Assessment of Exposure to Alcohol Vapor from Alcohol-Based Hand Rubs

Abstract
:1. Introduction
2. Materials and Methods
2.1. Alcohol-Based Hand Rubs
2.2. Hand Rubbing Procedures
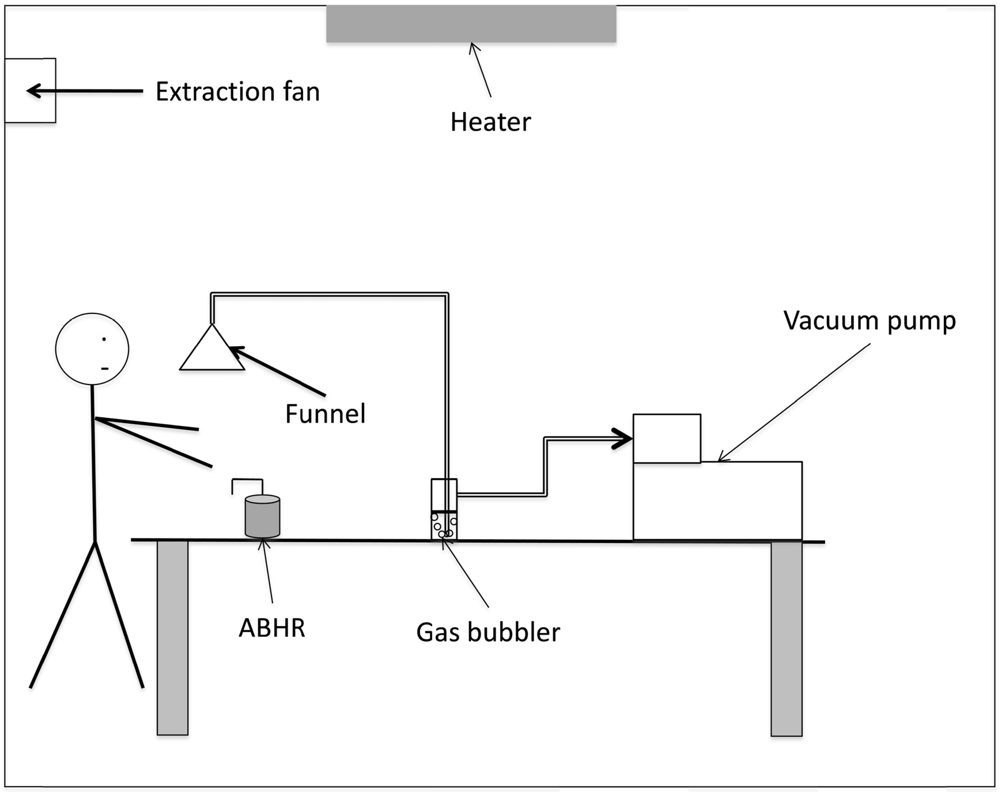
2.3. Experimental Apparatus


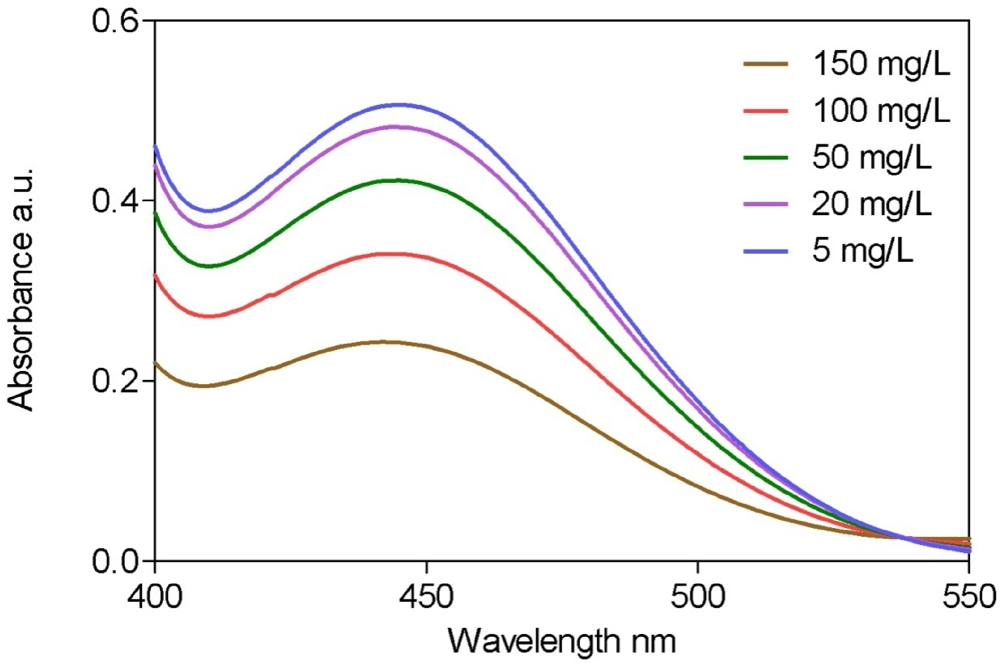
2.4. Analysis of Alcohol


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Value |
|---|---|
| Wavelength range(nm) | 400–550 |
| Wavelength quantification (nm) | 440 |
| Concentration range (mg/L) | 5–150 |
| Determination coefficient R² | 0.998 |
| Sensitivity (mg/L) | 0.4 |
| Limit of detection (mg/L) | 5 |
| Relative standard deviation (%) (n = 5) | 3 |
2.5. Data Analysis
3. Results
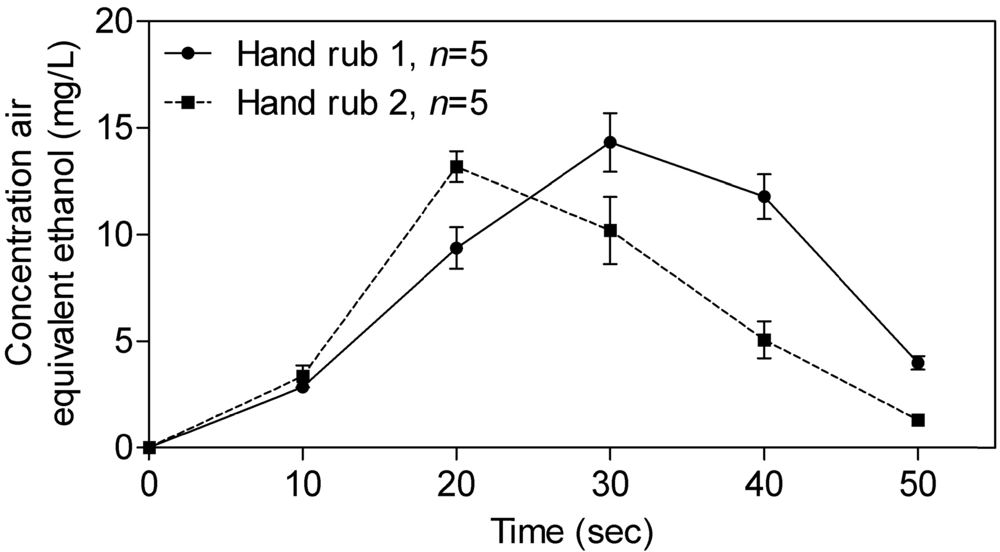
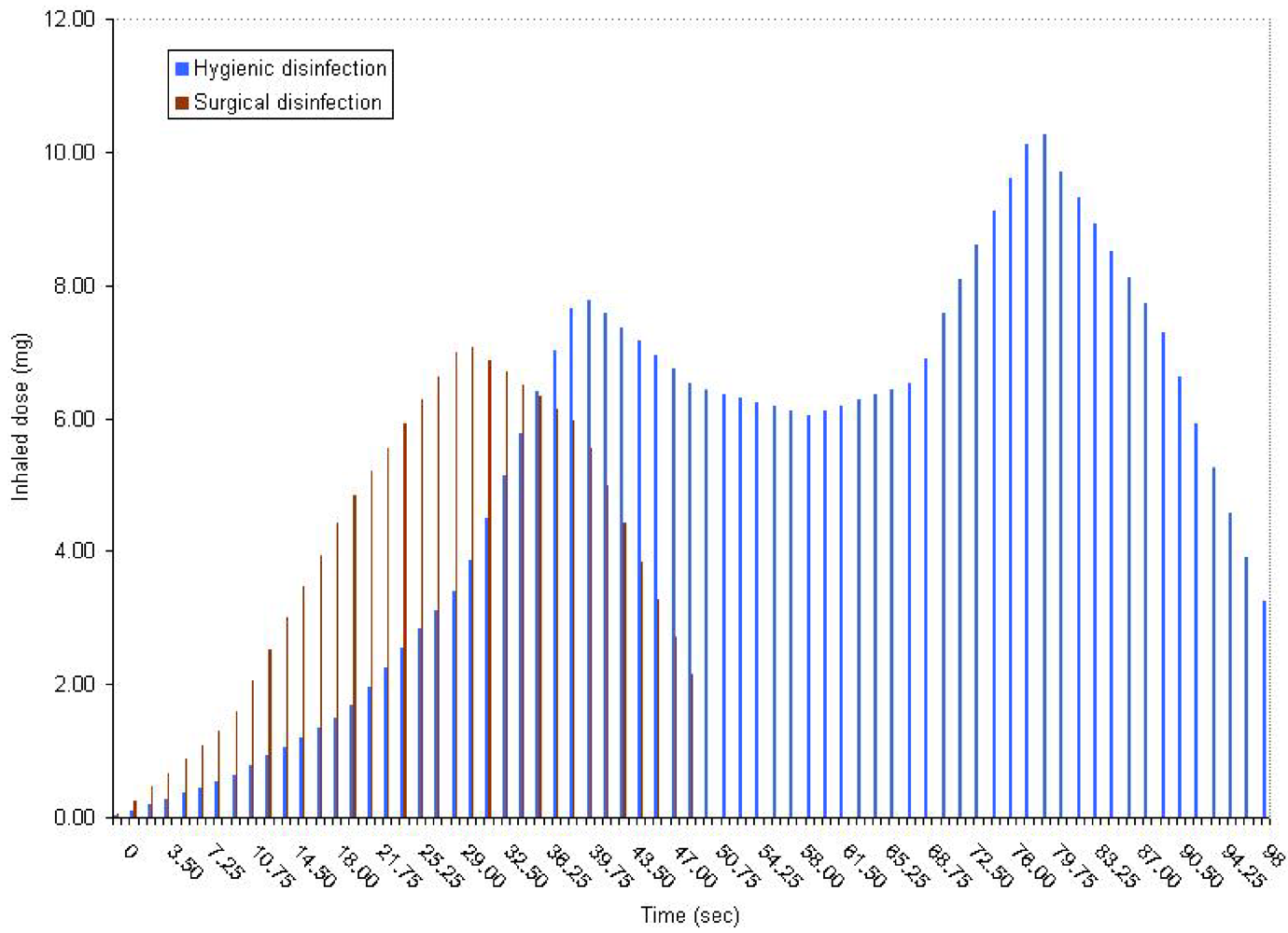
3.1. Hygienic Hand Disinfection

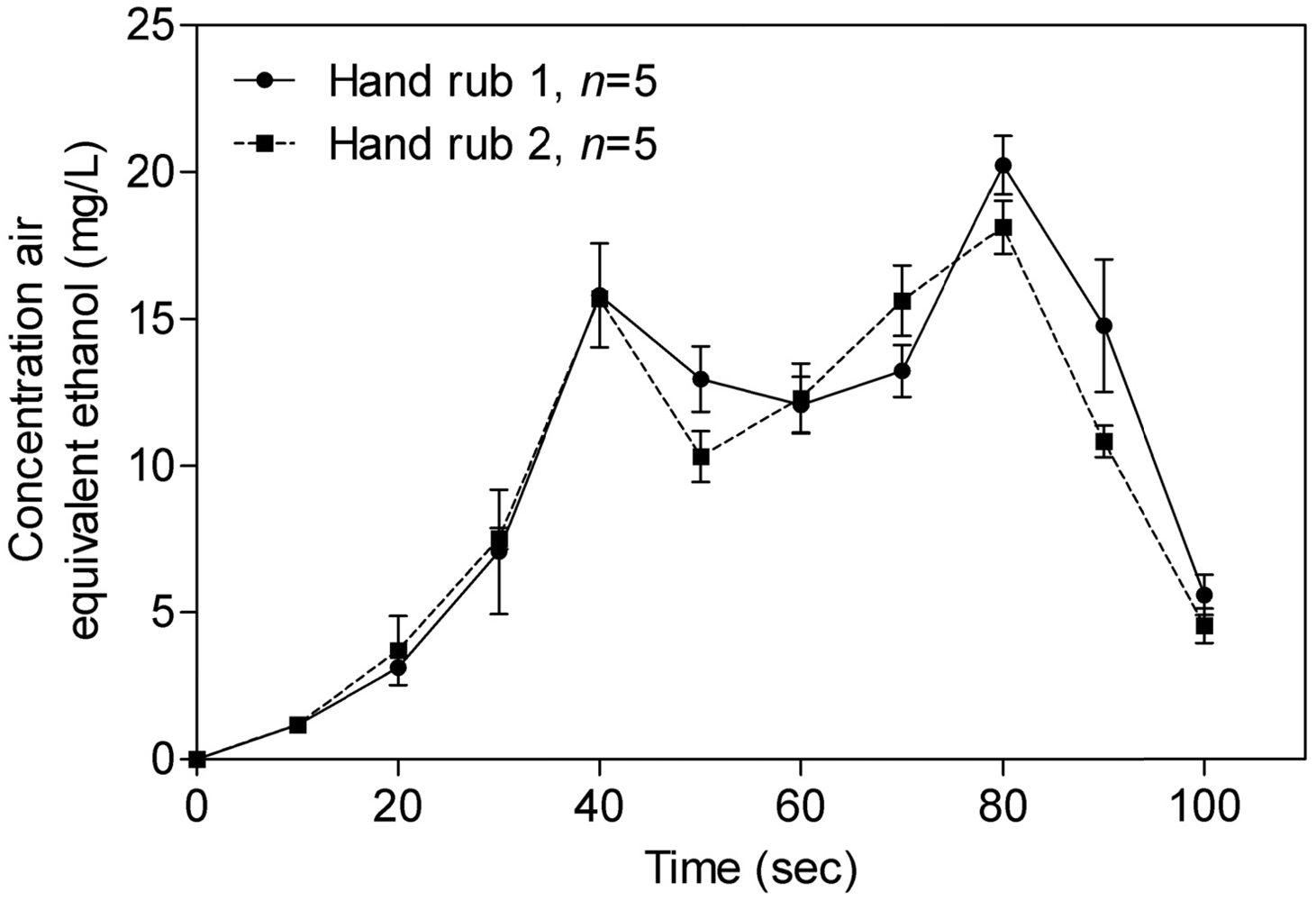
3.2. Surgical Hand Disinfection

3.3. Exposure Assessment



4. Discussion
4.1. Experimental Conditions
4.2. Comparison of Hand Rub 1 and Hand Rub 2
4.3. Risk Assessment
5. Conclusions
Acknowledgments
Conflict of Interest
References
- Boyce, J.M. Using alcohol for hand antisepsis: Dispelling old myths. Infect. Control Hosp. Epidemiol. 2000, 21, 438–441. [Google Scholar]
- Boyce, J.M.; Pittet, D. Guideline for hand hygiene in health-care settings. Am. J. Infect. Control 2002, 30, 1–46. [Google Scholar]
- Bessonneau, V.; Clément, M.; Thomas, O. Can intensive use of alcohol-based hand rubs lead to passive alcoholization? Int. J. Environ. Res. Public Health 2010, 7, 3038–3050. [Google Scholar] [CrossRef]
- Mayer, J.; Mooney, B.; Gundlapalli, A.; Harbarth, S.; Stoddard, G.J.; Rubin, M.A.; Eutropius, L.; Brinton, B.; Samore, M.H. Dissemination and sustainability of a hospital-wide hand hygiene program emphazing positive reinforcement. Infect. Control. Hosp. Epidemiol. 2011, 32, 59–66. [Google Scholar]
- Pittet, D.; Panesar, S.S.; Wilson, K.; Longtin, Y.; Morris, T.; Allan, V.; Storr, J.; Cleary, K.; Donaldson, L. Involving the patient to ask about hospital hand hygiene: A National Patient Safety Agency feasibility study. J. Hosp. Infect. 2011, 77, 299–303. [Google Scholar]
- Wilson, S.; Jacob, C.; Powell, D. Behavior-change interventions to improve hand-hygiene practice: A review of alternatives to education. Crit. Public Health 2011, 21, 119–127. [Google Scholar]
- Erasmus, V.; Daha, T.J.; Brug, H.; Richardus, J.H.; Behrendt, M.D.; Vos, M.C.; van Beeck, E.F. Systematic review of studies on compliance with hand hygiene guidelines in hospital care. Infect. Control Hosp. Epidemiol. 2010, 31, 283–294. [Google Scholar]
- Below, H.; Partecke, I.; Huebner, N.O.; Bieber, N.; Nicolai, T.; Usche, A.; Assadian, O.; Below, E.; Kampf, G.; Parzefall, W.; et al. Dermal and pulmonary absorption of propan-1-ol and propan-2-ol from hand rubs. Am. J. Infect. Control 2011. [Google Scholar] [CrossRef]
- Kramer, A.; Below, H.; Bieber, N.; Kampf, G.; Toma, C.D.; Huebner, N.O.; Assadian, O. Quantity of ethanol absorption after excessive hand disinfection using three commercially available hand rubs is minimal and below toxic levels in humans. BMC Infect. Dis. 2007, 7. [Google Scholar] [CrossRef]
- Miller, M.A.; Rosin, A.; Levsky, M.E.; Patel, M.M.; Gregory, T.J.D.; Crystal, C.S. Does the clinical use of ethanol-based hand sanitizer elevate blood alcohols levels? A prospective study. Am. J. Emerg. Med. 2006, 24, 815–817. [Google Scholar]
- Reisfield, G.M.; Goldberger, B.A.; Crews, B.O.; Pesce, A.J.; Wilson, G.R.; Teitelbaum, S.A.; Bertholf, R.L. Ethyl glucuronide, ethyl sulfate, and ethanol in urine after sustained exposure to an ethanol-based hand sanitizer. J. Anal. Toxicol. 2011, 35, 85–91. [Google Scholar]
- Reisfield, G.M.; Goldberger, B.A.; Crews, B.O.; Pesce, A.J.; Wilson, G.R.; Teitelbaum, S.A.; Bertholf, R.L. Ethyl glucuronide, ethyl sulfate, and ethanol in urine after intensive exposure to high ethanol content mouthwash. J. Anal. Toxicol. 2011, 35, 264–268. [Google Scholar]
- Société Française d’Hygiène Hospitalière. Liste positive désinfectants (in French). Hygiènes 2008, 16, 95–118.
- Thomas, O.; Mazas, N. La mesure de la demande chimique en oxygène dans les milieux faiblement pollués (in French). Analusis 1986, 14, 300–302. [Google Scholar]
- Boatman, R.J.; Perry, L.G.; Fiorica, L.A.; English, J.C.; Kapp, R.W.; Bevan, C.; Tyler, T.R.; Banton, M.I.; Wright, G.A. Dermal absorption and pharmacokinetics of isopropanol in the male and female F-344 rat. Drug Metab. Dispos. 1998, 26, 197–202. [Google Scholar]
- Scheuplein, R.J.; Irvin, H.; Blank, D. Mechanisms of percutaneaous absorption. IV: Penetration of nonelectrolytes (alcohols) from aqueous solutions and from pure liquids. J. Invest. Dermatol. 1973, 60, 286–396. [Google Scholar]
- U.S. Environmental Protection Agency (U.S. EPA), Exposure Factors Handbook; Office of Health and Environmental Assessment: Washington, DC, USA, 1997.
- Bingham, E.; Cohrssen, B.; Powell, C.H. Patty’s Toxicology, 5th ed; John Wiley and Sons: New York, NY, USA, 2001. [Google Scholar]
- Hämmerle, M.; Hilgert, K.; Achmann, S.; Moos, R. Direct monitoring of organic vapours with amperometric enzyme gas sensors. Biosens. Bioelectron. 2010, 25, 1521–1525. [Google Scholar]
- Roukos, J.; Plaisance, H.; Leonardis, T.; Bates, M.; Locoge, N. Development and validation of an automated monitoring system for oxygenated volatile organic compounds and nitrile compounds in ambient air. J. Chromatogr. A. 2009, 1216, 8642–8651. [Google Scholar]
- Rehm, J.; Room, R.; Graham, K.; Monteiro, M.; Gmel, G.; Sempos, C.T. The relationship of average volume of alcohol consumption and patterns of drinking to burden of disease: An overview. Addiction 2003, 98, 1209–1228. [Google Scholar]
- Bevan, R.J.; Slack, R.J.; Holmes, P.; Levy, L.S. An assessment of potential cancer risk following occupational exposure to ethanol. J. Toxicol. Environ. Health B Crit. Rev. 2009, 12, 188–205. [Google Scholar]
- Dutch Expert Committee on Occupational Standards, Ethanol (Ethyl Alcohol): Evaluation of the Health Effects from Occupational Exposure; Health Council of the Netherlands: The Hague, The Netherlands, 2006.
- Irvine, L.F.H. Relevance of the developmental toxicity of ethanol in the occupational setting: A review. J. Appl. Toxicol. 2003, 23, 289–299. [Google Scholar]
- Tardif, R.; Liu, L.; Raizenne, M. Exhaled ethanol and acetaldehyde in human subjects exposed to low levels of ethanol. Inhal. Toxicol. 2004, 16, 203–207. [Google Scholar]
- Gilpin, N.W.; Smith, A.D.; Cole, M.; Weiss, F.; Koob, G.F.; Richardson, H.N. Operant behavior and alcohol levels in blood and brain of alcohol-dependent rats. Alcohol Clin. Exp. Res. 2009, 33, 2113–2123. [Google Scholar]
- O’Dell, L.E.; Roberts, A.J.; Smith, R.T.; Koob, G.F. Enhanced alcohol self-administration after intermittent versus continuous alcohol vapor exposure. Alcohol Clin. Exp. Res. 2004, 28, 1676–1682. [Google Scholar]
© 2012 by the authors; licensee MDPI, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Bessonneau, V.; Thomas, O. Assessment of Exposure to Alcohol Vapor from Alcohol-Based Hand Rubs. Int. J. Environ. Res. Public Health 2012, 9, 868-879. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph9030868
Bessonneau V, Thomas O. Assessment of Exposure to Alcohol Vapor from Alcohol-Based Hand Rubs. International Journal of Environmental Research and Public Health. 2012; 9(3):868-879. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph9030868
Chicago/Turabian StyleBessonneau, Vincent, and Olivier Thomas. 2012. "Assessment of Exposure to Alcohol Vapor from Alcohol-Based Hand Rubs" International Journal of Environmental Research and Public Health 9, no. 3: 868-879. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph9030868