Satisfaction among Cancer Patients Undergoing Radiotherapy during the COVID-19 Pandemic: An Institutional Experience

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Survey Development
2.3. Data Collection
2.4. Statistical Analysis
3. Results
3.1. Response Rate and Demographic Characteristics
3.2. Pandemic Related Concerns
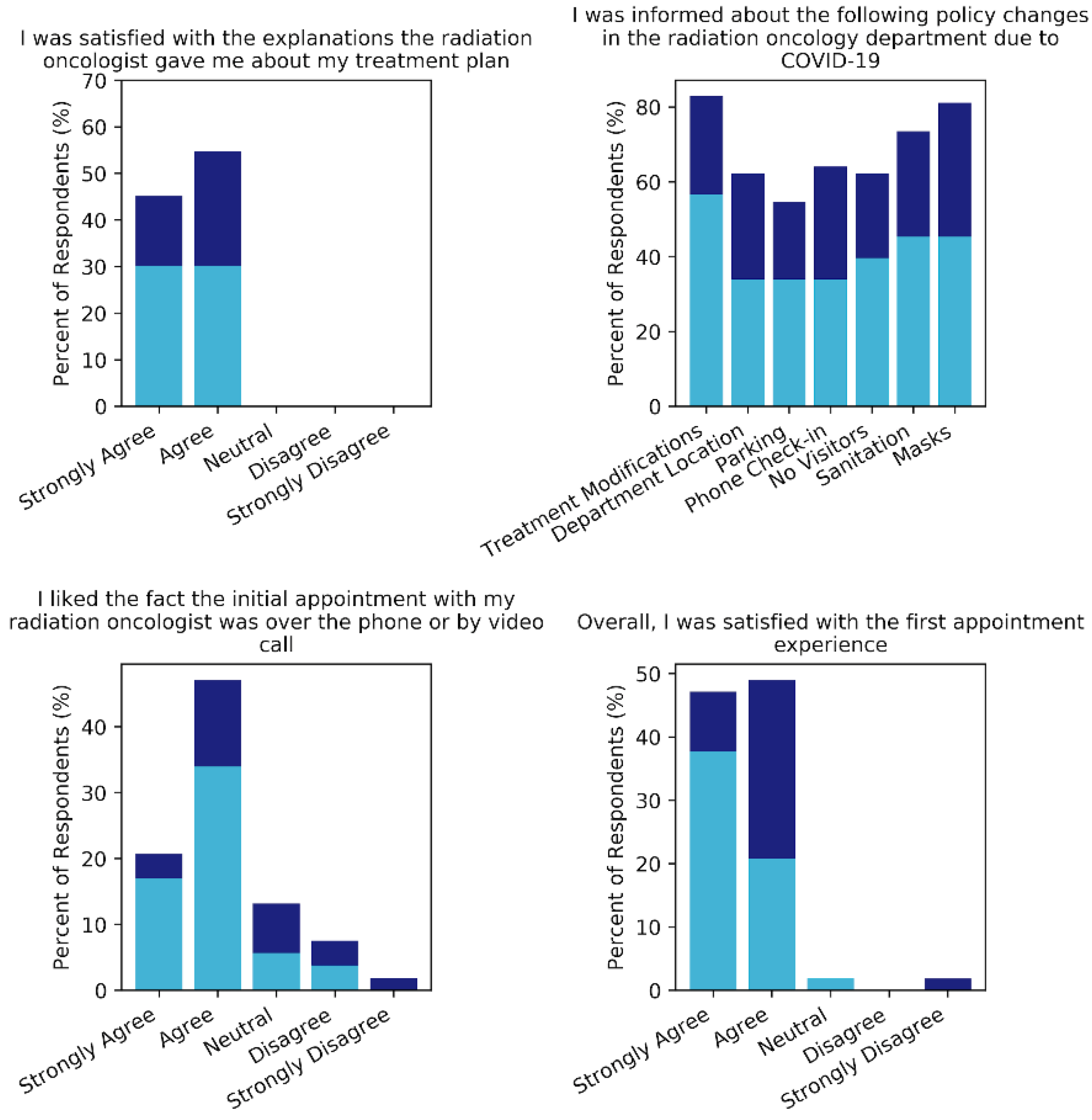
3.3. Initial Telemedicine Appointment Experience
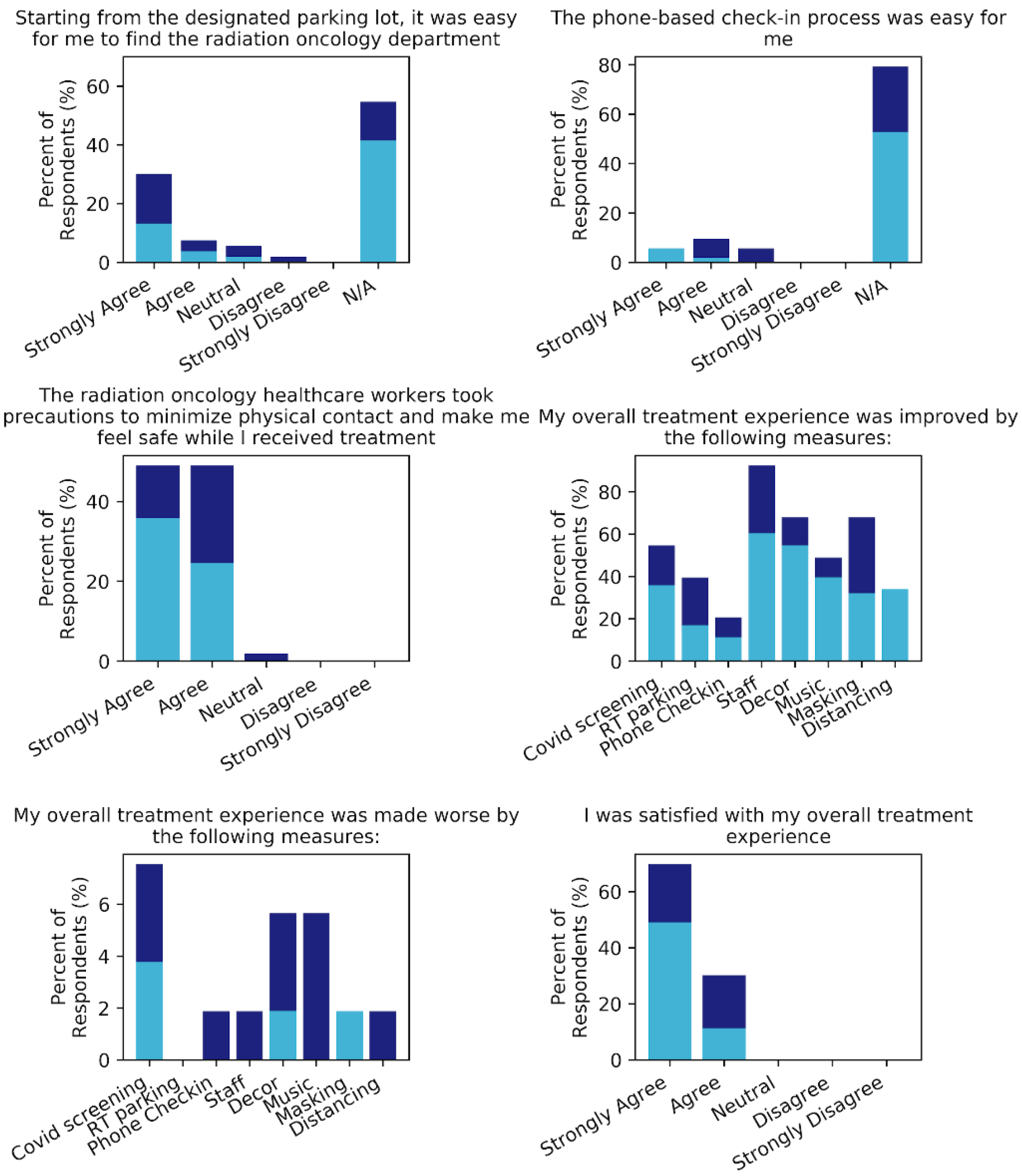
3.4. Hospital Visit and Treatment Experience
3.5. Qualitative Responses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Listings of WHO’s Response to COVID-19. 15 December 2020. Available online: https://www.who.int/news/item/29-06-2020-covidtimeline (accessed on 12 January 2021).
- Johns Hopkins University. Coronavirus Resource Center. 2021. Available online: https://0-coronavirus-jhu-edu.brum.beds.ac.uk/ (accessed on 12 January 2021).
- Tanne, J.H.; Hayasaki, E.; Zastrow, M.; Pulla, P.; Smith, P.; Rada, A.G. Covid-19: How doctors and healthcare systems are tackling coronavirus worldwide. BMJ 2020, 368, m1090. [Google Scholar] [CrossRef] [Green Version]
- Liang, W.; Guan, W.; Chen, R.; Wang, W.; Li, J.; Xu, K.; Li, C.; Ai, Q.; Lu, W.; Liang, H.; et al. Cancer patients in SARS-CoV-2 infection: A nationwide analysis in China. Lancet Oncol. 2020, 21, 335–337. [Google Scholar] [CrossRef]
- Garassino, M.C.; Whisenant, J.G.; Huang, L.-C.; Trama, A.; Torri, V.; Agustoni, F.; Baena, J.; Banna, G.; Berardi, R.; Bettini, A.C.; et al. COVID-19 in patients with thoracic malignancies (TERAVOLT): First results of an international, registry-based, cohort study. Lancet Oncol. 2020, 21, 914–922. [Google Scholar] [CrossRef]
- Kuderer, N.M.; Choueiri, T.K.; Shah, D.P.; Shyr, Y.; Rubinstein, S.M.; Rivera, D.R.; Shete, S.; Hsu, C.-Y.; Desai, A.; de Lima Lopes, G.; et al. Clinical impact of COVID-19 on patients with cancer (CCC19): A cohort study. Lancet 2020, 395, 1907–1918. [Google Scholar] [CrossRef]
- Lee, L.Y.W.; Cazier, J.-B.; Starkey, T.; Briggs, S.E.W.; Arnold, R.; Bisht, V.; Booth, S.; Campton, N.A.; Cheng, V.W.T.; Collins, G.; et al. COVID-19 prevalence and mortality in patients with cancer and the effect of primary tumour subtype and patient demographics: A prospective cohort study. Lancet Oncol. 2020, 21, 1309–1316. [Google Scholar] [CrossRef]
- Maringe, C.; Spicer, J.; Morris, M.; Purushotham, A.; Nolte, E.; Sullivan, R.; Rachet, B.; Aggarwal, A. The impact of the COVID-19 pandemic on cancer deaths due to delays in diagnosis in England, UK: A national, population-based, modelling study. Lancet Oncol. 2020, 21, 1023–1034. [Google Scholar] [CrossRef]
- Filippi, A.R.; Russi, E.; Magrini, S.M.; Corvò, R. Letter from Italy: First practical indications for radiation therapy departments during COVID-19 out-break. Int. J. Radiat. Oncol. Biol. Phys. 2020, 107, 597–599. [Google Scholar] [CrossRef]
- Krengli, M.; Ferrara, E.; Mastroleo, F.; Brambilla, M.; Ricardi, U. Running a Radiation Oncology Department at the Time of Coronavirus: An Italian Experience. Adv. Radiat. Oncol. 2020, 5 (Suppl. 1), 3–6. [Google Scholar] [CrossRef] [PubMed]
- Rivera, A.; Ohri, N.; Thomas, E.; Miller, R.; Knoll, M.A. The Impact of COVID-19 on Radiation Oncology Clinics and Patients with Cancer in the United States. Adv. Radiat. Oncol. 2020, 5, 538–543. [Google Scholar] [CrossRef]
- Wu, S.; Zheng, D.; Liu, Y.; Hu, D.; Wei, W.; Han, G. Radiation Therapy Care During a Major Outbreak of COVID-19 in Wuhan. Adv. Radiat. Oncol. 2020, 5, 531–533. [Google Scholar] [CrossRef]
- Cancer Care Ontario. COVID-19 Supplemental Clinical Guidance for Patients with Cancer. 2020. Available online: https://www.ontariohealth.ca/sites/ontariohealth/files/2020-04/Ontario%20Health%20Cancer%20Care%20Ontario%20COVID-19%20Supplemental%20Clinical%20Guidance%20for%20Patients%20with%20Cancer_29Mar20%20PDF.pdf (accessed on 12 January 2021).
- BC Cancer, Provincial Cancer Clinical Management Guidelines in Pandemic Situation (COVID-19). 2020. Available online: http://www.bccancer.bc.ca/health-professionals/clinical-resources/covid-19-resources (accessed on 12 January 2021).
- Ministere de Sante et Services Sociaux du Quebec, Recommandations en Radio-Oncologie dans le Contexte COVID-19. 2020. Available online: https://publications.msss.gouv.qc.ca/msss/document-002698/ (accessed on 12 January 2021).
- Patrick, H.M.; Hijal, T.; Souhami, L.; Freeman, C.; Parker, W.; Joly, L.; Kildea, J. A Canadian Response to the Coronavirus Disease 2019 (COVID-19) Pandemic: Is There a Silver Lining for Radiation Oncology Patients? Adv. Radiat. Oncol. 2020, 5, 774–776. [Google Scholar] [CrossRef]
- Gregucci, F.; Caliandro, M.; Surgo, A.; Carbonara, R.; Bonaparte, I.; Fiorentino, A. Cancer patients in Covid-19 era: Swimming against the tide. Radiother. Oncol. 2020, 149, 109–110. [Google Scholar] [CrossRef]
- Miaskowski, C.; Paul, S.M.; Snowberg, K.; Abbott, M.; Borno, H.; Chang, S.; Chen, L.M.; Cohen, B.; Cooper, B.A.; Hammer, M.J.; et al. Oncology patients’ perceptions of and experiences with COVID-19. Support. Care Cancer 2021, 29, 1941–1950. [Google Scholar] [CrossRef] [PubMed]
- Karacin, C.; Bilgetekin, I.; Basal, F.B.; Oksuzoglu, O.B. How does COVID-19 fear and anxiety affect chemotherapy adherence in patients with cancer. Futur. Oncol. 2020, 16, 2283–2293. [Google Scholar] [CrossRef] [PubMed]
- Kosir, U.; Loades, M.; Wild, J.; Wiedemann, M.; Krajnc, A.; Roškar, S.; Bowes, L. The impact of COVID-19 on the cancer care of adolescents and young adults and their well-being: Results from an online survey conducted in the early stages of the pandemic. Cancer 2020, 126, 4414–4422. [Google Scholar] [CrossRef] [PubMed]
- Sigorski, D.; Sobczuk, P.; Osmola, M.; Kuć, K.; Walerzak, A.; Wilk, M.; Ciszewski, T.; Kopeć, S.; Hryń, K.; Rutkowski, P.; et al. Impact of COVID-19 on anxiety levels among patients with cancer actively treated with systemic therapy. ESMO Open 2020, 5, e000970. [Google Scholar] [CrossRef]
- Cancer Research UK. Cancer Research UK Cancer Patient Experience Survey 2020: The Impact of COVID-19 on Cancer Patients in the UK. 2020. Available online: https://www.cancerresearchuk.org/sites/default/files/pes-covid_2020.pdf (accessed on 12 January 2021).
- Hawthorne, G.; Sansoni, J.; Hayes, L.; Marosszeky, N.; Sansoni, E. Measuring patient satisfaction with health care treatment using the Short Assessment of Patient Sat-isfaction measure delivered superior and robust satisfaction estimates. J. Clin. Epidemiol. 2014, 67, 527–537. [Google Scholar] [CrossRef]
- Desideri, I.; Francolini, G.; Ciccone, L.P.; Stocchi, G.; Salvestrini, V.; Aquilano, M.; Greto, D.; Bonomo, P.; Meattini, I.; Scotti, V.; et al. Impact of COVID-19 on patient–doctor interaction in a complex radiation therapy facility. Support. Care Cancer 2020, 1–7. [Google Scholar] [CrossRef]
- Gupta, D.; Rodeghier, M.; Lis, C.G. Patient satisfaction with service quality in an oncology setting: Implications for prognosis in non-small cell lung cancer. Int. J. Qual. Health Care 2013, 25, 696–703. [Google Scholar] [CrossRef] [Green Version]
- Lis, C.G.; Rodeghier, M.; Gupta, D. Distribution and determinants of patient satisfaction in oncology: A review of the literature. Patient Prefer. Adherence 2009, 3, 287–304. [Google Scholar]
- Saito, A.I.; Suda, M.; Sasai, K.; Jagsi, R. Satisfaction of breast cancer patients regarding surgery and radiation therapy: A survey in Japan. Adv. Radiat. Oncol. 2016, 1, 216–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shabason, J.E.; Mao, J.J.; Frankel, E.S.; Vapiwala, N. Shared decision-making and patient control in radiation oncology: Implications for patient satisfaction. Cancer 2014, 120, 1863–1870. [Google Scholar] [CrossRef] [PubMed]
- Miller, C.; Kaltman, R.D.; Leon, A.; Gesteira, A.; Duffy, S.; Burgess, P.B. Telemedicine usability for cancer care during the COVID-19 pandemic. J. Clin. Oncol. 2020, 265. [Google Scholar] [CrossRef]
- Ramaswamy, A.; Yu, M.; Drangsholt, S.; Ng, E.; Culligan, P.J.; Schlegel, P.N.; Hu, J.C. Patient Satisfaction with Telemedicine during the COVID-19 Pandemic: Retrospective Cohort Study. J. Med. Internet Res. 2020, 22, e20786. [Google Scholar] [CrossRef] [PubMed]
- Zimmerman, B.S.; Seidman, D.; Berger, N.; Cascetta, K.P.; Nezolosky, M.; Trlica, K.; Ryncarz, A.; Keeton, C.; Moshier, E.; Tiersten, A. Patient Perception of Telehealth Services for Breast and Gynecologic Oncology Care during the COVID-19 Pandemic: A Single Center Survey-based Study. J. Breast Cancer 2020, 23, 542–552. [Google Scholar] [CrossRef] [PubMed]
- Gadzinski, A.J.; Abarro, I.O. Telemedicine Multidisciplinary Urologic Cancer Clinics during COVID-19. In Proceedings of the Society of Urologic Oncology 21st Annual Meeting, Dallas, TX, USA, 2–4 December 2020. [Google Scholar]
- O’Reilly-Shah, V.N. Factors influencing healthcare provider respondent fatigue answering a globally administered in-app survey. PeerJ 2017, 5, e3785. [Google Scholar] [CrossRef] [Green Version]
- Falcone, R.; Grani, G.; Ramundo, V.; Melcarne, R.; Giacomelli, L.; Filetti, S.; Durante, C. Cancer Care During COVID-19 Era: The Quality of Life of Patients With Thyroid Malignancies. Front. Oncol. 2020, 10, 1128. [Google Scholar] [CrossRef]
- Blanchard, C.G.; Labrecque, M.S.; Ruckdeschel, J.C.; Blanchard, E.B. Physician behaviors, patient perceptions, and patient characteristics as predictors of satisfaction of hospitalized adult cancer patients. Cancer 1990, 65, 186–192. [Google Scholar] [CrossRef]
- Rahmqvist, M. Patient satisfaction in relation to age, health status and other background factors: A model for comparisons of care units. Int. J. Qual. Health Care 2001, 13, 385–390. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Total (n = 53) | ||
|---|---|---|
| Age | 18–25 | 0 |
| 26–45 | 3 (5.66%) | |
| 46–65 | 16 (30.19%) | |
| 66–75 | 25 (47.17%) | |
| Over 75 | 9 (16.80%) | |
| Gender | Male | 17 (32.08%) |
| Female | 36 (67.92%) | |
| Cancer Diagnosis | Breast | 24 (45.28%) |
| Prostate | 3 (5.66%) | |
| Lung | 7 (13.21%) | |
| Colon | 3 (5.66%) | |
| Gynecologic | 1 (1.89%) | |
| Other | 15 (28.30%) | |
| Diagnosis Date | Prior to March 2020 | 30 (56.60%) |
| March 2020 and later | 22 (41.51%) | |
| Unknown | 1 (1.89%) | |
| Cancer treatments received | Radiotherapy | 53 (100.00%) |
| Systemic Therapy | 34 (64.15%) | |
| Surgery | 35 (66.04%) |
| Frequency of Commentary on Various Aspects of Treatment Experience | ||||
|---|---|---|---|---|
| Total | Positive Attitude | Negative Attitude | p-Value | |
| Communication | 14 | 1 | 13 | 0.001 |
| Staff | 12 | 11 | 1 | 0.004 |
| Clinic Organization | 7 | 2 | 5 | ns |
| Environment & Decor | 7 | 4 | 3 | ns |
| Pandemic Safety Procedures | 10 | 5 | 5 | ns |
| Treatment Procedures | 6 | 0 | 4 | ns |
| Health Concerns (General) | 12 | 0 | 11 | 0.001 |
| Emotional State | 7 | 4 | 3 | ns |
| Waiting | 3 | 2 | 1 | ns |
| Transit to/from Centre | 5 | 3 | 2 | ns |
| Other Specialists | 5 | 0 | 5 | 0.025 |
| Generic Sentiments | 14 | 14 | 0 | <0.001 |
| Relation to overall treatment experience satisfaction p < 0.001 | ||||
| Very Satisfied | Satisfied | |||
| Positive Attitude | 40 | 6 | ||
| Negative Attitude | 29 | 24 | ||
| Relation to overall telehealth consult experience satisfaction p = 0.001 | ||||
| Very Satisfied | Satisfied | Neutral | Very Unsatisfied | |
| Positive Attitude | 37 | 6 | 0 | 3 |
| Negative Attitude | 23 | 26 | 1 | 3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Lalla, V.; Patrick, H.; Siriani-Ayoub, N.; Kildea, J.; Hijal, T.; Alfieri, J. Satisfaction among Cancer Patients Undergoing Radiotherapy during the COVID-19 Pandemic: An Institutional Experience. Curr. Oncol. 2021, 28, 1507-1517. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol28020142
Di Lalla V, Patrick H, Siriani-Ayoub N, Kildea J, Hijal T, Alfieri J. Satisfaction among Cancer Patients Undergoing Radiotherapy during the COVID-19 Pandemic: An Institutional Experience. Current Oncology. 2021; 28(2):1507-1517. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol28020142
Chicago/Turabian StyleDi Lalla, Vanessa, Haley Patrick, Nicolas Siriani-Ayoub, John Kildea, Tarek Hijal, and Joanne Alfieri. 2021. "Satisfaction among Cancer Patients Undergoing Radiotherapy during the COVID-19 Pandemic: An Institutional Experience" Current Oncology 28, no. 2: 1507-1517. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol28020142