
Parental Self-Compassion and Child Adjustment: The Mediating Role of Parental Depressive Symptoms


Abstract
:1. Introduction
1.1. Self-Compassion and Depression
1.2. Parental Self-Compassion and Child Adjustment
1.3. The Present Study
2. Materials and Methods
2.1. Participants and Procedure
2.2. Measures
2.3. Analytic Strategies
3. Results
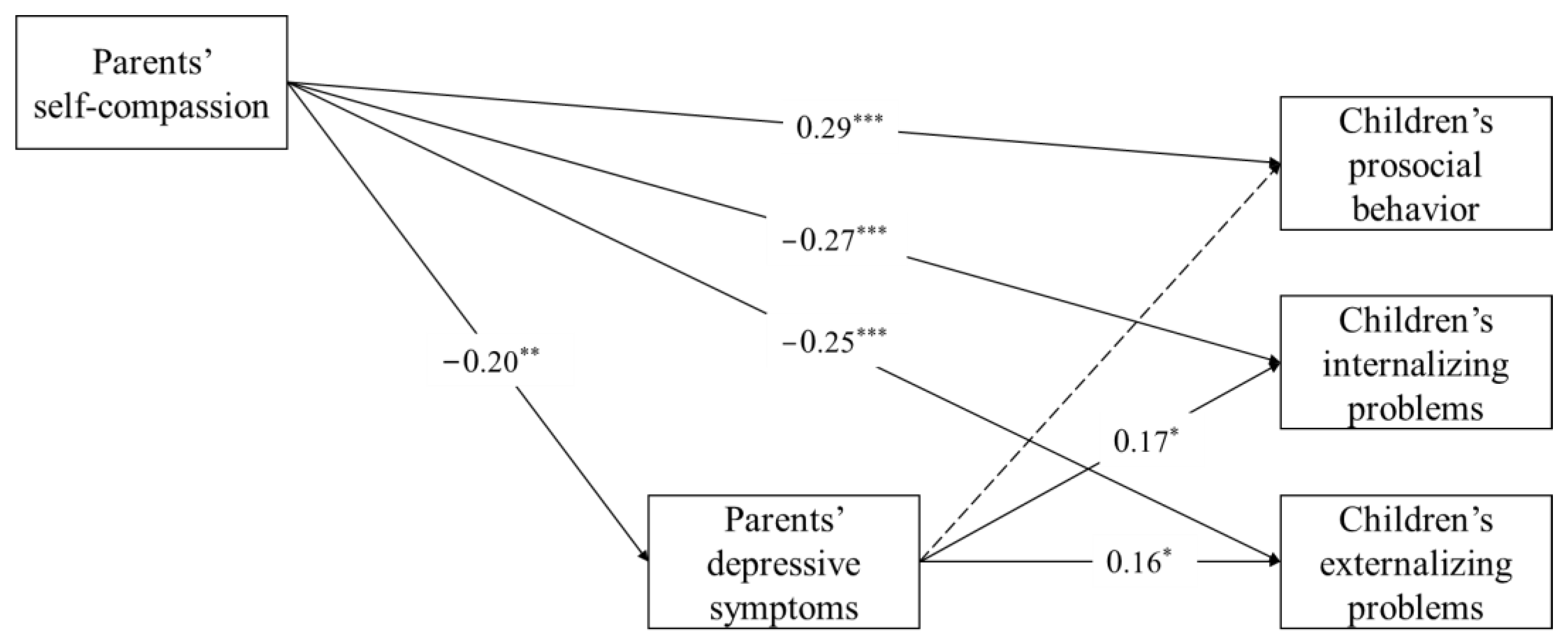
3.1. Parents’ Depressive Symptoms as a Mediator
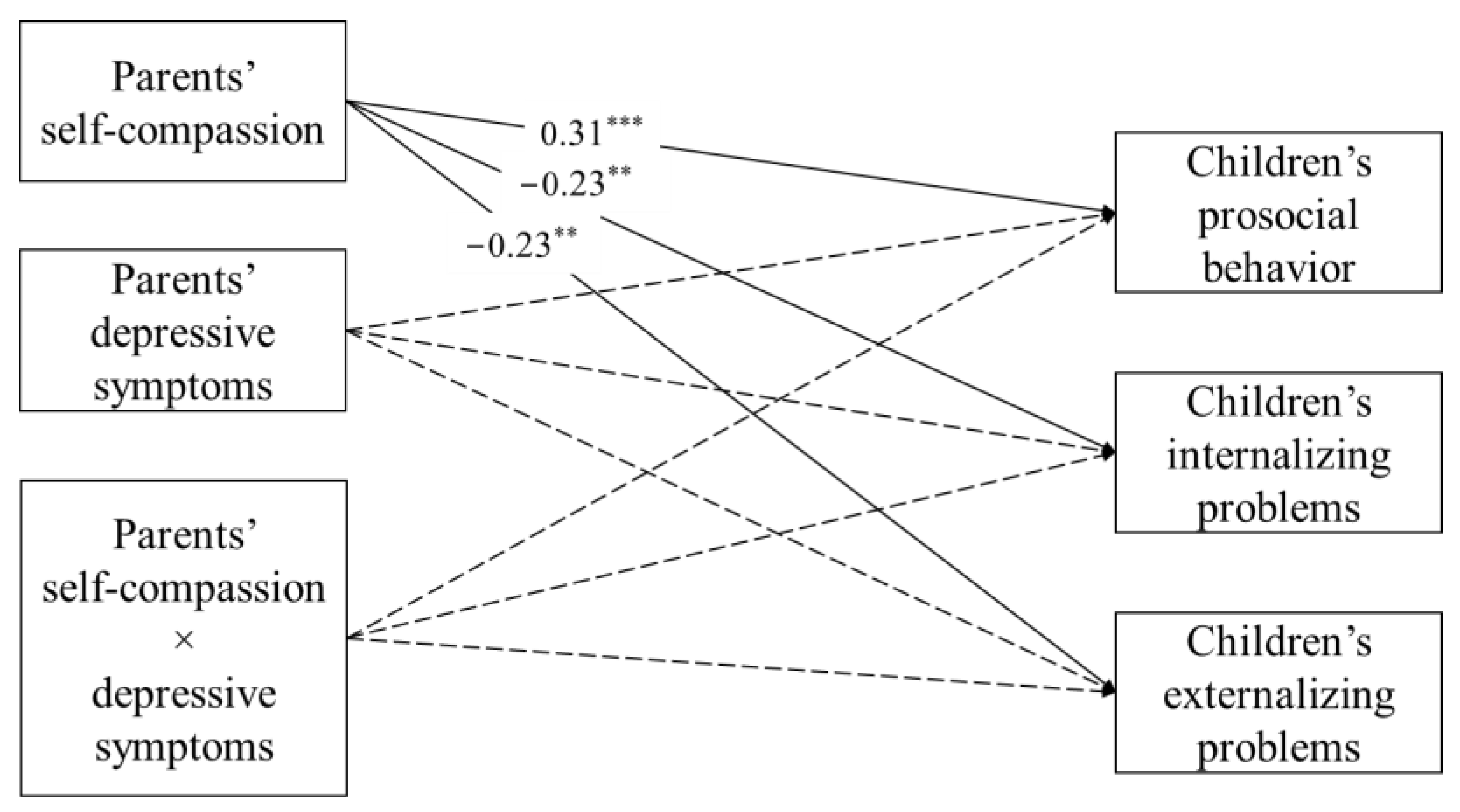
3.2. Alternative Hypothesis: Moderating Effect between Parents’ Self-Compassion and Depressive Symptoms
4. Discussion
5. Conclusions
Limitations and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Davé, S.; Petersen, I.; Sherr, L.; Nazareth, I. Incidence of Maternal and Paternal Depression in Primary Care. Arch. Pediatr. Adolesc. Med. 2010, 164, 1038–1044. [Google Scholar] [CrossRef] [Green Version]
- Cents, R.A.M.; Diamantopoulou, S.; Hudziak, J.J.; Jaddoe, V.W.V.; Hofman, A.; Verhulst, F.C.; Berg, M.P.L.-V.D.; Tiemeier, H. Trajectories of maternal depressive symptoms predict child problem behaviour: The Generation R Study. Psychol. Med. 2012, 43, 13–25. [Google Scholar] [CrossRef]
- Cheung, R.Y.M.; Cheng, W.Y.; Li, J.-B.; Lam, C.B.; Chung, K.K.H. Parents’ Depressive Symptoms and Child Adjustment: The Mediating Role of Mindful Parenting and Children’s Self-Regulation. Mindfulness 2021, 12, 2729–2742. [Google Scholar] [CrossRef]
- El-Sheikh, M.; Kelly, R.J.; Bagley, E.J.; Wetter, E.K. Parental depressive symptoms and children’s sleep: The role of family conflict. J. Child Psychol. Psychiatry 2012, 53, 806–814. [Google Scholar] [CrossRef] [Green Version]
- Letourneau, N.; Apron The APrON Team; Leung, B.; Ntanda, H.; Dewey, D.; Deane, A.J.; Giesbrecht, G.F. Maternal and paternal perinatal depressive symptoms associate with 2- and 3-year-old children’s behaviour: Findings from the APrON longitudinal study. BMC Pediatr. 2019, 19, 435. [Google Scholar] [CrossRef] [Green Version]
- MacBeth, A.; Gumley, A. Exploring compassion: A meta-analysis of the association between self-compassion and psychopathology. Clin. Psychol. Rev. 2012, 32, 545–552. [Google Scholar] [CrossRef] [Green Version]
- Cicchetti, D.; Rogosch, F.A. Equifinality and multifinality in developmental psychopathology. Dev. Psychopathol. 1996, 8, 597–600. [Google Scholar] [CrossRef] [Green Version]
- Campbell, S.B.; Ewing, L.J. Follow-up of Hard-to-Manage Preschoolers: Adjustment at Age 9 and Predictors of Continuing Symptoms. J. Child Psychol. Psychiatry 1990, 31, 871–889. [Google Scholar] [CrossRef]
- Goodman, S.H.; Gotlib, I.H. Risk for psychopathology in the children of depressed mothers: A developmental model for understanding mechanisms of transmission. Psychol. Rev. 1999, 106, 458–490. [Google Scholar] [CrossRef]
- Gravener, J.A.; Rogosch, F.A.; Oshri, A.; Narayan, A.J.; Cicchetti, D.; Toth, S.L. The relations among maternal depressive disorder, maternal expressed emotion, and toddler behavior problems and attachment. J. Abnorm. Child Psychol. 2011, 40, 803–813. [Google Scholar] [CrossRef] [Green Version]
- Ramchandani, P.G.; Psychogiou, L.; Vlachos, H.; Iles, J.; Sethna, V.; Netsi, E.; Lodder, A. Paternal depression: An examination of its links with father, child and family functioning in the postnatal period. Depress. Anxiety 2011, 28, 471–477. [Google Scholar] [CrossRef] [Green Version]
- Sethna, V.; Murray, L.; Ramchandani, P.G. Depressed fathers’ speech to their 3-month-old infants: A study of cognitive and mentalizing features in paternal speech. Psychol. Med. 2012, 42, 2361–2371. [Google Scholar] [CrossRef] [Green Version]
- Neff, K. Self-Compassion: An Alternative Conceptualization of a Healthy Attitude toward Oneself. Self Identity 2003, 2, 85–101. [Google Scholar] [CrossRef] [Green Version]
- Krieger, T.; Altenstein, D.; Baettig, I.; Doerig, N.; Holtforth, M.G. Self-Compassion in Depression: Associations with Depressive Symptoms, Rumination, and Avoidance in Depressed Outpatients. Behav. Ther. 2013, 44, 501–513. [Google Scholar] [CrossRef]
- Krieger, T.; Berger, T.; Holtforth, M.G. The relationship of self-compassion and depression: Cross-lagged panel analyses in depressed patients after outpatient therapy. J. Affect. Disord. 2016, 202, 39–45. [Google Scholar] [CrossRef]
- Raes, F. The Effect of Self-Compassion on the Development of Depression Symptoms in a Non-clinical Sample. Mindfulness 2011, 2, 33–36. [Google Scholar] [CrossRef]
- López, A.; Sanderman, R.; Schroevers, M.J. A Close Examination of the Relationship Between Self-Compassion and Depressive Symptoms. Mindfulness 2018, 9, 1470–1478. [Google Scholar] [CrossRef] [Green Version]
- Haukaas, R.B.; Gjerde, I.B.; Varting, G.; Hallan, H.E.; Solem, S. A Randomized Controlled Trial Comparing the Attention Training Technique and Mindful Self-Compassion for Students with Symptoms of Depression and Anxiety. Front. Psychol. 2018, 9, 827. [Google Scholar] [CrossRef]
- Ferrari, M.; Hunt, C.; Harrysunker, A.; Abbott, M.J.; Beath, A.; Einstein, D.A. Self-Compassion Interventions and Psychosocial Outcomes: A Meta—Analysis of RCTs. Mindfulness 2019, 10, 1455–1473. [Google Scholar] [CrossRef]
- Bögels, S.M.; Hellemans, J.; van Deursen, S.; Römer, M.; van der Meulen, R. Mindful Parenting in Mental Health Care: Effects on Parental and Child Psychopathology, Parental Stress, Parenting, Coparenting, and Marital Functioning. Mindfulness 2014, 5, 536–551. [Google Scholar] [CrossRef]
- Mann, J.; Kuyken, W.; O’Mahen, H.; Ukoumunne, O.C.; Evans, A.; Ford, T. Manual Development and Pilot Randomised Controlled Trial of Mindfulness-Based Cognitive Therapy Versus Usual Care for Parents with a History of Depression. Mindfulness 2016, 7, 1024–1033. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Potharst, E.S.; Zeegers, M.; Bögels, S.M. Mindful with Your Toddler Group Training: Feasibility, Acceptability, and Effects on Subjective and Objective Measures. Mindfulness 2021, 12, 489–503. [Google Scholar] [CrossRef] [Green Version]
- Psychogiou, L.; Legge, K.; Parry, E.; Mann, J.; Nath, S.; Ford, T.; Kuyken, W. Self-Compassion and Parenting in Mothers and Fathers with Depression. Mindfulness 2016, 7, 896–908. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheung, R.Y.M.; Boise, C.; Cummings, E.M.; Davies, P.T. Mothers’ and Fathers’ Roles in Child Adjustment: Parenting Practices and Mothers’ Emotion Socialization as Predictors. J. Child Fam. Stud. 2018, 27, 4033–4043. [Google Scholar] [CrossRef]
- Cummings, E.M.; Cheung, R.Y.M.C.; Koss, K.; Davies, P. Parental Depressive Symptoms and Adolescent Adjustment: A Prospective Test of an Explanatory Model for the Role of Marital Conflict. J. Abnorm. Child Psychol. 2014, 42, 1153–1166. [Google Scholar] [CrossRef] [Green Version]
- Sheeber, L.; Davis, B.; Hops, H. Gender-specific vulnerability to depression in children of depressed mothers. In Children of Depressed Parents: Mechanisms of Risk and Implications for Treatment; Goodman, S.H., Gotlib, I.H., Eds.; American Psychological Association Press: Washington, DC, USA, 2002; pp. 253–274. [Google Scholar]
- Connell, A.M.; Goodman, S.H. The association between psychopathology in fathers versus mothers and children’s internalizing and externalizing behavior problems: A meta-analysis. Psychol. Bull. 2002, 128, 746–773. [Google Scholar] [CrossRef]
- Lee, C.-Y.S.; Anderson, J.R.; Horowitz, J.L.; August, G.J. Family Income and Parenting: The Role of Parental Depression and Social Support. Fam. Relat. 2009, 58, 417–430. [Google Scholar] [CrossRef]
- Reising, M.M.; Watson, K.H.; Hardcastle, E.J.; Merchant, M.J.; Roberts, L.; Forehand, R.; Compas, B.E. Parental Depression and Economic Disadvantage: The Role of Parenting in Associations with Internalizing and Externalizing Symptoms in Children and Adolescents. J. Child Fam. Stud. 2013, 22, 335–343. [Google Scholar] [CrossRef] [Green Version]
- Goelman, H.; Zdaniuk, B.; Boyce, W.T.; Armstrong, J.M.; Essex, M.J. Maternal mental health, child care quality, and children’s behavior. J. Appl. Dev. Psychol. 2014, 35, 347–356. [Google Scholar] [CrossRef]
- Brett, B.E.; Stern, J.; Gross, J.T.; Cassidy, J. Maternal Depressive Symptoms and Preschoolers’ Helping, Sharing, and Comforting: The Moderating Role of Child Attachment. J. Clin. Child Adolesc. Psychol. 2020, 1–14. [Google Scholar] [CrossRef]
- Raes, F.; Pommier, E.; Neff, K.D.; Van Gucht, D. Construction and factorial validation of a short form of the Self-Compassion Scale. Clin. Psychol. Psychother. 2010, 18, 250–255. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L. The PHQ-9: A New Depression Diagnostic and Severity Measure. Psychiatr. Ann. 2002, 32, 509–515. [Google Scholar] [CrossRef] [Green Version]
- Goodman, R. The Strengths and Difficulties Questionnaire: A Research Note. J. Child Psychol. Psychiatry 1997, 38, 581–586. [Google Scholar] [CrossRef] [PubMed]
- Muthén, L.K.; Muthén, B.O. MPLUS: Statistical Analysis with Latent Variables: User’s Guide; Version 8; Muthén & Muthén: Los Angeles, CA, USA, 2017. [Google Scholar]
- Cummings, E.M.; Cheung, R.Y.M.C.; Davies, P. Prospective Relations Between Parental Depression, Negative Expressiveness, Emotional Insecurity, and Children’s Internalizing Symptoms. Child Psychiatry Hum. Dev. 2013, 44, 698–708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carlo, G.; Padilla-Walker, L.M.; Day, R.D. A Test of the Economic Strain Model on Adolescents’ Prosocial Behaviors. J. Res. Adolesc. 2011, 21, 842–848. [Google Scholar] [CrossRef]
- Elgar, F.J.; Mills, R.S.L.; McGrath, P.; Waschbusch, D.; Brownridge, D.A. Maternal and Paternal Depressive Symptoms and Child Maladjustment: The Mediating Role of Parental Behavior. J. Abnorm. Child Psychol. 2007, 35, 943–955. [Google Scholar] [CrossRef]
- Fabes, R.A.; Eisenberg, N. Meta-analyses of age and sex differences in children’s and adolescents’ prosocial behavior. Handb. Child Psychol. 1998, 3, 1–29. [Google Scholar]
- Streiner, D.L. Starting at the Beginning: An Introduction to Coefficient Alpha and Internal Consistency. J. Pers. Assess. 2003, 80, 99–103. [Google Scholar] [CrossRef]
- Meng, R.; Yu, Y.; Chai, S.; Luo, X.; Gong, B.; Liu, B.; Hu, Y.; Luo, Y.; Yu, C. Examining psychometric properties and measurement invariance of a Chinese version of the Self-Compassion Scale—Short Form (SCS-SF) in nursing students and medical workers. Psychol. Res. Behav. Manag. 2019, 12, 793–809. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Variable | M | SD | (1) | (2) | (3) | (4) | (5) | (6) | (7) |
|---|---|---|---|---|---|---|---|---|---|
| (1) Child gender | — | — | — | ||||||
| (2) Parent gender | — | — | 0.00 | — | |||||
| (3) Monthly family income (in RMB) | 33,406.31 | 31,861.49 | 0.10 | −0.41 *** | — | ||||
| (4) Parents’ self-compassion | 3.18 | 0.46 | −0.01 | 0.03 | 0.10 | — | |||
| (5) Parents’ depressive symptoms | 0.29 | 0.51 | 0.00 | −0.01 | −0.02 | −0.21 ** | — | ||
| (6) Children’s prosocial behavior | 2.24 | 0.61 | 0.16 * | −0.00 | 0.10 | 0.31 *** | −0.12 | — | |
| (7) Children’s externalizing problems | 1.51 | 0.28 | 0.14 | 0.02 | −0.22 ** | −0.33 *** | 0.26 *** | −0.20 ** | — |
| (8) Children’s internalizing problems | 1.76 | 0.31 | −0.03 | 0.07 | −0.13 | −0.30 *** | 0.23 ** | −0.24 *** | 0.49 *** |
| Parameter | Unstandardized B (SE) | Standardized β |
|---|---|---|
| Parents’ self-compassion → | ||
| Parents’ depressive symptoms | −0.21 (0.08) | −0.20 ** |
| Children’s prosocial behavior | 0.37 (0.09) | 0.29 *** |
| Children’s internalizing problems | −0.16 (0.04) | −0.27 *** |
| Children’s externalizing problems | −0.17 (0.05) | −0.25 *** |
| Parents’ depressive symptoms → | ||
| Children’s prosocial behavior | −0.06 (0.08) | −0.05 |
| Children’s internalizing problems | 0.09 (0.04) | 0.17 * |
| Children’s externalizing problems | 0.10 (0.04) | 0.16 * |
| Child gender → | ||
| Parents’ depressive symptoms | 0.01 (0.07) | 0.01 |
| Children’s prosocial behavior | 0.19 (0.08) | 0.16 * |
| Children’s internalizing problems | 0.09 (0.04) | 0.15 * |
| Children’s externalizing problems | −0.01 (0.04) | −0.02 |
| Parent gender → | ||
| Parents’ depressive symptoms | −0.04 (0.08) | −0.04 |
| Children’s prosocial behavior | 0.03 (0.09) | 0.02 |
| Children’s internalizing problems | −0.02 (0.04) | −0.04 |
| Children’s externalizing problems | 0.02 (0.04) | 0.04 |
| Monthly family income → | ||
| Parents’ depressive symptoms | −0.05 (0.03) | −0.13 |
| Children’s prosocial behavior | 0.06 (0.04) | 0.12 |
| Children’s internalizing problems | −0.05 (0.02) | −0.23 ** |
| Children’s externalizing problems | −0.03 (0.02) | −0.12 |
| Parents’ self-compassion ←→ | ||
| Child gender | −0.00 (0.02) | −0.02 |
| Parent gender | 0.01 (0.02) | 0.03 |
| Family income | 0.06 (0.04) | 0.11 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheung, R.Y.M.; Li, Z.; Ho, A.P.L. Parental Self-Compassion and Child Adjustment: The Mediating Role of Parental Depressive Symptoms. Int. J. Environ. Res. Public Health 2022, 19, 5133. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19095133
Cheung RYM, Li Z, Ho APL. Parental Self-Compassion and Child Adjustment: The Mediating Role of Parental Depressive Symptoms. International Journal of Environmental Research and Public Health. 2022; 19(9):5133. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19095133
Chicago/Turabian StyleCheung, Rebecca Y. M., Zechen Li, and Audrey Pui Lam Ho. 2022. "Parental Self-Compassion and Child Adjustment: The Mediating Role of Parental Depressive Symptoms" International Journal of Environmental Research and Public Health 19, no. 9: 5133. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19095133