Clinician Perspectives of COVID-19-Related Cancer Drug Funding Measures in Ontario

 ,
,
Abstract
:1. Introduction
2. Experimental Section
Methods
3. Results
3.1. Respondent Characteristics
3.2. The Majority of Clinicians Modified Treatment Plans for Their Cancer Patients during the Covid-19 Pandemic
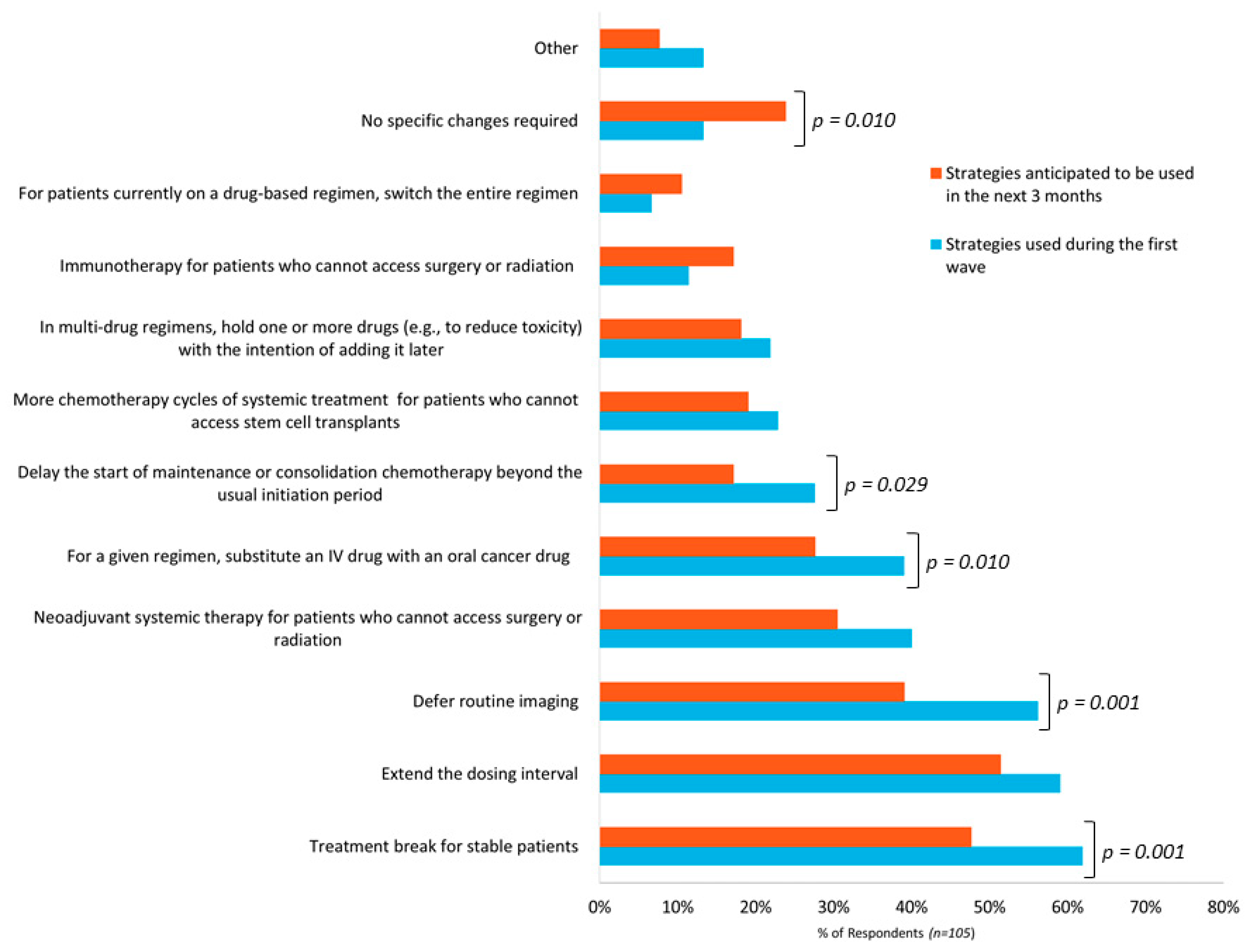
3.3. Clinicians Are Using Broad Range of Management Strategies and Will Continue to Do so in the Coming Months
3.4. Clinicians Require on-Going Support from the Cancer System for Optimal Patient Management during the Pandemic
- Flexibility in drug funding policy measures is required.
- Timely and efficient access to publicly funded drugs is important, especially for oral cancer drugs.
- Address current drug funding gaps to improve care during the COVID-19 pandemic.
- Addressing pre-pandemic funding issues remains important (e.g., drug wastage, care closer to home, physician shortages).
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Giannakoulis, V.G.; Papoutsi, E.; Siempos, I.I. Effect of Cancer on Clinical Outcomes of Patients With COVID-19: A Meta-Analysis of Patient Data. JCO Glob. Oncol. 2020, 6, 799–808. [Google Scholar] [CrossRef]
- Zhou, Y.; Yang, Q.; Chi, J.; Dong, B.; Lv, W.; Shen, L.; Wang, Y. Comorbidities and the risk of severe or fatal outcomes associated with coronavirus disease 2019: A systematic review and meta-analysis. Int. J. Infect. Dis. IJID Off. Publ. Int. Soc. Infect. Dis. 2020, 99, 47–56. [Google Scholar] [CrossRef]
- Cheruiyot, I.; Kipkorir, V.; Ngure, B.; Misiani, M.; Munguti, J. Cancer is associated with coronavirus disease (COVID-19) severity and mortality: A pooled analysis. Am. J. Emerg. Med. 2020. [Google Scholar] [CrossRef]
- Fillmore, N.R.; La, J.; Szalat, R.E.; Tuck, D.P.; Nguyen, V.; Yildirim, C.; Do, N.V.; Brophy, M.T.; Munshi, N.C. Prevalence and outcome of COVID-19 infection in cancer patients: A national Veterans Affairs study. J. Natl. Cancer Inst. 2020. [Google Scholar] [CrossRef] [PubMed]
- Rogado, J.; Obispo, B.; Pangua, C.; Serrano-Montero, G.; Martín Marino, A.; Pérez-Pérez, M.; López-Alfonso, A.; Gullón, P.; Lara, M.Á. Covid-19 transmission, outcome and associated risk factors in cancer patients at the first month of the pandemic in a Spanish hospital in Madrid. Clin. Transl. Oncol. Off. Publ. Fed. Span. Oncol. Soc. Natl. Cancer Inst. Mex. 2020, 22, 2364–2368. [Google Scholar] [CrossRef]
- Yu, J.; Ouyang, W.; Chua, M.L.K.; Xie, C. SARS-CoV-2 Transmission in Patients With Cancer at a Tertiary Care Hospital in Wuhan, China. JAMA Oncol. 2020, 6, 1108–1110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berghoff, A.S.; Gansterer, M.; Bathke, A.C.; Trutschnig, W.; Hungerländer, P.; Berger, J.M.; Kreminger, J.; Starzer, A.M.; Strassl, R.; Schmidt, R.; et al. SARS-CoV-2 Testing in Patients With Cancer Treated at a Tertiary Care Hospital During the COVID-19 Pandemic. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2020, 38, 3547–3554. [Google Scholar] [CrossRef]
- Shubber, N.; Sheppard, J.; Alradhawi, M.; Ali, Y. The impacts of the novel SARS-CoV-2 outbreak on surgical oncology—A letter to the editor on “The socio-economic implications of the coronavirus and COVID-19 pandemic: A review”. Int. J. Surg. Lond. Engl. 2020, 79, 109–110. [Google Scholar] [CrossRef]
- Biagioli, V.; Belloni, S.; Albanesi, B.; Piredda, A.; Caruso, R. Comment on “The experience on coronavirus disease 2019 and cancer from an oncology hub institution in Milan, Lombardy Region” and reflections from the Italian Association of Oncology Nurses. Eur. J. Cancer Oxf. Engl. 1990 2020, 135, 8–10. [Google Scholar] [CrossRef] [PubMed]
- Jazieh, A.R.; Akbulut, H.; Curigliano, G.; Rogado, A.; Alsharm, A.A.; Razis, E.D.; Mula-Hussain, L.; Errihani, H.; Khattak, A.; De Guzman, R.B.; et al. Impact of the COVID-19 Pandemic on Cancer Care: A Global Collaborative Study. JCO Glob. Oncol. 2020, 6, 1428–1438. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Vahid, S.; Eberg, M.; Milroy, S.; Milkovich, J.; Wright, F.C.; Hunter, A.; Kalladeen, R.; Zanchetta, C.; Wijeysundera, H.C.; et al. Clearing the surgical backlog caused by COVID-19 in Ontario: A time series modelling study. CMAJ Can. Med. Assoc. J. J. Assoc. Medicale Can. 2020, 192, E1347–E1356. [Google Scholar] [CrossRef]
- Koch, C.A.; Lee, G.; Liu, Z.A.; Liu, F.-F.; Fyles, A.; Han, K.; Barry, A.; Croke, J.; Rodin, D.; Helou, J.; et al. Rapid Adaptation of Breast Radiation Therapy Use During the Coronavirus Disease 2019 Pandemic at a Large Academic Cancer Center in Canada. Adv. Radiat. Oncol. 2020, 5, 749–756. [Google Scholar] [CrossRef]
- Ontario Health (Cancer Care Ontario). Pandemic Planning Clinical Guideline for Patients with Cancer. Available online: https://www.ontariohealth.ca/sites/ontariohealth/files/2020-04/Ontario%20Health%20Cancer%20Care%20Ontario%20Pandemic%20Planning%20Clinical%20Guideline%20for%20Patients%20with%20Cancer_10Mar20%20PDF.pdf (accessed on 19 November 2020).
- Ontario Health (Cancer Care Ontario). COVID-19 Supplemental Clinical Guidance for Patients with Cancer. Available online: https://www.cancercareontario.ca/en/guidelines-advice/types-of-cancer/64736 (accessed on 19 November 2020).
- Forbes, L.; Durocher-Allen, L.; Vu, K.; Gallo-Hershberg, D.; Pardhan, A.; Kennedy, K.; Newton, J.; Pitre, L.; Root, D. Regional Models of Care for Systemic Treatment: Standards for the Organization and Delivery of Systemic Treatment. Program in Evidence-Based Care Guideline No.: 12-10 Version 2. Available online: https://www.cancercareontario.ca/en/guidelines-advice/types-of-cancer/60086 (accessed on 10 December 2020).
- BC Cancer COVID-19 Information for Health Professionals in Cancer Care. Available online: http://www.bccancer.bc.ca/health-professionals/clinical-resources/provincial-cancer-clinical-management-guidelines-in-pandemic-situation-(covid-19) (accessed on 19 November 2020).
- American Society of Clinical Oncology (ASCO) COVID-19 Patient Care Information. Available online: https://www.asco.org/asco-coronavirus-information/care-individuals-cancer-during-covid-19 (accessed on 19 November 2020).
- European Society of Medical Oncology (ESMO) Cancer Patient Management during the COVID-19 Pandemic. Available online: https://www.esmo.org/guidelines/cancer-patient-management-during-the-covid-19-pandemic (accessed on 19 November 2020).
- National Health Service. Clinical Guide for the Management of Non-Coronavirus Patients Requiring Acute Treatment: Cancer. Available online: https://www.nice.org.uk/Media/Default/About/COVID-19/Specialty-guides/cancer-and-COVID-19.pdf (accessed on 19 November 2020).
- American Society of Hematology (ASH) COVID-19 Resources. Available online: https://www.hematology.org:443/covid-19 (accessed on 19 November 2020).
- Lalani, A.-K.A.; Chi, K.N.; Heng, D.Y.C.; Kollmannsberger, C.K.; Sridhar, S.S.; Blais, N.; Canil, C.; Czaykowski, P.; Hotte, S.J.; Iqbal, N.; et al. Prioritizing systemic therapies for genitourinary malignancies: Canadian recommendations during the COVID-19 pandemic. Can. Urol. Assoc. J. J. Assoc. Urol. Can. 2020, 14, E154–E158. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network COVID-19 Resources. Available online: https://www.nccn.org/covid-19/ (accessed on 19 November 2020).
- Public Health Ontario Ontario COVID-19 Data Tool. Available online: https://www.publichealthontario.ca/en/Data%and%Analysis/Infectious%Disease/COVID%19%Data%Surveillance/COVID%19%Data%Tool (accessed on 19 November 2020).
- Ministry of Health. Ramping Down Elective Surgeries and Other Non-Emergent Activities. Available online: http://www.health.gov.on.ca/en/pro/programs/publichealth/coronavirus/docs/memos/DM_OH_CMOH_memo_COVID19_elective_surgery_March_15_2020.pdf (accessed on 19 November 2020).
- Ministry of Health. Enhanced Public Health Measures for COVID-19. Available online: http://www.health.gov.on.ca/en/pro/programs/publichealth/coronavirus/docs/memos/CMOH_Memo_Enhanced_Public_Health_Measures_for_COVID-19_March_12_2020.pdf (accessed on 19 November 2020).
- BC Cancer. Provincial Cancer Therapy Clinical Management Guidelines in Pandemic Situation (COVID-19). Available online: http://www.bccancer.bc.ca/health-professionals-site/Documents/Provincial%20Cancer%20Therapy%20Clinical%20Management%20Guidelines.pdf (accessed on 19 November 2020).
- Ürün, Y.; Hussain, S.A.; Bakouny, Z.; Castellano, D.; Kılıçkap, S.; Morgan, G.; Mckay, R.R.; Pels, K.; Schmidt, A.; Doroshow, D.B.; et al. Survey of the Impact of COVID-19 on Oncologists’ Decision Making in Cancer. JCO Glob. Oncol. 2020, 6, 1248–1257. [Google Scholar] [CrossRef]
- Gill, S.; Hao, D.; Hirte, H.; Campbell, A.; Colwell, B. Impact of COVID-19 on Canadian medical oncologists and cancer care: Canadian Association of Medical Oncologists survey report. Curr. Oncol. 2020, 27, 71–74. [Google Scholar] [CrossRef]
- Simcock, R.; Thomas, T.V.; Estes, C.; Filippi, A.R.; Katz, M.S.; Pereira, I.J.; Saeed, H. COVID-19: Global radiation oncology’s targeted response for pandemic preparedness. Clin. Transl. Radiat. Oncol. 2020, 22, 55–68. [Google Scholar] [CrossRef] [Green Version]
- The Princess Margaret Cancer Foundation Our Impact. Available online: https://thepmcf.ca/Our-Impact/Top-5-Cancer-Research-Centre.aspx (accessed on 19 November 2020).
- Gill, S. CAMO COVID-19 National Survey #2. Canadian Association of Medical Oncology. Available online: https://camo-acom.ca/resources/Documents/CAMO%20survey%202%20COVID-19%20_2020.pdf (accessed on 19 November 2020).
- Government of Ontario. Archived—Reopening Ontario in Stages. Available online: https://www.ontario.ca/page/reopening-ontario-stages#section-1%5C (accessed on 19 November 2020).
- Ministry of Health. COVID-19 Operational Requirements: Health Sector Restart. Available online: http://www.health.gov.on.ca/en/pro/programs/publichealth/coronavirus/docs/operational_requirements_health_sector.pdf (accessed on 19 November 2020).
- Mahase, E. Cancer treatments fall as referrals are slow to recover, show figures. BMJ 2020, 371, m3958. [Google Scholar] [CrossRef]
- Norman, M.L.; Malcolmson, J.; Randall Armel, S.; Gillies, B.; Ou, B.; Thain, E.; McCuaig, J.M.; Kim, R.H. Stay at home: Implementation and impact of virtualising cancer genetic services during COVID-19. J. Med. Genet. 2020. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence. COVID-19 Rapid Guideline: Delivery of Systemic Anticancer Treatments NICE Guideline [NG161]. National Institute for Health and Care Excellence. Available online: https://www.nice.org.uk/guidance/ng161/chapter/modifications-to-usual-service#treatment-breaks (accessed on 19 November 2020).
- National Health Service. NHS England Interim Treatment Options during the COVID19 Pandemic. Available online: https://www.nice.org.uk/guidance/ng161/resources/nhs-england-interim-treatment-options-during-the-covid19-pandemic-pdf-8715724381 (accessed on 21 November 2020).
- de Joode, K.; Dumoulin, D.W.; Engelen, V.; Bloemendal, H.J.; Verheij, M.; van Laarhoven, H.W.M.; Dingemans, I.H.; Dingemans, A.C.; van der Veldt, A.M. Impact of the coronavirus disease 2019 pandemic on cancer treatment: The patients’ perspective. Eur. J. Cancer Oxf. Engl. 1990 2020, 136, 132–139. [Google Scholar] [CrossRef] [PubMed]
- Hanna, T.P.; King, W.D.; Thibodeau, S.; Jalink, M.; Paulin, G.A.; Harvey-Jones, E.; O’Sullivan, D.E.; Booth, C.M.; Sullivan, R.; Aggarwal, A. Mortality due to cancer treatment delay: Systematic review and meta-analysis. BMJ 2020, 371, m4087. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Parameter | Result |
|---|---|
| Sex, n (%) | |
| Female | 48 (45.7%) |
| Male | 52 (49.5%) |
| Not specified | 5 (4.8%) |
| Provider Type, n (%) | |
| Physicians | 79 (75.2%) |
| Medical Oncologist | 50 (47.6%) |
| Hematologist | 14 (13.3%) |
| Urologist | 10 (9.5%) |
| Gynecology Oncologist | 2 (1.9%) |
| Surgical Oncologist | 1 (1.0%) |
| Radiation Oncologist | 1 (1.0%) |
| General Practitioner in Oncology | 1 (1.0%) |
| Pharmacist | 22 (21.0%) |
| Nurse | 3 (2.9%) |
| Other | 1 (1.0%) |
| Years in Practice, n (%) | |
| <5 years | 26 (24.8%) |
| 5–10 years | 19 (18.1%) |
| 10–15 years | 19 (18.1%) |
| >15 years | 41 (39.0%) |
| Parameter | Result |
|---|---|
| Practice Setting, n (%) | |
| Level 1—Regional Cancer Centre (academic) 1 | 43 (41.0%) |
| Level 2—Regional Cancer Centre (academic) | 25 (23.8%) |
| Level 3—Affiliate centre (community) | 29 (27.6%) |
| Level 4—Satellite site 2 (community) | 8 (7.6%) |
| Regions of Ontario, n (%) | |
| 1. Erie St. Clair | 2 (1.9%) |
| 2. South West | 3 (2.9%) |
| 3. Waterloo Wellington | 14 (13.3%) |
| 4. Hamilton Niagara Haldimand Brant | 16 (15.2%) |
| 5. Central West | 4 (3.8%) |
| 6. Mississauga Halton | 3 (2.9%) |
| 7. Toronto Central | 15 (14.3%) |
| 8. Central | 5 (4.8%) |
| 9. Central East | 12 (11.4%) |
| 10. South East | 9 (8.6%) |
| 11. Champlain | 11 (10.5%) |
| 12. North Simcoe Muskoka | 4 (3.8%) |
| 13. North East | 5 (4.8%) |
| 14. North West | 2 (1.9%) |
| Tumor Types Treated, count (%) 3 | |
| All Solid Tumors | 21 (8.4%) |
| All hematology malignancies | 29 (11.6%) |
| Breast | 28 (11.2%) |
| CNS | 4 (1.6%) |
| Genitourinary | 32 (12.8%) |
| Gastrointestinal | 30 (12.0%) |
| Gynecologic | 17 (6.8%) |
| Head and Neck | 7 (2.8%) |
| Lung | 30 (12.0%) |
| Leukemia | 9 (3.6%) |
| Lymphoma | 11 (4.4%) |
| Myeloma | 8 (3.2%) |
| Melanoma | 20 (8.0%) |
| Other | 4 (3.8%) |
| Proportion of Patients Requiring Treatment Plan Changes | No. of Respondents (%) |
|---|---|
| <25% | 57 (54.3%) |
| 25–50% | 35 (33.3%) |
| 50–75% | 8 (7.6%) |
| >75% | 5 (4.8%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Naipaul, R.D.; Mercer, R.E.; Chan, K.K.W.; Yeung, L.; Forbes, L.; Gavura, S. Clinician Perspectives of COVID-19-Related Cancer Drug Funding Measures in Ontario. Curr. Oncol. 2021, 28, 1056-1066. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol28020103
Naipaul RD, Mercer RE, Chan KKW, Yeung L, Forbes L, Gavura S. Clinician Perspectives of COVID-19-Related Cancer Drug Funding Measures in Ontario. Current Oncology. 2021; 28(2):1056-1066. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol28020103
Chicago/Turabian StyleNaipaul, Rohini D., Rebecca E. Mercer, Kelvin K. W. Chan, Lyndee Yeung, Leta Forbes, and Scott Gavura. 2021. "Clinician Perspectives of COVID-19-Related Cancer Drug Funding Measures in Ontario" Current Oncology 28, no. 2: 1056-1066. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol28020103