
Muscle-Skeletal Abnormalities and Muscle Oxygenation during Isokinetic Strength Exercise in Heart Failure with Preserved Ejection Fraction Phenotype: A Cross-Sectional Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Baseline Clinical Characteristics
2.2.1. Dual-Energy X-ray Absorptiometry (DXA)
2.2.2. Echocardiography
2.2.3. Spirometry
2.2.4. Cardiopulmonary Exercise Test
2.3. Isokinetic Muscle Strength Test
2.4. Near-Infrared Spectroscopy (NIRS)
2.5. Ultrasound-Derived Measures: Echo Intensity and Muscle Thickness
2.6. Statistical Analysis
3. Results
3.1. Baseline Clinical Characteristics
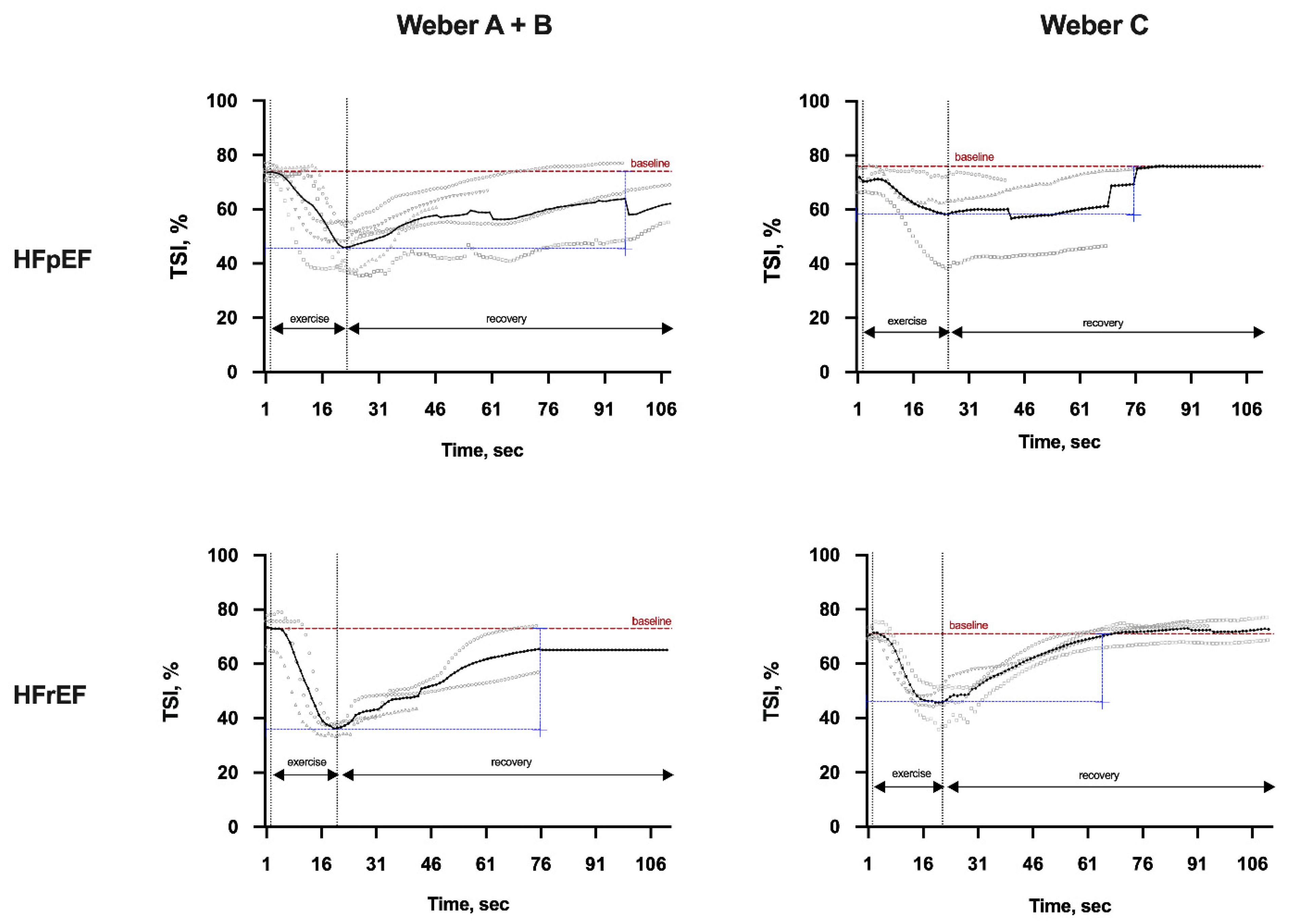
3.2. Peripheral Muscle Microcirculation Dynamics during Isokinetic Muscle Strength Testing
3.3. Isokinetic Muscle Strength Parameters
3.4. Ultrasound-Derived Parameters (Echo Intensity and Muscle Thickness)
3.5. Associations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Naghavi, M.; Wang, H.; Lozano, R.; Davis, A.; Liang, X.; Zhou, M.; Vollset, S.E.; Ozgoren, A.A.; Abdalla, S.; Abd-Allah, F.; et al. Global, regional, and national age–sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: A systematic analysis for the Global Burden of Disease study 2013. Lancet 2015, 385, 117–171. [Google Scholar] [CrossRef]
- World Health Organization. Cardiovascular Diseases: Key Facts. Available online: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds) (accessed on 30 October 2019).
- Junior, G.C.; Neves, L.M.T.; Cipriano, G.F.B.; Chiappa, G.R.; Borghi-Silva, A. Cardiovascular disease prevention and implications for worksite health promotion programs in Brazil. Prog. Cardiov. Dis. 2014, 56, 493–500. [Google Scholar] [CrossRef]
- Heidenreich, P.A.; Albert, N.M.; Allen, L.A.; Bluemke, D.A.; Butler, J.; Fonarow, G.C.; Ikonomidis, J.S.; Khavjou, O.; Konstam, M.A.; Maddox, T.M.; et al. Forecasting the impact of heart failure in the United States. Circ. Heart Fail. 2013, 6, 606–619. [Google Scholar] [CrossRef] [Green Version]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.-P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Eur. J. Heart Fail. 2016, 18, 891–975. [Google Scholar] [CrossRef]
- Redfield, M.M. Heart failure with preserved ejection fraction. N. Engl. J. Med. 2016, 375, 1868–1877. [Google Scholar] [CrossRef] [Green Version]
- Dhingra, A.; Garg, A.; Kaur, S.; Chopra, S.; Batra, J.S.; Pandey, A.; Chaanine, A.H.; Agarwal, S.K. Epidemiology of heart failure with preserved ejection fraction. Curr. Heart Fail. Rep. 2014, 11, 354–365. [Google Scholar] [CrossRef]
- Owan, T.E.; Hodge, D.O.; Herges, R.M.; Jacobsen, S.J.; Roger, V.L.; Redfield, M.M. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N. Engl. J. Med. 2006, 355, 251–259. [Google Scholar] [CrossRef] [Green Version]
- Kemp, C.D.; Conte, J.V. The pathophysiology of heart failure. Cardiovasc. Pathol. 2012, 21, 365–371. [Google Scholar] [CrossRef] [PubMed]
- Esposito, F.; Mathieu-Costello, O.; Shabetai, R.; Wagner, P.D.; Richardson, R.S. Limited maximal exercise capacity in patients with chronic heart failure: Partitioning the contributors. J. Am. Coll. Cardiol. 2010, 55, 1945–1954. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bocchi, E.A.; Marcondes-Braga, F.G.; Bacal, F.; Ferraz, A.S.; Albuquerque, D.; Rodrigues, D.; Mesquita, E.T.; Vilas-Boas, F.; Cruz, F.; Ramires, F.; et al. Sociedade Brasileira de Cardiologia. Atualização da Diretriz Brasileira de Insuficiência Cardíaca Crônica-2012. Arq. Bras. Cardiol. 2012, 98, 1–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poole, D.C.; Richardson, R.S.; Haykowsky, M.J.; Hirai, D.M.; Musch, T.I. Exercise limitations in heart failure with reduced and preserved ejection fraction. J. Appl. Physiol. 2018, 1, 208–224. [Google Scholar] [CrossRef]
- Coats, A.J.S.; Clark, A.L.; Piepoli, M.; Volterrani, M.; Poole-Wilson, P.A. Symptoms and quality of life in heart failure: The muscle hypothesis. Br. Heart J. 1994, 72, 36–39. [Google Scholar] [CrossRef] [Green Version]
- Adams, V.; Linke, A.; Winzer, E. Skeletal muscle alterations in HFrEF vs. HFpEF. Curr. Heart Fail. Rep. 2017, 14, 489–497. [Google Scholar] [CrossRef]
- Kan Van, G.A. Epidemiology and consenquences of sarcopenia. J. Nutr. Health Aging 2009, 13, 708–712. [Google Scholar] [CrossRef] [PubMed]
- Bekfani, T.; Pellicori, P.; Morris, D.A.; Ebner, N.; Valentova, M.; Steinbeck, L.; Wachter, R.; Elsner, S.; Sliziuk, V.; Schefold, J.C.; et al. Sarcopenia in patients with heart failure with preserved ejection fraction: Impact on muscle strength, exercise capacity and quality of life. Int. J. Cardiol. 2016, 222, 41–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDonagh, T.A.; McDonagh, T.A.; Metram, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Toth, M.J.; Miller, M.S.; Ward, K.A.; Ades, P.A. Skeletal muscle mitochondrial density, gene expression, and enzyme activities in human heart failure: Minimal effects of the disease and resistance training. J. Appl. Physiol. 2012, 112, 1864–1874. [Google Scholar] [CrossRef]
- Stevens, A.L.M.; Hansen, D.; Herbots, L.; Wens, I.; Creemers, A.; Dendale, P.; Eijnde, B.O. Exercise training improves insulin realease during glucose tolerance testing in stable chronic heart failure patients. J. Cardiopulm. Rehabil. Prev. 2015, 35, 37–46. [Google Scholar] [CrossRef]
- Manetos, C.; Dimopoulos, S.; Tzanis, G.; Vakrou, S.; Tasoulis, A.; Kapelios, C.; Agapitou, V.; Ntalianis, A.; Terrovitis, J.; Nanas, S. Skeletal muscle microcirculatory abnormalities are associated with exercise intolerance, ventilatory inefficiency, and impaired autonomic control in heart failure. J. Heart Lung Transpl. 2011, 30, 1403–1408. [Google Scholar] [CrossRef]
- Paneroni, M.; Pasini, E.; Comini, L.; Vitacca, M.; Schena, F.; Scalvini, S.; Venturelli, M. Skeletal Muscle Myopathy in Heart Failure: The Role of Ejection Fraction. Curr. Cardiol. Rep. 2018, 20, 116. [Google Scholar] [CrossRef]
- Poole, D.C.; Hirai, D.M.; Copp, S.W.; Musch, T.I. Muscle oxygen transport and utilization in heart failure: Implications for exercise (in)tolerance. Am. J. Physiol. Heart Circ. Physiol. 2012, 302, H1050–H1063. [Google Scholar] [CrossRef] [PubMed]
- Haykowsky, M.J.; Brubaker, P.H.; John, J.M.; Stewart, K.P.; Morgan, T.M.; Kitzman, D.W. Determinants of exercise intolerance in elderly heart failure patients with preserved ejection fraction. J. Am. Coll. Cardiol. 2011, 58, 265–274. [Google Scholar] [CrossRef] [Green Version]
- Dhakal, B.P.; Malhotra, R.; Murphy, R.M.; Pappagianopoulos, P.P.; Baggish, A.L.; Weiner, R.B.; Houstis, N.E.; Eisman, A.S.; Hough, S.S.; Lewis, G.D. Mechanisms of exercise intolerance in heart failure with preserved ejection fraction: The role of abnormal peripheral oxygen extraction. Circ. Heart Fail. 2015, 8, 286–294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, J.R.; Mancini, D.M.; Dunkman, W.B. Exertional fatigue due to skeletal muscle dysfunction in patients with heart failure. Circulation 1993, 87, 470–475. [Google Scholar] [CrossRef] [Green Version]
- Borlaug, B.A.; Olson, T.P.; Lam, C.S.P.; Flood, K.S.; Lerman, A.; Johnson, B.D.; Redfield, M.M. Global cardiovascular reserve dysfunction in heart failure with preserved ejection fraction. J. Am. Coll. Cardiol. 2010, 56, 845–854. [Google Scholar] [CrossRef] [Green Version]
- Boyes, N.G.; Eckstein, J.; Pylypchuk, S.; Marciniuk, D.D.; Butcher, S.J.; Lahti, D.S.; Dewa, D.M.K.; Haykowsky, M.K.; Wells, C.R.; Tomczak, C.R. Effects of heavy-intensity priming exercise on pulmonary oxygen uptake kinetics and muscle oxygenation in heart failure with preserved ejection fraction. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2019, 316, 199–209. [Google Scholar] [CrossRef]
- Kitzman, D.W.; Nicklas, B.; Kraus, W.E.; Lyles, M.F.; Eggebeen, J.; Morgan, T.M.; Haykowsky, M. Skeletal muscle abnormalities and exercise intolerance in older patients with heart failure and preserved ejection fraction. Am. J. Physiol. Heart Circ. Physiol. 2014, 306, H1364–H1370. [Google Scholar] [CrossRef] [PubMed]
- Haykowsky, M.J.; Nicklas, B.J.; Brubaker, P.H.; Hundley, W.G.; Brinkley, T.E.; Upadhya, B.; Becton, J.T.; Nelson, M.D.; Chen, H.; Kitzman, D.W. Regional adipose distribution and its relationship to exercise intolerance in older obese patients who have heart failure with preserved ejection fraction. JACC Heart Fail. 2018, 6, 640–649. [Google Scholar] [CrossRef]
- Niemeijer, V.M. Skeletal Muscle Characteristics and Exercise Intolerance in Chronic Heart Failure. Available online: https://pure.tue.nl/ws/files/88381011/20180111_Niemeijer.pdf (accessed on 20 January 2018).
- Marti, C.N.; Gheorghiade, M.; Kalogeropoulos, A.P.; Georgiopoulou, V.V.; Quyyumi, A.A.; Butler, J. Endothelial dysfunction, arterial stiffness and heart failure. J. Am. Coll. Cardiol. 2012, 60, 1455–1469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stock, M.S.; Thompson, B.J. Echo intensity as an indicator of skeletal muscle quality: Applications, methodology, and future directions. Eur. J. Appl. Physiol. 2021, 121, 369–380. [Google Scholar] [CrossRef]
- O’Connor, C.M.; Whellan, D.J.; Wojdyla, D.; Leifer, E.; Clare, R.M.; Ellis, S.J.; Fine, L.J.; Fleg, J.L.; Zannad, F.; Keteyian, S.J. Factors related to morbidity and mortality in patients with chronic heart failure with systolic dysfunction the HF-ACTION predictive risk score model. Circ. Heart Fail. 2012, 5, 63–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montero, D.; Diaz-Cañestro, C. Determinants of exercise intolerance in heart failure with preserved ejection fraction: A systematic review and meta-analysis. Int. J. Cardiol. 2018, 254, 224–229. [Google Scholar] [CrossRef] [PubMed]
- Nakano, I.; Hori, H.; Fukushima, A.; Yokota, T.; Kinugawa, S.; Takada, S.; Yamanashi, K.; Obata, Y.; Kitaura, Y.; Kakutani, N.; et al. Enhanced echo intensity of skeletal muscle is associated with exercise intolerance in patients with heart failure. J. Card. Fail. 2020, 8, 685–693. [Google Scholar] [CrossRef] [PubMed]
- Lopez, P.; Wilhelm, E.N.; Rech, A.; Minozzo, F.; Radaelli, R.; Pinto, R.S. Echo intensity independently predicts functionality in sedentary older men. Muscle Nerve 2017, 55, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Rech, A.; Radaelli, R.; Goltz, F.R.; da Rosa, L.H.; Schneider, C.D.; Pinto, R.S. Echo intensity is negatively associated with functional capacity in older women. AGE 2014, 36, 9708. [Google Scholar] [CrossRef]
- Wilhelm, E.N.; Rech, A.; Minozzo, F.; Radaelli, R.; Botton, C.E.; Pinto, R.S. Relationship between quadriceps femoris echo intensity, muscle power, and functional capacity of older men. AGE 2014, 36, 9625. [Google Scholar] [CrossRef] [Green Version]
- Malta, M.; Cardoso, L.O.; Bastos, F.I.; Magnanini, M.M.F.; da Silva, C.M.F.P. STROBE initiative: Guidelines on reporting obsevartional studies. Rev. Saúde Pública 2010, 44, 559–565. [Google Scholar] [CrossRef] [Green Version]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E., Jr.; Drazner, M.H.; Fonarow, G.C.; Geraci, S.A.; Horwich, T.; Januzzi, J.L.; et al. 2013 ACCF/AHA guideline for the management of heart failure: A report of the American College of Cardiology Foundation/American Heart Association task force on practice guidelines. J. Am. Coll. Cardiol. 2013, 62, e147–e239. [Google Scholar] [CrossRef] [Green Version]
- Guazzi, M.; Arena, R.; Halle, M.; Piepoli, M.F.; Myers, J.; Lavie, C.J. 2016 focused update: Clinical recommendations for cardiopulmonary exercise testing data assessment in specific patient populations. Eur. Heart J. 2018, 39, 1144–1161. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39.e14. [Google Scholar] [CrossRef] [Green Version]
- Miller, M.R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Crapo, R.; Enright, P.; van der Grinten, C.P.M.; Gustafsson, P.; et al. ATS/ERS task force: Standardisation of lung function testing. Eur. Respir. J. 2005, 26, 153–161. [Google Scholar] [CrossRef] [Green Version]
- Pereira, C.A.C.; Sato, T.; Rodrigues, S.C. New reference values for forced spirometry in white adults in Brazil. J. Bras. Pneumol. 2007, 33, 397–406. [Google Scholar] [CrossRef]
- Sandri, M.; Viehmann, M.; Adams, V.; Rabald, K.; Mangner, N.; Höllriegel, R.; Lurz, P.; Erbs, S.; Linke, A.; Kirsch, K.; et al. Chronic heart failure and aging-effects of exercise training on endothelial function and mechanisms of endothelial regeneration: Results from the Leipzig Exercise Intervention in Chronic heart failure and Aging (LEICA) study. Eur. J. Prev. Cardiol. 2015, 23, 349–358. [Google Scholar] [CrossRef]
- Gutiérrez, E.; Flammer, A.J.; Lerman, L.O.; Elízaga, J.; Lerman, A.; Fernández-Avilés, F. Endothelial dysfunction over the course of coronary artery disease. Eur. Heart J. 2013, 34, 3175–3181. [Google Scholar] [CrossRef] [Green Version]
- Matsue, Y.; Suzuki, M.; Nagahori, W.; Ohno, M.; Matsumura, A.; Hashimoto, Y.; Yoshida, K.; Yoshida, M. Endothelial dysfunction measured by peripheral arterial tonometry predicts prognosis in patients with heart failure with preserved ejection fraction. Int. J. Cardiol. 2013, 168, 36–40. [Google Scholar] [CrossRef]
- Arena, R.; Myers, J.; Aslam, S.S.; Varughese, E.B.; Peberdy, M.A. Peak VO2 and VE/VCO2 slope in patients with heart failure: A prognostic comparison. Am Heart J. 2004, 147, 354–360. [Google Scholar] [CrossRef]
- Jones, N.L.; Campbell, E.J. Clinical Exercise Testing; Saunders: Philadelphia, PA, USA, 1982; p. 202. [Google Scholar]
- Almeida, A.E.M.D.; Stefani, C.D.M.; Nascimento, J.A.D.; Almeida, N.M.D.; Santos, A.D.C.; Stein, R. An Equation for the Prediction of Oxygen Consumption in a Brazilian Population. Arq. Bras. Cardiol. 2014, 103, 299–307. [Google Scholar] [CrossRef] [PubMed]
- Toth, M.J.; Shaw, A.O.; Miller, M.S.; VanBuren, P.; LeWinter, M.M.; Maughan, D.W.; Ades, P.A. Reduced knee extensor function in heart failure is not explained by inactivity. Int. J. Cardiol. 2010, 143, 276–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delagardelle, C.; Feiereisen, P.; Krecké, R.; Essamri, B.; Beissel, J. Objective effects of a 6 months’ endurance and strength training program in outpatients with congestive heart failure. Med. Sci. Sports Exerc. 1999, 31, 1102–1107. [Google Scholar] [CrossRef] [PubMed]
- Delagardelle, C.; Feiereisen, P.; Autier, P.; Shita, R.; Krecke, R.; Beissel, J. Strength/endurance training versus endurance training in congestive heart failure. Med. Sci. Sports Exerc. 2002, 34, 1868–1872. [Google Scholar] [CrossRef] [PubMed]
- Minotti, J.R.; Christoph, I.; Oka, R.; Weiner, M.W.; Wells, L.; Massie, B.M. Impaired skeletal muscle function in patients with congestive heart failure: Relationship to systemic exercise performance. J. Clin. Investig. 1991, 88, 2077–2082. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Owen-Reece, H.; Smith, M.; Elwell, C.E.; Goldstone, J.C. Near infrared spectroscopy. Br. J. Anaesth 1999, 82, 418–426. Available online: https://www.bjanaesthesia.org/article/S0007-0912(17)38615-4/pdf (accessed on 20 January 2018). [CrossRef] [PubMed]
- Alvares, T.S.; Oliveira, G.V.; Soares, R.; Murias, M. Near-infrared spectroscopy-derived total haemoglobin as an indicator of changes in muscle blood flow during exercise-induced hyperaemia. J. Sports Sci. 2020, 38, 751–758. [Google Scholar] [CrossRef] [PubMed]
- Tillquist, M.; Kutsogiannis, D.J.; Wischmeyer, P.E.; Kummerlen, C.; Leung, R.; Stollery, D.; Karvellas, C.J.; Preiser, J.-C.; Bird, N.; Kozar, R.; et al. Bedside ultrasound is a practical and reliable measurement tool for assessing quadriceps Muscle layer thickness. J. Parenter. Enter. Nutr. 2013, 38, 886–890. [Google Scholar] [CrossRef] [Green Version]
- Abràmoff, M.D.; Magalhães, P.J.; Ram, S.J. Image processing with ImageJ. Biophotonics Int. 2005, 11, 36–42. [Google Scholar]
- Arts, I.M.P.; Phillens, S.; Schelhaas, H.J.; Overeem, S.; Zwarts, M.J. Normal values for quantitative muscle ultrasonography in adults. Muscle Nerve 2010, 41, 32–41. [Google Scholar] [CrossRef]
- Blazevich, A.J.; Gill, N.D.; Zhou, S. Intra- and intermuscular variation in human quadriceps femoris architecture assessed in vivo. J. Anat. 2006, 209, 289–310. [Google Scholar] [CrossRef]
- Zou, K.H.; Tuncali, K.; Silverman, S.G. Correlation and simple linear regression. Radiology 2003, 227, 617–622. [Google Scholar] [CrossRef]
- Prion, S.; Haerling, K.A. Making sense of methods and measurement: Spearman-rho ranked-order correlation coefficient. Clin. Simul. Nurs. 2014, 10, 535–536. [Google Scholar] [CrossRef]
- Zamani, P.; Proto, E.A.; Mazurek, J.A.; Prenner, S.B.; Margulies, K.B.; Townsend, R.R.; Kelly, D.P.; Arany, Z.; Poole, D.C.; Wagner, P.D.; et al. Peripheral determinants of oxygen utilization in heart failure with preserved ejection fraction: Central role of adiposity. JACC Basic Transl. Sci. 2020, 5, 211–225. [Google Scholar] [CrossRef]
- Bhella, P.S.; Prasad, A.; Heinicke, K.; Hastings, J.L.; Arbab-Zadeh, A.; Adams-Huet, B.; Pacini, E.L.; Shibata, S.; Palmer, M.D.; Newcomer, B.R.; et al. Abnormal haemodynamic response to exercise in heart failure with preserved ejection fraction. Eur. J. Heart Fail. 2011, 13, 1296–1304. [Google Scholar] [CrossRef] [PubMed]
- Weiss, K.; Schär, M.; Panjrath, G.S.; Zhang, Y.; Sharma, K.; Bottomley, P.A.; Golozar, A.; Steinberg, A.; Gerstenblith, G.; Russell, S.D.; et al. Fatigability, exercise intolerance and abnormal skeletal muscle energetics in heart failure. Circ. Heart Fail. 2017, 10, e004129. [Google Scholar] [CrossRef] [PubMed]
- Tucker, W.J.; Angadi, S.S.; Haykowsky, M.J.; Nelson, M.D.; Sarma, S.; Tomczak, C.R. Pathophysiology of exercise intolerance and its treatment with exercise-based cardiac rehabilitation in heart failure with preserved ejection fraction. J. Cardiopulm. Rehabil. Prev. 2020, 40, 9–16. [Google Scholar] [CrossRef]
- Hirai, D.M.; Musch, T.I.; Poole, D.C. Exercise training in chronic heart failure: Improving skeletal muscle O2 transport and utilization. Am. J. Physiol. Heart Circ. Physiol. 2015, 309, H1419–H1439. [Google Scholar] [CrossRef] [Green Version]
- Weavil, J.C.; Thurston, T.S.; Hureau, T.J.; Gifford, J.R.; Kithas, P.A.; Broxterman, R.M.; Bledsoe, A.D.; Nativi, J.N.; Richardson, R.S.; Amann, M. Heart failure with preserved ejection fraction diminishes peripheral hemodynamics and accelerates exercise-induced neuromuscular fatigue. Am. J. Physiol. Heart Circ. Physiol. 2021, 320, H338–H351. [Google Scholar] [CrossRef]
- Young, H.; Jenkins, N.T.; Zhao, Q.; Mccully, K.K. Measurement of intramuscular fat by muscle echo intensity. Muscle Nerve 2015, 6, 963–971. [Google Scholar] [CrossRef] [Green Version]
- Pillen, S.; Tak, R.O.; Zwarts, M.J.; Lammens, M.M.Y.; Verrijp, K.N.; Arts, I.M.P.; van der Laak, J.A.; Hoogerbrugge, P.M.; van Engelen, B.G.M.; Verrips, A. Skeletal muscle ultrasound: Correlation between fibrous tissue and echo intensity. Ultrasound Med. Biol. 2009, 35, 443–446. [Google Scholar] [CrossRef]
- Schaufelberger, M.; Eriksson, B.O.; Grimby, G.; Held, P.; Swedberg, K. Skeletal muscle fiber composition and capillarization in patients with chronic heart failure: Relation to exercise capacity and central hemodynamics. J. Card. Fail. 1995, 1, 267–272. [Google Scholar] [CrossRef]
- Haykowsky, M.J.; Brubaker, P.H.; Morgan, T.M.; Kritchevsky, S.; Eggebeen, J.; Kitzman, D.W. Impaired aerobic capacity and physical functional performance in older heart failure patients with preserved ejection fraction: Role of lean body mass. J. Gerontol. A Biol. Sci. Med. Sci. 2013, 68, 968–975. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haykowsky, M.J.; Kouba, E.J.; Brubaker, P.H.; Nicklas, B.J.; Eggebeen, J.; Kitzman, D.W. Skeletal muscle composition and its relation to exercise intolerance in older patients with heart failure and pre-served ejection fraction. Am. J. Cardiol. 2014, 113, 1211–1216. [Google Scholar] [CrossRef] [Green Version]
- Molina, A.J.A.; Bharadwaj, M.S.; Horn, C.V.; Nicklas, B.J.; Lyles, M.F.; Eggebeen, J.; Haykowsky, M.J.; Brubaker, P.H.; Kitzman, D.W. Skeletal muscle mitochondrial content, oxidative capacity, and Mfn2 expression are reduced in older patients with heart failure and preserved ejection fraction and are related to exercise intolerance. J. Am. Coll. Cardiol. 2016, 8, 636–645. [Google Scholar] [CrossRef] [PubMed]
- Del Buono, M.G.; Arena, R.; Borlaug, B.A.; Carbone, S.; Canada, J.M.; Kirkman, D.L.; Garten, R.; Rodriguez-Miguelez, P.; Guazzi, M.; Lavie, C.J.; et al. Exercise intolerance in patients with heart failure: JACC State-of-the-art-review. J. Am. Coll. Cardiol. 2019, 73, 2209–2225. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | HFpEF | HFrEF | HFpEF | HFrEF | HFpEF vs. HFrEF | Weber Class A + B vs. Weber Class C | HFpEF vs. HFrEF | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Weber Class A + B (n = 11) | Weber Class C (n = 5) | Weber Class A + B (n = 7) | Weber Class C (n = 5) | (n = 16) | (n = 12) | p-Value (A + B) | p-Value (C) | p-Value HFpEF | p-Value HFrEF | p-Value | |
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | ||||||
| Male (n, %) | 10 (90.9%) | 1 (20.0%) | 5 (71.4%) | 3 (60.0%) | 8 (66.7%) | 11 (68.8%) | -- | -- | 0.013 c,* | >0.999 c | >0.999 c |
| Age, years | 53.7 ± 9.4 | 59.8 ± 15.7 | 53.7 ± 7.9 | 55.4 ± 7.1 | 55.6 ± 11.5 | 54.4 ± 7.3 | 0.998 a | 0.590 a | 0.457 a | 0.708 a | 0.737 a |
| BMI, kg/m2 | 30.0 ± 3.9 | 30.1 ± 4.8 | 28.2 ± 5.5 | 28.3 ± 5.2 | 30.0 ± 4.0 | 28.3 ± 5.1 | 0.476 a | 0.588 a | 0.969 a | 0.981 a | 0.335 a |
| DXA | (n = 11) | (n = 4) | (n = 4) | (n = 3) | (n = 15) | (n = 7) | |||||
| Total body fat mass, % | 34.1 ± 3.8 | 45.4 ± 5.5 | 36.7 ± 5.8 | 40.5 ± 10.8 | 37.1 ± 6.6 | 38.3 ± 7.8 | 0.453 a | 0.533 a | 0.019 a,* | 0.624 a | 0.724 a |
| Body fat mass, Kg | 29.0 ± 6.9 | 36.8 ± 6.3 | 25.5 ± 7.3 | 31.8 ± 12.0 | 31.1 ± 7.4 | 28.2 ± 9.2 | 0.440 a | >0.999 b | 0.087 a | 0.400 b | 0.582 a |
| Total body lean mass, % | 63.6 ± 3.6 | 53.0 ± 5.3 | 61.4 ± 5.6 | 57.4 ± 9.7 | 60.8 ± 6.2 | 59.8 ± 7.2 | 0.503 a | 0.533 a | 0.020 a,* | 0.567 a | 0.732 a |
| Body lean mass, Kg | 55.4 ± 9.0 | 44.2 ± 6.2 | 44.7 ± 15.5 | 46.3 ± 16.4 | 52.4 ± 9.6 | 45.4 ± 14.5 | 0.266 a | 0.851 a | 0.026 a,* | 0.902 a | 0.273 a |
| Right leg fat mass, Kg | 3.8 ± 0.8 | 6.0 ± 1.4 | 3.2 ± 0.8 | 4.1 ± 1.9 | 4.4 ± 1.4 | 3.6 ± 1.3 | 0.246 a | 0.231 a | 0.046 a,* | 0.474 a | 0.219 a |
| Right leg lean mass, Kg | 9.3 ± 1.9 | 7.3 ± 1.0 | 7.1 ± 3.2 | 6.8 ± 2.8 | 8.8 ± 1.9 | 7.0 ± 2.8 | 0.270 a | 0.790 a | 0.026 a,* | 0.900 a | 0.160 a |
| Left leg fat mass, Kg | 3.6 ± 0.7 | 6.0 ± 1.4 | 3.2 ± 0.8 | 4.1 ± 1.8 | 4.3 ± 1.4 | 3.6 ± 1.3 | 0.406 a | 0.207 a | 0.040 a,* | 0.500 a | 0.501 b |
| Left leg lean mass, Kg | 9.4 ± 2.0 | 7.2 ± 0.9 | 7.0 ± 3.2 | 6.6 ± 2.4 | 8.8 ± 2.0 | 6.8 ± 2.6 | 0.240 a | 0.708 a | 0.012 a,* | 0.856 a | 0.114 a |
| Heart Diseases | |||||||||||
| Ischemic (n, %) | 10 (90.9%) | 3 (60.0%) | 5 (71.4%) | 3 (60.0%) | 13 (81.3%) | 8 (66.7%) | -- | -- | 0.214 c | >0.999 c | 0.418 c |
| Hypertension (n, %) | 0 (0.0%) | 1 (20.0%) | 0 (0.0%) | 0 (0.0%) | 1 (6.3%) | 0 (0.0%) | -- | -- | 0.313 c | >0.999 c | >0.999 c |
| Idiopathic (n, %) | 1 (9.1%) | 1 (20.0%) | 2 (28.6%) | 2 (40.0%) | 2 (12.5%) | 4 (33.3%) | -- | -- | >0.999 c | >0.999 c | 0.354 c |
| Risk Factors | |||||||||||
| Arterial Hypertension (n, %) | 6 (54.6%) | 3 (60.0%) | 5 (71.4%) | 2 (40.0%) | 9 (56.3%) | 7 (58.3%) | -- | -- | >0.999 c | 0.558 c | >0.999 c |
| Diabetes Mellitus (n, %) | 2 (18.2%) | 1 (20.0%) | 2 (28.6%) | 2 (40.0%) | 3 (20.0%) | 4 (33.3%) | -- | -- | >0.999 c | >0.999 c | 0.662 c |
| Dyslipidemia (n, %) | 10 (90.9%) | 2 (40.0%) | 5 (71.4%) | 3 (60.0%) | 12 (75.0%) | 8 (66.7%) | -- | -- | 0.063 c | >0.999 c | 0.691 c |
| Obesity (n, %) | 5 (45.5%) | 2 (40.0%) | 2 (28.6%) | 2 (40.0%) | 7 (43.8%) | 4 (33.3%) | -- | -- | >0.999 c | >0.999 c | 0.705 c |
| Tabagism (n, %) | 2 (18.2%) | 3 (60.0%) | 4 (57.1%) | 2 (40.0%) | 5 (31.3%) | 6 (50.0%) | -- | -- | 0.245 c | >0.999 c | 0.441 c |
| Coronary Artery Disease (n, %) | 8 (72.7%) | 2 (40.0%) | 2 (28.6%) | 3 (60.0%) | 10 (62.5%) | 8 (66.7%) | -- | -- | 0.300 c | 0.558 c | >0.999 c |
| Drugs | |||||||||||
| Beta-blocker (n, %) | 10 (90.1%) | 5 (100.0%) | 7 (100.0%) | 5 (100.0%) | 15 (93.8%) | 12 (100.0%) | -- | -- | >0.999 c | >0.999 c | >0.999 c |
| ACEI (n, %) | 6 (54.6%) | 2 (40.0%) | 6 (85.7%) | 3 (60.0%) | 8 (50.0%) | 9 (75.0%) | -- | -- | >0.999 c | >0.523 c | 0.253 c |
| ARB (n, %) | 2 (18.2%) | 2 (40.0%) | 3 (42.9%) | 0 (0.0%) | 4 (25.0%) | 3 (25.0%) | -- | -- | >0.547 c | >0.205 c | >0.999 c |
| Diuretics (n, %) | 2 (18.2%) | 3 (60.0%) | 7 (100.0%) | 5 (100.0%) | 5 (31.3%) | 11 (91.7%) | -- | -- | >0.245 c | >0.999 c | 0.020 c,* |
| Statins (n, %) | 10 (90.9%) | 3 (60.0%) | 5 (71.4.0%) | 3 (60.0%) | 13 (81.3%) | 8 (66.7%) | -- | -- | 0.214 c | >0.999 c | 0.418 c |
| Coronary Vasodilators (n, %) | 1 (9.1%) | 2 (40.0%) | 1 (14.3%) | 1 (20.0%) | 3 (18.8%) | 2 (16.7%) | -- | -- | >0.214 c | >0.999 c | >0.999 c |
| Antidiabetic (n, %) | 2 (18.2%) | 1 (20.0%) | 1 (14.3%) | 1 (20.0%) | 3 (18.8%) | 2 (16.7%) | -- | -- | >0.999 c | >0.999 c | >0.999 c |
| Anticoagulants (n, %) | 0 (0.0%) | 0 (0.0%) | 1 (14.3%) | 2 (40.0%) | 0 (0.0%) | 3 (25.0%) | -- | -- | >0.999 c | 0.523 c | 0.067 c |
| Parameters | HFpEF | HFrEF | HFpEF | HFrEF | HFpEF vs. HFrEF | Weber Class A + B vs. Weber Class C | HFpEF vs. HFrEF | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Weber Class A + B (n = 11) | Weber Class C (n = 5) | Weber Class A + B (n = 7) | Weber Class C (n = 5) | (n = 16) | (n = 12) | p-Value (A + B) | p-Value (C) | p-Value HFpEF | p-Value HFrEF | p-Value | |
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | ||||||
| Echocardiogram | |||||||||||
| LVEF Simpson (%) | 58.4 ± 6.3 | 59.2 ± 6.3 | 34.4 ± 4.9 | 28.6 ± 7.4 | 58.6 ± 6.1 | 32.0 ± 6.5 | <0.0001 b,* | 0.0001 a,* | 0.811 a | 0.407 b | <0.0001 a,* |
| LAVI, mL/m2 | 25.0 ± 2.9 | 29.1 ± 10.4 | 34.4 ± 5.7 | 39.4 ± 4.8 | 26.3 ± 6.2 | 36.5 ± 5.7 | 0.004 a,* | 0.094 a | 0.435 a | 0.136 a | <0.0001 b,* |
| LVMI, g/m2 | 83.8 ± 10.8 | 95.4 ± 38.4 | 102.6 ± 33.7 | 141.0 ± 22.9 | 87.4 ± 22.4 | 118.6 ± 34.7 | 0.197 a | 0.059 a | 0.543 a | 0.041 a,* | 0.002 b,* |
| E/e’, cm/s | 6.6 ± 2.1 | 7.5 ± 0.9 | 10.9 ± 4.6 | 11.9 ± 4.7 | 6.9 ± 1.8 | 11.3 ± 4.4 | 0.050 a,* | 0.099 a | 0.273 a | 0.706 a | 0.006 a,* |
| Mean e’ (septal wall), cm/s | 8.0 ± 1.9 | 6.4 ± 1.7 | 5.1 ± 1.3 | 3.8 ± 0.8 | 7.5 ± 2.0 | 4.6 ± 1.3 | 0.003 b,* | 0.022 a,* | 0.127 a | 0.096 a | <0.0001 a,* |
| Mean e’ (lateral wall), cm/s | 12.6 ± 3.7 | 9.4 ± 3.1 | 8.3 ± 1.9 | 5.2 ± 1.8 | 11.6 ± 3.7 | 7.0 ± 2.3 | 0.005 a,* | 0.040 b* | 0.097 a | 0.032 b,* | 0.001 a,* |
| Pulmonary Function | |||||||||||
| FEV1, L/s | 2.8 ± 0.8 | 1.8 ± 0.5 | 2.7 ± 0.8 | 2.5 ± 0.6 | 2.5 ± 0.8 | 2.6 ± 0.7 | 0.852 a | 0.092 a | 0.008 a,* | 0.583 a | 0.641 a |
| % Predicted FEV1 | 82.4 ± 23.0 | 59.6 ± 11.5 | 82.7 ± 14.7 | 80.4 ± 12.2 | 75.3 ± 22.5 | 81.8 ± 13.2 | 0.385 b | 0.024 a,* | 0.035 b,* | 0.772 a | 0.071 b |
| Forced Vital Capacity, L | 3.8 ± 0.8 | 2.5 ± 0.6 | 3.7 ± 1.0 | 2.9 ± 0.7 | 3.4 ± 1.0 | 3.4 ± 0.9 | 0.774 b | 0.277 a | 0.003 a,* | 0.133 b | 0.959 a |
| % Predicted Forced Vital Capacity | 90.4 ± 20.5 | 67.0 ± 15.3 | 91.1 ± 10.0 | 76.0 ± 10.6 | 83.1 ± 21.6 | 84.8 ± 12.5 | 0.339 b | 0.316 a | 0.064 b | 0.036 a,* | 0.788 a |
| FEV1/FVC, % | 72.8 ± 6.6 | 72.6 ± 7.4 | 73.0 ± 7.9 | 85.4 ± 6.3 | 72.8 ± 6.6 | 78.2 ± 9.5 | 0.808 b | 0.020 a,* | 0.957 a | 0.005 b,* | 0.106 a |
| % Predicted FEV1/FVC | 90.2 ± 6.7 | 89.2 ± 6.6 | 87.2 ± 8.1 | 92.0 ± 17.8 | 89.9 ± 6.5 | 89.2 ± 12.5 | 0.426 a | >0.999 b | 0.792 a | 0.965 b | 0.442 b |
| Cardiopulmonary exercise testing | |||||||||||
| Exercise, min | 10.8 ± 2.5 | 6.6 ± 0.9 | 10.1 ± 2.6 | 6.9 ± 2.2 | 9.5 ± 2.9 | 8.8 ± 2.9 | 0.641 b | 0.782 a | 0.001 b,* | 0.048 a,* | 0.639 b |
| Peak RER | 1.2 ± 0.1 | 1.3 ± 0.1 | 1.2 ± 0.1 | 1.3 ± 0.1 | 1.3 ± 0.1 | 1.3 ± 0.1 | 0.643 b | >0.999 a | 0.179 b | 0.191 a | 0.859 b |
| Peak Power Output, W | 140.3 ± 27.0 | 84.8 ± 15.3 | 107.3 ± 26.0 | 74.8 ± 21.7 | 122.9 ± 35.9 | 93.8 ± 28.6 | 0.024 a,* | 0.426 a | 0.0002 a,* | 0.041 a,* | 0.024 a,* |
| Peak HR, bpm | 141.9 ± 18.0 | 116.8 ± 28.3 | 130.6 ± 16.5 | 125.2 ± 25.6 | 133.8 ± 24.2 | 128.3 ± 19.9 | 0.192 a | 0.605 a | 0.113 a | 0.694 a | 0.516 a |
| Peak VO2, mL·kg−1·min−1 | 22.1 ± 3.4 | 14.4 ± 1.2 | 19.2 ± 2.7 | 13.7 ± 1.6 | 19.7 ± 4.7 | 16.9 ± 3.6 | 0.060 a | 0.434 a | <0.0001 a,* | 0.001 a,* | 0.081 a |
| % Predicted peak VO2, mL·kg−1.min−1 | 66.0 ± 9.1 | 54.3 ± 17.1 | 58.8 ± 10.7 | 43.4 ± 7.5 | 62.3 ± 12.8 | 52.4 ± 12.1 | 0.167 a | 0.151 b | 0.052 b | 0.048 b,* | 0.046 a,* |
| Peak VO2, mL·min−1 | 1884.6 ± 312.7 | 1180.6 ± 126.2 | 1469.6 ± 344.0 | 1034.8 ± 251.5 | 1664.6 ± 427.8 | 1288.4 ± 371.0 | 0.024 a,* | 0.291 a | <0.0001 a,* | 0.030 a,* | 0.020 a,* |
| VE/VCO2 Slope, L/min | 27.9 ± 3.7 | 28.8 ± 8.0 | 31.1 ± 5.4 | 30.1 ± 4.0 | 28.2 ± 5.1 | 30.7 ± 4.6 | 0.196 a | 0.310 b | 0.510 b | 0.876 b | 0.084 b |
| Parameters | HFpEF | HFrEF | HFpEF | HFrEF | HFpEF vs. HFrEF | Weber Class A + B vs. Weber Class C | HFpEF vs. HFrEF | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Weber Class A + B (n = 6) | Weber Class C (n = 4) | Weber Class A + B (n = 3) | Weber Class C (n = 4) | (n = 10) | (n = 7) | p-Value | p-Value | p-Value | p-Value | p-Value | |
|
Mean ± SD (95% CI) |
Mean ± SD (95% CI) |
Mean ± SD (95% CI) |
Mean ± SD (95% CI) |
Mean ± SD (95% CI) |
Mean ± SD (95% CI) | Mean Difference A + B (95% CI) | Mean Difference C (95% CI) | Mean Difference HFpEF (95% CI) | Mean Difference HFrEF (95% CI) | Mean Difference (95% CI) | |
| TSI (%) | |||||||||||
| Baseline | 73.7 ± 2.2 (71.3 to 76.0) | 72.0 ± 5.1 (63.9 to 80.2) | 73.4 ± 6.1 (58.3 to 88.6) | 70.5 ± 2.0 (67.3 to 73.7) | 73.0 ± 3.5 (70.5 to 75.5) | 71.8 ± 4.1 (68.0 to 75.6) |
0.958 a 0.21 (−13.8 to 14.2) |
0.616 a 1.5 (−6.2 to 9.2) |
0.578 a −1.7 (−9.4 to 6.1) |
0.497 a −2.9 (16.7 to 10.9) |
0.532 a 1.2 (−2.9 to 5.4) |
| Exercise | 44.2 ± 8.2 (35.7 to 52.8) | 57.6 ± 13.7 (35.9 to 79.4) | 36.0 ± 2.4 (30.1 to 41.9) | 44.8 ± 6.6 (34.3 to 55.3) | 49.6 ± 12.1 (40.9 to 58.3) | 41.0 ± 6.7 (34.8 to 47.2) |
0.060 a 8.2 (−0.5 to 16.9) |
0.161 a 12.9 (−7.6 to 33.3) |
0.146 a 13.4 (−6.9 to 33.7) |
0.071 a 8.8 (−1.2 to 18.8) |
0.082 a 8.6 (−1.3 to 18.5) |
| Recovery | 64.1 ± 8.5 (55.1 to 73.0) | 65.1 ± 13.5 (43.6 to 86.5) | 58.1 ± 15.3 (20.2 to 96.1) | 73.8 ± 3.7 (67.9 to 79.7) | 64.5 ± 10.1 (57.3 to 71.7) | 67.1 ± 12.5 (55.6 to 78.6) |
0.583 a 5.9 (−26.7 to 38.5) |
0.290 a −8.7 (−29.4 to 12.0) |
0.899 a 1.0 (−19.0 to 21.0) |
0.214 a 15.7 (−20.3 to 51.6) |
0.475 b −2.6 (−14.7 to 8.4) |
| O2Hb (μM) | |||||||||||
| Baseline | 0.0 ± 1.2 (−1.3 to 1.3) | 0.0 ± 0.6 (−0.9 to 0.9) | −0.2 ± 0.3 (−1.3 to 1.3) | 0.7 ± 0.9 (−0.5 to 1.5) | 0.0 ± 1.0 (−0.7 to 0.7) | 0.3 ± 0.8 (−0.4 to 1.0) |
0.712 a −0.2 (−1.1 to 1.5) |
0.245 a −0.7 (−2.0 to 0.6) |
0.990 a 0.0 (−1.4 to 1.3) |
0.132 a 0.9 (−0.4 to 2.2) |
0.475 b −0.2 (−1.4 to 0.5) |
| Exercise | −27.2 ± 9.2 (−36.8 to −17.6) | −10.9 ± 3.8 (−17.0 to −4.8) | −30.0 ± 6.7 (−46.5 to −13.4) | −23.7 ± 5.7 (−32.8 to −14.5) | −20.7 ± 11.1 (−28.7 to −12.8) | −26.4 ± 6.5 (−32.4 to −20.3) |
0.626 a 2.8 (−10.6 to 16.2) |
0.029 b,* 13.5 (0.1 to 21.2) |
0.006 a,* 16.3 (6.4 to 26.2) |
0.400 b 5.8 (−2.6 to 22.4) |
0.204 a 5.7 (−3.4 to 14.8) |
| Recovery | −4.1 ± 7.9 (−12.4 to 4.2) | −3.0 ± 3.4 (−8.4 to 2.4) | −4.5 ± 8.3 (−25.1 to 16.2) | 5.9 ± 2.8 (1.4 to 10.4) | −3.7 ± 6.2 (−8.2 to 0.8) | 1.5 ± 7.6 (−5.6 to 8.5) |
0.957 a 0.3 (−15.9 to 16.5) |
0.007 a,* −8.9 (−14.4 to −3.5) |
0.766 a 1.1 (−7.4 to 9.7) |
0.154 a 10.4 (−8.3 to 29.1) |
0.167 a −5.2 (−12.8 to 2.5) |
| HHb (μM) | |||||||||||
| Baseline | −0.1 ± 0.3 (−0.4 to 0.2) | −0.2 ± 0.4 (−0.7 to 0.4) | −0.1 ± 0.2 (−0.6 to 0.5) | 0.5 ± 0.6 (−0.5 to 1.0) | −0.1 ± 0.3 (−0.3 to 0.1) | 0.2 ± 0.5 (−0.2 to 0.7) |
0.809 a −0.04 (−0.5 to 0.4) |
0.128 a −0.6 (−1.5 to 0.3) |
0.866 a 0.0 (−0.6 to 0.5) |
0.160 a 0.5 (−0.3 to 1.4) |
0.124 a −0.4 (−0.9 to 0.1) |
| Exercise | 14.0 ± 6.4 (7.4 to 20.7) | 3.4 ± 7.6 (−8.7 to 15.5) | 11.6 ± 5.2 (−1.2 to 24.5) | 8.3 ± 4.3 (1.4 to 15.2) | 10.7 ± 8.2 (4.8 to 16.5) | 13.1 ± 6.5 (7.1 to 19.1) |
0.571 a 2.4 (−7.7 to 12.5) | 0.313 a −4.9 (−16.4 to 6.5) | 0.062 a −10.7 (−22.1 to 0.7) |
0.415 a −3.4 (−13.6 to 6.9) |
0.504 a −2.4 (−10.1 to 5.2) |
| Recovery | 8.9 ± 5.6 (3.0 to 14.8) | 4.6 ± 6.1 (−5.0 to 14.4) | 18.8 ± 4.8 (6.9 to 30.8) | 0.7 ± 1.7 (−2.0 to 3.5) | 6.9 ± 6.1 (2.5 to 11.3) | 5.4 ± 6.7 (−0.8 to 11.6) |
0.042 a,* −10.0 (−19.4 to −0.5) |
0.289 a 4.0 (−5.4 to 13.3) |
0.313 a −4.2 (−13.5 to 5.1) |
0.016 a,* −18.1 (−28.9 to −7.3) |
0.652 a −1.5 (−5.4 to 8.4) |
| Parameters | HFpEF | HFrEF | HFpEF | HFrEF | HFpEF vs. HFrEF | Weber Class A + B vs. Weber Class C | HFpEF vs. HFrEF | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Weber Class A + B (n = 6) | Weber Class C (n = 4) | Weber Class A + B (n = 3) | Weber Class C (n = 4) | (n = 10) | (n = 7) | p-Value | p-Value | p-Value | p-Value | p-Value | |
|
Mean ± SD (95% CI) |
Mean ± SD (95% CI) |
Mean ± SD (95% CI) |
Mean ± SD (95% CI) |
Mean ± SD (95% CI) |
Mean ± SD (95% CI) | Mean Difference A + B (95% CI) | Mean Difference C (95% CI) | Mean Difference HFpEF (95% CI) | Mean Difference HFrEF (95% CI) | Mean Difference (95% CI) | |
| PT, Nm |
125.5 ± 25.7 (98.6 to 152.4) |
68.2 ± 10.8 (51.1 to 85.3) |
136.8 ± 47.5 (18.7 to 254.8) |
83.4 ± 38.8 (21.6 to 145.1) |
102.6 ± 35.8 (77.0 to 128.2) |
106.3 ± 48.2 (61.7 to 150.8) |
>0.999 b −2.0 (−74.4 to 47.6) |
0.500 a −15.2 (−74.7 to 44.4) |
0.019 b,* 64.8 (11.4 to 83.6) |
0.190 a 53.4 (−41.3 to 148.1) |
0.887 b 10.4 (−49.8 to 37.2) |
| PT/Body Mass, Nm.kg |
139.2 ± 28.9 (108.9 to 169.6) |
82.4 ± 1.9 (79.4 to 85.3) |
159.7 ± 32.6 (78.6 to 240.7) |
105.2 ± 37.9 (45.0 to 165.5) |
116.5 ± 36.4 (90.4 to 142.5) |
128.6 ± 43.8 (88.0 to 169.1) |
0.414 a −20.5 (−84.6 to 43.7) |
0.314 a −22.9 (−83.0 to 37.3) |
0.005*a 56.8 (26.5 to 87.2) |
0.099 a 54.4 (−15.1 to 123.9) |
0.561 a −12.1 (−56.3 to 32.1) |
| Maximal Repetition Total Work, J |
143.5 ± 32.2 (109.7 to 177.3) |
79.5 ± 15.7 (54.4 to 104.5) |
151.5 ± 43.9 (42.6 to 260.5) |
99.4 ± 45.2 (27.5 to 171.4) |
117.9 ± 41.9 (87.9 to 147.8) |
121.8 ± 49.4 (76.1 to 167.4) |
0.796 a −8.0 (−96.7 to 80.7) |
0.454 a −20.0 (−88.5 to 48.6) |
0.003 a,* 64.1 (28.4 to 99.7) |
0.191 a 52.1 (−37.9 to 142.1) |
0.869 a −3.9 (−53.9 to 46.2) |
| Work/Body Weight, % |
159.2 ± 36.6 (120.8 to 197.7) |
95.9 ± 10.5 (79.1 to 112.6) |
177.9 ± 26.3 (112.5 to 243.3) |
125.1 ± 40.9 (60.0 to 190.1) |
133.9 ± 43.1 (103.1 to 164.7) |
147.7 ± 43.2 (107.8 to 187.6) |
0.417 a −18.7 (−71.7 to 34.3) |
0.251 a −29.2 (−92.1 to 33.8) |
0.007 a,* 63.4 (24.8 to 101.9) |
0.093 a 52.9 (−12.8 to 118.5) |
0.527 a −13.8 (−59.7 to 32.1) |
| Total Work, J |
2253.5 ± 523.0 (1704.6 to 2802.3) |
1245.4 ± 193.5 (937.5 to 1553.2) |
2351.1 ± 674.5 (675.7 to 4026.6) |
1398.2 ± 593.7 (453.5 to 2342.9) |
1850.2 ± 659.9 (1378.2 to 2322.3) |
1806.6 ± 766.4 (1097.9 to 2515.4) |
0.839 a −98.7 (−1448.2 to 1252.8) |
0.653 a −152.9 (−1055.7 to 749.9) |
0.004 a,* 1008.1 (450.3 to 1565.9) |
0.122 a 952.9 (−396.0 to 2301.8) |
0.905 a 43.6 (−736.2 to 823.4) |
| Work Fatigue, % |
36.5 ± 11.0 (24.9 to 48.0) |
32.8 ± 19.2 (2.2 to 63.4) |
40.0 ± 9.3 (17.0 to 63.0) |
48.1 ± 2.0 (44.9 to 51.3) |
35.0 ± 13.9 (25.0 to 45.0) |
44.6 ± 7.0 (38.1 to 51.1) |
0.634 a −3.6 (−21.7 to 14.6) |
0.209 a −15.3 (−45.7 to 15.1) |
0.747 a 3.7 (−24.9 to 32.2) |
0.267 a −8.1 (−30.1 to 13.9) |
0.133 b −8.3 (−15.1 to 1.7) |
| Average Power, W |
189.4 ± 47.1 (140.0 to 238.8) |
103.0 ± 22.7 (66.9 to 139.1) |
206.4 ± 78.1 (12.4 to 400.3) |
114.4 ± 54.6 (27.6 to 201.2) |
154.8 ± 58.2 (113.1 to 196.5) |
153.8 ± 77.1 (82.6 to 225.1) |
0.753 a −17.0 (−181.1 to 147.1) |
0.719 a −11.4 (−93.4 to 70.6) |
0.005 a,* 86.4 (34.4 to 138.4) |
0.168 a 92.0 (−64.6 to 248.4) |
0.978 a 1.0 (−75.2 to 77.2) |
| Parameters | HFpEF | HFrEF | HFpEF | HFrEF | HFpEF vs. HFrEF | Weber Class A + B vs. Weber Class C | HFpEF vs. HFrEF | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Weber Class A + B (n = 11) | Weber Class C (n = 5) | Weber Class A + B (n = 7) | Weber Class C (n = 5) | (n = 16) | (n = 12) | p-Value | p-Value | p-Value | p-Value | p-Value | |
|
Mean ± SD (95% CI) |
Mean ± SD (95% CI) |
Mean ± SD (95% CI) |
Mean ± SD (95% CI) |
Mean ± SD (95% CI) |
Mean ± SD (95% CI) | Mean Difference A + B (95% CI) | Mean Difference C (95% CI) | Mean Difference HFpEF (95% CI) | Mean Difference HFrEF (95% CI) | Mean Difference (95% CI) | |
| Echo intensity, 0–255 | |||||||||||
| m. rectus femoris |
14.1 ± 8.7 (8.2 to 19.9) |
29.7 ± 8.4 (19.3 to 40.2) |
13.1 ± 5.5 (8.0 to 18.2) |
15.1 ± 6.8 (6.8 to 23.5) |
19.0 ± 11.2 (13.0 to 25.0) |
13.9 ± 5.9 (10.2 to 17.7) |
0.786 a 0.9 (−6.2 to 8.1) |
0.017 a,* 14.6 (3.4 to 25.9) |
0.009 a,* −15.7 (−26.2 to −5.2) |
0.606 a −2.0 (−10.6 to 6.6) |
0.140 a 5.0 (−1.8 to 11.8) |
| Muscle thickness, cm | |||||||||||
| m. rectus femoris |
2.1 ± 0.5 (1.7 to 2.4) |
1.7 ± 0.3 (1.3 to 2.1) |
1.9 ± 0.4 (1.5 to 2.3) |
1.5 ± 0.5 (0.9 to 2.1) |
2.0 ± 0.5 (1.7 to 2.2) |
1.7 ± 0.5 (1.4 to 2.0) |
0.435 b 0.2 (−0.3 to 0.9) |
0.397 a 0.2 (−0.4 to 0.8) |
0.134 a 0.4 (−0.1 to 0.8) |
0.145 b 0.3 (−0.2 to 1.0) |
0.196 a 0.2 (−0.1 to 0.6) |
| (n = 10) | (n = 4) | (n = 7) | (n = 5) | ||||||||
| m. quadriceps femoris |
3.8 ± 0.7 (3.3 to 4.3) |
3.0 ± 0.4 (2.3 to 3.6) |
3.6 ± 0.8 (2.8 to 4.3) |
2.8 ± 1.0 (1.6 to 4.0) |
3.6 ± 0.7 (3.1 to 4.0) |
3.2 ± 0.9 (2.6 to 3.8) |
0.570 a 0.2 (−0.6 to 1.1) |
0.734 a 0.2 (−1.1 to 1.4) |
0.023 a,* 0.8 (0.1 to 1.5) |
0.203 a 0.8 (−1.5 to 2.0) |
0.364 a 0.4 (−0.6 to 1.3) |
| Groups | TSI × PT | TSI × peak VO2 | RF_EI × PT | RF_EI × peak VO2 | RF_MT × PT | RF_MT × Peak VO2 | |
|---|---|---|---|---|---|---|---|
| HFpEF (Weber A + B) | r | −0.429 b | 0.008 a | −0.331 a | −0.060 a | 0.235 a | 0.687 a |
| p | 0.419 | 0.988 | 0.320 | 0.861 | 0.487 | 0.020 * | |
| HFrEF (Weber A + B) | r | 0.626 a | 0.999 a | 0.151 a | 0.294 a | 0.649 a | 0.612 a |
| p | 0.569 | 0.010 * | 0.747 | 0.522 | 0.114 | 0.144 | |
| HFpEF (Weber C) | r | −0.417 a | −0.786 a | 0.121 a | −0.537 a | 0.405 a | 0.937 a |
| p | 0.583 | 0.214 | 0.847 | 0.350 | 0.499 | 0.019 * | |
| HFrEF (Weber C) | r | 0.311 a | 0.476 a | −0.228 a | 0.152 a | 0.880 a | 0.838 a |
| p | 0.689 | 0.524 | 0.713 | 0.807 | 0.049 * | 0.077 | |
| HFpEF | r | −0.697 b | −0.586 a | −0.570 a | −0.581 a | 0.398 a | 0.672 a |
| p | 0.031 * | 0.075 | 0.021 * | 0.018* | 0.127 | 0.004 * | |
| HFrEF | r | −0.229 a | −0.291 a | −0.074 a | 0.079 a | 0.778 a | 0.751 a |
| p | 0.621 | 0.527 | 0.820 | 0.808 | 0.003* | 0.005 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vale-Lira, A.; Turri-Silva, N.; Verboven, K.; Durigan, J.L.Q.; de Lima, A.C.G.B.; Bottaro, M.; Chiappa, G.R.; Hansen, D.; Cipriano, G., Jr. Muscle-Skeletal Abnormalities and Muscle Oxygenation during Isokinetic Strength Exercise in Heart Failure with Preserved Ejection Fraction Phenotype: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 709. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19020709
Vale-Lira A, Turri-Silva N, Verboven K, Durigan JLQ, de Lima ACGB, Bottaro M, Chiappa GR, Hansen D, Cipriano G Jr. Muscle-Skeletal Abnormalities and Muscle Oxygenation during Isokinetic Strength Exercise in Heart Failure with Preserved Ejection Fraction Phenotype: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2022; 19(2):709. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19020709
Chicago/Turabian StyleVale-Lira, Amanda, Natália Turri-Silva, Kenneth Verboven, João Luiz Quagliotti Durigan, Alexandra Corrêa G. B. de Lima, Martim Bottaro, Gaspar R. Chiappa, Dominique Hansen, and Gerson Cipriano, Jr. 2022. "Muscle-Skeletal Abnormalities and Muscle Oxygenation during Isokinetic Strength Exercise in Heart Failure with Preserved Ejection Fraction Phenotype: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 19, no. 2: 709. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19020709