A Multilevel Analysis of Neighbourhood Built and Social Environments and Adult Self-Reported Physical Activity and Body Mass Index in Ottawa, Canada

Abstract
:1. Introduction
2. Methods
2.1. Rapid Risk Factor Surveillance System (RRFSS)
2.2. Ottawa Neighbourhood Study (ONS)
2.3. Neighbourhood Environments
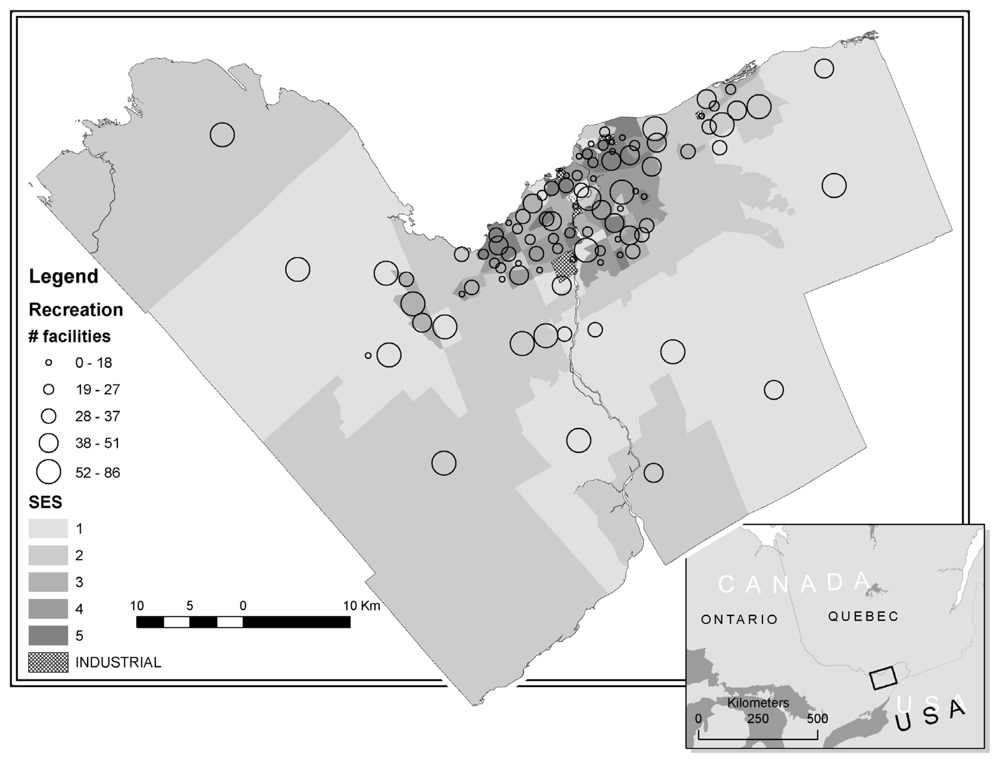
2.3.1. Recreation Environment
2.3.2. Food Environment
2.3.3. Social Environment
2.4. Individual-Level Data
2.4.1. Physical Activity
2.4.2. Overweight and Obesity
2.5. Covariates
2.6. Statistical Analysis
3. Results
3.1. Sample Characteristics
3.2. Neighbourhood Environments
3.3. Multilevel Analysis
3.3.1. Physical Activity Models
3.3.2. Overweight/Obesity Models
4. Discussion
5. Conclusions
Supplementary Material
ijerph-08-03953-s001.pdfAcknowledgements
- Conflict of InterestsAll of the authors declare no competing interests.
- Authors’ ContributionsSAP conceived the study, carried out the design, performed the analyses, and drafted and edited the manuscript. EAK is a principal investigator with the ONS and was responsible for the environmental data; she participated in this study’s design and coordination, provided analytical input and helped draft and edit the manuscript. KR participated in the study’s design, abstraction of data from the RRFSS, provided analytical input and aided with the editing of the manuscript. J-MB provided analytical advice and interpretation and helped edit the manuscript. MS is a principal investigator with the ONS and was responsible for the environmental data, specifically the GIS components; he also participated in the design of the study, provided methodological input, and assisted in the editing of the manuscript. AA participated in the study’s design and coordination of data acquisition and edited the manuscript. MST and DP participated in the design of the study, provided methodological input, and assisted in the editing of the manuscript. All authors read and approved the final manuscript.
References and Notes
- Warburton, DER; Charlesworth, S; Ivey, A; Nettlefold, L; Bredin, SSD. A systematic review of the evidence for Canada’s Physical Activity Guidelines for Adults. Int. J. Behav. Nutr. Phys. Act 2010, 7, 39. [Google Scholar]
- Statistics Canada. Physical Activity During Leisure Time, 2009. Catalogue no. 82-625-X2010002; Minister of Industry: Ottawa, ON, Canada, 2010. Available online: http://www.statcan.gc.ca/pub/82-625-x/2010002/article/11267-eng.htm accessed on 4 July 2011.
- Statistics Canada. Overweight and Obese Adults (Self-Reported), 2009. Catalogue no. 82-625-X2010002; Minister of Industry: Ottawa, ON, Canada, 2010. Available online: http://www.statcan.gc.ca/pub/82-625-x/2010002/article/11255-eng.htm accessed on 4 July 2011.
- Trost, SG; Owen, N; Bauman, AE; Sallis, JF; Brown, W. Correlates of adults' participation in physical activity: review and update. Med. Sci. Sport. Exer 2002, 34, 1996–2001. [Google Scholar]
- Katzmarzyk, PT. The Canadian obesity epidemic, 1985–1998. CMAJ 2002, 166, 1039–1040. [Google Scholar]
- Hill, JO; Peters, JC. Environmental contributions to the obesity epidemic. Science 1998, 280, 1371–1374. [Google Scholar]
- McCormack, G; Giles-Corti, B; Lange, A; Smith, T; Martin, K; Pikora, TJ. An update of recent evidence of the relationship between objective and self-report measures of the physical environment and physical activity behaviours. J. Sci. Med. Sport 2004, 7, 81–92. [Google Scholar]
- Raine, K; Spence, JC; Church, J; Boulé, N; Slater, L; Marko, J; Gibbons, K; Hemphill, E. State of the evidence review on urban health and healthy weights; Canadian Institute of Health Information: Ottawa, ON, Canada, 2008. [Google Scholar]
- Saelens, BE; Handy, SL. Built environment correlates of walking: a review. Med. Sci. Sports Exerc 2008, 40, S550–S566. [Google Scholar]
- Feng, J; Glass, TA; Curriero, FC; Stewart, WF; Schwartz, BS. The built environment and obesity: A systematic review of the epidemiologic evidence. Health Place 2010, 16, 175–190. [Google Scholar]
- McNeill, LH; Kreuter, MW; Subramanian, SV. Social environment and physical activity: A review of concepts and evidence. Soc. Sci. Med 2006, 63, 1011–1022. [Google Scholar]
- Abercrombie, LC; Sallis, JF; Conway, TL; Frank, LD; Saelens, BE; Chapman, JE. Income and racial disparities in access to public parks and private recreation facilities. Am. J. Prev. Med 2008, 34, 9–15. [Google Scholar]
- Estabrooks, PA; Lee, RE; Gyurcsik, NC. Resources for physical activity participation: Does availability and accessibility differ by neighborhood socioeconomic status? Ann. Behav. Med 2003, 25, 100–104. [Google Scholar]
- Moore, LV; Diez Roux, AV; Evenson, KR; McGinn, AP; Brines, SJ. Availability of recreational resources in minority and low socioeconomic status areas. Am. J. Prev. Med 2008, 34, 16–22. [Google Scholar]
- Giles-Corti, B; Donovan, RJ. The relative influence of individual, social and physical environment determinants of physical activity. Soc. Sci. Med 2002, 54, 1793–1812. [Google Scholar]
- Riva, M; Gauvin, L; Richard, L. Use of local area facilities for involvement in physical activity in Canada: Insights for developing environmental and policy interventions. Health Promot. Int 2007, 22, 227–235. [Google Scholar]
- Regidor, E; Gutierrez-Fisac, JL; Ronda, E; Calle, ME; Martinez, D; Dominguez, V. Impact of cumulative area-based adverse socioeconomic environment on body mass index and overweight. J. Epidemiol. Commun. Health 2008, 62, 231–238. [Google Scholar] [Green Version]
- Ross, NA; Crouse, D; Tremblay, S; Khan, S; Tremblay, M; Berthelot, JM. Body mass index in urban Canada: neighborhood and metropolitan area effects. Am. J. Public Health 2007, 97, 500–508. [Google Scholar]
- Ball, K; Cleland, VJ; Timperio, AF; Salmon, J; Giles-Corti, B; Crawford, DA. Love thy neighbour? Associations of social capital and crime with physical activity amongst women. Soc. Sci. Med 2010, 71, 807–814. [Google Scholar]
- Fisher, KJ; Li, FZ. Neighborhood walking and health status in older adults: A multilevel path analysis. J. Aging Phys. Act 2004, 12, 273–273. [Google Scholar]
- Lindstrom, M; Hanson, BS; Ostergren, P-O. Socioeconomic differences in leisure-time physical activity: the role of social participation and social capital in shaping health related behaviour. Soc. Sci. Med 2001, 52, 441–451. [Google Scholar]
- McGinn, AP; Evenson, KR; Herring, AH; Huston, SL; Rodriguez, DA. The association of perceived and objectively measured crime with physical activity: a cross-sectional analysis. J. Phys. Act. Health 2008, 5, 117–131. [Google Scholar]
- Humpel, N; Owen, N; Leslie, E. Environmental factors associated with adults' participation in physical activity: A review. Am. J. Prev. Med 2002, 22, 188–199. [Google Scholar]
- Sallis, JF; Kerr, J. Physical activity and the built environment. Res. Dig 2006, 7, 1–8. [Google Scholar]
- Wendel-Vos, W; Droomers, M; Kremers, S; Brug, J; van Lenthe, F. Potential environmental determinants of physical activity in adults: a systematic review. Obes. Rev 2007, 8, 425–440. [Google Scholar]
- Parenteau, M-P; Sawada, M; Kristjansson, EA; Calhoun, M; Leclair, S; Labonté, R; Runnels, V; Musiol, A; Herold, S. Development of neighborhoods to measure spatial indicators of health. URISA J 2008, 20, 43–55. [Google Scholar]
- Statistics Canada. North American Industry Classification System (NAICS) - Canada. Catalogue no. 12-501-XIE; Statistics Canada: Ottawa, Ontario, Canada, 2007. Available online: http://www.statcan.gc.ca/bsolc/olc-cel/olc-cel?catno=12-501-X&CHROPG=1&lang=eng accessed on 4 July 2011.
- Sawada, M; Kristjansson, EA. Measuring socioeconomic and health inequality in Ottawa, Canada: The methods and measures of the Ottawa Neighbourhood Study. To be submitted for publication.
- Statistics Canada. Low Income Cut-Offs. Catalogue no. 13-551-XIB; Statistics Canada: Ottawa, Ontario, Canada, 1999. Available online: http://www.statcan.gc.ca/bsolc/olc-cel/olc-cel?catno=13-551-X&lang=eng accessed on 4 July 2011.
- Kawachi, I; Kennedy, BP; Glass, R. Social capital and self-rated health: a contextual analysis. Am. J. Publ. Health 1999, 89, 1187–1193. [Google Scholar]
- Macinko, J; Starfield, B. The utility of social capital in research on health determinants. Milbank Q 2001, 79, 387–427. [Google Scholar]
- Statistics Canada. Questionnaire(s) and Reporting Guide(s) - Canadian Community Health Survey (CCHS); Ottawa, Ontario, Canada: Statistics Canada, 2011. Available online: http://www.statcan.gc.ca/cgi-bin/imdb/p2SV.pl?Function=getInstrumentLink&SurvItem_Id=1630&Query_Id=22642&Query=instance&lang=en&db=imdb&adm=8&dis=2 accessed on 4 July 2011.
- Statistics Canada. Uniform Crime Reporting Survey (2.2); Canadian Centre for Justics Statistics (CCJS): Ottawa, Ontario, Canada, 2009. Available online: http://www.statcan.gc.ca/cgi-bin/imdb/p2SV.pl?Function=getSurvey&SDDS=3302&lang=en&db=imdb&adm=8&dis=2 accessed on 4 July 2011.
- Craig, CL; Marshall, AL; Sjostrom, M; Bauman, AE; Booth, ML; Ainsworth, BE; Pratt, M; Yngve, A; Sallis, JF; Oja, P. International Physical Activity Questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc 2003, 35, 1381–1395. [Google Scholar]
- IPAQ Research Committee. Guidelines for Data Processing and Analysis of the International Physical Activity Questionnaire (IPAQ); IPAQ Research Committee, November 2005. Available online: http://www.ipaq.ki.se/scoring.pdf accessed on 4 July 2011.
- Health Canada. Canadian Guidelines for Body Weight Classification in Adults. Catalogue no. H49-179/2003E; Health Canada: Ottawa, ON, Canada, 2003. Available online: http://www.hc-sc.gc.ca/fn-an/nutrition/weights-poids/guide-ld-adult/index-eng.php accessed on 4 July 2011.
- Browne, W; Goldstein, H. An Introduction to Bayesian Multilevel Hierarchical Modelling using MLwiN; Centre for Multilevel Modelling: London England, 2002. Available online: http://0-seis-bris-ac-uk.brum.beds.ac.uk/~frwjb/materials/brussels.pdf accessed on 4 July 2011.
- Merlo, J; Chaix, B; Yang, M; Lynch, J; Rastam, L. A brief conceptual tutorial of multilevel analysis in social epidemiology: linking the statistical concept of clustering to the idea of contextual phenomenon. J. Epidemiol. Commun. Health 2005, 59, 443–449. [Google Scholar]
- Gauvin, L; Riva, M; Barnett, T; Richard, L; Craig, CL; Spivock, M; Laforest, S; Laberge, S; Fournel, M-C; Gagnon, H; et al. Association between neighborhood active living potential and walking. Am. J. Epidemiol 2008, 167, 944–953. [Google Scholar]
- Lebel, A; Pampalon, R; Hamel, D; Theriault, M. The geography of overweight in Quebec: A multilevel perspective. Can. J. Publ. Health 2009, 100, 18–23. [Google Scholar]
- Harrington, DW; Elliott, SJ. Weighing the importance of neighbourhood: A multilevel exploration of the determinants of overweight and obesity. Soc. Sci. Med 2009, 68, 593–600. [Google Scholar]
- Maas, J; Verheij, RA; Spreeuwenberg, P; Groenewegen, PP. Physical activity as a possible mechanism behind the relationship between green space and health: A multilevel analysis. BMC Publ. Health 2008, 8, 206. [Google Scholar]
- Cohen, DA; McKenzie, TL; Sehgal, A; Williamson, S; Golinelli, D; Lurie, N. Contribution of public parks to physical activity. Am. J. Publ. Health 2007, 97, 509–514. [Google Scholar]
- Kaczynski, A; Potwarka, L; Smale, B; Havitz, M. Association of parkland proximity with neighborhood and park-based physical activity: Variations by gender and age. Leisure Sci 2009, 31, 174–191. [Google Scholar]
- Kaczynski, A; Henderson, K. Parks and recreation settings and active living: A review of associations with physical activity function and intensity. J. Phys. Act. Health 2008, 5, 619–632. [Google Scholar]
- Holsten, JE. Obesity and the community food environment: A systematic review. Public Health Nutr 2009, 12, 397–405. [Google Scholar]
- Black, JL; Macinko, J; Dixon, LB; Fryer, J. Neighborhoods and obesity in New York City. Health Place 2010, 16, 489–499. [Google Scholar]
- Morland, K; Diez Roux, A; Wing, S. Supermarkets, other food stores, and obesity: the atherosclerosis risk in communities study. Am. J. Prev. Med 2006, 30, 333–339. [Google Scholar]
- Bodor, JN; Rice, JC; Farley, TA; Swalm, CM; Rose, D. The association between obesity and urban food environments. J. Urb. Health 2010, 87, 771–781. [Google Scholar]
- Jilcott, SB; McGuirt, JT; Imai, S; Evenson, KR. Measuring the retail food environment in rural and urban North Carolina counties. J. Publ. Health Manage. Pract 2010, 16, 432–440. [Google Scholar]
- Spence, JC; Cutumisu, N; Edwards, J; Raine, KD; Smoyer-Tomic, K. Relation between local food environments and obesity among adults. BMC Publ. Health 2009, 9, 192. [Google Scholar]
- McLaren, L. Socioeconomic status and obesity. Epidemiol. Rev 2007, 29, 29–48. [Google Scholar]
- Ball, K; Crawford, D. Socioeconomic status and weight change in adults: A review. Soc. Sci. Med 2005, 60, 1987–2010. [Google Scholar]
- Stafford, M; Cummins, S; MacIntyre, S; Ellaway, A; Marmot, M. Gender differences in the associations between health and neighbourhood environment. Soc. Sci. Med 2005, 60, 1681–1692. [Google Scholar]
- Berry, TR; Spence, JC; Blanchard, CM; Cutumisu, N; Edwards, J; Selfridge, G. A longitudinal and cross-sectional examination of the relationship between reasons for choosing a neighbourhood, physical activity and body mass index. Int. J. Behav. Nutr. Phys. Act 2010, 7, 57. [Google Scholar]
- Lachapelle, U; Frank, L; Saelens, BE; Sallis, JF; Conway, TL. Commuting by Public Transit and Physical Activity: Where You Live, Where You Work, and How You Get There. J. Phys. Act. Health 2011, 8, S72–S82. [Google Scholar]
- Hoehner, CM. Perceived and objective environmental measures and physical activity among urban adults. Am J Prev Med 2005, 2(Suppl 2), 105–116. [Google Scholar]
- Fisher, KJ; Li, F; Michael, Y; Cleveland, M. Neighborhood-level influences on physical activity among older adults: a multilevel analysis. J. Aging Phys. Act 2004, 12, 45–63. [Google Scholar]
- Cohen, DA; Finch, BK; Bower, A; Sastry, N. Collective efficacy and obesity: The potential influence of social factors on health. Soc. Sci. Med 2006, 62, 769–778. [Google Scholar]
- Wilson, DK; Kirtland, KA; Ainsworth, BE; Addy, CL. Socioeconomic status and perceptions of access and safety for physical activity. Ann. Behav. Med 2004, 28, 20–28. [Google Scholar]
- Powell, LM; Bao, Y. Food prices, access to food outlets and child weight. Econ. Hum. Biol 2009, 7, 64–72. [Google Scholar]
- Prince, SA; Adamo, KB; Hamel, ME; Hardt, J; Gorber, SC; Tremblay, M. A comparison of direct versus self-report measures for assessing physical activity in adults: a systematic review. Int. J. Behav. Nutr. Phys. Act 2008, 5, 56. [Google Scholar]


{kind=link}
| Total (n = 3,514) | Men (n = 1,632) | Women (n = 1,882) | |
|---|---|---|---|
| Age category, n (%) | |||
| 18–24 years | 401 (11%) | 177 (11%) | 224 (12%) |
| 25–44 years | 1,490 (42%) | 700 (43%) | 790 (42%) |
| 45–64 years | 1,456 (41%) | 664 (41%) | 791 (42%) |
| 65+ years | 167 (5%) | 91 (5%) | 77 (4%) |
| Body mass index category, n (%) | |||
| Underweight/Normal weight | 1,688 (48%) | 556 (34%) * | 1,132 (60%) * |
| Overweight/Obese | 1,826 (52%) | 1,076 (66%) * | 750 (40%) * |
| Level of physical activity, n (%) | |||
| Insufficiently active | 1,706 (49%) | 755 (46%) ** | 951 (51%) ** |
| Active | 1,808 (51%) | 877 (54%) ** | 931 (49%) ** |
| Education, n (%) | |||
| Did not graduate from high school | 191 (5%) | 106 (6%) ** | 85 (5%) ** |
| Graduated from high school | 528 (15%) | 243 (15%) | 285 (15%) |
| Some post-high school education | 409 (12%) | 195 (12%) | 214 (11%) |
| College/university diploma/degree | 2,386 (68%) | 1,088 (67%) | 1,298 (69%) |
| Household income, n (%) | |||
| ≤ $29,999 | 393 (11%) | 140 (9%) * | 252 (13%) * |
| ≥ $30,000 | 3,121 (89%) | 1,492 (91%) * | 1,630 (87%) * |
| Smoking status, n (%) | |||
| Daily | 474 (14%) | 237 (15%) | 237 (13%) |
| Occasional | 156 (4%) | 84 (5%) | 72 (4%) |
| Former | 1,022 (29%) | 494 (30%) | 529 (28%) |
| Never | 1,862 (53%) | 817 (50%) | 1044 (55%) |
| Season of data collection, n (%) | |||
| Summer | 907 (26%) | 438 (27%) ** | 469 (25%) ** |
| Fall | 886 (25%) | 388 (24%) ** | 498 (26%) ** |
| Winter | 794 (23%) | 399 (24%) ** | 395 (21%) ** |
| Spring | 927 (26%) | 407 (25%) ** | 520 (28%) ** |
| Mean ± SD | Range (min–max) | |
|---|---|---|
| Recreation environment | ||
| Indoor recreation facilities per 1,000 people | 0.17 ± 0.16 | 0–0.64 |
| Outdoor–Winter per 1,000 people | 0.29 ± 0.17 | 0–1.10 |
| Outdoor–Summer per 1,000 people | 3.93 ± 2.01 | 0–13.98 |
| Park area (km2) per 1,000 people | 39.75 ± 44.95 | 2.09–329.42 |
| Bike/walking path length (km) | 11.54 ± 16.24 | 0–140.83 |
| Green space (km2) per 1,000 people | 0.63 ± 3.48 | 0.01–32.09 |
| Food environment | ||
| Grocery stores per 1,000 people | 0.12 ± 0.15 | 0–0.87 |
| Fast food outlets per 1,000 people | 1.24 ± 2.20 | 0–17.93 |
| Convenience stores per 1,000 people | 0.53 ± 0.40 | 0–1.99 |
| Restaurants per 1,000 people | 0.97 ± 1.79 | 0–14.76 |
| Specialty food stores per 1,000 people | 0.38 ± 0.60 | 0–4.03 |
| Social environment | ||
| Socioeconomic index (t-score)* | 41.75, 48.69, 57.73 | 36.00–77.69 |
| Strong sense of belonging (%)* | 56.00, 60.90, 63.70 | 36.70–77.90 |
| Councillor voting rates (%) | 46.70 ± 8.25 | 32.06–100.00 |
| Founded offences of property and violent crime (counts in 2006) | 455.01 ± 440.48 | 72.00–3019.00 |
| Null/empty model | Built environment | Social environment | Built and social environment | Built, social and individual model | Full model with season | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Males | Females | Males OR 95% CI | Females OR 95% CI | Males OR 95% CI | Females OR 95% CI | Males OR 95% CI | Females OR 95% CI | Males OR 95% CI | Females OR 95% CI | Males OR 95% CI | Females OR 95% CI | |
| Built Environment | ||||||||||||
| Number of indoor recreation facilities per 1000 people | 0.65 (0.31, 1.38) | 0.89 (0.91, 1.04) | 0.57 (0.28, 1.14) | 0.91 (0.53, 1.56) | 0.62 (0.28, 1.34) | 0.93 (0.55, 1.58) | 0.60 (0.27, 1.30) | 0.92 (0.54, 1.57) | ||||
| Number of summer outdoor facilities per 1000 people | 1.05 (0.97, 1.14) | 1.04 (0.96, 1.13) | 1.04 (0.95, 1.13) | 1.04 (0.95, 1.14) | 1.05 (0.95, 1.15) | 1.04 (0.95, 1.14) | 1.05 (0.96, 1.15) | 1.04 (0.96, 1.14) | ||||
| Number of winter outdoor facilities per 1000 people | 1.04 (0.40, 2.71) | 1.06 (0.49, 2.31) | 1.00 (0.38, 2.61) | 1.10 (0.50, 2.42) | 1.05 (0.41, 2.69) | 1.11 (0.51, 2.41) | 0.85 (0.35, 2.07) | 1.10 (0.50, 2.44) | ||||
| Park area (km2) per 1000 | 1.00 (0.99, 1.00) | 1.00 (1.00, 1.00) | 1.00 (0.99, 1.00) | 1.00 (1.00, 1.00) | 1.00 (0.99, 1.00) | 1.00 (1.00, 1.00) | 1.00 (0.99, 1.00) | 1.00 (1.00, 1.00) | ||||
| Green space area (km2) per 1000 people | 0.90 (0.84, 0.96) | 0.98 (0.91, 1.04) | 0.92 (0.86, 0.98) | 0.98 (0.95, 1.14) | 0.93 (0.87, 0.99) | 0.97 (0.91, 1.03) | 0.93 (0.87, 0.99) | 0.97 (0.91, 1.03) | ||||
| Bike and walking path length (km) (total) | 1.01 (0.99, 1.02) | 1.00 (0.99, 1.02) | 1.00 (0.99, 1.02) | 1.00 (0.99, 1.02) | 1.00 (0.99, 1.02) | 1.01 (0.99, 1.02) | 1.00 (0.99, 1.02) | 1.01 (0.99, 1.02) | ||||
| Number of grocery stores per 1000 people | 0.46 (0.19, 1.15) | 1.29 (0.49, 3.37) | 0.44 (0.18, 1.03) | 1.21 (0.41, 3.55) | 0.49 (0.19, 1.27) | 1.20 (0.41, 3.53) | 0.54 (0.21, 1.39) | 1.21 (0.41, 3.57) | ||||
| Number of convenience stores per 1000 people | 1.51 (1.14, 2.00) | 1.18 (0.87, 1.61) | 1.95 (1.39, 2.74) | 1.19 (0.79, 1.78) | 2.08 (1.46, 2.96) | 1.19 (0.79, 1.81) | 2.09 (1.46, 2.99) | 1.19 (0.79, 1.81) | ||||
| Number of fast food outlets per 1000 people | 0.96 (0.86, 1.08) | 0.93 (0.83, 1.05) | 0.97 (0.86, 1.09) | 0.93 (0.83, 1.05) | 0.98 (0.86, 1.11) | 0.92 (0.81, 1.04) | 0.97 (0.85, 1.10) | 0.91 (0.81, 1.04) | ||||
| Number of restaurants per 1000 people | 1.03 (0.85, 1.27) | 1.25 (1.03, 1.52) | 0.98 (0.80, 1.19) | 1.25 (1.03, 1.51) | 0.95 (0.77, 1.18) | 1.28 (1.04, 1.56) | 0.97 (0.79, 1.20) | 1.28 (1.04, 1.56) | ||||
| Number of specialty stores per 1000 people | 0.91 (0.59, 1.41) | 0.66 (0.43, 1.01) | 0.95 (0.63, 1.44) | 0.66 (0.44, 1.00) | 1.03 (0.67, 1.58) | 0.68 (0.45, 1.04) | 0.98 (0.64, 1.48) | 0.69 (0.45, 1.04) | ||||
| Social Environment | ||||||||||||
| t-score SES | 0.99 (0.98, 1.00) | 1.00 (0.98, 1.01) | 0.99 (0.98, 1.00) | 1.00 (0.98, 1.02) | 0.99 (0.97, 1.00) | 1.00 (0.98, 1.02) | 0.99 (0.97, 1.00) | 1.00 (0.99, 1.02) | ||||
| Sense of Belonging | 1.01 (0.99, 1.03) | 1.00 (0.99, 1.02) | 1.02 (1.00, 1.03) | 1.01 (0.99, 1.02) | 1.02 (1.00, 1.03) | 1.01 (0.99, 1.02) | 1.02 (1.00, 1.03) | 1.01 (0.99, 1.02) | ||||
| Councilor voting | 0.99 (0.97, 1.01) | 0.99 (0.98, 1.02) | 1.00 (0.98, 1.01) | 0.99 (0.98, 1.01) | 1.00 (0.98, 1.01) | 0.99 (0.98, 1.01) | 1.00 (0.98, 1.02) | 0.99 (0.98, 1.01) | ||||
| Crime rate | 1.00 (1.00, 1.00) | 1.00 (1.00, 1.00) | 1.00 (1.00, 1.00) | 1.00 (1.00, 1.00) | 1.00 (1.00, 1.00) | 1.00 (1.00, 1.00) | 1.00 (1.00, 1.00) | 1.00 (1.00, 1.00) | ||||
| Individual-level | ||||||||||||
| Age | ||||||||||||
| 18–24 years | 1.00 | 1.00 | 1.00 | 1.00 | ||||||||
| 25–44 years | 0.31 (0.18, 0.54) | 0.61 (0.39, 0.94) | 0.32 (0.19, 0.54) | 0.61 (0.39, 0.95) | ||||||||
| 45–64 years | 0.22 (0.13, 0.39) | 0.64 (0.37, 1.08) | 0.22 (0.13, 0.38) | 0.64 (0.37, 1.09) | ||||||||
| 65+ years | 0.16 (0.08, 0.33) | 0.43 (0.23, 0.80) | 0.15 (0.07, 0.32) | 0.43 (0.23, 0.81) | ||||||||
| Household income | ||||||||||||
| ≤ $29,999 | 1.00 | 1.00 | 1.00 | 1.00 | ||||||||
| ≥ $30,000 | 1.41 (0.91, 2.18) | 1.56 (1.10, 2.23) | 1.39 (0.89, 2.16) | 1.56 (1.10, 2.21) | ||||||||
| Education | ||||||||||||
| did not graduate from high school | 1.00 | 1.00 | 1.00 | 1.00 | ||||||||
| graduated from high school | 1.13 (0.60, 2.13) | 1.21 (0.72, 2.05) | 1.11 (0.58, 2.13) | 1.21 (0.71, 2.05) | ||||||||
| some post-high school education | 1.18 (0.62, 2.25) | 1.27 (0.74, 2.19) | 1.14 (0.58, 2.13) | 1.28 (0.74, 2.20) | ||||||||
| college/university diploma/degree | 1.04 (0.64, 1.70) | 1.02 (0.63, 1.64) | 1.00 (0.60, 1.66) | 1.01 (0.63, 1.63) | ||||||||
| Smoking status | ||||||||||||
| Current smoker | 1.00 | 1.00 | 1.00 | 1.00 | ||||||||
| Daily | 1.04 (0.82, 1.33) | 1.21 (0.95, 1.54) | 1.01 (0.78, 1.29) | 1.21 (0.95, 1.54) | ||||||||
| Occasional | 1.22 (0.66, 2.26) | 1.16 (0.66, 2.05) | 1.26 (0.69, 2.31) | 1.15 (0.65, 2.04) | ||||||||
| Former | 1.03 (0.76, 1.39) | 1.33 (0.91, 1.94) | 1.04 (0.77, 1.40) | 1.33 (0.91, 1.94) | ||||||||
| Contextual (Season) | ||||||||||||
| Summer | 1.00 | 1.00 | ||||||||||
| Fall | 0.71 (0.51, 0.99) | 0.86 (0.67, 1.11) | ||||||||||
| Winter | 0.44 (0.32, 0.60) | 0.82 (0.60, 1.12) | ||||||||||
| Spring | 0.66 (0.49, 0.88) | 0.85 (0.64, 1.12) | ||||||||||
| ICC | 0.01 | 0.01 | 0.01 | 0.01 | 0.00 | 0.01 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 |
| Null/empty model | Built environment | Social environment | Built and social environment | Built, social and individual model | Full model with season | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Males | Females | Males OR 95% CI | Females OR 95% CI | Males OR 95% CI | Females OR 95% CI | Males OR 95% CI | Females OR 95% CI | Males OR 95% CI | Females OR 95% CI | Males OR 95% CI | Females OR 95% CI | |
| Built Environment | ||||||||||||
| Number of indoor recreation facilities per 1000 people | 1.67 (0.74, 3.77) | 1.02 (0.45, 2.30) | 1.65 (0.78, 3.49) | 1.34 (0.60, 2.98) | 1.50 (0.71, 3.19) | 1.28 (0.55, 3.00) | 1.50 (0.71, 3.16) | 1.27 (0.54, 2.97) | ||||
| Number of summer outdoor facilities per 1000 people | 1.02 (0.93, 1.13) | 1.09 (1.03, 1.16) | 0.98 (0.89, 1.08) | 1.09 (1.03, 1.15) | 0.98 (0.89, 1.07) | 1.08 (1.03, 1.10) | 0.98 (0.90, 1.08) | 1.08 (1.02, 1.14) | ||||
| Number of winter outdoor recreation facilities per 1000 people | 0.71 (0.22, 2.24) | 1.08 (0.54, 2.19) | 1.06 (0.38, 2.99) | 1.09 (0.57, 2.10) | 0.89 (0.30, 2.69) | 1.00 (0.52, 1.90) | 0.88 (0.29, 2.63) | 1.06 (0.53, 2.10) | ||||
| Park area (km2) per 1000 | 1.00 (1.00, 1.01) | 0.99 (0.99, 0.99) | 1.00 (1.00, 1.01) | 0.99 (0.99, 0.99) | 1.00 (1.00, 1.01) | 1.00 (1.00, 1.00) | 1.00 (1.00, 1.01) | 1.00 (0.99, 1.00) | ||||
| Green space area (km2) per 1000 people | 1.09 (0.98, 1.22) | 0.73 (0.63, 0.85) | 1.12 (1.03, 1.23) | 0.65 (0.53, 0.80) | 1.10 (1.01, 1.21) | 0.67 (0.50, 0.80) | 1.10 (1.00, 1.20) | 0.67 (0.54, 0.84) | ||||
| Bike and walking path length (km) (total) | 1.00 (0.98, 1.02) | 1.01 (1.00, 1.02) | 0.99 (0.98, 1.01) | 1.01 (1.00, 1.02) | 1.00 (0.98, 1.01) | 1.01 (0.99, 1.00) | 1.00 (0.98, 1.01) | 1.01 (0.99, 1.02) | ||||
| Number of grocery stores per 1000 people | 1.84 (0.68, 5.01) | 1.17 (0.51, 2.57) | 1.87 (0.68, 5.17) | 1.30 (0.55, 3.30) | 1.40 (0.51, 3.86) | 1.21 (0.50, 2.90) | 1.40 (0.50, 3.90) | 1.21 (0.49, 2.98) | ||||
| Number of convenience stores per 1000 people | 0.91 (0.66, 1.26) | 1.19 (0.84, 1.69) | 1.28 (0.84, 1.94) | 0.90 (0.57, 1.50) | 1.32 (0.90, 1.93) | 0.97 (0.60, 1.60) | 1.31 (0.89, 1.91) | 0.96 (0.60, 1.56) | ||||
| Number of fast food outlets per 1000 people | 1.03 (0.92, 1.16) | 1.14 (0.97, 1.34) | 1.03 (0.90, 1.23) | 1.10 (0.96, 1.40) | 1.06 (0.91, 1.23) | 1.14 (0.96, 1.30) | 1.05 (0.90, 1.23) | 1.14 (0.96, 1.35) | ||||
| Number of restaurants per 1000 people | 0.82 (0.67, 1.00) | 0.78 (0.60, 0.99) | 0.72 (0.56, 0.91) | 0.80 (0.63, 1.00) | 0.71 (0.56, 0.91) | 0.78 (0.62, 0.99) | 0.71 (0.56, 0.90) | 0.78 (0.61, 0.99) | ||||
| Number of specialty stores per 1000 people | 1.15 (0.82, 1.61) | 1.65 (1.06, 2.57) | 1.39 (0.95, 2.03) | 1.71 (1.11, 2.60) | 1.32 (0.85, 2.04) | 1.78 (1.15, 2.80) | 1.33 (0.86, 2.07) | 1.79 (1.16, 2.78) | ||||
| Social Environment | ||||||||||||
| t-score SES | 0.98 (0.97, 1.00) | 1.01 (0.99, 1.02) | 0.97 (0.96, 0.99) | 1.00 (0.98, 1.00) | 0.98 (0.96, 0.99) | 1.00 (1.00, 1.00) | 0.98 (0.96, 0.99) | 0.99 (0.98, 1.01) | ||||
| Sense of Belonging | 1.01 (1.00, 1.03) | 1.00 (0.98, 1.02) | 1.02 (1.00, 1.03) | 1.00 (0.96, 1.00) | 1.02 (1.00, 1.04) | 0.98 (0.99, 1.00) | 1.02 (1.00, 1.04) | 0.98 (0.96, 1.00) | ||||
| Councilor voting | 0.98 (0.96, 0.99) | 0.99 (0.98, 1.00) | 0.97 (0.96, 0.99) | 1.00 (0.97, 1.00) | 0.98 (0.96, 0.99) | 0.99 (0.99, 1.00) | 0.97 (0.96, 0.99) | 0.99 (0.97, 1.00) | ||||
| Crime rate | 1.00 (1.00, 1.00) | 1.00 (1.00,1.00) | 1.00 (1.00, 1.00) | 1.00 (1.00, 1.00) | 1.00 (1.00, 1.00) | 1.00 (1.00, 1.00) | 1.00 (1.00, 1.00) | 1.00 (1.00, 1.00) | ||||
| Individual-level | ||||||||||||
| Age | ||||||||||||
| 18–24 years | 1.00 | 1.00 | 1.00 | 1.00 | ||||||||
| 25–44 years | 2.73 (1.56–4.78) | 2.30 (1.41, 3.80) | 2.80 (1.58, 4.95) | 2.30 (1.40, 3.78) | ||||||||
| 45–64 years | 3.32 (1.87–5.88) | 3.57 (2.24, 5.70) | 3.40 (1.90–6.09) | 3.59 (2.25, 5.73) | ||||||||
| 65+ years | 1.71 (0.87, 3.34) | 4.44 (2.09, 9.40) | 1.74 (0.88, 3.43) | 4.60 (2.18, 9.71) | ||||||||
| Household income | ||||||||||||
| ≤ $29,999 | 1.00 | 1.00 | 1.00 | 1.00 | ||||||||
| ≥ $30,000 | 1.43 (0.86, 2.39) | 0.74 (0.52, 1.10) | 1.45 (0.87, 2.41) | 0.75 (0.52, 1.08) | ||||||||
| Education | ||||||||||||
| did not graduate from high school | 1.00 | 1.00 | 1.00 | 1.00 | ||||||||
| graduated from high school | 1.14 (0.65, 2.00) | 0.74 (0.41, 1.30) | 1.11 (0.62, 1.98) | 0.75 (0.42, 1.34) | ||||||||
| some post-high school education | 0.98 (0.52, 1.84) | 0.84 (0.46, 1.60) | 0.96 (0.51, 1.80) | 0.86 (0.47, 1.57) | ||||||||
| college/university diploma/degree | 0.90 (0.51, 1.59) | 0.53 (0.32, 0.90) | 0.87 (0.49, 1.55) | 0.54 (0.32, 0.90) | ||||||||
| Smoking status | ||||||||||||
| Current smoker | 1.00 | 1.00 | 1.00 | 1.00 | ||||||||
| Daily | 1.90 (1.38, 2.62) | 1.16 (0.93, 1.45) | 1.90 (1.38, 2.62) | 1.14 (0.91, 1.44) | ||||||||
| Occasional | 1.05 (0.64, 1.72) | 1.26 (0.80, 1.99) | 1.06 (0.65, 1.73) | 1.25 (0.80, 1.95) | ||||||||
| Former | 1.18 (0.80, 1.75) | 0.83 (0.55, 1.24) | 1.20 (0.81, 1.77) | 0.82 (0.55, 1.23) | ||||||||
| Contextual (Season) | ||||||||||||
| Summer | 1.00 | 1.00 | ||||||||||
| Fall | 1.28 (0.94, 1.73) | 0.87 (0.66, 1.15) | ||||||||||
| Winter | 0.99 (0.72, 1.38) | 1.11 (0.81, 1.52) | ||||||||||
| Spring | 1.28 (0.93, 1.75) | 0.94 (0.73, 1.21) | ||||||||||
| ICC | 0.05 | 0.02 | 0.04 | 0.02 | 0.02 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 |
© 2011 by the authors; licensee MDPI, Basel, Switzerland This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Prince, S.A.; Kristjansson, E.A.; Russell, K.; Billette, J.-M.; Sawada, M.; Ali, A.; Tremblay, M.S.; Prud’homme, D. A Multilevel Analysis of Neighbourhood Built and Social Environments and Adult Self-Reported Physical Activity and Body Mass Index in Ottawa, Canada. Int. J. Environ. Res. Public Health 2011, 8, 3953-3978. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph8103953
Prince SA, Kristjansson EA, Russell K, Billette J-M, Sawada M, Ali A, Tremblay MS, Prud’homme D. A Multilevel Analysis of Neighbourhood Built and Social Environments and Adult Self-Reported Physical Activity and Body Mass Index in Ottawa, Canada. International Journal of Environmental Research and Public Health. 2011; 8(10):3953-3978. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph8103953
Chicago/Turabian StylePrince, Stephanie A., Elizabeth A. Kristjansson, Katherine Russell, Jean-Michel Billette, Michael Sawada, Amira Ali, Mark S. Tremblay, and Denis Prud’homme. 2011. "A Multilevel Analysis of Neighbourhood Built and Social Environments and Adult Self-Reported Physical Activity and Body Mass Index in Ottawa, Canada" International Journal of Environmental Research and Public Health 8, no. 10: 3953-3978. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph8103953