public Health Nurs. 2016, 33, 206–213. [Google Scholar] [CrossRef]
- Young, J.; Watson, K.; Ellis, L.; Raven, L. Responding to evidence: Breastfeed baby if you can-the sixth public health recommendation to reduce the risk of sudden and unexpected death in infancy. Breastfeed. Rev. 2012, 20, 7–15. [Google Scholar]
- ISPID Epidemiology and Education Working Group. Guidelines on Risk Reduction: Safe Infant Sleep Recommenations. Available online: https://www.ispid.org/fileadmin/user_upload/textfiles/ISPID_Safe_Sleep_Recommendations_17_May_2021__final_version_.pdf (accessed on 12 April 2022).
- Mitchell, E.A.; Freemantle, J.; Young, J.; Byard, R.W. Scientific consensus forum to review the evidence underpinning the recommendations of the Australian SIDS and Kids Safe Sleeping Health Promotion Programme—October 2010. J. Paediatr. Child Health 2012, 48, 626–633. [Google Scholar] [CrossRef]
- Ball, H.L.; Volpe, L.E. Sudden Infant Death Syndrome (SIDS) risk reduction and infant sleep location—Moving the discussion forward. Soc. Sci. Med. 2013, 79, 84–91. [Google Scholar] [CrossRef] [Green Version]
- Fleming, P.J.; Blair, P.S.; Pease, A. Sudden unexpected death in infancy: Aetiology, pathophysiology, epidemiology and prevention in 2015. Arch. Dis. Child. 2015, 100, 984–988. [Google Scholar] [CrossRef]
- Well Child Tamariki Ora. Keep Your Baby Safe during Sleep. Available online: https://www.healthed.govt.nz/system/files/resource-files/HE1228%20Keep%20your%20baby%20safe%20during%20sleep.pdf (accessed on 15 December 2016).
- Moon, R.Y.; AAP Task Force on Sudden Infant Death Syndrome. SIDS and other sleep-related infant deaths: Updated 2016 recommendations for a safe infant sleeping environment. Pediatrics 2016, 138, e20162938. [Google Scholar] [CrossRef] [Green Version]
- Lullaby Trust. Safer Sleep for Babies: A Guide for Parents. Available online: https://www.lullabytrust.org.uk/wp-content/uploads/Safer-Sleep-for-babies-a-guide-for-parents.pdf (accessed on 30 April 2019).
- Hwang, S.S.; Lu, E.; Cui, X.; Diop, H.; Barfield, W.D.; Manning, S.E. Home care practices for preterm and term infants after hospital discharge in Massachusetts, 2007 to 2010. J. Perinatol. 2015, 35, 880–884. [Google Scholar] [CrossRef] [Green Version]
- Red Nose. Safe Sleeping Brochure. Available online: https://rednose.com.au/downloads/Safe_Sleeping_Brochure.pdf (accessed on 15 December 2016).
- Vennemann, M.M.; Hense, H.W.; Bajanowski, T.; Blair, P.S.; Complojer, C.; Moon, R.Y.; Kiechl-Kohlendorfer, U. Bed sharing and the risk of sudden infant death syndrome: Can we resolve the debate? J. Pediatrics 2012, 160, 44–48.e42. [Google Scholar] [CrossRef] [PubMed]
- Red Nose. Is It Safe to Use Products Designed to Keep Baby in a Particular Position during Sleep? Available online: https://rednose.com.au/article/is-it-safe-to-use-products-designed-to-keep-baby-in-a-particular-position (accessed on 22 December 2016).
- Horne, R.S.; Hauck, F.R.; Moon, R.Y. Sudden infant death syndrome and advice for safe sleeping. Br. Med. J. 2015, 350, 1–7. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization [WHO]; United Nations Children’s Fund [UNICEF]. Global Nutrition Targets 2025: Breastfeeding Policy Brief (WHO/NMH/NHD/14.7). Available online: https://apps.who.int/iris/bitstream/handle/10665/149022/WHO_NMH_NHD_14.7_eng.pdf (accessed on 26 March 2019).
- Thompson, J.M.D.; Tanabe, K.; Moon, R.Y.; Mitchell, E.A.; McGarvey, C.; Tappin, D.; Blair, P.S.; Hauck, F.R. Duration of Breastfeeding and Risk of SIDS: An Individual Participant Data Meta-analysis. Pediatrics 2017, 140, e20171324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pease, A.; Garstang, J.J.; Ellis, C.; Watson, D.; Ingram, J.; Cabral, C.; Blair, P.S.; Fleming, P.J. Decision-making for the infant sleep environment among families with children considered to be at risk of sudden unexpected death in infancy: A systematic review and qualitative metasynthesis. BMJ Paediatr. Open 2021, 5, e000983. [Google Scholar] [CrossRef]
- Shipstone, R.A.; Young, J.; Kearney, L.; Thompson, J.M.D. Prevalence of risk factors for sudden infant death among Indigenous and non-Indigenous people in Australia. Acta Paediatr. 2020, 109, 2614–2626. [Google Scholar] [CrossRef]
- Shipstone, R.A.; Young, J.; Thompson, J.M.D. The real divide: The use of algorithm-derived Indigenous status to measure disparities in sudden unexpected deaths in infancy in Queensland. Aust. N. Z. J. Public Health 2019, 43, 570–576. [Google Scholar] [CrossRef] [Green Version]
- Moon, R.Y.; Hauck, F.R.; Colson, E.R. Safe Infant Sleep Interventions: What is the Evidence for Successful Behavior Change? Curr. Pediatric Rev. 2016, 12, 67–75. [Google Scholar] [CrossRef] [Green Version]
- Pease, A. Factors Influencing Infant Care Practices in the Sleep Environment among Families at High Risk of Sudden Infant Death Syndrome; University of Bristol: Bristol, UK, 2015. [Google Scholar]
- Shipstone, R. Extending the Reach: A Retrospective Cohort Study of Sudden Unexpected Deaths in Infancy in Queensland, Australia; University of the Sunshine Coast: Queensland, Australia, 2021. [Google Scholar]


{kind=link}
| Population | Sample cohort terms | Caregiver* OR parent* OR mother* OR maternal OR women |
| AND | ||
| Study type terms | “cross-sectional” OR survey OR questionnaire OR interview | |
| AND | ||
| Context | SUDI terms | sids OR sudi OR suid OR “sudden infant death” OR “unexplained infant death*” OR “sleep-related death*” OR “cot death*” OR “crib death*” |
| AND | ||
| Concept | Uptake and engagement with safe sleep advice (i.e., prevalence of care practices, awareness of messages, challenges implementing advice) | prevalence OR “infant care” OR practice* OR knowledge OR awareness OR understand* OR recommendation* OR advice OR message* OR challeng* OR barrier* OR difficult* OR facilitator* OR enabler* OR concern* |
| Inclusion Criteria |
|
| Exclusion Criteria |
|
| Prevalence | Awareness | Challenges | ||||||||
| Article | Sleep Position | Smoking | Items in Sleep Area | Bed Type or Surface | Room Location | Surface Sharing | Breast Feeding | Other Practice | ||
| Abdulrazzaq et al. (2008) [36] | ● | ● | ● | ● | ● | |||||
| Aitken et al. (2016) [37] | ● | ● | ● | |||||||
| Ajao et al. (2011) [26] | ● | |||||||||
| Alahmadi et al. (2020) [11] | ● | ● | ● | ● | ● | ● | ● | ● | ● | |
| Alzahrani et al. (2020) [27] | ● | |||||||||
| Anderson et al. (2002) [38] | ● | ● | ● | ● | ● | ● | ● | |||
| Anuntaseree et al. (2008) [39] | ● | ● | ● | |||||||
| Ateah and Hamelin (2008) [40] | ● | ● | ● | ● | ||||||
| Austin et al. (2017) [41] | ● | |||||||||
| Baeis et al. (2015) [17] | ● | ● | ● | ● | ● | ● | ||||
| Bailey (2016) [42] | ● | ● | ● | |||||||
| Bailey et al. (2020) [43] | ● | ● | ● | |||||||
| Ball et al. (2012a) [12] | ● | ● | ● | ● | ● | ● | ● | ● | ||
| Ball et al. (2012b) [44] | ● | ● | ● | ● | ||||||
| Barbir et al. (2020) [45] | ● | ● | ● | ● | ● | |||||
| Beck et al. (2002) [46] | ● | ● | ● | |||||||
| Bombard et al. (2018) [47] | ● | ● | ● | ● | ||||||
| Brenner et al. (2003) [48] | ● | ● | ● | ● | ● | ● | ||||
| Broussard et al. (2012) [49] | ● | ● | ● | ● | ||||||
| Caraballo et al. (2016) [50] | ● | ● | ● | ● | ||||||
| Cesar et al. (2018) [51] | ● | ● | ||||||||
| Cesar et al. (2019) [52] | ● | ● | ● | |||||||
| Chung et al. (2003) [53] | ● | ● | ● | |||||||
| Chung-Park (2012) [54] | ● | ● | ● | ● | ||||||
| Cole et al. (2020) [16] | ● | ● | ● | ● | ● | ● | ● | ● | ||
| Cole et al. (2020) [55] | ● | ● | ● | ● | ● | ● | ||||
| Cole et al. (2021) [24] | ● | ● | ● | ● | ● | ● | ● | |||
| Cole et al. (2021) [25] | ● | ● | ● | ● | ● | ● | ● | |||
| Colson et al. (2000) [56] | ● | ● | ● | |||||||
| Colson et al. (2001) [57] | ● | ● | ● | |||||||
| Colson et al. (2006) [58] | ● | ● | ||||||||
| Colson et al. (2009) [59] | ● | ● | ● | |||||||
| Colson et al. (2013) [60] | ● | ● | ● | ● | ||||||
| Colson et al. (2017) [61] | ● | ● | ● | |||||||
| Cornwell et al. (2021) [62] | ● | ● | ||||||||
| Corwin et al. (2003) [63] | ● | |||||||||
| Crane and Ball (2016) [64] | ● | ● | ● | ● | ● | ● | ● | |||
| Cullen et al. (2000) [65] | ● | ● | ● | ● | ● | ● | ||||
| Cunningham et al. (2018) [66] | ● | ● | ● | ● | ||||||
| da Silva et al. (2019) [67] | ● | ● | ● | |||||||
| Damato et al. (2016) [13] | ● | ● | ● | ● | ● | ● | ● | |||
| Douglas et al. (2001) [68] | ● | ● | ● | ● | ● | ● | ||||
| Duzinski et al. (2013) [69] | ● | ● | ● | ● | ||||||
| Efe and Ak (2012) [70] | ● | ● | ● | ● | ||||||
| Eisenberg et al. (2015) [71] | ● | ● | ● | ● | ||||||
| Epstein and Jolly (2009) [72] | ● | ● | ● | ● | ● | ● | ||||
| Erdoğan and Turan (2018) [73] | ● | ● | ● | ● | ||||||
| Erick-Peleti et al. (2007) [74] | ● | |||||||||
| Fernandes et al. (2020) [28] | ● | |||||||||
| Ford et al. (2000) [75] | ● | ● | ● | ● | ||||||
| Fowler et al. (2013) [76] | ● | ● | ● | ● | ● | ● | ● | |||
| Galland et al. (2014) [77] | ● | ● | ● | ● | ● | |||||
| Gaydos et al. (2015) [78] | ● | ● | ● | ● | ||||||
| Gibson et al. (2000) [79] | ● | ● | ● | ● | ● | ● | ||||
| Goodstein et al. (2015) [80] | ● | ● | ● | ● | ● | |||||
| Haas et al. (2017) [18] | ● | ● | ● | ● | ● | ● | ● | |||
| Hamadneh et al. (2016) [81] | ● | ● | ● | ● | ● | |||||
| Hannan et al. (2020) [82] | ● | ● | ● | |||||||
| Hauck et al. (2008) [83] | ● | ● | ● | ● | ● | |||||
| Hauck et al. (2015) [84] | ● | ● | ● | ● | ● | ● | ||||
| Hirabayashi et al. (2016) [85] | ● | ● | ● | ● | ||||||
| Homer et al. (2012) [86] | ● | ● | ||||||||
| Hussain et al. (2018) [87] | ● | ● | ● | ● | ● | |||||
| Hutchison et al. (2006) [88] | ● | ● | ● | ● | ● | ● | ● | ● | ||
| Hutchison et al. (2007) [89] | ● | ● | ● | |||||||
| Hutchison et al. (2010) [90] | ● | ● | ● | ● | ● | ● | ● | ● | ||
| Hutchison et al. (2015) [19] | ● | ● | ● | ● | ● | ● | ● | ● | ||
| Hwang et al. (2013) [91] | ● | ● | ● | |||||||
| Hwang et al. (2016) [92] | ● | ● | ● | ● | ||||||
| Inbar et al. (2005) [93] | ● | |||||||||
| Joyner et al. (2016) [94] | ● | ● | ● | |||||||
| Kelmanson (2013) [95] | ● | ● | ||||||||
| Kihlström et al. (2020) [35] | ● | ● | ||||||||
| Konstat-Korzenny et al. (2019) [96] | ● | ● | ● | ● | ||||||
| Krouse et al. (2012) [97] | ● | ● | ● | |||||||
| Kuhlmann et al. (2016) [29] | ● | ● | ||||||||
| Lahr et al. (2005a) [98] | ● | ● | ||||||||
| Lahr et al. (2005b) [99] | ● | |||||||||
| Lahr et al. (2007) [100] | ● | ● | ● | ● | ||||||
| Lau and Hall (2016) [30] | ● | ● | ||||||||
| Martiniuk et al. (2016) [101] | ● | ● | ● | ● | ||||||
| Mathews et al. (2015) [102] | ● | ● | ● | ● | ● | ● | ||||
| Miladinia et al. (2015) [103] | ● | ● | ● | ● | ||||||
| Möllborg et al. (2011) [104] | ● | ● | ● | ● | ||||||
| Moon et al. (2010) [105] | ● | ● | ● | ● | ● | ● | ● | |||
| Moon et al. (2019) [31] | ● | |||||||||
| Moon and Omron (2002) [106] | ● | ● | ● | ● | ||||||
| Nelson et al. (2001a) [107] | ● | ● | ● | |||||||
| Nelson et al. (2001b) [108] | ● | ● | ● | ● | ||||||
| Nelson et al. (2005) [109] | ● | ● | ● | |||||||
| Norton and Grellner (2011) [110] | ● | ● | ||||||||
| Nongkynrih et al. (2017) [111] | ● | ● | ● | ● | ● | |||||
| Oden et al. (2012) [112] | ● | ● | ||||||||
| Osberg et al. (2021) [113] | ● | ● | ● | ● | ||||||
| Panaretto et al. (2002) [114] | ● | ● | ● | ● | ● | ● | ||||
| Paterson et al. (2002) [115] | ● | ● | ● | ● | ||||||
| Pease et al. (2017) [116] | ● | ● | ● | |||||||
| Pease et al. (2018) [117] | ● | ● | ||||||||
| Phares et al. (2004) [118] | ● | ● | ● | ● | ||||||
| Pretorius et al. (2020) [32] | ● | ● | ||||||||
| Provini et al. (2017) [119] | ● | ● | ● | ● | ● | |||||
| Raines (2018) [33] | ● | |||||||||
| Roberts and Upton (2000) [120] | ● | ● | ● | |||||||
| Robida and Moon (2012) [121] | ● | ● | ||||||||
| Rohana et al. (2018) [122] | ● | ● | ● | |||||||
| Ruiz Botia et al. (2020) [123] | ● | ● | ● | ● | ● | |||||
| Salm Ward and Ngui (2015) [124] | ● | ● | ● | ● | ||||||
| Salm Ward et al. (2018) [125] | ● | ● | ● | |||||||
| Salm Ward et al. (2016) [126] | ● | ● | ||||||||
| Sawaguchi et al. (2002) [20] | ● | ● | ● | ● | ● | ● | ● | |||
| Schluter et al. (2007) [14] | ● | ● | ● | ● | ● | ● | ● | ● | ||
| Schluter and Young (2002) [15] | ● | ● | ● | ● | ● | ● | ● | ● | ||
| Shapiro-Mendoza et al. (2015) [127] | ● | ● | ● | ● | ||||||
| Shields et al. (2005) [21] | ● | ● | ● | ● | ● | ● | ||||
| Sivan et al. (2004) [128] | ● | |||||||||
| Smith et al. (2012) [129] | ● | ● | ● | |||||||
| Smith et al. (2016) [130] | ● | ● | ● | ● | ||||||
| Smylie et al. (2014) [131] | ● | ● | ● | ● | ||||||
| Specker et al. (2020) [23] | ● | ● | ● | ● | ● | ● | ||||
| Sperhake et al. (2009) [132] | ● | ● | ||||||||
| Strömberg Celind et al. (2017) [133] | ● | ● | ● | ● | ● | |||||
| Tipene-Leach et al. (2010) [134] | ● | ● | ● | ● | ● | ● | ● | ● | ||
| Tirosh et al. (2000) [135] | ● | ● | ● | |||||||
| Tully et al. (2015) [136] | ● | ● | ● | ● | ● | ● | ||||
| van Sleuwen et al. (2003) [137] | ● | ● | ● | ● | ● | ● | ||||
| Vernacchio et al. (2003) [138] | ● | |||||||||
| Varghese et al. (2015) [34] | ● | ● | ||||||||
| Vilvens et al. (2020) [139] | ● | ● | ● | |||||||
| Von Kohorn et al. (2010) [140] | ● | ● | ||||||||
| Walcott et al. (2018) [141] | ● | ● | ● | ● | ||||||
| Wennergren et al. (2021) [142] | ● | ● | ● | ● | ||||||
| Willinger et al. (2000) [143] | ● | ● | ||||||||
| Wilson (2000) [22] | ● | ● | ● | ● | ● | ● | ● | |||
| Woods et al. (2015) [144] | ● | ● | ● | |||||||
| Wright et al. (2014) [145] | ● | ● | ||||||||
| Yikilkan et al. (2011) [146] | ● | ● | ● | ● | ● | ● | ● | |||
| Zoucha et al. (2016) [147] | ● | ● | ● | |||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cole, R.; Young, J.; Kearney, L.; Thompson, J.M.D. Infant Care Practices, Caregiver Awareness of Safe Sleep Advice and Barriers to Implementation: A Scoping Review. Int. J. Environ. Res. Public Health 2022, 19, 7712. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19137712
Cole R, Young J, Kearney L, Thompson JMD. Infant Care Practices, Caregiver Awareness of Safe Sleep Advice and Barriers to Implementation: A Scoping Review. International Journal of Environmental Research and Public Health. 2022; 19(13):7712. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19137712
Chicago/Turabian StyleCole, Roni, Jeanine Young, Lauren Kearney, and John M. D. Thompson. 2022. "Infant Care Practices, Caregiver Awareness of Safe Sleep Advice and Barriers to Implementation: A Scoping Review" International Journal of Environmental Research and Public Health 19, no. 13: 7712. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19137712