1. Introduction
Stable iodide (
127I
−), as potassium iodide (KI) or “dietary iodine”, has been recognized for over 30 years as a practical thyroid radioprotectant for people exposed to radioactive isotopes of iodide [
1,
2]. In a recent National Academies of Science report on the distribution and administration of KI in the event of a nuclear incident [
3], sodium perchlorate (Irenat
®) was recommended for adults if KI treatment was contraindicated, such as in patients with preexisting thyroid disease. Successful thyroid radioprotectant treatments, such as KI or ammonium perchlorate (NH
4ClO
4), are judged by their ability to block or limit thyroidal uptake of trace amounts of radioactive iodide (e.g.,
131I
−), while limited research has focused on treatment doses promoting excretion of the isotopes. Currently, the United States Food and Drug Administration (US FDA) recommends KI tablets as a preventative treatment for
131I
− poisoning of the thyroid gland [
4].
Studies utilizing rats in the 1950s and 1960s demonstrated that perchlorate (ClO
4−) altered the serum pharmacokinetics of
131I
− [
5,
6,
7]. The kinetic profile of
131I
− in laboratory animals treated with ClO
4− was characterized by decreased serum
131I
− levels and increased urine
131I
− levels [
6]. In the presence of ClO
4−,
131I
− is excreted in urine more rapidly, presumably because perchlorate blocks basolateral and/or apical uptake of
131I
− into sodium iodide symporter- or pendrin-protein rich tissues, such as the thyroid and small intestine [
5,
8,
9,
10,
11,
12]. Additionally, perchlorate administration displaces non-organified iodide from the thyroid, and the perchlorate discharge test has been used to diagnose iodide organification defects in humans for decades [
10]. Perchlorate has been shown to have side effects ranging from rash and fever to several fatal cases of aplastic anemia [
13,
14], though these effects typically manifest from large bolus doses administered over weeks or months [
15].
Rats administered ClO
4− intravenously (0.1–3.0 mg/kg) excreted approximately 83% of the administered ClO
4− dose over 24 hours [
16]. In a similar experiment, these authors also intravenously dosed rats with 3.3 mg/kg of isotonically labeled ClO
4− (
36ClO
4) and reported that 96% of the dose was excreted in 24 hours and 99.5% by 48 hours [
17]. In a recent study, an oral dose of 30 mg/kg of ClO
4− was administered to rats, and 38% of the dose was recovered in urine within the first 12 hours after dosing [
15].
In the present rat study, the effectiveness of KI and NH
4ClO
4 to increase excretion of
131I
− into urine over a 3 day period was assessed, with and without T
4 administration. In previous rat studies we reported that over a 15 hour post dosing period, KI and NH
4ClO
4 were equally effective at reducing thyroid gland exposure to
131I
− [
15]. However, NH
4ClO
4 was more effective at increasing urinary clearance of
131I
− than KI. This study extends the timeframe of the experiment from 15 to 75 hours and also evaluates the influence of T
4 administration on
131I
− kinetics. Rats, unlike humans, have short thyroxine half-lives in serum, and are sensitive to up-regulation of the thyroid gland by thyroid stimulating hormone (TSH) [
18]. To control the potential for TSH mediated stimulation of the thyroid gland, one subset of rats for each treatment group received replacement doses of T
4 to suppress the potential for TSH release [
19,
20].
2. Materials and Methods
2.1. Chemicals
Ammonium perchlorate (99.8%), 100% ethanol, and sodium hydroxide were purchased from Aldrich (Milwaukee, WI, USA). Nonradioactive thyroxine was purchased from Sigma Chemical Corporation (St. Louis, MO, USA). Potassium iodide was obtained from J. T. Baker (Phillipsburg, NJ, USA), carrier-free iodide-131 (131I−) from Amersham Biosciences (29.4 mCi/µg), acepromazine maleate (10 mg/mL) and ketamine HCl (100 mg/mL) from Fort Dodge Animal Health (Fort Dodge, IA, USA) and xylazine (20 mg/mL) from Ben Venue Laboratories (Bedford, OH, USA). Isoflurane (99.9%) was purchased from Abbott Laboratories (Abbott Park, IL, USA).
2.2. Animals and Experimental Design
Male Sprague-Dawley rats (330 ± 30 g, approximately 11 weeks old) from Harlan Laboratories (Indianapolis, IN, USA) were provided LabDiet™ Laboratory Rodent Diet 5001 rat chow and water ad libitum. The animals used in this study were handled in accordance with the procedures of The University of Georgia Institutional Animal Care and Use Committee (IACUC), AUP# A2005-10110-0. The rats experienced a 12 hour light and dark cycle, with room air temperature at 22 ± 2 °C and relative humidity at 50 ± 20%.
Rats were housed individually in metabolism cages for a 5 day acclimation period prior to the start of the experiments. Twelve hours before the experiment commenced, food was removed from the animals to ensure complete absorption of the radiotracer and treatment doses. A summary of the experiments is shown in
Table 1. The general experimental protocol was to dose rats orally with 2.91 µCi (6 ng/kg)
131I
− in saline solution (1 mL) by oral gavage and then return the rats to their metabolism cages. Rats from Group 1 (n = 6 for each treatment group) were removed from their metabolism cages after 3 hours and dosed by oral gavage with 1 mL of either 0.9% saline, 30 mg/kg of KI (calculated as iodide) or 30 mg/kg of NH
4ClO
4 (calculated as ClO
4−) dissolved in 0.9% aqueous saline. Rats from Group 2 (n = 6 for each treatment group) followed the same experimental protocol as Group 1 except each animal received a 0.1 mL intraperitoneal (ip) injection of 15 µg/kg of T
4 (based on euthyroid replacement T
4 doses administered by [
21]) dissolved in 0.1 M NaOH and 1 animal from each treatment group received a 0.1 mL ip injection of 0.1 M NaOH (controls). Data from animals in Group 2 that received ip injections of NaOH had not statistically different from animals of a similar treatment in Group 1. As a result, data from animals in Group 2 that received ip injections of NaOH were assimilated with animals of a similar treatment in Group 1. The rats were held in metabolism cages for 75 hours for urine collections. Urine from Groups 1 and 2 were collected via metabolism cage vials at +3, 6, 12, 18, 24, 30, 36, 42, 48, 54, 60, 66, 72, and 75 hours. Blood was collected from the tail vein of animals in dose Groups 1 and 2 at 15 hours after dosing with
131I
− and at sacrifice. At sacrifice (75 hours after dosing with
131I
−), animals in Groups 1 and 2 were anesthetized with a ketamine cocktail (50 mg/kg ketamine, 3.3 mg/kg xylazine, and 3.4 mg/kg acepromazine administered at 0.1 mL per 100 g BW), then killed by asphyxiation at +75 hours. Blood was collected via cardiac puncture and serum prepared by centrifugation at 1,500 rpm at 4 °C for 15 min. Thyroid lobes were removed from the trachea and weighed. Urine was removed from the bladder via syringe. Sera, urine, and thyroid glands were stored at −80 °C until analysis.
Table 1.
Summary of experiments in the rat to characterize excretion profiles of 131I− following prophylactic administration of saline, KI, or perchlorate with and without T4 hormone replacement.
Table 1.
Summary of experiments in the rat to characterize excretion profiles of 131I− following prophylactic administration of saline, KI, or perchlorate with and without T4 hormone replacement.
| Experiment | Description | Dose (mg/kg) | Urine Collection Times (hours) | T4 Injection Times (hours) | Serum and Thyroid Collection Time (hours) |
|---|
| Group 1 (n = 36) 12 rats each for saline, KI and NH4ClO4 treatment groups | Single oral dose of 131I− followed 3 hours later by single oral doses of saline, KI, or NH4ClO4 | ORAL 131I−: 6 × 10−6 KI: 30 ClO4: 30 | 3, 6, 12, 18, 24, 30, 36, 42, 48, 54, 60, 66, 72, and 75 | --- | Serum: 15 and 75 Thyroid: 75 |
| Group 2 (n = 18) 6 rats each for saline, KI and NH4ClO4 treatment groups | Equal to Group 1 | Equal to Group 1 ip T4: 0.015 | Equal to Group 1 | T4 doses at time of saline, KI and NH4ClO4 doses, then 24, and 48 hours later | Serum: 15 and 75 Thyroid: 75 |
2.3. 131I− Analysis
Serial urine samples were placed on a gamma counter (1470 Wallac Wizard) equipped with one detector and 131I− counts/minute (cpm) were measured within 2 hours after collection. 131I− cpm were also assessed in whole thyroids and serum samples within 2 hours of sacrifice. Raw counts were recorded. Urine and sera were then stored at −80 °C for no less than 80 days (10 half-lives for 131I−) in order for the radioactivity to decay.
Serum TSH measurements were made using a rat TSH radioimmunoassay kit from A. F. Parlow and the National Hormone & Peptide Program (lot numbers AFP329691Rb, AFP11542B, and AFP5512B).
2.4. 127I− and ClO4− Analysis
Non-radioactive analytes (
127I
− and ClO
4−) were quantified using ion chromatography coupled with tandem mass spectrometry. Serum samples were spiked with internal standard (
129I
− and Cl
18O
4−), treated to remove proteins, and analyzed by ion chromatography electrospray ionization tandem mass spectrometry [
22]. Urine samples were spiked with internal standard (
129I
− and Cl
18O
4−) and analyzed by ion chromatography electrospray ionization tandem mass spectrometry [
23].
2.5. Urinary Excretion Kinetics of Anions
All urine samples for Groups 1 and 2 were analyzed for 131I− excretion kinetics. Animals in Groups 1 and 2 that received 127I− or ClO4− also had urine samples analyzed for 127I− or ClO4− excretion kinetics. All half-life calculations were prepared using Win Non Lin 5.2 software.
2.6. Statistical Analysis
Single factor analysis of variance (ANOVA) was used initially to determine significance across the treatment groups (control saline, KI and NH4ClO4) with statistical significance set at p < 0.05. Once statistical significance was determined across the treatment groups by ANOVA, a limited number of comparisons were carried out using a two-sample t-test (assuming equal variance) to compare each treatment group (p < 0.05) to control and to each other. All calculations were performed using Microsoft Excel. It should be noted that animals in Group 2 that received ip injections of NaOH were lumped together with animals in Group 1 of a similar treatment dose, i.e., saline, KI, or ClO4−.
3. Results
3.1. 131I− Excretion in Urine
Rats were administered
131I
−, then 3 hours later either saline, 30 mg/kg of KI or 30 mg/kg of NH
4ClO
4 by oral bolus gavage. Group 2 was distinguished from Group 1 (
Table 1) by repeated T
4 administration, first at the time of dosing with saline, KI or NH
4ClO
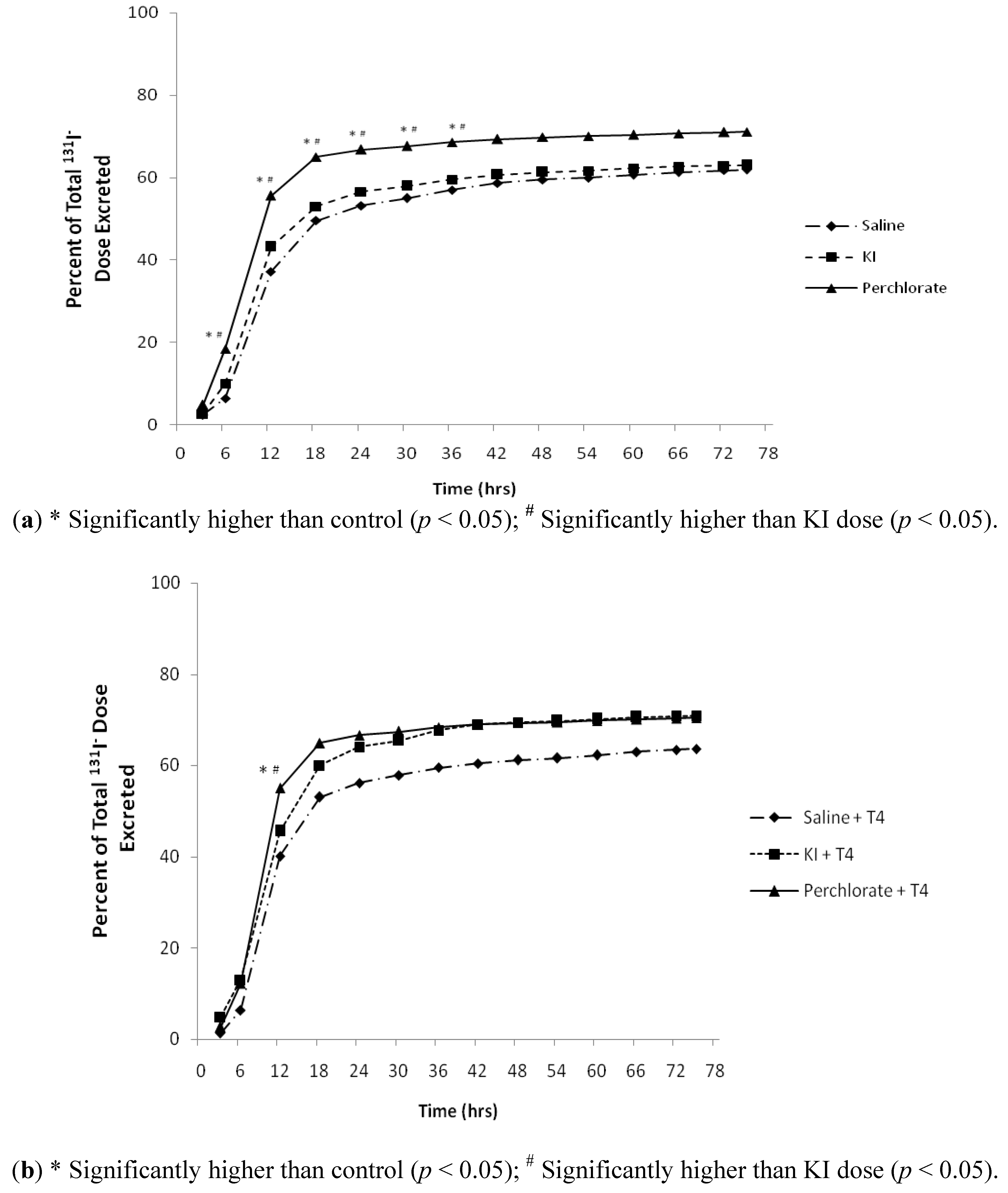
4, then at +27 hours and +51 hours during the time-course. The 3-day cumulative volumes of urine produced were 39.7 ± 7.7 mL for Group 1 and 41.3 ± 5.7 mL for Group 2. In Group 1, 71, 63, and 62% of the administered
131I
− doses for NH
4ClO
4, KI, and control saline treatment groups, respectively (
Figure 1a), were excreted in urine by 75 hours after dosing with
131I
−. In Group 2, 72, 71, and 63% of the administered doses of
131I
− were excreted in urine for the NH
4ClO
4, KI, and saline control treatment groups, respectively (
Figure 1b) by 75 hours after dosing with
131I
−. Most of the
131I
− collected over the 3-day period (60.5 ± 6%) was excreted in urine by 24 hours after dosing in all treatments for Groups 1 and 2 (
Figure 1(a,b)). The 24-hour urinary excretion half-lives for
131I
− (
Table 2) in control and KI treated rats ranged from 3.5 to 4 hours; conversely, NH
4ClO
4 treated rats excreted
131I
− more rapidly (2.6 hour urinary excretion half-life,
p < 0.001).
Table 2.
Twenty four hour urinary excretion half-lives for 131I− for Group 1 and 2 rats.
Table 2.
Twenty four hour urinary excretion half-lives for 131I− for Group 1 and 2 rats.
| 131I− Excretion Half Lives (hours) |
|---|
| | Group 1 131I− | Group 2 131I− + T4 |
|---|
| Saline Control | 4.0 ± 0.7 | 3.7 ± 1.2 |
| KI | 3.5 ± 0.5 | 3.8 ± 0.3 |
| NH4ClO4 | 2.6 ± 0.4 *,# | 2.6 ± 0.4 *,# |
Figure 1.
(a) Percent of total 131I− dose excreted in urine 75 hour of Group 1 male rats collected via metabolism cages dosed with 131I− followed by saline, KI (30 mg/kg), or perchlorate (30 mg/kg) 3 hours later (n = 12), statistical analysis was conducted on concentration data for each individual time-point (data not shown); (b) Percent of total 131I− dose excreted in 75 hour urine of Group 2 male rats collected via metabolism cages dosed with 131I− followed by saline, KI (30 mg/kg), or perchlorate (30 mg/kg) at +3 hours and dosed with replacement T4 at +3, +27, and +51 hours (n = 6), statistical analysis was conducted on concentration data for each individual time-point (data not shown).
Figure 1.
(a) Percent of total 131I− dose excreted in urine 75 hour of Group 1 male rats collected via metabolism cages dosed with 131I− followed by saline, KI (30 mg/kg), or perchlorate (30 mg/kg) 3 hours later (n = 12), statistical analysis was conducted on concentration data for each individual time-point (data not shown); (b) Percent of total 131I− dose excreted in 75 hour urine of Group 2 male rats collected via metabolism cages dosed with 131I− followed by saline, KI (30 mg/kg), or perchlorate (30 mg/kg) at +3 hours and dosed with replacement T4 at +3, +27, and +51 hours (n = 6), statistical analysis was conducted on concentration data for each individual time-point (data not shown).
3.2. 131I− in Serum and Thyroid
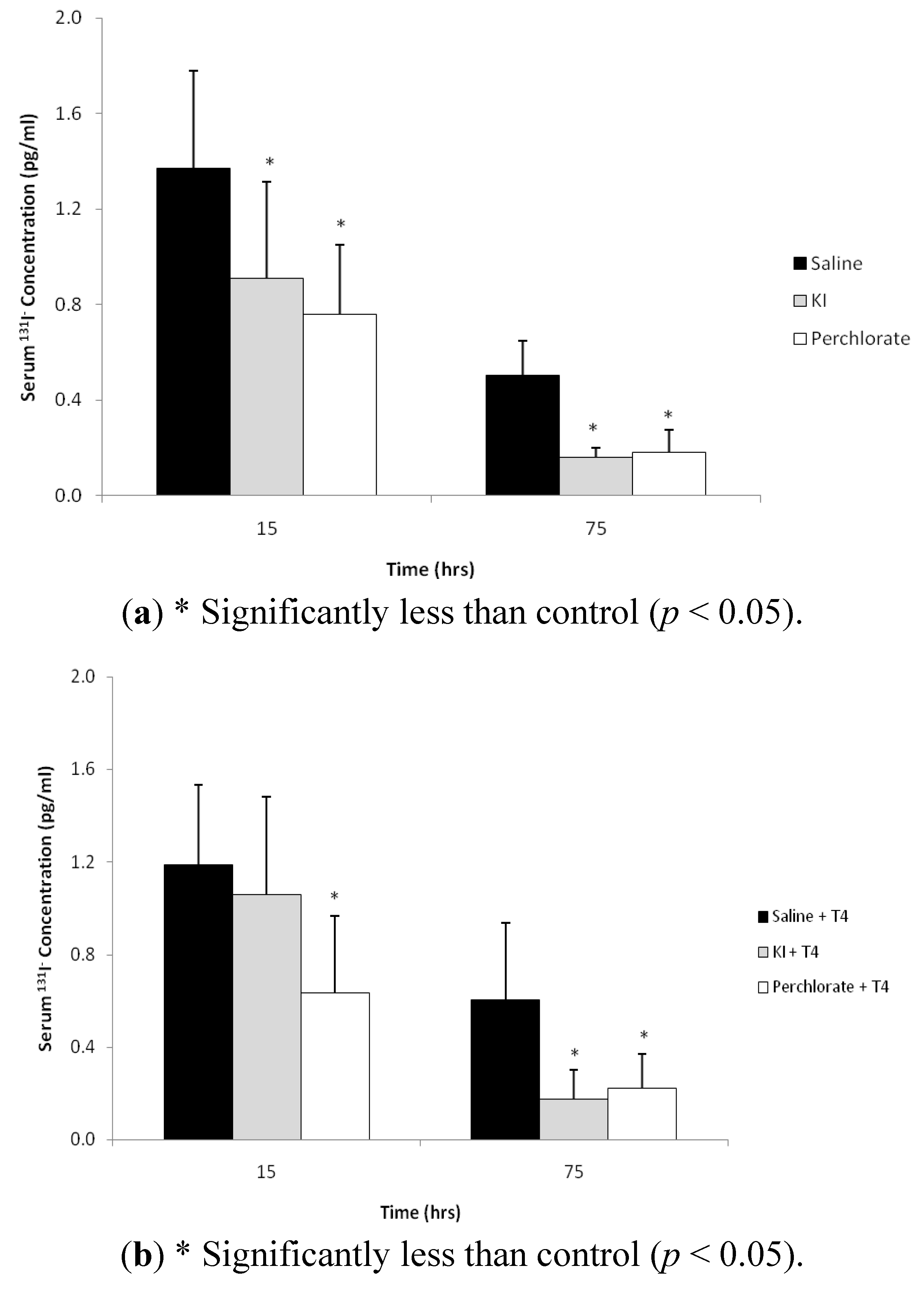
The mean
131I
− concentration in the Group 1 control serum at 15 hours after
131I
− dosing was 1.37 ± 0.41 pg/mL and decreased to 0.50 ± 0.15 pg/mL at 75 hours post dosing (
Figure 2a). In Group 1, the mean
131I
− serum levels in the KI and the NH
4ClO
4 treatment groups at 15 hours were 0.91 ± 0.40 and 0.76 ± 0.29 pg/mL, and decreased to 0.16 ± 0.04 and 0.18 ± 0.09 pg/mL, respectively, at 75 hours post dosing. The
131I
− serum concentrations in the KI and NH
4ClO
4 treatment groups were significantly less than saline controls for both sampling times (
p < 0.05). The addition of T
4 proved to have little effect on mean serum
131I
− concentration for Group 2 (
Figure 2b). The mean serum
131I
− concentrations at 15 hours following T
4 and saline, KI and NH
4ClO
4 treatments was 1.2 ± 0.35, 1.06 ± 0.42, and 0.64 ± 0.33 pg/mL respectively, and decreased to 0.61 ± 0.33, 0.17 ± 0.12, and 0.22 ± 0.15 pg/mL at 75 hours post dosing. At 15 hours post
131I
− dosing, only the NH
4ClO
4 treatment group
131I
− concentrations were significantly less (
p < 0.05) than controls, while both KI and NH
4ClO
4 treatment group
131I
− concentrations were significantly less than controls at the 75 hour sampling time.
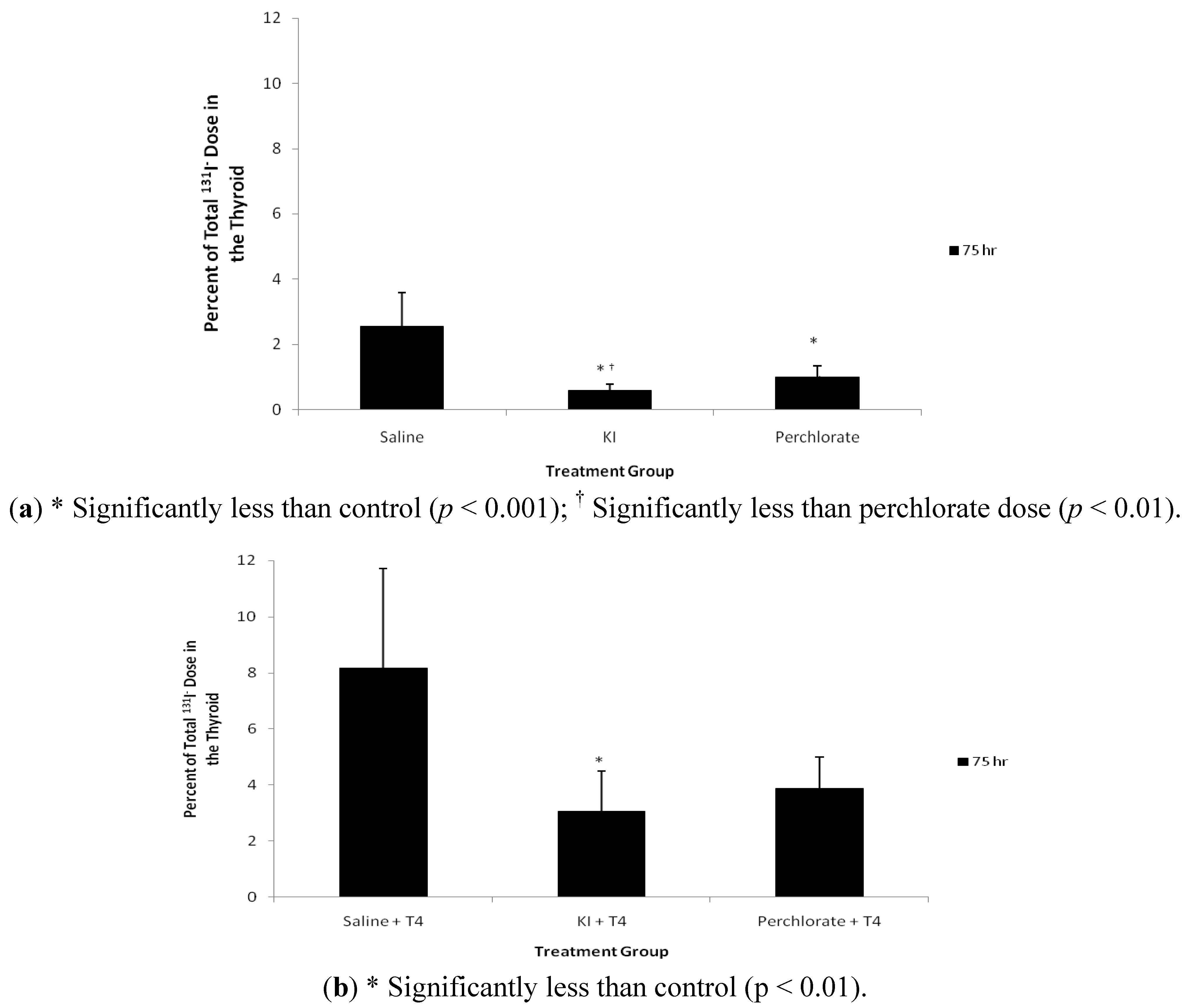
Compared with control saline, KI and NH
4ClO
4 treatment reduced levels of
131I
− in thyroid gland at 75 hours post exposure (
Figure 3a). Also the residual
131I
− levels in the thyroid gland in the KI treatment group were lower than the NH
4ClO
4 treatment group (
p < 0.01). KI and NH
4ClO
4 treatment reduced the thyroid content of
131I
− by 77 and 61%, respectively, 3 days after administration of
131I
−. Group 2 animals treated with T
4 displayed a different thyroidal
131I
− content (
Figure 3b). The mean residual percentage of
131I
− doses were less in both the KI (38% of control) and NH
4ClO
4 (48% of control) treatment groups, compared with saline controls; however, only the KI treatment was significantly less than controls (
p < 0.01). Interestingly, control, KI, and NH
4ClO
4 treated rats from Group 2 retained more thyroidal
131I
− than rats from Group 1, which did not receive T
4 treatment.
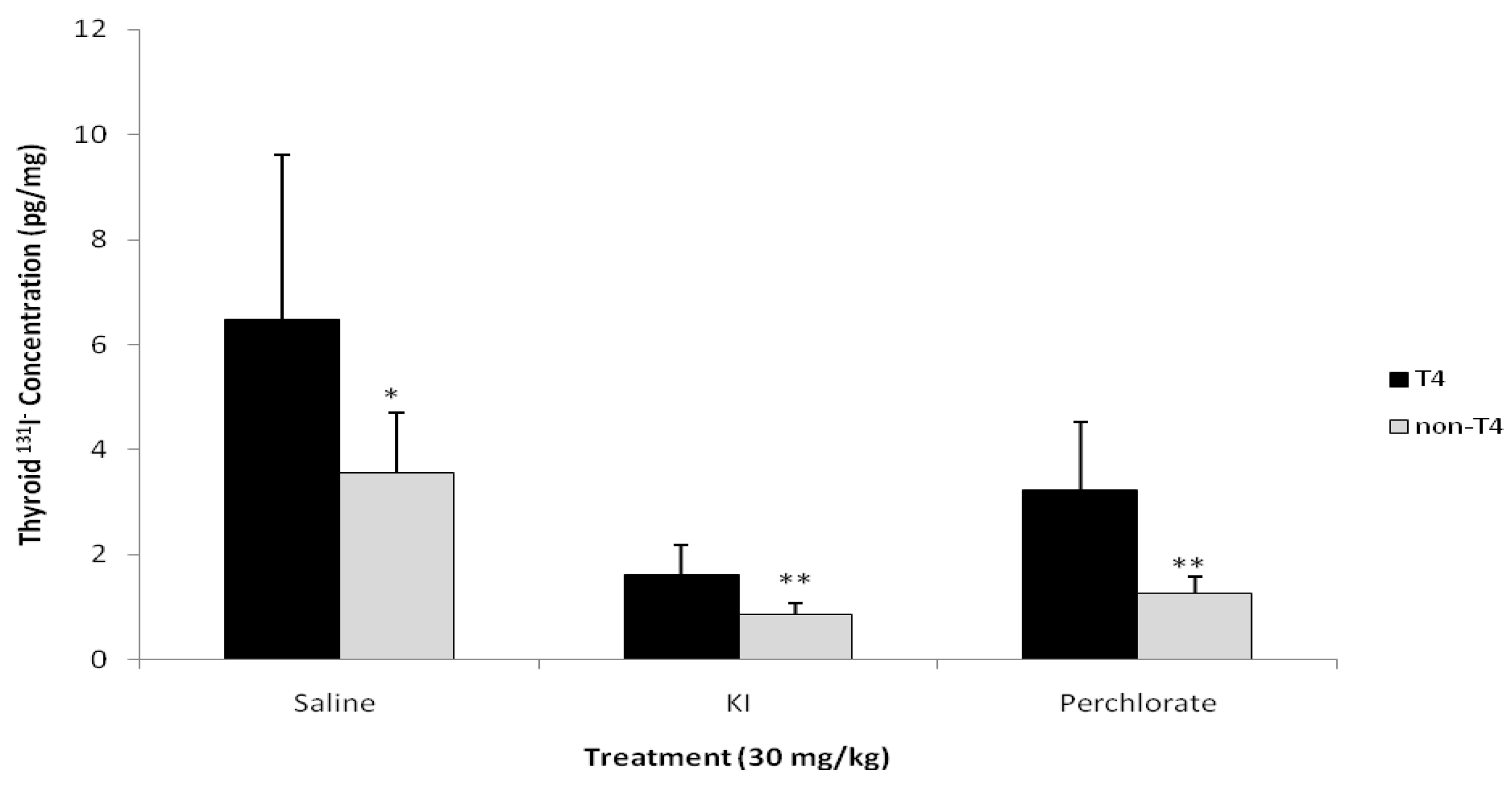
Figure 4 compares the thyroidal
131I
− concentrations for Groups 1 and 2. In all cases, T
4 treatment resulted in increased thyroidal
131I
− concentrations (
p < 0.05).
3.3. 127I− and ClO4−: Urinary Excretion and Serum Concentrations
In Group 1 rats, the cumulative amounts of 127I− and ClO4− excreted in urine over 72 hours were 128 and 92%, respectively, of the administered doses of 127I− as KI, and ClO4−, as NH4ClO4. Most of the excretion of 127I− (93%) and ClO4− (97%) occurred within 24 hours of dosing. In the T4 treated group, 106% and 86% of 127I− and ClO4−, respectively, was excreted in urine by 72 hours after dosing. Eighty four and 96% of the excreted 127I− and ClO4− anions occurred within 24 hours.
Stable iodide urinary half lives determined using 24 h urine collections in rats that were treated with KI for Groups 1 and 2 were 3.5 ± 0.6 and 3.9 ± 0.3 hours respectively, with no significance between groups. Perchlorate 24 hour urinary half lives in rats that were treated with NH4ClO4 for Groups 1 and 2 were 2.5 ± 0.5 and 2.5 ± 0.4 hours, respectively.
Serum concentrations of 127I− and ClO4− 72 hours after administration were 200.4 ± 199.8 and 81.3 ± 31.6 ng/mL, respectively, in Group 1 and 56.7 ± 15.9 ng/mL and 26.3 ± 14.6 ng/mL, respectively in Group 2.
Figure 2.
(
a)
131I
− concentrations (pg/mL) in serum of Group 1 male rats collected via tail vein bleed at 15 and via cardiac puncture 75 hours after oral administration of
131I
− and 12 and 72 hours after oral administration of either saline, KI (30 mg/kg), or perchlorate (30 mg/kg) as described in
Figure 1a. Data are means ± standard deviation (n = 12); (
b)
131I
−concentrations (pg/mL) in serum of Group 2 male rats collected via tail vein bleed at +15 hours and via cardiac puncture at 75 hours after oral administration of
131I
−. Animals were dosed with
131I
− followed by saline, KI (30 mg/kg), or perchlorate (30 mg/kg) and dosed with replacement T
4 as described in
Figure 1b. Data are means ± standard deviation (n = 6).
Figure 2.
(
a)
131I
− concentrations (pg/mL) in serum of Group 1 male rats collected via tail vein bleed at 15 and via cardiac puncture 75 hours after oral administration of
131I
− and 12 and 72 hours after oral administration of either saline, KI (30 mg/kg), or perchlorate (30 mg/kg) as described in
Figure 1a. Data are means ± standard deviation (n = 12); (
b)
131I
−concentrations (pg/mL) in serum of Group 2 male rats collected via tail vein bleed at +15 hours and via cardiac puncture at 75 hours after oral administration of
131I
−. Animals were dosed with
131I
− followed by saline, KI (30 mg/kg), or perchlorate (30 mg/kg) and dosed with replacement T
4 as described in
Figure 1b. Data are means ± standard deviation (n = 6).
Figure 3.
(
a) 75 hour percent of total
131I
− in the thyroid of Group 1 male rats dosed with
131I
− via gavage followed by saline, KI (30 mg/kg), or perchlorate (30 mg/kg) as described in
Figure 1a. Data are means ± standard deviation (n = 12); (
b) 75 hour + T
4 percent of total
131I
− in the thyroid of Group 2 male rats dosed with
131I
− via gavage followed by saline, KI (30 mg/kg), or perchlorate (30 mg/kg) and dosed with T
4 replacement as described in
Figure 1b. Data are means ± standard deviation (n = 6).
Figure 3.
(
a) 75 hour percent of total
131I
− in the thyroid of Group 1 male rats dosed with
131I
− via gavage followed by saline, KI (30 mg/kg), or perchlorate (30 mg/kg) as described in
Figure 1a. Data are means ± standard deviation (n = 12); (
b) 75 hour + T
4 percent of total
131I
− in the thyroid of Group 2 male rats dosed with
131I
− via gavage followed by saline, KI (30 mg/kg), or perchlorate (30 mg/kg) and dosed with T
4 replacement as described in
Figure 1b. Data are means ± standard deviation (n = 6).
Figure 4.
Comparison of 131I− concentration in the thyroid of male rats administered T4 versus rats not administered hormone replacement therapy (n = 12 for non-T4 and n = 6 for T4). * Saline treatment without T4 has a significantly less 131I− thyroid concentration than saline with T4 (p < 0.05); ** KI and perchlorate treatment without T4 has a significantly less 131I− thyroid concentration than KI and perchlorate with T4 (p < 0.001).
Figure 4.
Comparison of 131I− concentration in the thyroid of male rats administered T4 versus rats not administered hormone replacement therapy (n = 12 for non-T4 and n = 6 for T4). * Saline treatment without T4 has a significantly less 131I− thyroid concentration than saline with T4 (p < 0.05); ** KI and perchlorate treatment without T4 has a significantly less 131I− thyroid concentration than KI and perchlorate with T4 (p < 0.001).
3.4. Serum TSH Levels
The mean serum TSH concentrations for Group 1 was 4.12 ± 1.1, 4.04 ± 1.5, and 3.35 ± 1.8 ng/mL for the saline, KI, and NH4ClO4 treatments, respectively. No statistical significance was determined between treatment groups. Serum TSH concentrations were below the limit of detection of the assay (1.4 ng/mL) in Group 2.
4. Discussion
The objective of this study was to compare the relative efficacy of stable iodide and perchlorate to purge
131I
− from the body of rats. We evaluated the efficacy of these post-exposure treatments by monitoring
131I
− in the thyroid gland, urine, and serum for up to 3 days after dosing. This study design was based on a previous study in our laboratory [
15], which showed that at 15 hours after treatment with KI or NH
4ClO
4, the perchlorate treated rats excreted three times the amount of
131I
− in urine compared with control treatments, while stable iodide treated rats excreted only twice the amount of
131I
− in urine compared with control treatments. In the current study, we confirm our earlier results that perchlorate treatment led to faster
131I
− excretion compared with KI treatment (
Table 2). Interestingly, by 75 hours after dosing there was no difference in the total amount of
131I
− excreted in urine between treatment groups and the controls. This attenuation of the initial efficacy can be attributed to the short half-lives of perchlorate and iodide, 7.3 and 6 hours respectively [
17,
24], and suggests that repeated dosing with either treatment may most effectively clear
131I
− from the human body and thus protect the thyroid from radiation poisoning.
One interesting finding in this study is that rats treated with T
4 retained more thyroidal
131I
− than rats without T
4 treatment for all treatment groups at 75 hours after dosing (
Figure 4). Other metrics of
131I
− internal exposure for urine and serum were comparable for Groups 1 and 2,
i.e., no significant differences were determined between groups in the cumulative amounts of
131I
−, stable iodide, or perchlorate excreted in the urine at 75 hours after dosing or in the concentrations of
131I
−, stable iodide, or perchlorate in serum at 15 and 75 hours after dosing. Although the goal of T
4 administration was to inhibit spikes in serum TSH levels after administration of KI or NH
4ClO
4, the outcome was diminished serum TSH levels below euthyroid levels, thus altering the thyroid gland function. The stimulatory effect of the reduced levels of TSH in T
4-treated rats on thyroid hormone secretion was probably very low compared with the non-T
4 treated rats, resulting in increased residual
131I
− radioactivity. The increase in residual thyroid radioactivity can likely not be attributed to the well known Wolff-Chaikoff effect given its transient nature relative to the duration of the experiment. However, the Wolff-Chaikoff effect must be considered if multiple doses of the treatments are administered over time.
The effectiveness of stable iodide and perchlorate as radioprotectants for
131I
− uptake into the thyroid gland is time-dependent [
25,
26]. Zanzonico and Becker (2000) [
25] determined that when KI is administered to rats 2 hours after
131I
− exposure there is an 80% reduction in uptake of radioactive iodide in the thyroid. However, when KI is administered 8 hours after
131I
− exposure the reduction in uptake of radioactive iodide is reduced by 50%. Sinadinovic and Jovanovic (1971) [
26] concluded that when rats were administered perchlorate and KI 30 min or 24 hours prior to radioiodide tracer administration, the perchlorate treated animals accelerated the elimination of radioiodide from the body, reducing its systemic biological half life, compared to KI treated rats. In our experiments, the KI treated rats excreted the same total amount of radioiodide at 3 days post exposure as perchlorate treated animals, but at a slower excretion rate. We plan further experiments to evaluate the efficacy of repeated treatments of perchlorate and KI.
In conclusion, our findings suggest that stable iodide and perchlorate appear equally potent at enhancing urinary elimination of radioiodide over a 3 day period. However, the perchlorate treatment offers an accelerated elimination rate of radioiodide within the first 24 to 36 hours and has a significant reduction in the biological half-life of 131I− in the first 24 hours. This suggests that repeated doses of perchlorate post radioiodide exposure may increase the effectiveness of blocking uptake in the thyroid and eliminating radiation in the urine. These data support continued consideration of perchlorate as a prophylactic drug to treat radioiodide poisoning. Intentional and unintentional releases of radiation remain a public health concern in many countries and more research is needed to identify the most effective therapies for protecting the thyroid from radioiodide poisoning.


{kind=link}
{kind=link}
{kind=link}
{kind=link}



