Improvement of EGFR Testing over the Last Decade and Impact of Delaying TKI Initiation

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Population
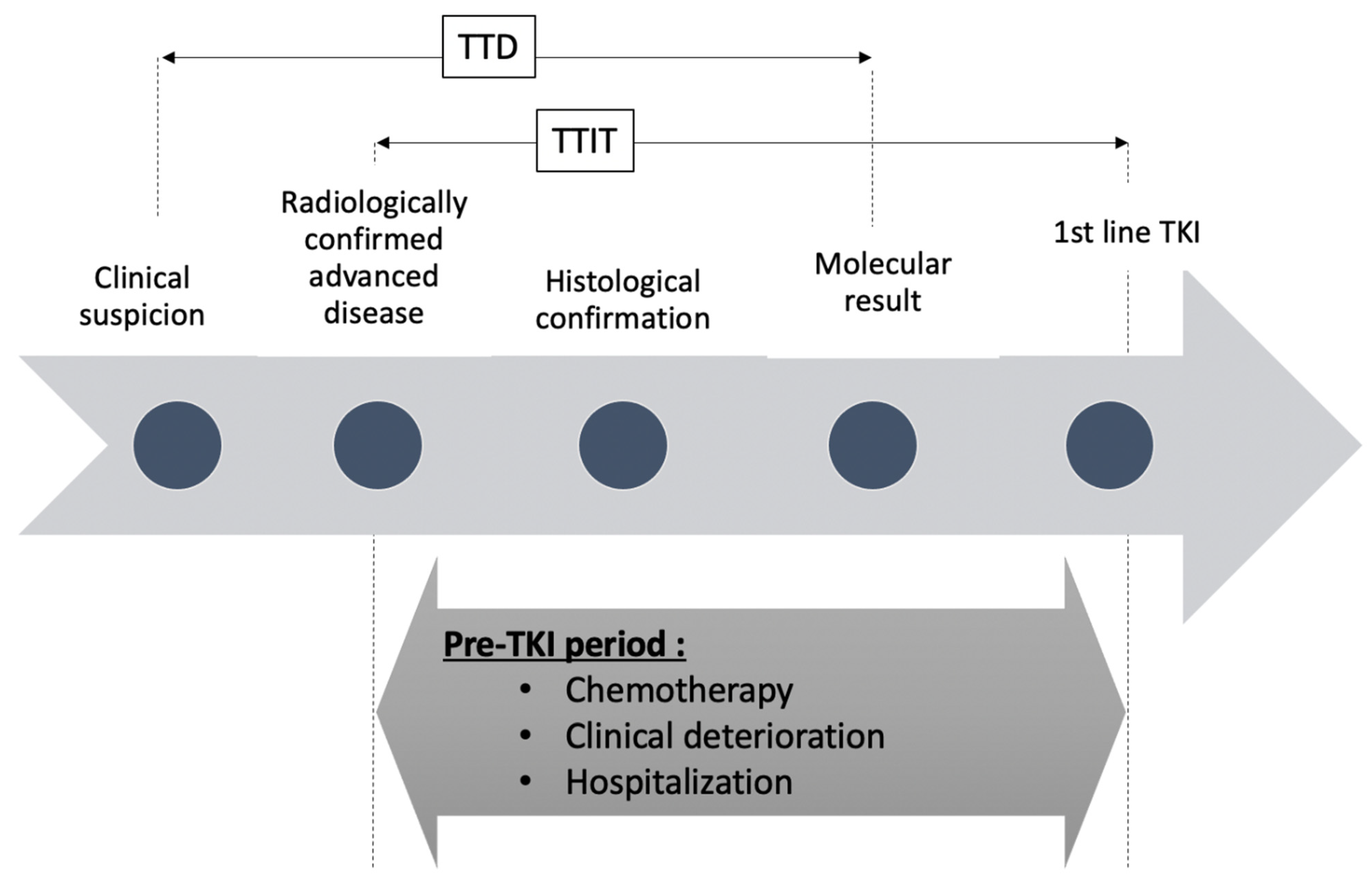
2.2. Endpoints
2.3. Statistical Analysis
3. Results
3.1. General Outcomes
3.2. Interval before the Initiation of a TKI
3.3. Survival Impact
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sharma, S.V.; Bell, D.W.; Settleman, J.; Haber, D.A. Epidermal growth factor receptor mutations in lung cancer. Nat. Rev. Cancer 2007, 7, 169–181. [Google Scholar] [CrossRef]
- Varghese, A.M.; Zakowski, M.F.; Yu, H.A.; Won, H.H.; Riely, G.J.; Krug, L.M.; Kris, M.G.; Rekhtman, N.; Ladanyi, M.; Wang, L.; et al. Small-Cell Lung Cancers in Patients Who Never Smoked Cigarettes. J. Thorac. Oncol. 2014, 9, 892–896. [Google Scholar] [CrossRef] [Green Version]
- Shi, Y.; Au, J.S.-K.; Thongprasert, S.; Srinivasan, S.; Tsai, C.-M.; Khoa, M.T.; Heeroma, K.; Itoh, Y.; Cornelio, G.; Yang, P.-C. A Prospective, Molecular Epidemiology Study of EGFR Mutations in Asian Patients with Advanced Non–Small-Cell Lung Cancer of Adenocarcinoma Histology (PIONEER). J. Thorac. Oncol. 2014, 9, 154–162. [Google Scholar] [CrossRef] [Green Version]
- Ellis, P.M.; Blais, N.; Soulieres, D.; Ionescu, D.N.; Kashyap, M.; Liu, G.; Melosky, B.; Reiman, T.; Romeo, P.; Shepherd, F.A.; et al. A Systematic Review and Canadian Consensus Recommendations on the Use of Biomarkers in the Treatment of Non-small Cell Lung Cancer. J. Thorac. Oncol. 2011, 6, 1379–1391. [Google Scholar] [CrossRef] [Green Version]
- Rosell, R.; Carcereny, E.; Gervais, R.; Vergnenegre, A.; Massuti, B.; Felip, E.; Palmero, R.; Garcia-Gomez, R.; Pallares, C.; Sanchez, J.M.; et al. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): A multicentre, open-label, randomised phase 3 trial. Lancet Oncol. 2012, 13, 239–246. [Google Scholar] [CrossRef]
- Zhou, C.; Wu, Y.L.; Chen, G.; Feng, J.; Liu, X.-Q.; Wang, C.; Zhang, S.; Wang, J.; Zhou, S.; Ren, S.; et al. Final overall survival results from a randomised, phase III study of erlotinib versus chemotherapy as first-line treatment of EGFR mutation-positive advanced non-small-cell lung cancer (OPTIMAL, CTONG-0802). Ann. Oncol. 2015, 26, 1877–1883. [Google Scholar] [CrossRef]
- Fukuoka, M.; Wu, Y.-L.; Thongprasert, S.; Sunpaweravong, P.; Leong, S.-S.; Sriuranpong, V.; Chao, T.-Y.; Nakagawa, K.; Chu, D.-T.; Saijo, N.; et al. Biomarker Analyses and Final Overall Survival Results from a Phase III, Randomized, Open-Label, First-Line Study of Gefitinib Versus Carboplatin/Paclitaxel in Clinically Selected Patients With Advanced Non–Small-Cell Lung Cancer in Asia (IPASS). J. Clin. Oncol. 2011, 29, 2866–2874. [Google Scholar] [CrossRef]
- Paz-Ares, L.; Tan, E.-H.; O’Byrne, K.; Zhang, L.; Hirsh, V.; Boyer, M.; Yang, J.-H.; Mok, T.; Lee, K.H.; Lu, S.; et al. Afatinib versus gefitinib in patients with EGFR mutation-positive advanced non-small-cell lung cancer: Overall survival data from the phase IIb LUX-Lung 7 trial. Ann. Oncol. 2017, 28, 270–277. [Google Scholar] [CrossRef]
- Wu, Y.-L.; Cheng, Y.; Zhou, X.; Lee, K.H.; Nakagawa, K.; Niho, S.; Tsuji, F.; Linke, R.; Rosell, R.; Corral, J.; et al. Dacomitinib versus gefitinib as first-line treatment for patients with EGFR-mutation-positive non-small-cell lung cancer (ARCHER 1050): A randomised, open-label, phase 3 trial. Lancet Oncol. 2017, 18, 1454–1466. [Google Scholar] [CrossRef]
- Soria, J.-C.; Ohe, Y.; Vansteenkiste, J.; Reungwetwattana, T.; Chewaskulyong, B.; Lee, K.H.; Dechaphunkul, A.; Imamura, F.; Nogami, N.; Kurata, T.; et al. Osimertinib in UntreatedEGFR-Mutated Advanced Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 378, 113–125. [Google Scholar] [CrossRef]
- Ramalingam, S.S.; Vansteenkiste, J.; Planchard, D.; Cho, B.C.; Gray, J.E.; Ohe, Y.; Zhou, C.; Reungwetwattana, T.; Cheng, Y.; Chewaskulyong, B.; et al. Overall Survival with Osimertinib in Untreated, EGFR-Mutated Advanced NSCLC. N. Engl. J. Med. 2020, 382, 41–50. [Google Scholar] [CrossRef]
- Mazieres, J.; Drilon, A.; Lusque, A.; Mhanna, L.; Cortot, A.; Mezquita, L.; Thai, A.; Mascaux, C.; Couraud, S.; Veillon, R.; et al. Immune checkpoint inhibitors for patients with advanced lung cancer and oncogenic driver alterations: Results from the IMMUNOTARGET registry. Ann. Oncol. 2019, 30, 1321–1328. [Google Scholar] [CrossRef]
- Noronha, V.; Joshi, A.; Patil, V.M.; Chougule, A.; Mahajan, A.; Janu, A.; Purandare, N.; Kumar, R.; More, S.; Goud, S.; et al. Phase III randomized trial comparing gefitinib to gefitinib with pemetrexed-carboplatin chemotherapy in patients with advanced untreated EGFR mutant non-small cell lung cancer (gef vs. gef+C). J. Clin. Oncol. 2019, 37, 9001. [Google Scholar] [CrossRef]
- Saito, H.; Fukuhara, T.; Furuya, N.; Watanabe, K.; Sugawara, S.; Iwasawa, S.; Tsunezuka, Y.; Yamaguchi, O.; Okada, M.; Yoshimori, K.; et al. Erlotinib plus bevacizumab versus erlotinib alone in patients with EGFR-positive advanced non-squamous non-small-cell lung cancer (NEJ026): Interim analysis of an open-label, randomised, multicentre, phase 3 trial. Lancet Oncol. 2019, 20, 625–635. [Google Scholar] [CrossRef]
- Soria, J.-C.; Wu, Y.-L.; Nakagawa, K.; Kim, S.-W.; Yang, J.-J.; Ahn, M.-J.; Wang, J.; Yang, J.C.-H.; Lu, Y.; Atagi, S.; et al. Gefitinib plus chemotherapy versus placebo plus chemotherapy in EGFR-mutation-positive non-small-cell lung cancer after progression on first-line gefitinib (IMPRESS): A phase 3 randomised trial. Lancet Oncol. 2015, 16, 990–998. [Google Scholar] [CrossRef]
- Mok, T.S.; Kim, S.-W.; Wu, Y.-L.; Nakagawa, K.; Yang, J.-J.; Ahn, M.-J.; Wang, J.; Yang, J.C.-H.; Lu, Y.; Atagi, S.; et al. Gefitinib Plus Chemotherapy Versus Chemotherapy in Epidermal Growth Factor Receptor Mutation–Positive Non–Small-Cell Lung Cancer Resistant to First-Line Gefitinib (IMPRESS): Overall Survival and Biomarker Analyses. J. Clin. Oncol. 2017, 35, 4027–4034. [Google Scholar] [CrossRef]
- Dagogo-Jack, I.; Azzolli, C.G.; Fintelmann, F.; Mino-Kenudson, M.; Farago, A.F.; Gainor, J.F.; Jiang, G.; Piotrowska, Z.; Heist, R.S.; Lennes, I.T.; et al. Clinical Utility of Rapid EGFR Genotyping in Advanced Lung Cancer. JCO Precis. Oncol. 2018, 2018, 1–13. [Google Scholar] [CrossRef]
- Rosell, R.; Moran, T.; Queralt, C.; Porta, R.; Cardenal, F.; Camps, C.; Majem, M.; Lopez-Vivanco, G.; Isla, D.; Provencio, M.; et al. Screening for Epidermal Growth Factor Receptor Mutations in Lung Cancer. N. Engl. J. Med. 2009, 361, 958–967. [Google Scholar] [CrossRef] [Green Version]
- Ettinger, D.S.; Aisner, D.L.; Wood, D.E.; Akerley, W.; Bauman, J.; Chang, J.Y.; Chirieac, L.R.; D’Amico, T.A.; Dilling, T.J.; Dobelbower, M.; et al. NCCN Guidelines Insights: Non–Small Cell Lung Cancer, Version 5.2018. J. Natl. Compr. Cancer Netw. 2018, 16, 807–821. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kelly, K.; Altorki, N.K.; Eberhardt, W.E.E.; O’Brien, M.E.; Spigel, D.R.; Crinò, L.; Tsai, C.-M.; Kim, J.-H.; Cho, E.K.; Hoffman, P.C.; et al. Adjuvant Erlotinib Versus Placebo in Patients with Stage IB-IIIA Non–Small-Cell Lung Cancer (RADIANT): A Randomized, Double-Blind, Phase III Trial. J. Clin. Oncol. 2015, 33, 4007–4014. [Google Scholar] [CrossRef]
- Zhong, W.-Z.; Wang, Q.; Mao, W.-M.; Xu, S.-T.; Wu, L.; Shen, Y.; Liu, Y.-Y.; Chen, C.; Cheng, Y.; Xu, L.; et al. Gefitinib versus vinorelbine plus cisplatin as adjuvant treatment for stage II–IIIA (N1–N2) EGFR-mutant NSCLC (ADJUVANT/CTONG1104): A randomised, open-label, phase 3 study. Lancet Oncol. 2018, 19, 139–148. [Google Scholar] [CrossRef]
- Mitsudomi, T.; Yatabe, Y. Epidermal growth factor receptor in relation to tumor development: EGFR gene and cancer. FEBS J. 2010, 277, 301–308. [Google Scholar] [CrossRef]
- O’Kane, G.M.; Bradbury, P.A.; Feld, R.; Leighl, N.B.; Liu, G.; Pisters, K.-M.; Kamel-Reid, S.; Tsao, M.S.; Shepherd, F.A. Uncommon EGFR mutations in advanced non-small cell lung cancer. Lung Cancer 2017, 109, 137–144. [Google Scholar] [CrossRef]
- Samson, P.; Patel, A.; Garrett, T.; Crabtree, T.; Kreisel, D.; Krupnick, A.S.; Patterson, G.A.; Broderick, S.; Meyers, B.F.; Puri, V. Effects of Delayed Surgical Resection on Short-Term and Long-Term Outcomes in Clinical Stage I Non-Small Cell Lung Cancer. Ann. Thorac. Surg. 2015, 99, 1906–1913. [Google Scholar] [CrossRef] [Green Version]
- Gomez, D.R.; Liao, K.-P.; Swisher, S.G.; Blumenschein, G.R.; Erasmus, J.J.; Buchholz, T.A.; Giordano, S.H.; Smith, B.D. Time to treatment as a quality metric in lung cancer: Staging studies, time to treatment, and patient survival. Radiother. Oncol. 2015, 115, 257–263. [Google Scholar] [CrossRef]
- Jacobsen, M.M.; Silverstein, S.C.; Quinn, M.; Waterston, L.B.; Thomas, C.A.; Benneyan, J.C.; Han, P.K. Timeliness of access to lung cancer diagnosis and treatment: A scoping literature review. Lung Cancer 2017, 112, 156–164. [Google Scholar] [CrossRef]
- Kate, S.; Chougule, A.; Joshi, A.; Noronha, V.; Patil, V.; Dusane, R.; Solanki, L.; Tiwrekar, P.; Trivedi, V.; Prabhash, K. Outcome of uncommon EGFR mutation positive newly diagnosed advanced non-small cell lung cancer patients: A single center retrospective analysis. Lung Cancer Targets Ther. 2019, 10, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Shi, J.; Yang, H.; Jiang, T.; Li, X.; Zhao, C.; Zhang, L.; Zhao, S.; Liu, X.; Jia, Y.; Wang, Y.; et al. Uncommon EGFR mutations in a cohort of Chinese NSCLC patients and outcomes of first-line EGFR-TKIs and platinum-based chemotherapy. Chin. J. Cancer Res. 2017, 29, 543–552. [Google Scholar] [CrossRef]
- Yang, J.C.-H.; Sequist, L.V.; Geater, S.L.; Tsai, C.-M.; Mok, T.S.K.; Schuler, M.; Yamamoto, N.; Yu, C.-J.; I Ou, S.-H.; Zhou, C.; et al. Clinical activity of afatinib in patients with advanced non-small-cell lung cancer harbouring uncommon EGFR mutations: A combined post-hoc analysis of LUX-Lung 2, LUX-Lung 3, and LUX-Lung 6. Lancet Oncol. 2015, 16, 830–838. [Google Scholar] [CrossRef]
- Wu, J.-Y.; Yu, C.-J.; Chang, Y.-C.; Yang, C.-H.; Shih, J.-Y.; Yang, P.-C. Effectiveness of Tyrosine Kinase Inhibitors on “Uncommon” Epidermal Growth Factor Receptor Mutations of Unknown Clinical Significance in Non–Small Cell Lung Cancer. Clin. Cancer Res. 2011, 17, 3812–3821. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, I.; Morise, M.; Kodama, Y.; Matsui, A.; Ozawa, N.; Ozone, S.; Goto, D.; Miyazawa, A.; Hase, T.; Hashimoto, N.; et al. Potential for afatinib as an optimal treatment for advanced non-small cell lung carcinoma in patients with uncommon EGFR mutations. Lung Cancer 2019, 127, 169–171. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.-L.; Hirsh, V.; Sequist, L.V.; Hu, C.-P.; Feng, J.; Lu, S.; Huang, Y.; Schuler, M.; Mok, T.; Yamamoto, N.; et al. Does EGFR Mutation Type Influence Patient-Reported Outcomes in Patients with Advanced EGFR Mutation-Positive Non-Small-Cell Lung Cancer? Analysis of Two Large, Phase III Studies Comparing Afatinib with Chemotherapy (LUX-Lung 3 and LUX-Lung 6). Patient Patient Cent. Outcomes Res. 2017, 11, 131–141. [Google Scholar] [CrossRef] [Green Version]
- Cho, J.H.; Lim, S.H.; An, H.J.; Kim, K.H.; Park, K.U.; Kang, E.J.; Choi, Y.H.; Ahn, M.S.; Lee, M.H.; Sun, J.-M.; et al. Osimertinib for Patients with Non–Small-Cell Lung Cancer Harboring Uncommon EGFR Mutations: A Multicenter, Open-Label, Phase II Trial (KCSG-LU15-09). J. Clin. Oncol. 2020, 38, 488–495. [Google Scholar] [CrossRef] [PubMed]
- Arcila, M.E.; Nafa, K.; Chaft, J.E.; Rekhtman, N.; Lau, C.; Reva, B.A.; Zakowski, M.F.; Kris, M.G.; Ladanyi, M. EGFR Exon 20 Insertion Mutations in Lung Adenocarcinomas: Prevalence, Molecular Heterogeneity, and Clinicopathologic Characteristics. Mol. Cancer Ther. 2013, 12, 220–229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kobayashi, Y.; Mitsudomi, T. Not all epidermal growth factor receptor mutations in lung cancer are created equal: Perspectives for individualized treatment strategy. Cancer Sci. 2016, 107, 1179–1186. [Google Scholar] [CrossRef]
- Qian, X.; Liu, J.; Sun, Y.; Wang, M.; Lei, H.; Luo, G.; Liu, X.; Xiong, C.; Liu, D.; Liu, J.; et al. Circulating cell-free DNA has a high degree of specificity to detect exon 19 deletions and the single-point substitution mutation L858R in non-small cell lung cancer. Oncotarget 2016, 7, 29154–29165. [Google Scholar] [CrossRef] [Green Version]
- Qiu, M.; Wang, J.; Xu, Y.; Ding, X.; Li, M.; Jiang, F.; Xu, L.; Yin, R. Circulating Tumor DNA Is Effective for the Detection of EGFR Mutation in Non–Small Cell Lung Cancer: A Meta-analysis. Cancer Epidemiol. Biomark. Prev. 2015, 24, 206–212. [Google Scholar] [CrossRef] [Green Version]
- Reck, M.; Hagiwara, K.; Han, B.; Tjulandin, S.; Grohé, C.; Yokoi, T.; Morabito, A.; Novello, S.; Arriola, E.; Molinier, O.; et al. ctDNA Determination of EGFR Mutation Status in European and Japanese Patients with Advanced NSCLC: The ASSESS Study. J. Thorac. Oncol. 2016, 11, 1682–1689. [Google Scholar] [CrossRef] [Green Version]
- Sacher, A.G.; Paweletz, C.; Dahlberg, S.E.; Alden, R.S.; O’Connell, A.; Feeney, N.; Mach, S.L.; Jänne, P.A.; Oxnard, G.R. Prospective Validation of Rapid Plasma Genotyping for the Detection of EGFR and KRAS Mutations in Advanced Lung Cancer. JAMA Oncol. 2016, 2, 1014–1022. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Clinical Characteristics | N = 102 |
|---|---|
| Age-Yr | 62.1 (21.8–91.5) |
| Sex | |
| Male | 32 (31.4%) |
| Female | 70 (68.6%) |
| Smoking status | |
| Current/former | 44 (43.1%) |
| Never/light | 54 (52.9%) |
| Unknown | 4 (3.9%) |
| Stage at diagnosis | |
| I-II | 19 (18.6%) |
| IIIA/C | 16 (15.7%) |
| IV | 66 (64.7%) |
| unknown | 1 (1%) |
| Histologic subtype | |
| Adenocarcinoma | 98 (96.1%) |
| Squamous | 2 (1.9%) |
| Other | 2 (1.9%) |
| EGFR mutation | |
| Exon 19 | 45 (44.1%) |
| Exon 21 | 46 (45.1%) |
| Others | 11 (10.8%) |
| Exon 18 | 7 (6.9%) |
| Exon 20 | 3 (2.9%) |
| Other | 1 (1%) |
| 1st line TKI | |
| Erlotinib | 16 (15.7%) |
| Gefitinib | 53 (52.0%) |
| Afatinib | 20 (19.6%) |
| Osimertinib | 3 (2.9%) |
| None | 10 (9.8%) |
| Parameters | Mean (Days) | Range (Days) |
|---|---|---|
| Time between 1st biopsy and histological confirmation | 24.2 | 1–190 |
| 2006–2010 (n = 14) | 31.5 | 3–147 |
| 2011–2013 (n = 28) | 42.4 | 4–190 |
| 2014–2016 (n = 32) | 18.2 | 1–72 |
| 2017–2019 (n = 28) | 9.1 | 2–20 |
| Time between clinical suspicion of cancer and EGFR result (TTD) | 342.9 | 13–3003 |
| 2006–2010 (n = 14) | 1730.3 | 85–3003 |
| 2011–2013 (n = 28) | 438.6 | 13–2056 |
| 2014–2016 (n = 32) | 187.6 | 14–1058 |
| 2017–2019 (n = 28) | 48.4 | 17–119 |
| For primary metastatic disease: Time between clinical suspicion and EGFR result | 140.4 | 13–3003 |
| 2006–2010 (n = 2) | 1542.8 | 85–3003 |
| 2011–2013 (n = 17) | 190.6 | 13–1204 |
| 2014–2016 (n = 22) | 78.7 | 14–451 |
| 2017–2019 (n = 25) | 48.4 | 17–119 |
| Time between confirmed advanced disease and 1st day TKI (TTIT) | 173.6 | 1–2431 |
| 2006–2010 (n = 14) | 402.3 | 40–2431 |
| 2011–2013 (n = 28) | 199.7 | 1–1256 |
| 2014–2016 (n = 32) | 148.2 | 2–1046 |
| 2017–2019 (n = 28) | 81.7 | 9–250 |
| For primary metastatic disease: Time between EGFR result and 1st day TKI | 6.1 | −1035–404 |
| 1st Line Treatment | N = 102 |
|---|---|
| Platinum-based chemotherapy | 23 (22.5%) |
| 2006–2010 (n = 14) | 6 (42.9%) |
| 2011–2013 (n = 28) | 8 (28.6%) |
| 2014–2016 (n = 32) | 4 (12.5%) |
| 2017–2019 (n = 28) | 5 (17.8%) |
| TKI | 71 (69.6%) |
| Other | 1 (1%) |
| No treatment | 7 (6.9%) (3 refused, 4 unfit) |
| Pre-TKI Complications | Number of Patients n = 101 | Symptoms | Number of Patients | Duration Median (Range) | |
|---|---|---|---|---|---|
| Clinical deterioration (n = 29) | Symptomatic disease | 20 | PS deterioration | 17 | |
| Dyspnea | 8 | ||||
| Pain | 6 | ||||
| Cough | 1 | ||||
| Pleural effusion | 6 | ||||
| Pericardial effusion | 1 | ||||
| Other causes | 9 | Chemotherapy severe adverse events | 5 | ||
| Anxiety | 2 | ||||
| Pulmonary embolism | 1 | ||||
| Tuberculosis | 1 | ||||
| Hospitalization | 16 | Pleural effusion | 3 | 17 days (1–30) | |
| Fatigue | 8 | 21 days (1–60) | |||
| Dyspnea | 3 | 17 days (1–30) | |||
| Pain | 3 | 1 day (1–21) | |||
| Pulmonary embolism | 1 | 3 days | |||
| Tuberculosis | 1 | 30 days | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blanc-Durand, F.; Florescu, M.; Tehfe, M.; Routy, B.; Alameddine, R.; Tran-Thanh, D.; Blais, N. Improvement of EGFR Testing over the Last Decade and Impact of Delaying TKI Initiation. Curr. Oncol. 2021, 28, 1045-1055. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol28020102
Blanc-Durand F, Florescu M, Tehfe M, Routy B, Alameddine R, Tran-Thanh D, Blais N. Improvement of EGFR Testing over the Last Decade and Impact of Delaying TKI Initiation. Current Oncology. 2021; 28(2):1045-1055. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol28020102
Chicago/Turabian StyleBlanc-Durand, Félix, Marie Florescu, Mustapha Tehfe, Bertrand Routy, Raafat Alameddine, Danh Tran-Thanh, and Normand Blais. 2021. "Improvement of EGFR Testing over the Last Decade and Impact of Delaying TKI Initiation" Current Oncology 28, no. 2: 1045-1055. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol28020102