Differential Effects of High-Carbohydrate and High-Fat Diet Composition on Metabolic Control and Insulin Resistance in Normal Rats


Abstract
:1. Introduction
2. Material and Methods
2.1. Materials
2.2. Animals and Diets

{kind=link}
{kind=link}
| HSFD | HUFD | HDSD | HRSD | ||
|---|---|---|---|---|---|
| g/Kg | g/Kg | g/Kg | g/Kg | ||
| Protein | |||||
| Casein | 254.1 | 254.1 | 212.9 | 212.9 | |
| Lipid | |||||
| Corn oil | 11.1 | 11.1 | |||
| Olive oil | 364.5 | ||||
| Lard | 364.5 | ||||
| Carbohydrates | |||||
| Corn starch | 305 | 305 | 675 | ||
| Banana starch | 675 | ||||
| Sucrose | 33.8 | 33.8 | 67 | 67 | |
| Vit. & Min. | 15 | 15 | 15 | 15 | |
| Caloric value (Kcal/g) | 5.6 | 5.6 | 3.9 | 3.9 | |
2.3. Oral Glucose Tolerance Test
2.4. Rat Euthanization and Sample Collection
2.5. Biochemical Measurements
2.6. Statistical Analysis
3. Results
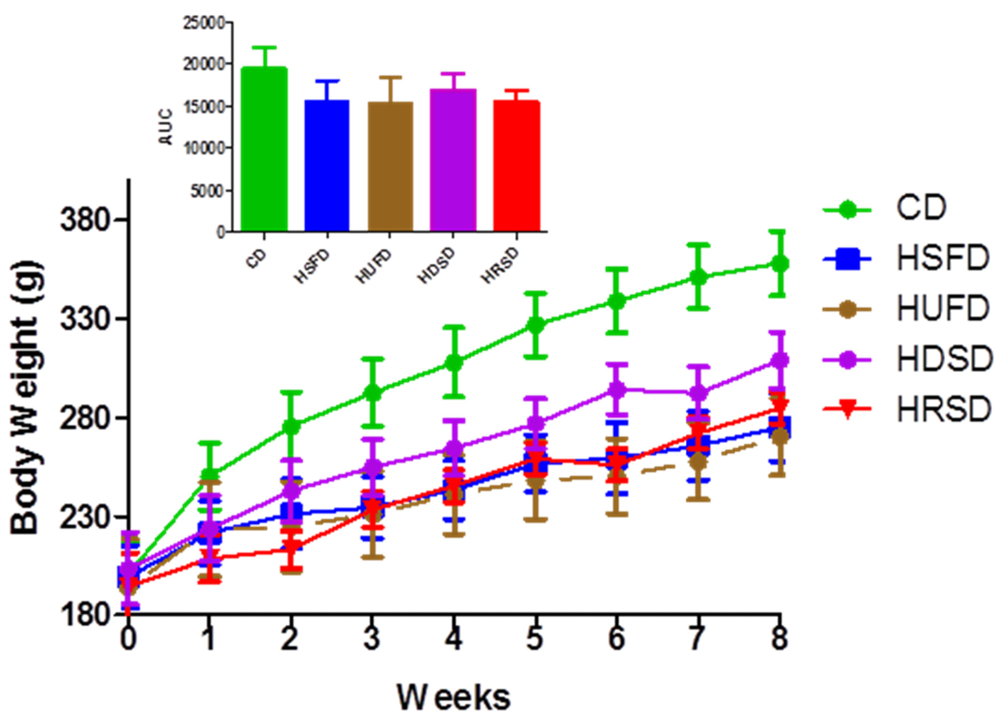
3.1. Body Weight and Energy Intake
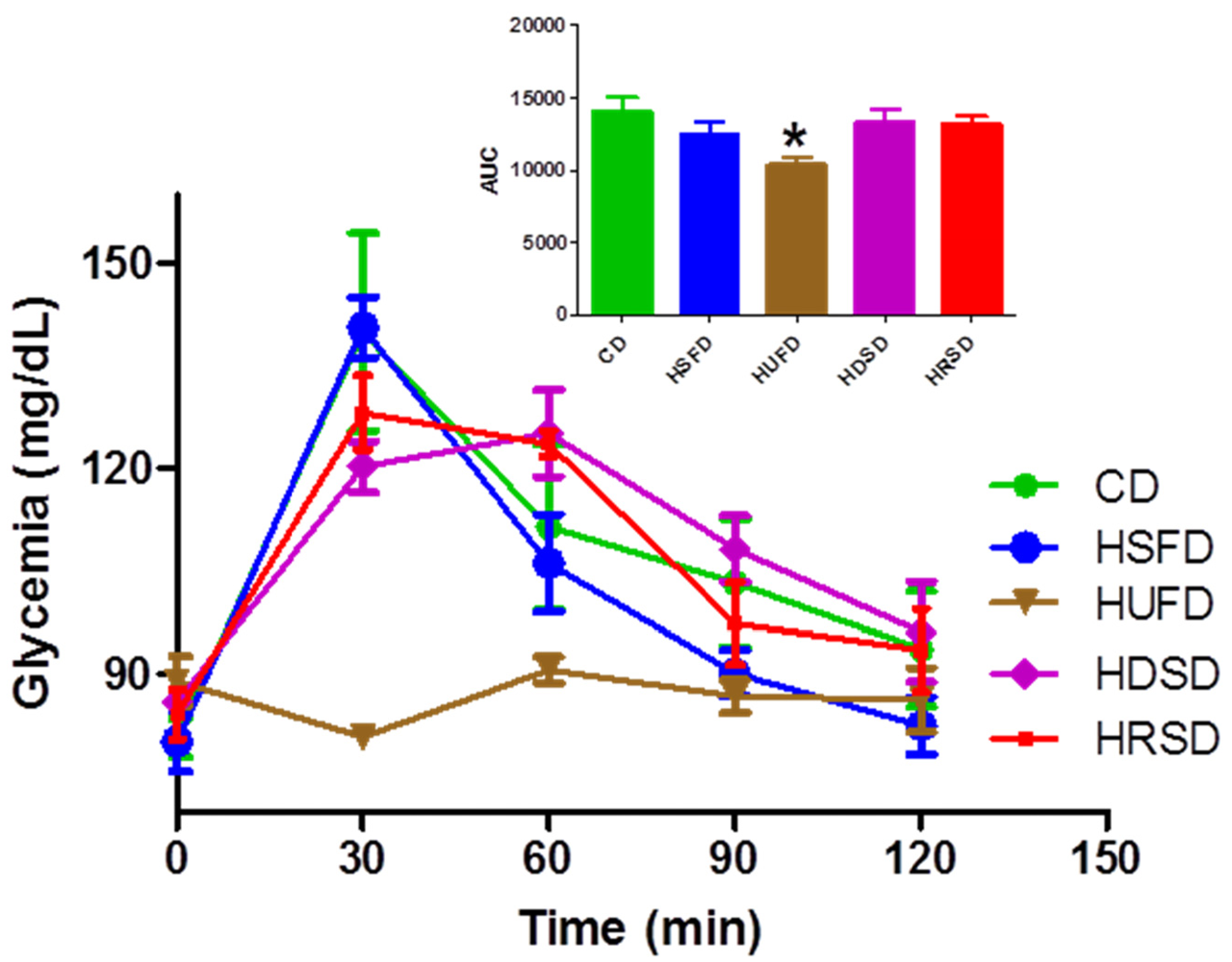
3.2. Glycemic Control

| CD | HSFD | HUFD | HDSD | HRSD | |
|---|---|---|---|---|---|
| Body weight (g) | 307 ± 16.7 a,B,C | 247 ± 8.0 a | 242 ± 7.7 B | 268 ± 11.7 | 246 ± 10.7C |
| Calories (Cal) | 395 ± 7.5 A,E | 378 ± 11.3 B,F | 355 ± 11.3 C | 628 ± 8.7 D,E,F | 845 ± 44.4 A,B,C,D |
| Variable | CD | HSFD | HUFD | HDSD | HRSD |
|---|---|---|---|---|---|
| Glucose (mg/dL) | 108.2 ± 11.2 | 94 ± 5.9 | 83 ± 4.0 a | 98 ± 4.0 | 121 ± 3.0 a |
| Insulin (ng/mL) | 1.1 ± 0.2 a | 0.6 ± 0.2 | 0.2 ± 0.1 a,B | 1.3 ± 0.3 B | 0.9 ± 0.2 |
| HOMA Index | 7.5 ± 1.7 A | 3.8 ± 1.3 | 0.9 ± 0.3 A,B,C | 7.8 ± 1.9 B | 6.6 ± 1.5 C |

3.3. Lipidic Control
| Variable | CD | HSFD | HUFD | HDSD | HRSD |
|---|---|---|---|---|---|
| TAG (mg/dL) | 118 ± 17.1 a | 67 ± 6.8 c | 65 ± 9.2 | 147 ± 17.9 B,c | 55 ±9.4 a,B |
| Chol (mg/dL) | 73 ± 4.1 | 73 ± 4.5 | 81 ± 3.3 A | 70 ± 4.9 | 50 ± 2.6A |
| HDL-Chol (mg/dL) | 30 ± 1.2 | 34 ± 1.9 b | 35 ± 1.6 a | 31 ± 2.0 | 26 ± 0.8 a,b |
3.4. Hepatic Determinations
| Variable (mg/g) | CD | HSFD | HUFD | HDSD | HRSD |
|---|---|---|---|---|---|
| Total Lipids | 36 ± 1.3 A | 50 ± 3.4 B | 58 ± 2.3 A,C,D | 39 ± 3.3 D | 29 ± 0.7 B,C |
| CHOL | 2.1 ± 0.08 | 3.0 ± 0.07 a | 2.2 ± 0.1 | 3.0 ± 0.2 b | 1.9 ± 0.09 a,b |
| TAG | 2.9 ± 0.2 c,d | 3.6 ± 0.6 a,d,f | 2.8 ± 0.4 a,b | 3.7 ± 1.1 b,c,e | 2.9 ± 0.4 e,f |
4. Discussion
5. Conclusions
Conflict of Interest
Contributions
Acknowledgements
References
- Centers for Disease Control and Prevention. National Diabetes Fact Sheet: National Estimates and General Information on Diabetes and Prediabetes in the United States, 2011; U.S. Department of Health and Human Services, Centers for Disease Control and Prevention: Atlanta, GA, USA, 2011. Available online: http://www.cdc.gov/diabetes/pubs/factsheet.htm (accessed on 1 October 2011).
- Bessesen, D.H. Update on obesity. J. Clin. Endocr. Metab. 2008, 93, 2027–2034. [Google Scholar]
- Bray, G.A. Medical consequences of obesity. J. Clin. Endocr. Metab. 2004, 89, 2583–2589. [Google Scholar]
- Reaven, G.; Abbasi, F.; McLaughlin, T. Obesity, insulin resistance, and cardiovascular disease. Recent Prog. Horm. Res. 2004, 59, 207–223. [Google Scholar] [CrossRef]
- Nordmann, A.J.; Nordmann, A.; Briel, M.; Keller, U.; Yancy, W.S., Jr.; Brehm, B.J.; Bucher, H.C. Effects of low-carbohydrate vs. low-fat diets on weight loss and cardiovascular risk factors: A meta-analysis of randomized controlled trials. Arch. Intern. Med. 2006, 166, 285–293. [Google Scholar] [CrossRef]
- Yancy, W.S., Jr.; Olsen, M.K.; Guyton, J.R.; Bakst, R.P.; Westman, E.C. A low-carbohydrate, ketogenic diet versus a low-fat diet to treat obesity and hyperlipidemia: A randomized, controlled trial. Ann. Intern. Med. 2004, 140, 769–777. [Google Scholar]
- Volek, J.S.; Fernandez, M.L.; Feinman, R.D.; Phinney, S.D. Dietary carbohydrate restriction induces a unique metabolic state positively affecting atherogenic dyslipidemia, fatty acid partitioning, and metabolic syndrome. Prog. Lipid Res. 2008, 47, 307–318. [Google Scholar] [CrossRef]
- Lara-Castro, C.; Garvey, W.T. Diet, insulin resistance, and obesity: Zoning in on data for Atkins dieters living in South Beach. J. Clin. Endocr. Metab. 2004, 89, 4197–4205. [Google Scholar] [CrossRef]
- Lichtenstein, A.H.; Appel, L.J.; Brands, M.; Carnethon, M.; Daniels, S.; Franch, H.A.; Franklin, B.; Kris-Etherton, P.; Harris, W.S.; Howard, B.; et al. Diet and lifestyle recommendations revision 2006: A scientific statement from the American Heart Association Nutrition Committee. Circulation 2006, 114, 82–96. [Google Scholar]
- U.S. Department of Agriculture and U.S. Department of Health and Human Services, Dietary Guidelines for Americans, 7th edU.S. Government Printing Office: Washington, DC, USA, 2010.
- Surwit, R.S.; Kuhn, C.M.; Cochrane, C.; McCubbin, J.A.; Feinglos, M.N. Diet-induced type II diabetes in C57BL/6J mice. Diabetes 1988, 37, 1163–1167. [Google Scholar]
- Rossmeisl, M.; Rim, J.S.; Koza, R.A.; Kozak, L.P. Variation in type 2 diabetes—Related traits in mouse strains susceptible to diet-induced obesity. Diabetes 2003, 52, 1958–1966. [Google Scholar]
- Chun, M.R.; Lee, Y.J.; Kim, K.H.; Kim, Y.W.; Park, S.Y.; Lee, K.M.; Kim, J.Y.; Park, Y.K. Differential effects of high-carbohydrate and high-fat diet composition on muscle insulin resistance in rats. J. Korean Med. Sci. 2010, 25, 1053–1059. [Google Scholar]
- Higgins, J.A. Resistant starch: Metabolic effects and potential health benefits. J. AOAC Int. 2004, 87, 761–768. [Google Scholar]
- Nugent, A.P. Health properties of resistant starch. Nutr. Bull. 2005, 30, 27–54. [Google Scholar]
- Department of Food, Environment and Rural Affairs, Family Food: Report on the Expenditure and Food Survey; DEFRA: London, UK, 2006.
- Anderson, G.H.; Woodend, D. Effect of glycemic carbohydrates on short-term satiety and food intake. Nutr. Rev. 2003, 61, S17–S26. [Google Scholar]
- Mermelstein, N.H. Analyzing for resistant starch. Food Technol. 2009, 63, 80–84. [Google Scholar]
- Pérez-Sánchez, E. Efectos del Consumo de una Formulación que Incluye Almidón Resistente de Plátano en la Glucemia Postprandial de Pacientes con Diabetes Mellitus tipo 2. Tesis de Maestría en Ciencias Alimentarias, Universidad Juárez Autónoma de Tabasco, Villahermosa, Tabasco, México, 2007. [Google Scholar]
- Olvera-Hernández, V. Almidón Resistente de Banano Enano Gigante (Cavendish AAA) en la Glicemia y Producción de Acidos Grasos de Cadena Corta en Ratas con Síndrome Metabólico. Tesis de Maestría en Ciencias Alimentarias, Universidad Juárez Autónoma de Tabasco, Villahermosa, Tabasco, México, 2009. [Google Scholar]
- Ble-Castillo, J.L.; Aparicio-Trapala, M.A.; Francisco-Luria, M.U.; Cordova-Uscanga, R.; Rodriguez-Hernandez, A.; Mendez, J.D.; Diaz-Zagoya, J.C. Effects of native banana starch supplementation on body weight and insulin sensitivity in obese type 2 diabetics. Int. J. Environ. Res. Public Health 2010, 7, 1953–1962. [Google Scholar]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar]
- Folch, J.; Lees, M.; Sloane Stanley, G.H. A simple method for the isolation and purification of total lipides from animal tissues. J. Biol. Chem. 1957, 226, 497–509. [Google Scholar]
- Uhley, V.E.; Jen, K.L. Changes in feeding efficiency and carcass composition in rats on repeated high-fat feedings. Int. J. Obesity 1989, 13, 849–856. [Google Scholar]
- Hill, J.O.; Fried, S.K.; DiGirolamo, M. Effects of a high-fat diet on energy intake and expenditure in rats. Life Sci. 1983, 33, 141–149. [Google Scholar]
- Aziz, A.A.; Kenney, L.S.; Goulet, B.; Abdel-Aal, el-S. Dietary starch type affects body weight and glycemic control in freely fed but not energy-restricted obese rats. J. Nutr. 2009, 139, 1881–1889. [Google Scholar] [CrossRef]
- Willis, H.J.; Eldridge, A.L.; Beiseigel, J.; Thomas, W.; Slavin, J.L. Greater satiety response with resistant starch and corn bran in human subjects. Nutr. Res. 2009, 29, 100–105. [Google Scholar]
- Bodinham, C.L.; Frost, G.S.; Robertson, M.D. Acute ingestion of resistant starch reduces food intake in healthy adults. Br. J. Nutr. 2010, 103, 917–922. [Google Scholar]
- Bradley, U.; Spence, M.; Courtney, C.H.; McKinley, M.C.; Ennis, C.N.; McCance, D.R.; McEneny, J.; Bell, P.M.; Young, I.S.; Hunter, S.J. Low-fat versus low-carbohydrate weight reduction diets: Effects on weight loss, insulin resistance, and cardiovascular risk: A randomized control trial. Diabetes 2009, 58, 2741–2748. [Google Scholar] [CrossRef]
- Tay, J.; Brinkworth, G.D.; Noakes, M.; Keogh, J.; Clifton, P.M. Metabolic effects of weight loss on a very-low-carbohydrate diet compared with an isocaloric high-carbohydrate diet in abdominally obese subjects. J. Am. Coll. Cardiol. 2008, 51, 59–67. [Google Scholar]
- Visioli, F.; Galli, C. Antiatherogenic components of olive oil. Curr. Atheroscler. Rep. 2001, 3, 64–67. [Google Scholar]
- Turner, R.; Etienne, N.; Alonso, M.G.; de Pascual-Teresa, S.; Minihane, A.M.; Weinberg, P.D.; Rimbach, G. Antioxidant and anti-atherogenic activities of olive oil phenolics. Int. J. Vitam. Nutr. Res. 2005, 75, 61–70. [Google Scholar]
- Pan, D.A.; Lillioja, S.; Milner, M.R.; Kriketos, A.D.; Baur, L.A.; Bogardus, C.; Storlien, L.H. Skeletal muscle membrane lipid composition is related to adiposity and insulin action. J. Clin. Invest. 1995, 96, 2802–2808. [Google Scholar]
- Prieto, P.G.; Cancelas, J.; Villanueva-Penacarrillo, M.L.; Valverde, I.; Malaisse, W.J. Effects of an olive oil-enriched diet on plasma GLP-1 concentration and intestinal content, plasma insulin concentration, and glucose tolerance in normal rats. Endocrine 2005, 26, 107–115. [Google Scholar] [CrossRef]
- Garg, A.; Bantle, J.P.; Henry, R.R.; Coulston, A.M.; Griver, K.A.; Raatz, S.K.; Brinkley, L.; Chen, Y.-D.I.; Grundy, S.M.; Huet, B.A.; et al. Effects of varying carbohydrate content of diet in patients with non-insulin-dependent diabetes mellitus. J. Am. Med. Assoc. 1994, 271, 1421–1428. [Google Scholar]
- Thomsen, C.; Storm, H.; Holst, J.J.; Hermansen, K. Differential effects of saturated and monounsaturated fats on postprandial lipemia and glucagon-like peptide 1 responses in patients with type 2 diabetes. Am. J. Clin. Nutr. 2003, 77, 605–611. [Google Scholar]
- Bessesen, D.H. The role of carbohydrates in insulin resistance. J. Nutr. 2001, 131, S2782–S2786. [Google Scholar]
- Zhou, J.; Martin, R.J.; Tulley, R.T.; Raggio, A.M.; McCutcheon, K.L.; Shen, L.; Danna, S.C.; Tripathy, S.; Hegsted, M.; Keenan, M.J. Dietary resistant starch upregulates total GLP-1 and PYY in a sustained day-long manner through fermentation in rodents. Am. J. Physiol. Endoc. M. 2008, 295, E1160–E1166. [Google Scholar]
© 2012 by the authors; licensee MDPI, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Ble-Castillo, J.L.; Aparicio-Trapala, M.A.; Juárez-Rojop, I.E.; Torres-Lopez, J.E.; Mendez, J.D.; Aguilar-Mariscal, H.; Olvera-Hernández, V.; Palma-Cordova, L.C.; Diaz-Zagoya, J.C. Differential Effects of High-Carbohydrate and High-Fat Diet Composition on Metabolic Control and Insulin Resistance in Normal Rats. Int. J. Environ. Res. Public Health 2012, 9, 1663-1676. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph9051663
Ble-Castillo JL, Aparicio-Trapala MA, Juárez-Rojop IE, Torres-Lopez JE, Mendez JD, Aguilar-Mariscal H, Olvera-Hernández V, Palma-Cordova LC, Diaz-Zagoya JC. Differential Effects of High-Carbohydrate and High-Fat Diet Composition on Metabolic Control and Insulin Resistance in Normal Rats. International Journal of Environmental Research and Public Health. 2012; 9(5):1663-1676. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph9051663
Chicago/Turabian StyleBle-Castillo, Jorge L., María A. Aparicio-Trapala, Isela E. Juárez-Rojop, Jorge E. Torres-Lopez, Jose D. Mendez, Hidemi Aguilar-Mariscal, Viridiana Olvera-Hernández, Leydi C. Palma-Cordova, and Juan C. Diaz-Zagoya. 2012. "Differential Effects of High-Carbohydrate and High-Fat Diet Composition on Metabolic Control and Insulin Resistance in Normal Rats" International Journal of Environmental Research and Public Health 9, no. 5: 1663-1676. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph9051663