The Geography of Diabetes in London, Canada: The Need for Local Level Policy for Prevention and Management


Abstract
:1. Introduction
2. Methodology
2.1. Study Population
2.2. Study Design and Variables
2.3. Analyses
2.4. Ethical Approval
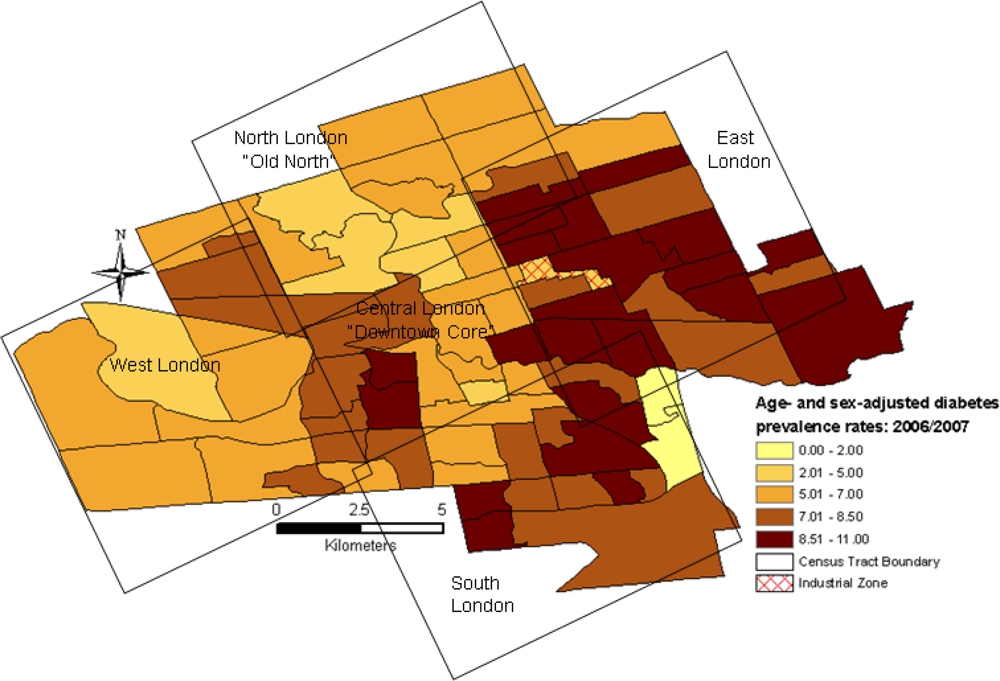
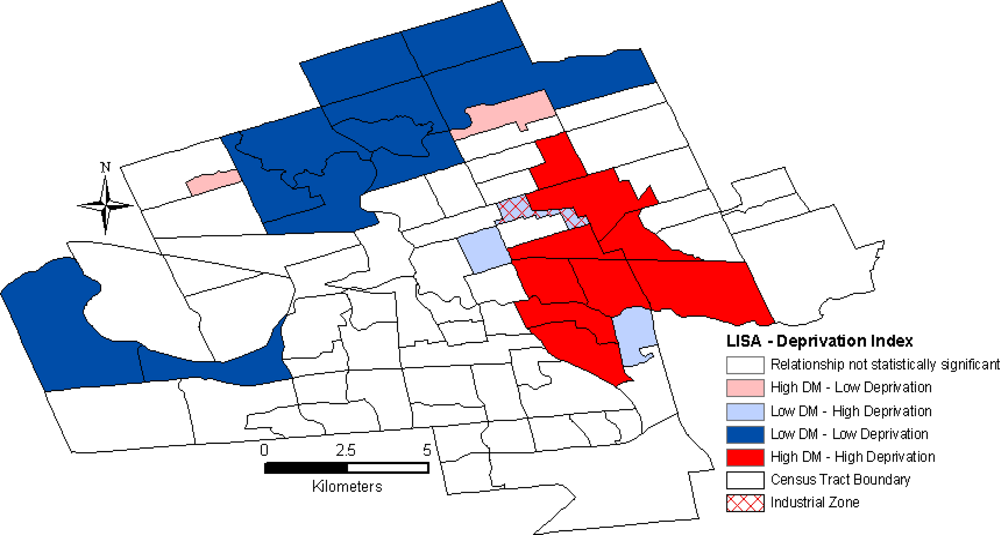
3. Results
4. Discussion
4.1. Policy Options
4.2. Methodological Limitations
4.3. Future Research
5. Conclusions
Acknowledgments
References
- Booth, GL; Hux, JE; Fang, J; Chan, BT. Time trends and geographic disparities in acute complications of diabetes in Ontario, Canada. Diabetes Care 2005, 28, 1045–1050. [Google Scholar]
- Creatore, MI; Gozdyra, P; Booth, GL; Ross, K; Glazier, RH. Socioeconomic status and diabetes. In Neighbourhoods Environments and Resources for Healthy Living—A Focus on Diabetes in Toronto: An ICES Practice Atlas; Glazier, RH, Booth, GL, Eds.; Institute for Clinical Evaluative Sciences: Toronto, ON, Canada, 2007; pp. 36–56. [Google Scholar]
- Robert, SA. Community-level socioeconomic status effects on adult health. J. Health Soc. Behav 1998, 39, 18–37. [Google Scholar]
- Yu, VL; Raphael, D. Identifying and addressing the social determinants of the incidence and successful management of type 2 diabetes mellitus in Canada. Can. J. Public Health 2004, 95, 366–368. [Google Scholar]
- Hartwell, H. Health inequalities—fair inequality? Perspect. Public Health 2009, 129, 194. [Google Scholar]
- Glazier, RH; Bajcar, J; Kennie, NR; Willson, K. A systematic review of interventions to improve diabetes care in socially disadvantaged populations. Diabetes Care 2006, 29, 1675–1688. [Google Scholar]
- Luginaah, I; Jerrett, M; Elliott, S; Eyles, J; Parizeau, K; Birch, S; Abernathy, T; Veenstra, G; Hutchinson, B; Giovis, C. Health profiles of Hamilton: spatial characterisation of neighbourhoods for health investigations. GeoJournal 2001, 53, 135–147. [Google Scholar]
- Hux, JE; Ivis, F; Flintoft, V; Bica, A. Diabetes in Ontario: Determination of prevalence and incidence using a validated administrative data algorithm. Diabetes Care 2002, 25, 512–516. [Google Scholar]
- 2006 Community Profiles Catalogue No 92-591-XWE; Statistics Canada: Ottawa, ON, Canada, 2007.
- Pickett, KE; Pearl, M. Multilevel analyses of neighbourhood socioeconomic context and health outcomes: a critical review. J. Epidemiol. Community Health 2001, 55, 111–122. [Google Scholar]
- Birch, S; Jerrett, M; Eyles, J. Heterogeneity in the determinants of health and illness: the example of socioeconomic status and smoking. Soc. Sci. Med 2000, 51, 307–317. [Google Scholar]
- Jerrett, M; Eyles, J; Cole, D. Socioeconomic and environmental covariates of premature mortality in Ontario. Soc. Sci. Med 1998, 47, 33–49. [Google Scholar]
- Wilkinson, RG. Unhealthy Societies: the Afflictions of Inequality; Routledge: London, UK, 1996. [Google Scholar]
- Townsend, P; Phillimore, P; Beattie, A. Health and Deprivation: Inequality and the North; Croom Helm Ltd: Kent, UK, 1988. [Google Scholar]
- Gilliland, J; Ross, N. Opportunities for video lottery terminal gambling in Montreal: an environmental analysis. Can. J. Public Health 2005, 96, 55–59. [Google Scholar]
- Jolliffe, IT. Principal Component Analysis; Springer-Verlag: New York, NY, USA, 1986. [Google Scholar]
- Kaiser, HF. The varimax criterion for analytic rotation in factor analysis. Psychometrika 1958, 23, 187–201. [Google Scholar]
- Anselin, L. Local indicators of spatial association LISA. Geogr. Anal 1995, 27, 94–115. [Google Scholar]
- Fotheringham, AS; Brunsdon, C; Charlton, N. Quantitative geography; Sage: London, UK, 2000. [Google Scholar]
- Lipscombe, LL. The growing prevalence of diabetes in Ontario: are we prepared? Healthc. Q 2007, 10, 23–25. [Google Scholar]
- Kawachi, I; Kennedy, BP. Health and social cohesion: why care about income inequality? BMJ 1997, 314, 1037–1040. [Google Scholar]
- Everson, SA; Maty, SC; Lynch, JW; Kaplan, GA. Epidemiologic evidence for the relation between socioeconomic status and depression, obesity, and diabetes. J. Psychosom. Res 2002, 53, 891–895. [Google Scholar]
- Hux, JE; Tang, M. Patterns of prevalence and incidence of diabetes. In Diabetes in Ontario: An ICES Practice Atlas; Hux, JE, Booth, GL, Slaughter, PM, Laupacis, A, Eds.; Institute for Clinical Evaluative Sciences: Toronto, ON, Canada, 2003; pp. 2–15. [Google Scholar]
- Ross, NA; Tremblay, SS; Graham, K. Neighbourhood influences on health in Montreal, Canada. Soc. Sci. Med 2004, 59, 1485–1494. [Google Scholar]
- Buckingham, K; Freeman, PR. Sociodemographic and morbidity indicators of need in relation to the use of community health services: observational study. BMJ 1997, 315, 994–996. [Google Scholar]
- South West LHIN. Transforming Health Care: A Community Approach; 2007–2008 Annual Report; South West Local Health Integration Network: London, ON, Canada, 2008. [Google Scholar]
- Harrington, DW; Elliott, SJ. Weighing the importance of neighbourhood: a multilevel exploration of the determinants of overweight and obesity. Soc. Sci. Med 2009, 68, 593–600. [Google Scholar]
- He, M; Beynon, C. Prevalence of overweight and obesity in school-aged children. Can. J. Diet. Pract. Res 2006, 67, 125–129. [Google Scholar]
- He, M; Evans, A. Are parents aware that their children are overweight or obese? Do they care? Can. Fam. Physician 2007, 53, 1493–1499. [Google Scholar]
- Tucker, P; Gilliland, J; Irwin, JD. Splashpads, swings, and shade: parents’ preferences for neighbourhood parks. Can. J. Public Health 2007, 98, 198–202. [Google Scholar]
- Larsen, K; Gilliland, J. Mapping the evolution of ‘food deserts’ in a Canadian city: supermarket accessibility in London, Ontario, 1961–2005. Int. J. Health Geogr 2008, 7, 16. [Google Scholar]
- Lynch, JW; Kaplan, GA; Salonen, JT. Why do poor people behave poorly? Variation in adult health behaviours and psychosocial characteristics by stages of the socioeconomic lifecourse. Soc. Sci. Med 1997, 44, 809–819. [Google Scholar]
- Drewnowski, A; Specter, SE. Poverty and obesity: the role of energy density and energy costs. Am. J. Clin. Nutr 2004, 79, 6–16. [Google Scholar]
- Adler, NE; Newman, K. Socioeconomic disparities in health: pathways and policies. Health Aff 2002, 21, 60–76. [Google Scholar]
- Kirkpatrick, SI; McIntyre, L. The chief public health officer’s report on health inequalities: what are the implications for public health practitioners and researchers? Can. J. Public Health 2009, 100, 93–95. [Google Scholar]
- Rose, G. The Strategy of Preventive Medicine; Oxford University Press: Oxford, UK, 1992. [Google Scholar]
- Luginaah, I. Health geography in Canada: where are we headed? Can. Geogr 2009, 53, 89–97. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| X1 | X2 | X3 | X4 | X5 | X6 | X7 | X8 | X9 | X10 | X11 | X12 | X13 | X14 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Single Parent, X1 | 1.000 | 0.099 | 0.227* | 0.471** | 0.194* | 0.397** | 0.136 | 0.503** | –0.560** | 0.568** | 0.262** | –0.454** | –0.518** | 0.683** |
| Recent Immigrant, X2 | 1.000 | 0.627** | 0.226* | 0.566** | 0.320** | 0.227* | –0.160 | 0.265** | 0.481** | 0.499** | –0.344** | –0.291** | –0.049 | |
| Visible Minority, X3 | 1.000 | 0.550** | 0.241* | 0.279** | 0.150 | –0.122 | 0.178 | 0.449** | 0.319** | –0.128 | –0.130 | 0.026 | ||
| No French/English, X4 | 1.000 | 0.119 | 0.250* | 0.197* | 0.347** | –0.288** | 0.420** | 0.206* | –0.228* | –0.257** | 0.367** | |||
| Rented Dwellings, X5 | 1.000 | 0.514** | 0.455** | 0.264** | –0.053 | 0.647** | 0.797** | –0.829** | –0.654** | 0.252* | ||||
| Unemployment, X6 | 1.000 | 0.305** | 0.154 | –0.128 | 0.583** | 0.694** | –0.525** | –0.458** | 0.327** | |||||
| Not in Labour Force, X7 | 1.000 | 0.255** | –0.006 | 0.284** | 0.330** | –0.376** | –0.230* | 0.193 | ||||||
| Lacking High School, X8 | 1.000 | –0.820** | 0.359** | 0.180 | –0.545** | –0.649** | 0.805** | |||||||
| University Educated, X9 | 1.000 | –0.256** | –0.014 | 0.390** | 0.572** | –0.860** | ||||||||
| LICOa – families, X10 | 1.000 | 0.806** | –0.677** | –0.621** | 0.418** | |||||||||
| LICOa – private, X11 | 1.000 | –0.778** | –0.609** | 0.213* | ||||||||||
| Median Income, X12 | 1.000 | 0.852** | –0.537** | |||||||||||
| Average Income, X13 | 1.000 | –0.668** | ||||||||||||
| DM Prevalence, X14 | 1.000 |
| Component | ||||
|---|---|---|---|---|
| Variables | 1 | 2 | 3 | Communalitiesa |
| Single parent | 0.217 | 0.723 | 0.383 | 0.716 |
| Recent Immigrant | 0.554 | 0.326 | 0.553 | 0.720 |
| Visible Minority | 0.195 | −0.157 | 0.902 | 0.876 |
| Language | 0.027 | 0.424 | 0.766 | 0.767 |
| Rented Dwelling | 0.936 | 0.031 | 0.072 | 0.881 |
| Unemployment | 0.703 | 0.147 | 0.213 | 0.561 |
| Not in Labour Force | 0.502 | 0.056 | 0.040 | 0.257 |
| Education (lacking high school) | 0.215 | 0.905 | −0.056 | 0.868 |
| Education (university or more) | −0.018 | −0.934 | 0.078 | 0.879 |
| Low income–LICO(families) | 0.703 | 0.302 | 0.446 | 0.783 |
| Low income–LICO(individuals) | 0.900 | 0.025 | 0.187 | 0.846 |
| Median household income | −0.849 | −0.420 | −0.013 | 0.898 |
| Mean household income | −0.681 | −0.589 | −0.051 | 0.813 |
| Eigenvalueb | 4.550 | 2.510 | 1.520 | |
| Percentage variance explained | 35.0 | 24.3 | 16.5 | 75.8 |
| Component | ||||||||
|---|---|---|---|---|---|---|---|---|
| Variables | 1 | 2 | 3 | Communalitiesa | ||||
| Male | Female | Male | Female | Male | Female | Male | Female | |
| Single parent | 0.475 | 0.660 | 0.254 | 0.295 | 0.460 | –0.160 | 0.502 | 0.548 |
| Recent Immigrant | –0.297 | –0.209 | 0.757 | 0.785 | 0.161 | 0.006 | 0.687 | 0.660 |
| Language | 0.372 | 0.421 | 0.248 | 0.306 | –0.199 | 0.036 | 0.240 | 0.272 |
| Unemployment | 0.320 | 0.154 | 0.606 | 0.658 | –0.244 | 0.008 | 0.529 | 0.457 |
| Not in Labour Force | –0.051 | 0.375 | 0.570 | 0.395 | –0.094 | 0.684 | 0.337 | 0.765 |
| Education (lacking high school) | 0.910 | 0.929 | 0.039 | 0.076 | –0.004 | 0.031 | 0.830 | 0.869 |
| Education (university or more) | –0.921 | –0.913 | 0.093 | 0.119 | –0.083 | 0.195 | 0.863 | 0.886 |
| Low income–LICO (families) | 0.351 | 0.387 | 0.554 | 0.690 | 0.126 | –0.228 | 0.446 | 0.677 |
| Lowincome–LICO (individuals) | 0.171 | 0.235 | 0.776 | 0.837 | 0.010 | –0.126 | 0.632 | 0.772 |
| Median household income | –0.030 | –0.444 | –0.062 | –0.413 | 0.948 | 0.674 | 0.903 | 0.823 |
| Mean household income | –0.003 | –0.488 | –0.049 | –0.395 | 0.954 | 0.669 | 0.913 | 0.842 |
| Eigenvalueb | 2.387 | 3.160 | 2.214 | 2.900 | 1.877 | 1.500 | ||
| Percentage variance explained | 21.7 | 28.7 | 21.1 | 26.4 | 19.8 | 13.7 | 62.6 | 68.8 |
© 2010 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Tompkins, J.W.; Luginaah, I.N.; Booth, G.L.; Harris, S.B. The Geography of Diabetes in London, Canada: The Need for Local Level Policy for Prevention and Management. Int. J. Environ. Res. Public Health 2010, 7, 2407-2422. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph7052407
Tompkins JW, Luginaah IN, Booth GL, Harris SB. The Geography of Diabetes in London, Canada: The Need for Local Level Policy for Prevention and Management. International Journal of Environmental Research and Public Health. 2010; 7(5):2407-2422. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph7052407
Chicago/Turabian StyleTompkins, Jordan W., Isaac N. Luginaah, Gillian L. Booth, and Stewart B. Harris. 2010. "The Geography of Diabetes in London, Canada: The Need for Local Level Policy for Prevention and Management" International Journal of Environmental Research and Public Health 7, no. 5: 2407-2422. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph7052407