Integrating Susceptibility into Environmental Policy: An Analysis of the National Ambient Air Quality Standard for Lead

Abstract
:1. Introduction
2. Methods
2.1. EPA Analytical Approach
2.1.1. Determining the Lead NAAQS

{kind=link}
{kind=link}
| Potential Level for Standard (µg/m3) | Air-to-Blood Lead Ratio* | ||
|---|---|---|---|
| 1:5 | 1:7 | 1:10 | |
| 0.50 | 4.4 (3.9–7.4) | >5 a | >5 a |
| 0.40 | 3.5 (3.1–5.9) | 4.9 (4.4–8.2) | b |
| 0.30 | 2.6 (2.3–4.4) | 3.7 (3.3–6.2) | 5.3 (4.7–8.8) |
| 0.25 | 2.2 (2.0–3.7) | 3.1 (2.7–5.1) | 4.4 (3.9–7.4) |
| 0.20 | 1.8 (1.6–2.9) | 2.5 (2.2–4.1) | 3.5 (3.1–5.9) |
| 0.15 | 1.3 (1.2–2.2) | 1.8 (1.6–3.1) c | 2.6 (2.3–4.4) |
| 0.10 | 0.9 (0.8–1.5) | 1.2 (1.1–2.1) | 1.8 (1.6–2.9) |
| 0.05 | 0.4 (0.4–0.7) | 0.6 (0.5–1.0) | 0.9 (0.8–1.5) |
| 0.02 | 0.2 (0.2–0.3) | 0.2 (0.2–0.4) | 0.4 (0.3–0.6) |
2.2. Incorporation of Susceptibility
2.2.1. Data Analysis
3. Results
3.1. Description of Data
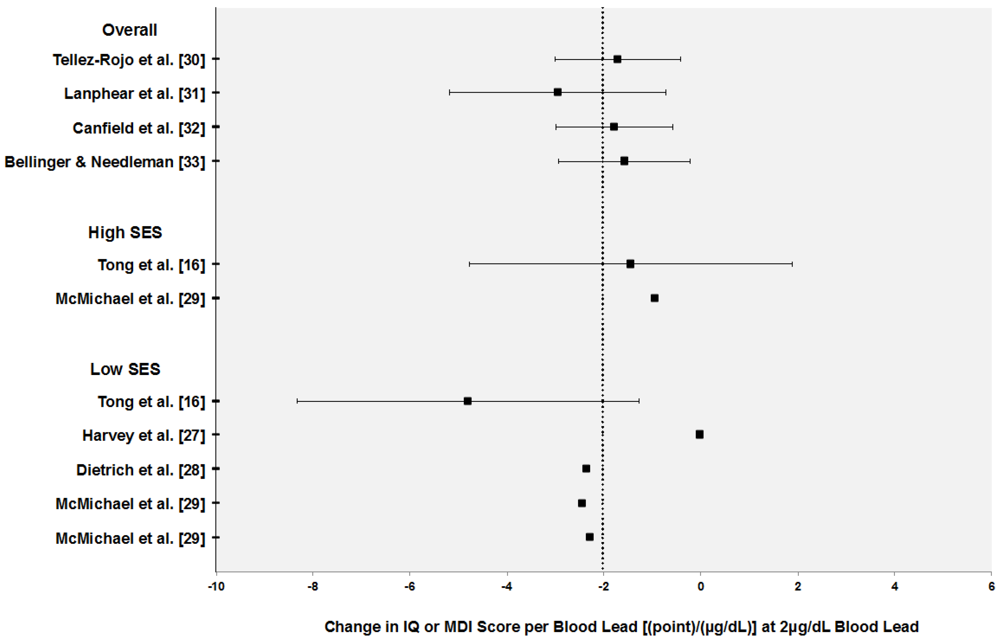
| β (SE or 95th CI if reported) a | Susceptibility | Lead Form | Lead Measure | Overall Lead Mean (µg/dL) | Outcome | Age at Assessment | Reference |
|---|---|---|---|---|---|---|---|
| Studies used by EPA to determine concentration-response function | |||||||
| −1.71 | Overall | Linear | Concurrent | 2.9 (0.8–4.9) b,c | MDI (BSID) | 24 months | Tellez-Rojo et al. [30] |
| −2.94 | Overall | Linear | Concurrent | 3.2 (0.9–7.4) b,c | IQ (WISC-R) | 4–10 years | Lanphear et al. [31] d |
| −1.79 | Overall | Linear | Concurrent | 3.3 (0.5–8.4) b,c | IQ (SBIS) | 5 years | Canfield et al. [32] |
| −1.56 | Overall | Linear | Neonatal | 3.8 (1.0–9.3) b,c | IQ (WISC-R) | 10 years | Bellinger & Needleman [33] |
| Studies with SES-subgroup specific effects included in the analysis | |||||||
| −4.70 | Low SES | Ln | Neonatal | 4.5 (2.9) | MDI (BSID) | 6 months | Dietrich et al. [28] |
| −4.90 e | Low SES | Ln | Average Postnatal | 21.3 | MDI (BSID) | 2 years | McMichael et al. [29] |
| −4.57 e | Middle SES | ||||||
| −1.87 e | High SES | (13.3–33.8) f | |||||
| −9.60 (3.60) | Low SES | Ln | Lifetime Average | 14.1 (1.2) b | IQ (WISC-R) | 11–13 years | Tong et al. [16] |
| −2.90 (3.40) | High SES | ||||||
| −0.03 | Manual | Linear | Concurrent | 15.6 (4.1) | IQ (BAS) | 2–6 years | Harvey et al. [27] |

3.2. Selection of Parameters and Analysis Results
3.2.1. Concentration-Response Functions
| Reference | Susceptibility | CR Function (95% CI) | Median CR (95% CI) | Pooled CR (95% CI) |
|---|---|---|---|---|
| Tellez-Rojo et al. [30] | Overall | −1.71 (−3.00, −0.42) | −1.75 (−3.00, −0.51) | −1.82 (−2.52, −1.12) |
| Lanphear et al. [31] | Overall | −2.94 (−5.16, −0.71) | ||
| Canfield et al. [32] | Overall | −1.79 (−3.00, −0.60) | ||
| Bellinger & Needleman [33] | Overall | −1.56 (−2.90, −0.20) | ||
| McMichael et al. [29] | High SES | −0.94 | -1.19 | NA |
| Tong et al. [16] | High SES | −1.45 (−4.78, 1.88) | ||
| Dietrich et al. [28] | Low SES | −2.35 | −2.40 | NA |
| McMichael et al. [29] | Low SES | −2.45 | ||
| Tong et al. [16] | Low SES | −4.80 (−8.33, −1.27) | ||
| Harvey et al. [27] | Low SES | −0.03 |
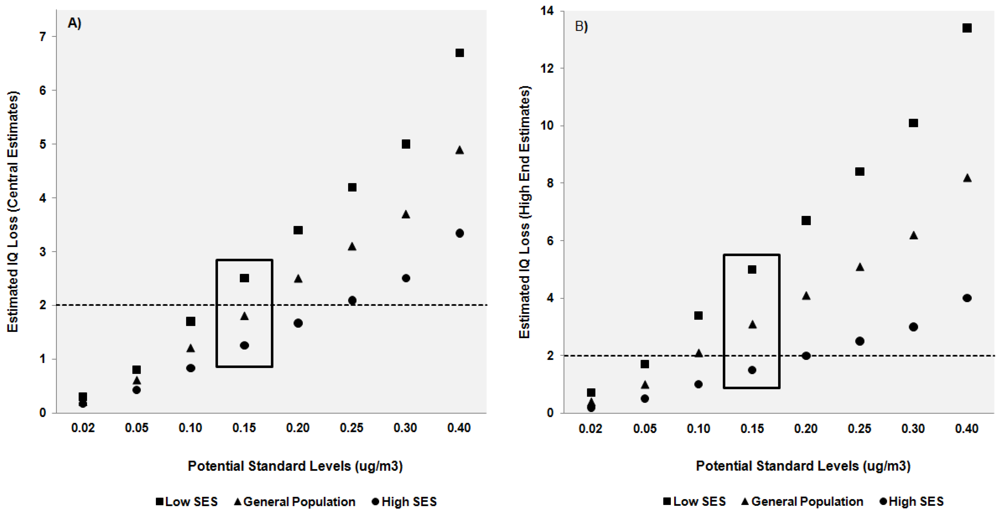
3.2.2. Ratios and Standard Levels
3.3. Analysis Results
| Potential Standard (µg/m3) | Air-to-Blood Lead Ratio | ||
|---|---|---|---|
| 1:5 | 1:7 | 1:10 | |
| 0.02 | 0.2 (0.00, 0.5) | 0.3 (0.00, 0.7) | 0.5 (0.01, 0.1) |
| 0.05 | 0.6 (0.01, 1.2) | 0.8 (0.01, 1.7) | 1.2 (0.02, 2.4) |
| 0.10 | 1.2 (0.02, 2.4) | 1.7 (0.02, 3.4) | 2.4 (0.03, 4.8) |
| 0.15 | 1.8 (0.02, 3.6) | 2.5 (0.03, 5.0) | 3.6 (0.1, 7.2) |
| 0.20 | 2.4 (0.03, 4.8) | 3.4 (0.04, 6.7) | 4.8 (0.1, 9.6) |
| 0.25 | 3.0 (0.04, 6.0) | 4.2 (0.1, 8.4) | 6.0 (0.1, 12.0) |
| 0.30 | 3.6 (0.15, 7.2) | 5.0 (0.1, 10.1) | 7.2 (0.1, 14.4) |
| 0.40 | 4.8 (0.16, 9.6) | 6.7 (0.1, 13.4) | 9.6 (0.1, 19.2) |
| 0.50 | 6.0 (0.1, 12.0) | 8.4 (0.1, 16.8) | 12.0 (0.2, 24.0) |
4. Discussion
4.1. Overview of Results
4.1.1. Analysis Limitations
4.2. Role for Cumulative Risk Assessment in Policy Development
4.2.1. Susceptibility and Decision-making
“…included among those persons whose health should be protected by the ambient standard are particularly sensitive citizens…who in the normal course of daily activity are exposed to the ambient environment…an ambient air quality standard, therefore, should be the maximum permissible ambient air level of an air pollution agent…which will protect the health of any group in the population.” (S. Rep. No. 91-1196, 91st Cong., 2d Sess. 10 (1970)) [43].
4.2.2. Defining Acceptable Risks
“EPA is not determining a specific quantitative public health policy goal in terms of an air-related IQ loss that is acceptable or unacceptable in the U.S. population per se, but instead is determining what magnitude of estimated air-related IQ loss should be used in conjunction with the specific…evidence-based framework being applied in this review, recognizing the uncertainties and limitations in this framework…the estimated air-related IQ loss resulting from the application of this evidence-based framework should not be viewed as a bright line estimate of expected IQ loss in the population that would or would not occur. Nonetheless, these results provide a useful guide…to use in making the basically qualitative public health policy judgment about the risk to public health that could reasonably be expected to result from exposure….” (FR 73 67000) [11].

4.2.3. Prioritizing Decision Elements
4.3. Data Needs for Cumulative Risk Assessment
5. Conclusions
Acknowledgments
Conflict of Interest
References
- Hattis, D.; Banati, P.; Goble, R.; Burmaster, D.E. Human interindividual variability in parameters related to health risks. Risk Anal. 1999, 19, 711–726. [Google Scholar]
- Hattis, D.; Banati, P.; Goble, R. Distributions of individual susceptibility among humans for toxic effects: How much protection does the traditional tenfold factor provide for what fraction of which kinds of chemicals and effects? Ann. NY Acad. Sci. 1999, 895, 286–316. [Google Scholar] [CrossRef]
- Aldridge, J.E.; Gibbons, J.A.; Flaherty, M.M.; Kreider, M.L.; Romano, J.A.; Levin, E.D. Heterogeneity of toxicant response: sources of human variability. Toxicol. Sci. 2003, 76, 3–20. [Google Scholar]
- U.S. Environmental Protection Agency (EPA), Framework for Cumulative Risk Assessment. Risk Assessment Forum. In EPA/630/P-02/001F; EPA: Washington, DC, USA, 2003.
- Levy, J.I. Is epidemiology the key to cumulative risk assessment? Risk Anal. 2008, 28, 1507–1513. [Google Scholar] [CrossRef]
- National Research Council (NRC), Science and Decisions: Advancing Risk Assessment; National Academies Press: Washington, DC, USA, 2009.
- Sexton, K. Sociodemographic aspects of human susceptibility to toxic chemicals: Do class and race matter for realistic risk assessment? Environ. Toxicol. Pharmacol. 1997, 4, 261–269. [Google Scholar] [CrossRef]
- Robbins, J.M.; Vaccarino, V.; Zhang, H.; Kasl, S.V. Socioeconomic status and type 2 diabetes in African American and Non-Hispanic White women and men: Evidence from the Third National Health and Nutrition Examination Survey. Am. J. Public Health. 2001, 91, 76–83. [Google Scholar]
- Adler, N.E.; Newman, K. Socioeconomic disparities in health: pathways and policies. Health Aff. 2002, 21, 60–76. [Google Scholar]
- Darmon, N.; Drewnowski, A. Does social class predict diet quality? Am. J. Clin. Nutr. 2008, 87, 1107–1117. [Google Scholar]
- National Ambient Air Quality Standards for Lead, Final Rule; Federal Register 73; 12 November 2008; pp. 66964–67062.
- Agency for Toxic Substances and Disease Registry (ATSDR), Toxicological Profile for Lead; U.S. Department of Health and Human Services, Public Health Service: Atlanta, GA, USA, 2007.
- Bellinger, D.; Leviton, A.; Waternaux, C.; Needleman, H.; Rabinowitz, M. Low-level lead exposure, social class, and infant development. Neurotoxicol. Teratol. 1988, 10, 497–503. [Google Scholar] [CrossRef]
- Dietrich, K.N.; Krafft, K.M.; Bornschein, R.L.; Hammond, P.B.; Berger, O.; Succop, P.A.; Bier, M. Low-level fetal lead exposure effect on neurobehavioral development in early infancy. Pediatrics 1987, 80, 721–730. [Google Scholar]
- Dietrich, K.N.; Succop, P.A.; Berger, O.G.; Hammond, P.B.; Bornschein, R.L. Lead exposure and the cognitive development of urban preschool children: The Cincinnati lead study cohort at age 4 years. Neurotoxicol. Teratol. 1991, 13, 203–211. [Google Scholar]
- Tong, S.; McMichael, A.J.; Baghurst, P.A. Interactions between environmental lead exposure and sociodemographic factors on cognitive development. Arch. Environ. Health 2000, 55, 330–335. [Google Scholar]
- Winneke, G.; Kramer, U. Neuropsychological effects of lead in children: interactions with social background variables. Neuropsychobiology 1984, 11, 195–204. [Google Scholar]
- Raab, G.M.; Thomson, G.O.B.; Boyd, L.; Fulton, M.; Laxen, D.P.H. Blood lead levels, reaction time, inspection time and ability in Edinburgh children. Br. J. Dev. Psychol. 1990, 8, 101–118. [Google Scholar] [CrossRef]
- Borella, P.; Sturloni, N.; Rovesti, S.; Vivoli, R.; Bargellini, A.; Vivoli, G. Evaluation of the risk of neuropsychological damage from lead exposure in childhood. Ann. Ist. Super. Sanità 1998, 34, 97–104. (in Italian). [Google Scholar]
- “National primary and secondary ambient air quality standards.” Title 42 U.S. Code, Sec. 7409. pp. 6223–6224, 2010 ed.
- U.S. Environmental Protection Agency (EPA), Air Quality Criteria for Lead, Volume I of II; EPA/600/R-05/144aF; EPA: Washington, DC, USA, 2006.
- U.S. Environmental Protection Agency (EPA), Lead: Human Exposure and Health Risk Assessments for Selected Case Studies. Human Exposure and Health Risk Assessments - Full-Scale, Volume I; EPA-452/R-07-014a; EPA: Washington, DC, USA, 2007.
- Henderson, R. Letter from Dr. Rogene Henderson, Chair, Clean Air Scientific Advisory Committee, to Administrator Stephen L. Johnson. Re: Clean Air Scientific Advisory Committee’s (CASAC) Review of the 1st Draft Lead Staff Paper and Draft Lead Exposure and Risk Assessments. 27 March 2007. [Google Scholar]
- Brunekreef, B. The relationship between air lead and blood lead in children: A critical review. Sci. Total Environ. 1984, 38, 79–123. [Google Scholar]
- Henderson, R. Letter from Dr. Rogene Henderson, Chair, Clean Air Scientific Advisory Committee, to Administrator Stephen L. Johnson. Re: Clean Air Scientific Advisory Committee’s (CASAC) Review of the Advance Notice of Proposed Rulemaking (ANPR) for the NAAQS for Lead. 22 January 2008. [Google Scholar]
- Chari, R. Modification of Lead Toxicity by Socioeconomic Factors and Implications for Environmental Policy. Doctoral dissertation, Johns Hopkins University, Baltimore, MD, March 2011. [Google Scholar]
- Harvey, P.; Hamlin, M.; Kumar, R.; Delves, T. Blood lead, behaviour, and intelligence test performance in preschool children. Sci. Total Environ. 1984, 40, 45–60. [Google Scholar] [CrossRef]
- Dietrich, K.N.; Krafft, K.M.; Bier, M.; Succop, P.A.; Berger, O.; Bornschein, R.L. Early effects of fetal lead exposure: neurobehavioral findings at 6 months. Int. J. Biosoc. Res. 1986, 8, 151–168. [Google Scholar]
- McMichael, A.J.; Baghurst, P.A.; Vimpani, G.V.; Robertson, E.F.; Wigg, N.R.; Tong, S.L. Sociodemographic factors modifying the effect of environmental lead on neuro-psychological development in early childhood. Neurotoxicol. Teratol. 1992, 14, 321–327. [Google Scholar]
- Tellez-Rojo, M.M.; Bellinger, D.C.; Arroyo-Quiroz, C.; Lamadrid-Figueroa, H.; Mercado-Garcia, A.; Schnaas-Arrieta, L.; Wright, R.O.; Hernandez-Avila, M.; Hu, H. Longitudinal associations between blood lead concentrations <10 µg/dL and neurobehavioral development in environmentally-exposed children in Mexico City. Pediatrics 2006, 118, e323–e330. [Google Scholar]
- Lanphear, B.P.; Hornung, R.; Khoury, J.; Yolton, K.; Baghurst, P.; Bellinger, D.C.; Canfield, R.L.; Dietrich, K.N.; Bornschein, R.; Greene, T.; et al. Low-level environmental lead exposure and children’s intellectual function: An international pooled analysis. Environ. Health Perspect. 2005, 113, 894–899. [Google Scholar]
- Canfield, R.L.; Henderson, C.R., Jr.; Cory-Slechta, D.A.; Cox, C.; Jusko, T.A.; Lanphear, B.P. Intellectual impairment in children with blood lead concentrations below 10 µg per deciliter. N. Engl. J. Med. 2003, 348, 1517–1526. [Google Scholar]
- Bellinger, D.C.; Needleman, H.L. Intellectual impairment and blood lead levels (letter). N. Engl. J. Med. 2003, 349, 500–502. [Google Scholar]
- Bailey, A.J.; Sargent, J.D.; Goodman, D.C.; Freeman, J.; Brown, M.J. Poisoned landscapes: The epidemiology of environmental lead exposure in Massachusetts children 1990-1991. Soc. Sci. Med. 1994, 39, 757–766. [Google Scholar]
- Perlin, S.A.; Wong, D.; Sexton, K. Residential proximity to industrial sources of air pollution: Interrelationships among race, poverty, and age. J. Air Waste Manag. Assoc. 2001, 51, 406–421. [Google Scholar]
- Sicotte, D.; Swanson, S. Whose risk in Philadelphia? Proximity to unequally hazardous industrial facilities. Soc. Sci. Q. 2007, 88, 515–534. [Google Scholar]
- U.S. Environmental Protection Agency (EPA), Integrated Risk Information System: IRIS Glossary; EPA: Washington, DC, USA, 2009.
- U.S. Environmental Protection Agency (EPA), Guidelines for carcinogen risk assessment. Risk Assessment Forum; EPA/630/P-03/001F; EPA: Washington, DC, USA, 2005.
- U.S. Environmental Protection Agency (EPA), Guidelines for developmental toxicity risk assessment. Risk Assessment Forum; EPA/600/FR-91/001; EPA: Washington, DC, USA, 1991.
- U.S. Environmental Protection Agency (EPA), Guidelines for reproductive toxicity risk assessment. Risk Assessment Forum; EPA/630/R-96/009; EPA: Washington, DC, USA, 1996.
- U.S. Environmental Protection Agency (EPA), Guidelines for neurotoxicity risk assessment. Risk Assessment Forum; EPA/630/R-95/001F; EPA: Washington, DC, USA, 1998.
- Schwartz, J.; Bellinger, D.; Glass, T. Expanding the scope of environmental risk assessment to better include differential vulnerability and susceptibility. Am. J. Public Health. 2011, 101, S88–S93. [Google Scholar]
- U.S. SenateCommittee on Public WorksNational air quality standards act of 1970. (S Rpt. 91-1196); Washington: Government Printing Office, 1970.
- Slovic, P.; Fischhoff, B.; Lichtenstein, S. Behavioral decision theory. Annu. Rev. Psychol. 1977, 28, 1–39. [Google Scholar]
- Hattis, D.; Anderson, E.L. What should be the implications of uncertainty, variability, and inherent “biases”/“conservatism” for risk management decision-making? Risk Anal. 1999, 19, 95–107. [Google Scholar]
- Krupnick, A.; Morgenstern, R.; Batz, M.; Nelson, P.; Burtraw, D.; Shih, J.S.; McWilliams, M. Not a Sure Thing: Making Regulatory Choices under Uncertainty; Resources for the Future: Washington, DC, USA, 2006. [Google Scholar]
- Rodricks, J.V. Some attributes of risk influencing decision-making by public health and regulatory officials. Am. J. Epidemiol. 2001, 154, S7–S12. [Google Scholar]
- Schwartz, J.; Bellinger, D.; Glass, T. Expanding the scope of risk assessment: Methods of studying differential vulnerability and susceptibility. Am. J. Public Health 2011, 101, S102–S109. [Google Scholar]
- Mahaffey, K.R. Environmental lead toxicity: Nutrition as a component of intervention. Environ. Health Perspect. 1990, 89, 75–78. [Google Scholar]
- Ruff, H.A.; Markowitz, M.E.; Bijur, P.E.; Rosen, J.F. Relationships among blood lead levels, iron deficiency, and cognitive development in two-year-old children. Environ. Health Perspect. 1996, 104, 180–185. [Google Scholar]
- Peraza, M.A.; Ayala-Fierro, F.; Barber, D.S.; Casarez, E.; Rael, L.T. Effects of micronutrients on metal toxicity. Environ. Health Perspect. 1998, 106, 203–216. [Google Scholar]
- Elmarsafawy, S.F.; Jain, N.B.; Schwartz, J.; Sparrow, D.; Nie, H.; Hu, H. Dietary calcium as a potential modifier of the relationship of lead burden to blood pressure. Epidemiology 2006, 17, 531–537. [Google Scholar]
- Cory-Slechta, D.A.; Virgolini, M.B.; Thiruchelvam, M.; Weston, D.D.; Bauter, M.R. Maternal stress modulates the effects of developmental lead exposure. Environ. Health Perspect. 2004, 112, 717–730. [Google Scholar]
- Virgolini, M.B.; Chen, K.; Weston, D.D.; Bauter, M.R.; Cory-Slechta, D.A. Interactions of chronic lead exposure and intermittent stress: consequences for brain catecholamine systems and associated behaviors and HPA axis function. Toxicol. Sci. 2005, 87, 469–482. [Google Scholar]
- Virgolini, M.B.; Bauter, M.R.; Weston, D.D.; Cory-Slechta, D.A. Permanent alterations in stress responsivity in female offspring subjected to combined maternal lead exposure and/or stress. Neurotoxicology 2006, 27, 11–21. [Google Scholar]
- Virgolini, M.B.; Rossi-George, A.; Lisek, R.; Weston, D.D.; Thiruchelvam, M.; Cory-Slechta, D.A. CNS effects of developmental Pb exposure are enhanced by combined maternal and offspring stress. Neurotoxicology 2008, 29, 812–827. [Google Scholar]
- Peters, J.L.; Kubzansky, L.; McNeely, E.; Schwartz, J.; Spiro 3rd, A.; Sparrow, D.; Wright, R.O.; Nie, H.; Hu, H. Stress as a potential modifier of the impact of lead levels on blood pressure: the normative aging study. Environ. Health Perspect. 2007, 115, 1154–1159. [Google Scholar]
- Surkan, P.J.; Schnaas, L.; Wright, R.J.; Tellez-Rojo, M.M.; Lamadrid-Figueroa, H.; Hu, H.; Hernandez-Avila, M.; Bellinger, D.C.; Schwartz, J.; Perroni, E.; et al. Maternal self-esteem, exposure to lead, and child neurodevelopment. Neurotoxicology 2008, 29, 278–285. [Google Scholar] [CrossRef]
- Nordberg, G.F.; Jin, T.; Hong, F.; Zhang, A.; Buchet, J.P.; Bernard, A. Biomarkers of cadmium and arsenic interactions. Toxicol. Appl. Pharmacol. 2005, 206, 191–197. [Google Scholar]
- de Burbure, C.; Buchet, J.P.; Leroyer, A.; Nisse, C.; Haguenoer, J.M.; Mutti, A.; Smerhovsky, Z.; Cikrt, M.; Trzcinka-Ochocka, M.; Razniewska, G.; et al. Renal and neurologic effects of cadmium, lead, mercury, and arsenic in children: Evidence of early effects and multiple interactions at environmental exposure levels. Environ. Health Perspect. 2006, 114, 584–590. [Google Scholar]
- Kim, Y.; Kim, B.N.; Hong, Y.C.; Shin, M.S.; Yoo, H.J.; Kim, J.W.; Bhang, S.Y.; Cho, S.C. Co-exposure to environmental lead and manganese affects the intelligence of school-aged children. Neurotoxicology 2009, 30, 564–571. [Google Scholar]
- Navas-Acien, A.; Tellez-Plaza, M.; Guallar, E.; Muntner, P.; Silbergeld, E.; Jaar, B.; Weaver, V. Blood cadmium and lead and chronic kidney disease in U.S. adults: A joint analysis. Am. J. Epidemiol. 2009, 170, 1156–1164. [Google Scholar] [CrossRef]
- Park, S.K.; Schwartz, J.; Weisskopf, M.; Sparrow, D.; Vokonas, P.S.; Wright, R.O.; Coull, B.; Nie, H.; Hu, H. Low-level lead exposure, metabolic syndrome, and heart rate variability: The VA Normative Aging Study. Environ. Health Perspect. 2006, 114, 1718–1724. [Google Scholar]
© 2012 by the authors; licensee MDPI, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Chari, R.; Burke, T.A.; White, R.H.; Fox, M.A. Integrating Susceptibility into Environmental Policy: An Analysis of the National Ambient Air Quality Standard for Lead. Int. J. Environ. Res. Public Health 2012, 9, 1077-1096. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph9041077
Chari R, Burke TA, White RH, Fox MA. Integrating Susceptibility into Environmental Policy: An Analysis of the National Ambient Air Quality Standard for Lead. International Journal of Environmental Research and Public Health. 2012; 9(4):1077-1096. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph9041077
Chicago/Turabian StyleChari, Ramya, Thomas A. Burke, Ronald H. White, and Mary A. Fox. 2012. "Integrating Susceptibility into Environmental Policy: An Analysis of the National Ambient Air Quality Standard for Lead" International Journal of Environmental Research and Public Health 9, no. 4: 1077-1096. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph9041077