Incidence and Mortality of Prostate Cancer in Canada during 1992–2010

 , ,
, ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Data Collection
2.2. Mandatory Data Rounding
2.3. Data Analysis
3. Results
3.1. Demographic Information on Canadian Patients
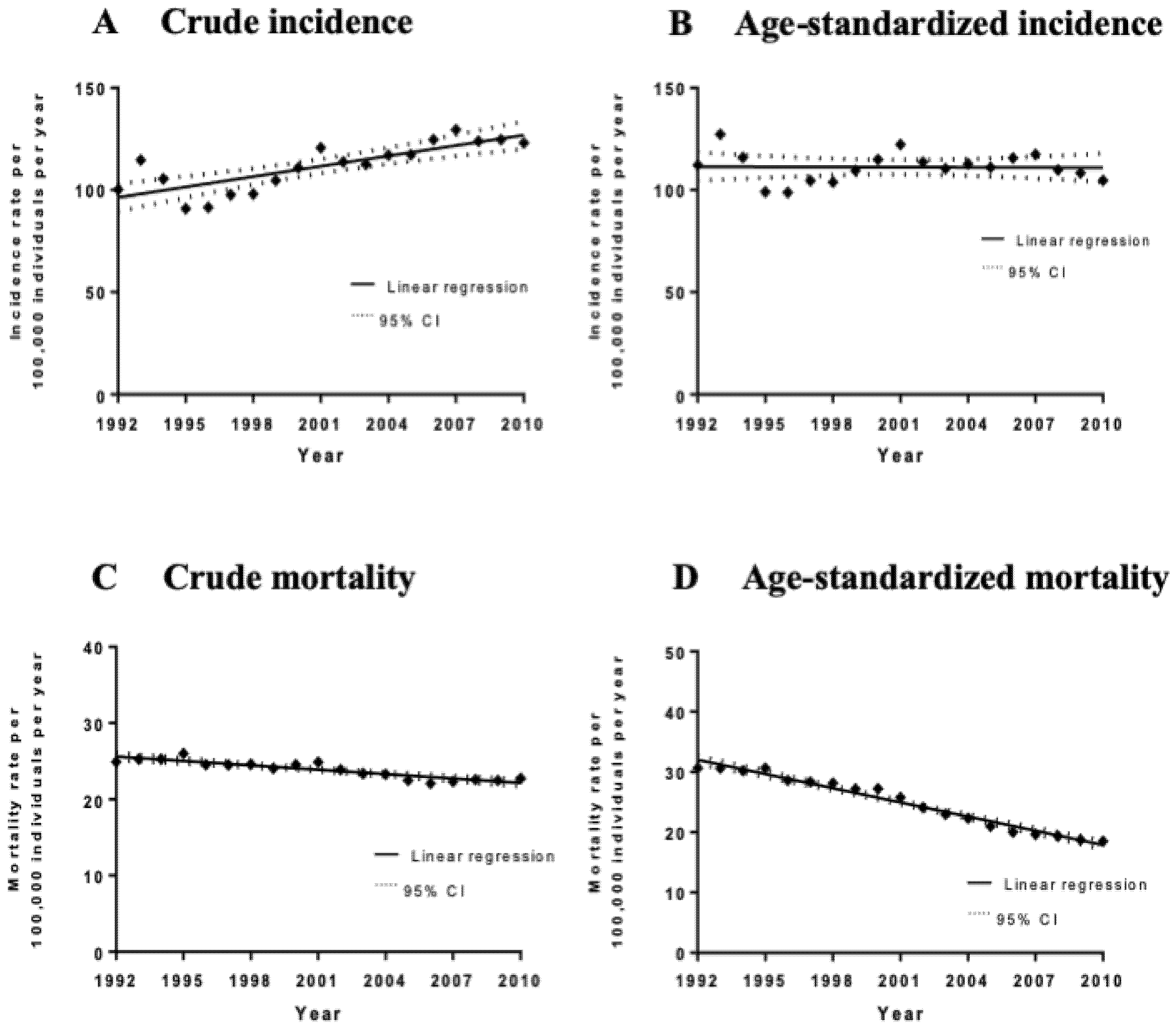
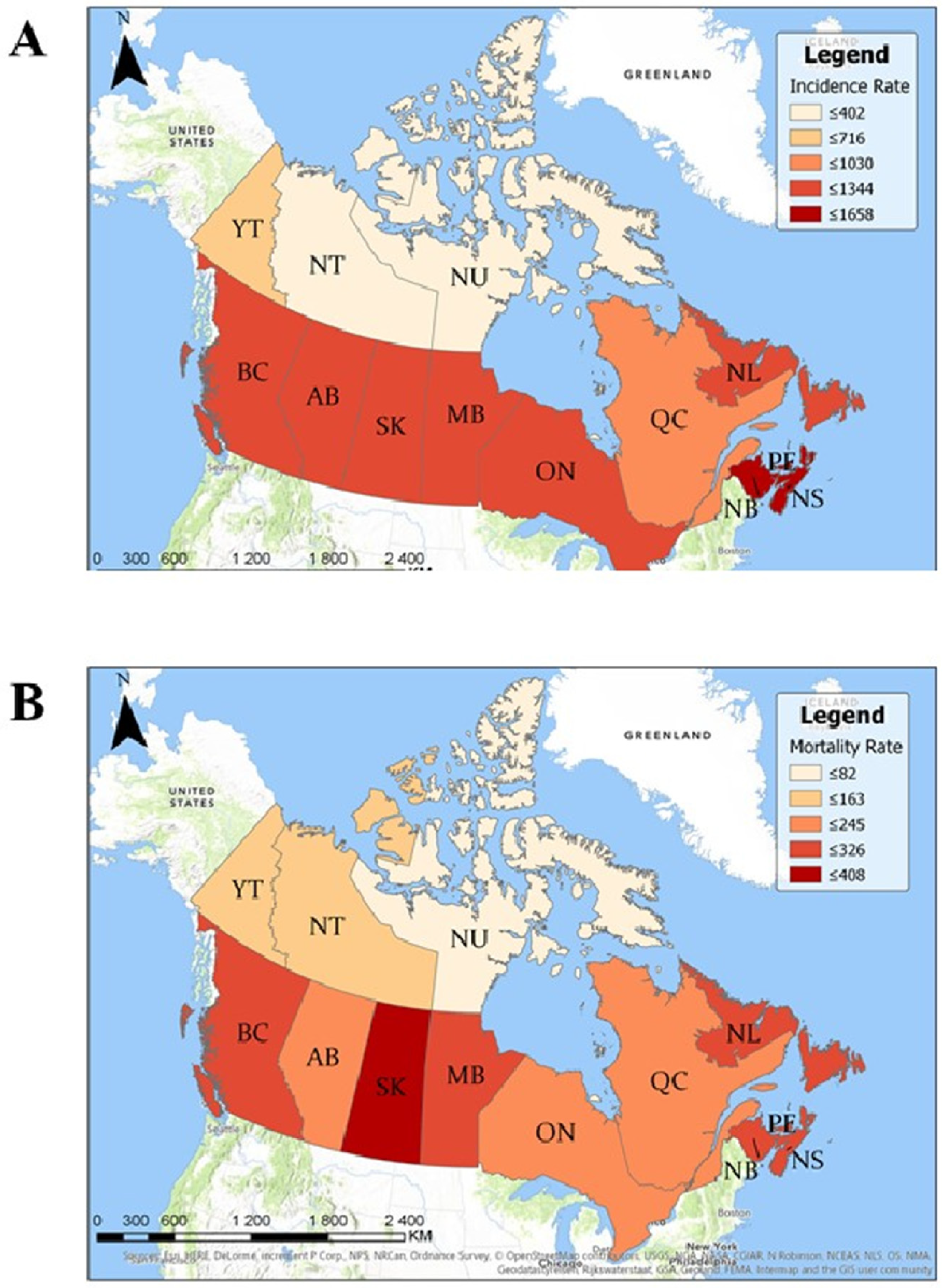
3.2. Analysis of Incidence and Geographic Distribution of Cases of Prostate Cancer in Canada
3.3. Analysis of Mortality Rates and Geographic Distribution of Deaths Due to Prostate Cancer
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Crawford, E. Epidemiology of prostate cancer. Urology 2003, 62, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Martin, D.; Miller, A.P.; Quesnel-Vallée, A.; Caron, N.R.; Vissandjée, B.; Marchildon, G.P. Canada’s universal health-care system: Achieving its potential. Lancet 2018, 391, 1718–1735. [Google Scholar] [CrossRef]
- Strumpf, E.C.; Chai, Z.; Kadiyala, S. Adherence to cancer screening guidelines across Canadian provinces: An observational study. BMC Cancer 2010, 10, 304. [Google Scholar] [CrossRef] [Green Version]
- Kadiyala, S.; Strumpf, E.C. Are United States and Canadian cancer screening rates consistent with guideline information regarding the age of screening initiation? Int. J. Qual. Health Care 2011, 23, 611–620. [Google Scholar] [CrossRef]
- Bell, N.; Gorber, S.C.; Shane, A.; Joffres, M.; Singh, H.; Dickinson, J.; Shaw, E.; Dunfield, L.; Tonelli, M.; Canadian Task Force on Preventive Health Care. Recommendations on screening for prostate cancer with the prostate-specific antigen test. Can. Med. Assoc. J. 2014, 186, 1225–1234. [Google Scholar] [CrossRef] [Green Version]
- Leslie, S.W. Cancer, Prostate; StatPearls Publishing: Treasure Island, FL, USA, 2018. [Google Scholar]
- Bashir, M.N. Epidemiology of Prostate Cancer. Asian Pac. J. Cancer Prev. 2015, 16, 5137–5141. [Google Scholar] [CrossRef] [Green Version]
- Daniyal, M.; Siddiqui, Z.A.; Akram, M.; Asif, H.; Sultana, S.; Khan, A. Epidemiology, Etiology, Diagnosis and Treatment of Prostate Cancer. Asian Pac. J. Cancer Prev. 2014, 15, 9575–9578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brawley, O.W. Prostate cancer epidemiology in the United States. World J. Urol. 2012, 30, 195–200. [Google Scholar] [CrossRef] [PubMed]
- Tsang, M.; Le, M.; Ghazawi, F.M.; Cyr, J.; Alakel, A.; Rahme, E.; Lagacé, F.; Netchiporouk, E.; Moreau, L.; Zubarev, A.; et al. Multiple myeloma epidemiology and patient geographic distribution in Canada: A population study. Cancer 2019, 125, 2435–2444. [Google Scholar] [CrossRef]
- Lagacé, F.; Ghazawi, F.M.; Le, M.; Rahme, E.; Savin, E.; Zubarev, A.; Alakel, A.; Sasseville, D.; Moreau, L.; Meterissian, S.; et al. Analysis of incidence, mortality trends, and geographic distribution of breast cancer patients in Canada. Breast Cancer Res. Treat. 2019, 178, 683–691. [Google Scholar] [CrossRef]
- Ghazawi, F.M.; Netchiporouk, E.; Rahme, E.; Tsang, M.; Moreau, L.; Glassman, S.; Provost, N.; Gilbert, M.; Jean, S.; Roshdy, O. Distribution and Clustering of Cutaneous T-Cell Lymphoma (CTCL) Cases in Canada During 1992 to 2010. J. Cutan. Med. Surg. 2018, 22, 154–165. [Google Scholar] [CrossRef]
- Ghazawi, F.M.; Netchiporouk, E.; Rahme, E.; Tsang, M.; Moreau, L.; Glassman, S.; Provost, N.; Gilbert, M.; Jean, S.-E.; Pehr, K.; et al. Comprehensive analysis of cutaneous T-cell lymphoma (CTCL) incidence and mortality in Canada reveals changing trends and geographic clustering for this malignancy. Cancer 2017, 123, 3550–3567. [Google Scholar] [CrossRef] [Green Version]
- Le, M.; Ghazawi, F.M.; Alakel, A.; Netchiporouk, E.; Rahme, E.; Zubarev, A.; Powell, M.; Moreau, L.; Roshdy, O.; Glassman, S.J. Incidence and mortality trends and geographic patterns of follicular lymphoma in Canada. Curr. Oncol. 2019, 26, e473–e481. [Google Scholar] [CrossRef] [Green Version]
- Le, M.; Ghazawi, F.M.; Rahme, E.; Alakel, A.; Netchiporouk, E.; Savin, E.; Zubarev, A.; Glassman, S.J.; Sasseville, D.; Popradi, G.; et al. Identification of significant geographic clustering of polycythemia vera cases in Montreal, Canada. Cancer 2019, 125, 3953–3959. [Google Scholar] [CrossRef]
- Ghazawi, F.M.; Darwich, R.; Le, M.; Rahme, E.; Zubarev, A.; Moreau, L.; Burnier, J.V.; Sasseville, D.; Burnier, M.N. Uveal melanoma incidence trends in Canada: A national comprehensive population-based study. Br. J. Ophthalmol. 2019, 103, 1872–1876. [Google Scholar] [CrossRef]
- Darwich, R.; Ghazawi, F.M.; Rahme, E.; AlGhazawi, N.; Burnier, J.V.; Sasseville, D.; Burnier, M.N.; Litvinov, I.V. Retinoblastoma Incidence Trends in Canada: A National Comprehensive Population-Based Study. J. Pediatr. Ophthalmol. Strabismus 2019, 56, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Amar, L.; Le, M.; Ghazawi, F.M.; Rahme, E.; Segal, A.; Netchiporouk, E.; Popradi, G.; Moreau, L.; Roshdy, O.; Sasseville, D.; et al. Prevalence of human T cell lymphotropic virus 1 infection in Canada. Curr. Oncol. 2019, 26, e3–e5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cattelan, L.; Ghazawi, F.M.; Le, M.; Lagacé, F.; Savin, E.; Zubarev, A.; Gantchev, J.; Tomaszewski, M.; Sasseville, D.; Waschke, K.; et al. Epidemiologic trends and geographic distribution of esophageal cancer in Canada: A national population-based study. Cancer Med. 2020, 9, 401–417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cattelan, L.; Ghazawi, F.M.; Le, M.; Savin, E.; Zubarev, A.; Lagacé, F.; Sasseville, D.; Waschke, K.; Litvinov, I.V. Investigating epidemiologic trends and the geographic distribution of patients with anal squamous cell carcinoma throughout Canada. Curr. Oncol. 2020, 27, e294–e306. [Google Scholar] [CrossRef] [PubMed]
- Darwich, R.; Ghazawi, F.M.; Le, M.; Rahme, E.; AlGhazawi, N.; Zubarev, A.; Moreau, L.; Sasseville, D.; Jr, M.N.B.; Litvinov, I.V. Epidemiology of invasive ocular surface squamous neoplasia in Canada during 1992–2010. Br. J. Ophthalmol. 2020, 104, 1368–1372. [Google Scholar] [CrossRef] [PubMed]
- Darwich, R.; Ghazawi, F.M.; Rahme, E.; AlGhazawi, N.; Zubarev, A.; Moreau, L.; Sasseville, D.; Jr, M.N.B.; Litvinov, I.V. Epidemiology of ophthalmic lymphoma in Canada during 1992–2010. Br. J. Ophthalmol. 2019, 104, 1176–1180. [Google Scholar] [CrossRef]
- Ghazawi, F.M.; Darwich, R.; Le, M.; Jfri, A.; Rahme, E.; Burnier, J.V.; Sasseville, D.; Jr, M.N.B.; Litvinov, I.V. Incidence trends of conjunctival malignant melanoma in Canada. Br. J. Ophthalmol. 2019, 104, 23–25. [Google Scholar] [CrossRef] [PubMed]
- Ghazawi, F.M.; Lu, J.; Savin, E.; Zubarev, A.; Chauvin, P.; Sasseville, D.; Zeitouni, A.; Litvinov, I.V. Epidemiology and Patient Distribution of Oral Cavity and Oropharyngeal SCC in Canada. J. Cutan. Med. Surg. 2020, 24, 340–349. [Google Scholar] [CrossRef] [PubMed]
- Lagacé, F.; Ghazawi, F.M.; Le, M.; Savin, E.; Zubarev, A.; Powell, M.; Moreau, L.; Sasseville, D.; Popa, I.; Litvinov, I.V. Penile Invasive Squamous Cell Carcinoma: Analysis of Incidence, Mortality Trends, and Geographic Distribution in Canada. J. Cutan. Med. Surg. 2019, 24, 124–128. [Google Scholar] [CrossRef] [PubMed]
- Muntyanu, A.; Ghazawi, F.M.; Nedjar, H.; Rahme, E.; Alakel, A.; Zubarev, A.; Netchiporouk, E.; Litvinov, I.V. Non-Melanoma Skin Cancer Distribution in the Russian Federation. Dermatology 2020, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Muntyanu, A.; Savin, E.; Ghazawi, F.M.; Alakel, A.; Zubarev, A.; Litvinov, I.V. Geographic Variations in Cutaneous Melanoma Distribution in the Russian Federation. Dermatology 2020, 236, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Roy, S.F.; Ghazawi, F.M.; Le, M.; Lagacé, F.; Roy, C.F.; Rahme, E.; Savin, E.; Zubarev, A.; Sasseville, D.; Popradi, G.; et al. Epidemiology of adult and pediatric Burkitt lymphoma in Canada: Sequelae of the HIV epidemic. Curr. Oncol. 2019, 27, 83–89. [Google Scholar] [CrossRef]
- Fradet, Y.; Klotz, L.; Trachtenberg, J.; Zlotta, A. The burden of prostate cancer in Canada. Can. Urol. Assoc. J. 2013, 3, S92–S100. [Google Scholar] [CrossRef] [Green Version]
- Brawley, O.W. Trends in Prostate Cancer in the United States. J. Natl. Cancer Inst. Monogr. 2012, 2012, 152–156. [Google Scholar] [CrossRef] [Green Version]
- Prostate Cancer Statistics. Canadian Cancer Society 2018. Available online: https://prostatecancerfree.org/prostate-cancer/?gclid=EAIaIQobChMIj8Oau6f07gIVVsvICh3GkwC9EAAYASAAEgJ4-vD_BwE (accessed on 1 July 2020).
- Feletto, E.; Bang, A.; Cole-Clark, D.; Chalasani, V.; Rasiah, K.; Smith, D.P. An examination of prostate cancer trends in Australia, England, Canada and USA: Is the Australian death rate too high? World J. Urol. 2015, 33, 1677–1687. [Google Scholar] [CrossRef] [Green Version]
- Neutel, C.I.; Gao, R.-N.; Blood, P.A.; Gaudette, L.A. The Changing Age Distribution of Prostate Cancer in Canada. Can. J. Public Health 2007, 98, 60–64. [Google Scholar] [CrossRef] [PubMed]
- Levy, I. Prostate cancer: The epidemiologic perspective. Can. J. Oncol. 1994, 4, 4–7. [Google Scholar] [PubMed]
- Tchir, D.; Farag, M.; Szafron, M. Prostate specific antigen (PSA) screening rates and factors associated with screening in Eastern Canadian men: Findings from cross-sectional survey data. Can. Urol. Assoc. J. 2020, 14, E319–E327. [Google Scholar] [CrossRef] [PubMed]
- Leblanc, A.G.; Demers, A.; Shaw, A. Recent trends in prostate cancer in Canada. Public Health Rep. (1896–1970) 2019, 30, 12–17. [Google Scholar]
- Dickinson, J.; Shane, A.; Tonelli, M.; Gorber, S.C.; Joffres, M.; Singh, H.; Bell, N. Trends in prostate cancer incidence and mortality in Canada during the era of prostate-specific antigen screening. CMAJ Open 2016, 4, E73–E79. [Google Scholar] [CrossRef] [Green Version]
- Barry, M.J.; Simmons, L.H. Prevention of Prostate Cancer Morbidity and Mortality: Primary Prevention and Early Detection. Med. Clin. N. Am. 2017, 101, 787–806. [Google Scholar] [CrossRef] [PubMed]
- Cheng, I.; Witte, J.S.; McClure, L.A.; Shema, S.J.; Cockburn, M.G.; John, E.M.; Clarke, C.A. Socioeconomic status and prostate cancer incidence and mortality rates among the diverse population of California. Cancer Causes Control 2009, 20, 1431–1440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adler, N.E.; Newman, K. Socioeconomic Disparities in Health: Pathways and Policies. Health Aff. 2002, 21, 60–76. [Google Scholar] [CrossRef] [PubMed]
- Watson, M.; Grande, D.; Radhakrishnan, A.; Mitra, N.; Ward, K.R.; Pollack, C.E. Racial Differences in Prostate Cancer Treatment: The Role of Socioeconomic Status. Ethn. Dis. 2017, 27, 201–208. [Google Scholar] [CrossRef]
- Weiner, A.B.; Matulewicz, R.S.; Tosoian, J.J.; Feinglass, J.M.; Schaeffer, E.M. The effect of socioeconomic status, race, and insurance type on newly diagnosed metastatic prostate cancer in the United States (2004–2013). Urol. Oncol. Semin. Orig. Investig. 2018, 36, 91.e1–91.e6. [Google Scholar] [CrossRef]
- Debre, B.; Geraud, M.; Flam, T.; Steg, A. Epidemiology of Prostatic Cancer. J. Int. Med Res. 1990, 18, 3–7. [Google Scholar] [CrossRef] [PubMed]
- Whittemore, A.S.; Kolonel, L.N.; Wu, A.H.; John, E.M.; Gallagher, R.P.; Howe, G.R.; Burch, J.D.; Hankin, J.; Dreon, D.M.; West, D.W.; et al. Prostate Cancer in Relation to Diet, Physical Activity, and Body Size in Blacks, Whites, and Asians in the United States and Canada. J. Natl. Cancer Inst. 1995, 87, 652–661. [Google Scholar] [CrossRef]
- McDavid, K.; Lee, J.; Fulton, J.P.; Tonita, J.; Thompson, T.D. Prostate cancer incidence and mortality rates and trends in the United States and Canada. Public Health Rep. 2004, 119, 174–186. [Google Scholar] [CrossRef] [PubMed]
- Sanders, C.M.; Saltzstein, S.L.; Schultzel, M.M.; Nguyen, D.H.; Stafford, H.S.; Sadler, G.R. Understanding the limits of large datasets. J. Cancer Educ. 2012, 27, 664–669. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| ICD-O3 Code | Neoplasm | Count † (%) | Mean Age ± SD |
|---|---|---|---|
| 8140 | Adenocarcinoma NOS | 327,195 (99.81) | 68.50 ± 9.15 |
| 8201 | Cribriform carcinoma NOS | 90 (0.03) | 70.33 ± 7.88 |
| 8260 | Papillary adenocarcinoma NOS | 65 (0.02) | 72.92 ± 9.17 |
| Papillary renal cell carcinoma | |||
| Papillary carcinoma of thyroid | |||
| 8310 | Clear cell adenocarcinoma NOS | 100 (0.03) | 68.36 ± 8.27 |
| Clear cell adenocarcinoma, mesonephroid | |||
| 8480 | Mucinous adenocarcinoma | 225 (0.07) | 65.25 ± 10.61 |
| Pseudomyxoma peritonei with unknown primary site | |||
| 8490 | Signet ring cell carcinoma | 90 (0.03) | 70.02 ± 9.51 |
| 8560 | Adenosquamous carcinoma | 20 (0.01) | 73.55 ± 8.54 |
| 8574 | Adenocarcinoma with neuroendocrine differentiation | 25 (0.01) | 68.15 ± 10.93 |
| - | Total | 327,810 (100) | 78.4 ± 9.19 |
| Province/Territory | Male Population (Rounded to 1000) | Crude Incidence Rate (95% CI) | Age-Adjusted Incidence Rate (95% CI) | Crude Mortality Rate (95% CI) | Age-Adjusted Mortality Rate (95% CI) |
|---|---|---|---|---|---|
| Alberta | 1,573,000 | 105.78 (104.62–195.95) | 118.68 (117.45–118.87) | 21.08 (20.56–21.12) | 23.70 (23.15–23.74) |
| British Columbia | 2,007,000 | 134.18 (133.02–134.36) | 118.84 (117.74–119.00) | 24.61 (24.12–24.65) | 20.35 (19.90–20.38) |
| Manitoba | 575,000 | 120.41 (118.36–129.73) | 116.73 (114.69–117.04) | 30.16 (29.14–31.24) | 26.13 (25.17–26.20) |
| New Brunswick | 370,000 | 155.26 (152.36–155.77) | 140.03 (137.24–140.50) | 28.59 (27.36–28.69) | 24.62 (23.46–24.71) |
| Newfoundland and Labrador | 265,000 | 111.72 (108.82–112.16) | 103.63 (100.78–104.04) | 25.22 (23.86–25.33) | 23.86 (22.51–23.97) |
| Nova Scotia | 457,000 | 141.43 (138.94–141.84) | 126.13 (123.74–126.51) | 29.31 (28.18–29.43) | 24.92 (23.87–25.01) |
| Ontario | 5,853,000 | 115.85 (115.22–115.95) | 111.10 (110.48–111.19) | 23.19 (22.90–23.24) | 21.48 (21.21–21.50) |
| Prince Edward Island | 67,000 | 165.75 (158.75–167.46) | 146.76 (140.15–147.94) | 31.82 (28.79–32.12) | 26.66 (23.88–26.92) |
| Quebec | 3,676,000 | 84.56 (83.88–84.65) | 77.63 (76.98–77.71) | 21.04 (20.70–21.96) | 19.57 (19.24–19.59) |
| Saskatchewan | 502,000 | 133.10 (130.79–133.48) | 123.45 (121.20–123.80) | 40.78 (39.51–45.93) | 31.89 (30.75–31.98) |
| Northwest Territories | 22,000 | 37.08 (31.47–37.74) | 63.95 (56.78–64.92) | 9.57 (6.84–9.86) | 21.14 (17.11–21.56) |
| Nunavut | 15,000 | 8.77 (5.68–9.15) | 21.38 (16.37–21.96) | - | - |
| Yukon | 16,000 | 59.21 (50.88–67.36) | 73.11 (63.73–74.49) | 11.51 (8.02–11.92) | 17.89 (13.41–18.40) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lagacé, F.; Ghazawi, F.M.; Le, M.; Savin, E.; Zubarev, A.; Powell, M.; Moreau, L.; Sasseville, D.; Popa, I.; Litvinov, I.V. Incidence and Mortality of Prostate Cancer in Canada during 1992–2010. Curr. Oncol. 2021, 28, 978-990. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol28010096
Lagacé F, Ghazawi FM, Le M, Savin E, Zubarev A, Powell M, Moreau L, Sasseville D, Popa I, Litvinov IV. Incidence and Mortality of Prostate Cancer in Canada during 1992–2010. Current Oncology. 2021; 28(1):978-990. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol28010096
Chicago/Turabian StyleLagacé, François, Feras M. Ghazawi, Michelle Le, Evgeny Savin, Andrei Zubarev, Mathieu Powell, Linda Moreau, Denis Sasseville, Ioana Popa, and Ivan V. Litvinov. 2021. "Incidence and Mortality of Prostate Cancer in Canada during 1992–2010" Current Oncology 28, no. 1: 978-990. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol28010096