1. Introduction
Compared to esophageal adenocarcinoma, which is more common in Western countries [
1], ninety percent of esophagus malignancies in Asian countries such as Taiwan are esophageal squamous cell carcinoma (ESCC). In Taiwan, locally advanced disease is the most common condition in newly diagnosed patients with ESCC, owing to delayed diagnosis [
2].
For patients with ESCC, esophagectomy plus the dissection of lymph nodes is one of the gold standard treatment modalities for curative intent. However, patients who are diagnosed with locally advanced ESCC receiving operation alone have unsatisfactory outcomes, with five-year survival below thirty percent [
3,
4,
5,
6,
7]. A multimodality approach, preoperative chemoradiation therapy followed by surgery, has been advocated to downstage the primary tumor, thus increasing resectability rates and reducing micrometastases for a better survival rate [
8,
9,
10]. The first randomized controlled trial of esophageal cancer treated with preoperative chemoradiotherapy was reported in 1992 by Nygaard et al. [
11], and showed that preoperative chemoradiation therapy prolonged overall patient survival. After that literature, several studies [
4,
5,
12,
13] comparing preoperative chemoradiation therapy followed by surgery with surgery alone have shown better survival for preoperative chemoradiotherapy, whereas others have not revealed survival benefits from preoperative chemoradiotherapy compared to surgery alone [
6,
14,
15,
16,
17]. In 2007, Gebski et al. conducted a meta-analysis and showed that significantly better survival was evident for preoperative chemoradiation therapy in patients with ESCC [
18]. In addition, a recent phase III clinical trial [
19], the Chemoradiotherapy for Oesophageal Cancer Followed by Surgery Study (CROSS), demonstrated that preoperative chemoradiotherapy has a significant survival benefit compared to surgery alone. Thus, preoperative chemoradiation therapy followed by surgery has been applied to clinical practice in many hospitals for patients with locally advanced ESCC.
Although the survival benefit has been found in preoperative chemoradiotherapy approaches, there was still a discrepancy in radiotherapy doses in preoperative chemoradiotherapy between several trials. To the best of our knowledge, a study addressing the role of radiotherapy dose of preoperative chemoradiotherapy in patients with locally advanced ESCC is lacking. Diverse radiotherapy doses of preoperative chemoradiotherapy may result in different treatment outcomes and surgical complications. Therefore, the aim of this paper is to review our experience of 141 AJCC 7th stage III ESCC patients receiving preoperative chemoradiation therapy followed by surgery and to evaluate the impact of radiotherapy doses of preoperative chemoradiotherapy on patient treatment outcomes.
4. Discussion
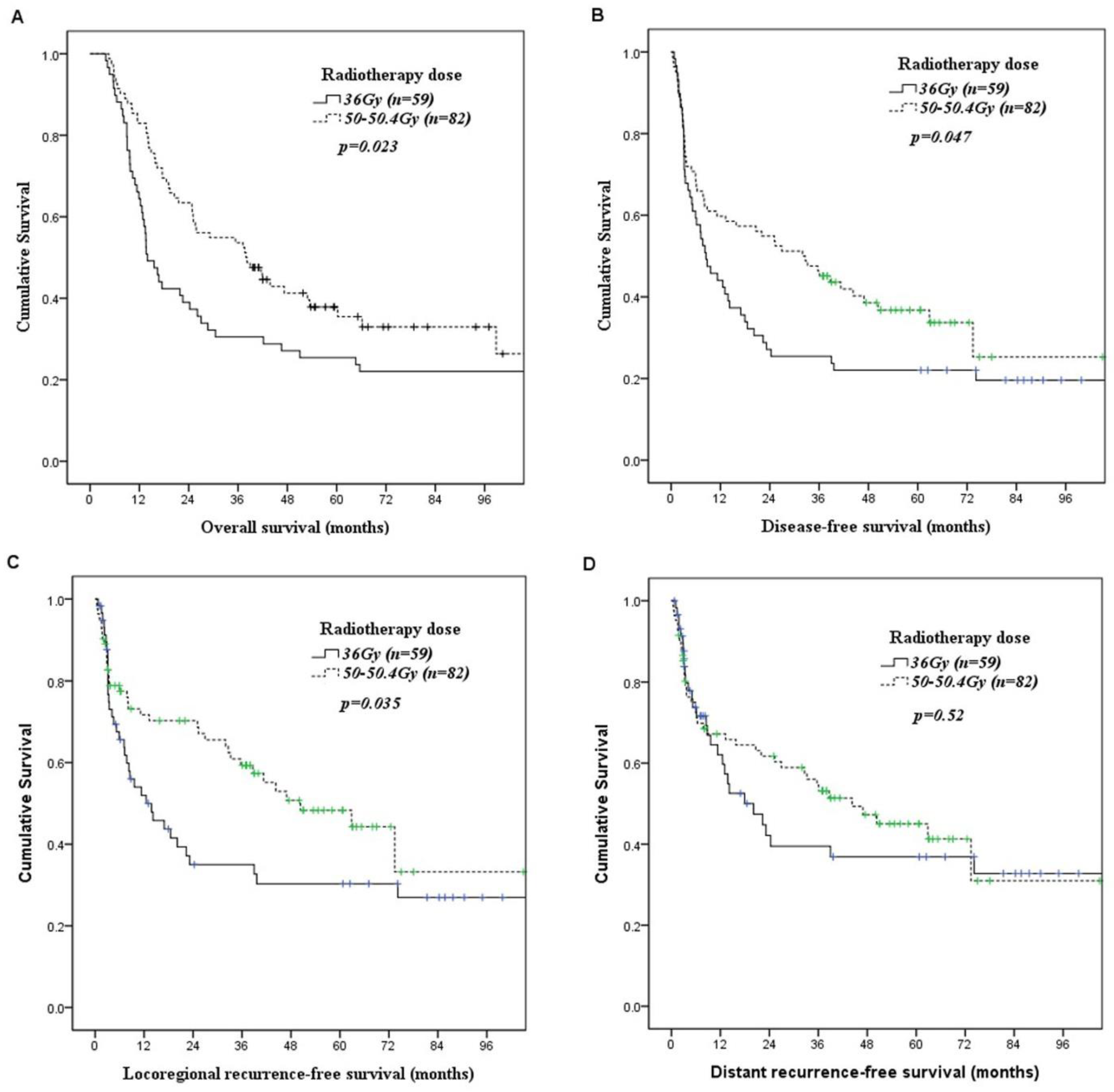
In our study, we found that the three-year overall survival rates were 31% and 54% in patients receiving preoperative chemoradiotherapy with radiotherapy dose 36 Gy and 50–50.4 Gy, respectively (
p = 0.023). Patients receiving higher radiotherapy doses had better overall survival than those receiving lower radiotherapy dose. We suggest that the survival benefit may be ascribed to more patients with pathological complete response after higher radiotherapy dose. Our study found that 12 of the 59 patients with 7th AJCC stage III ESCC receiving 36 Gy preoperative chemoradiotherapy achieved pathological complete response, a pathological compete response rate of only 20%. In the study of Bedenne et al. [
9], pathological complete response was found in 25 (23%) of 110 patients with 6th AJCC T3N0-1M0 esophageal cancer receiving 30 Gy preoperative chemoradiotherapy. Fujita et al. [
13] reported that the pathological complete response rate was 13% in patients with 6th AJCC T4N0-1M0 ESCC receiving 36 Gy preoperative chemoradiotherapy. Burmeister et al. [
14] showed that a pathological complete response was found in 10 (27%) of 37 patients with 6th AJCC T1-3N0-1M0 ESCC receiving 35 Gy preoperative chemoradiotherapy. However, when we applied 50–50.4 Gy preoperative chemoradiotherapy, a pathological complete response was found in 37 (45%) of 82 patients. Hagen et al. [
19] revealed that pathological complete response was found in 18 (49%) of 37 patients with 6th AJCC T1N1M0 or T2-3N0-1M0 ESCC receiving 41.4 Gy preoperative chemoradiotherapy. Lee et al. [
15] reported a 43% pathological complete response rate in 35 patients with 6th AJCC stage II or III ESCC receiving 45.6 Gy preoperative chemoradiotherapy. In the study of Tepper et al. [
5], 10 (40%) of 25 patients with 6th AJCC T1-3NxM0 esophageal cancer receiving 50.4 Gy preoperative chemoradiotherapy achieved a pathological complete response. Stahl et al. [
8] showed that pathological complete response was found in 18 (32%) of 57 patients with 6th AJCC T3-4N0-1M0 ESCC receiving 40 Gy preoperative chemoradiotherapy. Yang et al. described a 43% pathological complete response rate in 185 patients with 6th AJCC T1-4N1M0/T4N0M0 receiving 40 Gy preoperative chemoradiotherapy. The above series (summarized in
Table 7) seem to further support that higher radiotherapy doses of preoperative chemoradiotherapy contribute to increased pathological complete response. However, in a meta-analysis by Engel et al. [
20], evaluating radiotherapy dose in patients with esophageal cancer treated by preoperative chemoradiotherapy, no difference in OS was revealed between high dose radiotherapy (>48.85 Gy biologically effective dose) and low dose radiotherapy (<48.85 Gy biologically effective dose). Further prospective study is necessary to clarify this issue.
In our study, we found that the incidence of acute respiratory distress syndrome after esophagectomy in patients receiving radiotherapy doses of 50–50.4 Gy was significantly higher (13% versus 3%) than that in patients receiving radiotherapy doses of 36 Gy. Pulmonary complications including pneumonia, acute respiratory distress syndrome, or empyema were noted in 27% of patients receiving a radiotherapy dose of 36 Gy, and 37% of patients receiving radiotherapy doses of 50–50.4 Gy. Thomas et al. [
22] reported that mean lung radiation dose was a predictor for pulmonary complications in patients with esophageal cancer receiving preoperative chemoradiotherapy followed by esophagectomy. A previous study by Burmeister et al. [
14] found a 20% major pulmonary complication rate in patients with 6th AJCC T1-3N0-1M0 esophageal cancer receiving 35 Gy preoperative chemoradiotherapy. However, in patients with 6th AJCC T1N1M0 or T2-3N0-1M0 esophageal cancer receiving 41.4Gy preoperative chemoradiotherapy, Hagen et al. [
19] reported a 46% pulmonary complication rate. Moreover, in patients with 6th AJCC T1-3NxM0 esophageal cancer receiving 50.4 Gy preoperative chemoradiotherapy, Tepper et al. [
5] described a 38% pulmonary complication rate. Among these studies, pulmonary complications were still the most common form of postoperative morbidity and seemed increase with radiation dose. Reducing the incidence of severe postoperative pulmonary complications is important in patients receiving preoperative chemoradiotherapy followed by esophagectomy to achieve better prognoses.
The rate of anastomosis leakage ranged from 3% to 30% and varied between studies. Multiple factors including radiotherapy field, radiotherapy dose, surgical procedure, and chemotherapy regimen may influence anastomosis leakage rates. Koëter et al. [
23] analyzed 53 patients receiving preoperative chemoradiotherapy (41.4 Gy in 18 fractions combined with paclitaxel and carboplatin) followed by esophagectomy with cervical anastomosis, and reported that radiation dose has no impact on anastomosis leakage occurrence. However, forty-nine (92%) of 53 patients in their study had adenocarcinoma, which usually involves the lower third of the esophagus and neck area, which is the future anastomosis site and is seldom covered by radiotherapy in lower third esophageal cancer. Walle et al. [
24] analyzed 54 patients receiving preoperative chemoradiotherapy (36 Gy in 20 fractions combined with cisplatin and 5-fluorouracil) followed by Ivor Lewis esophagectomy with intrathoracic anastomosis and found that the incidence of anastomosis leak was related to the radiotherapy dose on the gastric fundus. In our study, patients receiving radiotherapy doses of 50–50.4 Gy had a higher anastomosis leak rate (23% versus 5%,
p = 0.004) than those receiving a radiotherapy dose of 36 Gy. We suggest that it may be ascribed to our radiotherapy field containing a future cervical anastomosis site. In our concurrent chemoradiotherapy planning, the esophagus, neck, and supraclavicular areas, which were future cervical anastomosis sites, were covered in the clinical target volume (CTV) of radiotherapy, and therefore higher radiotherapy doses contributed to more anastomosis leaks. Further studies with detailed radiotherapy fields, radiotherapy doses, surgical procedures, and chemotherapy regimen analysis are necessary to define the impact of radiotherapy on the incidence of anastomosis leak.
It is well known that perioperative complications have a negative impact on both OS and DFS [
25,
26]. In our study, although patients receiving 50–50.4 Gy preoperative chemoradiotherapy had more acute respiratory distress syndrome and anastomosis leaks than those receiving 36 Gy preoperative chemoradiotherapy, they had better OS and DFS, which is contrary to the existing literature studying perioperative complications of esophagectomy. This may be ascribed to a higher pathological complete response rate in patients receiving 50–50.4 Gy preoperative chemoradiotherapy.
Our study has important limitations. First, our results are based on a retrospective analysis which was conducted in a single hospital. The retrospective design of this analysis further justifies the conclusion that a prospective study in the future is needed to define our findings. Secondly, the patient number was small. Thirdly, the long treatment period of 15 years in our study is also an important limitation. The treatment characteristics may have changed over time. For example, PET-CT was not routinely reimbursed before 2010 by Taiwan’s health-insurance system, and thus some patients before 2010 may have been understaged. Three different surgeons joined our group in the fifteen years. Although all of them performed minimally invasive esophagectomy in the same fashion, different surgeons will lead to different results and impact the survival.
In conclusion, for patients with locally advanced esophageal squamous cell carcinoma, preoperative chemoradiotherapy with higher radiotherapy dose led to increased pathologic complete response rates and improved overall survival. In the future, prospective clinical trials evaluating the role of radiotherapy doses in patients with locally advanced esophageal squamous cell carcinoma receiving preoperative chemoradiotherapy are required.

 ,
, 

{kind=link}