Regression of Intracranial Meningiomas Following Treatment with Cabozantinib

 , ,
, ,
Abstract
:1. Introduction
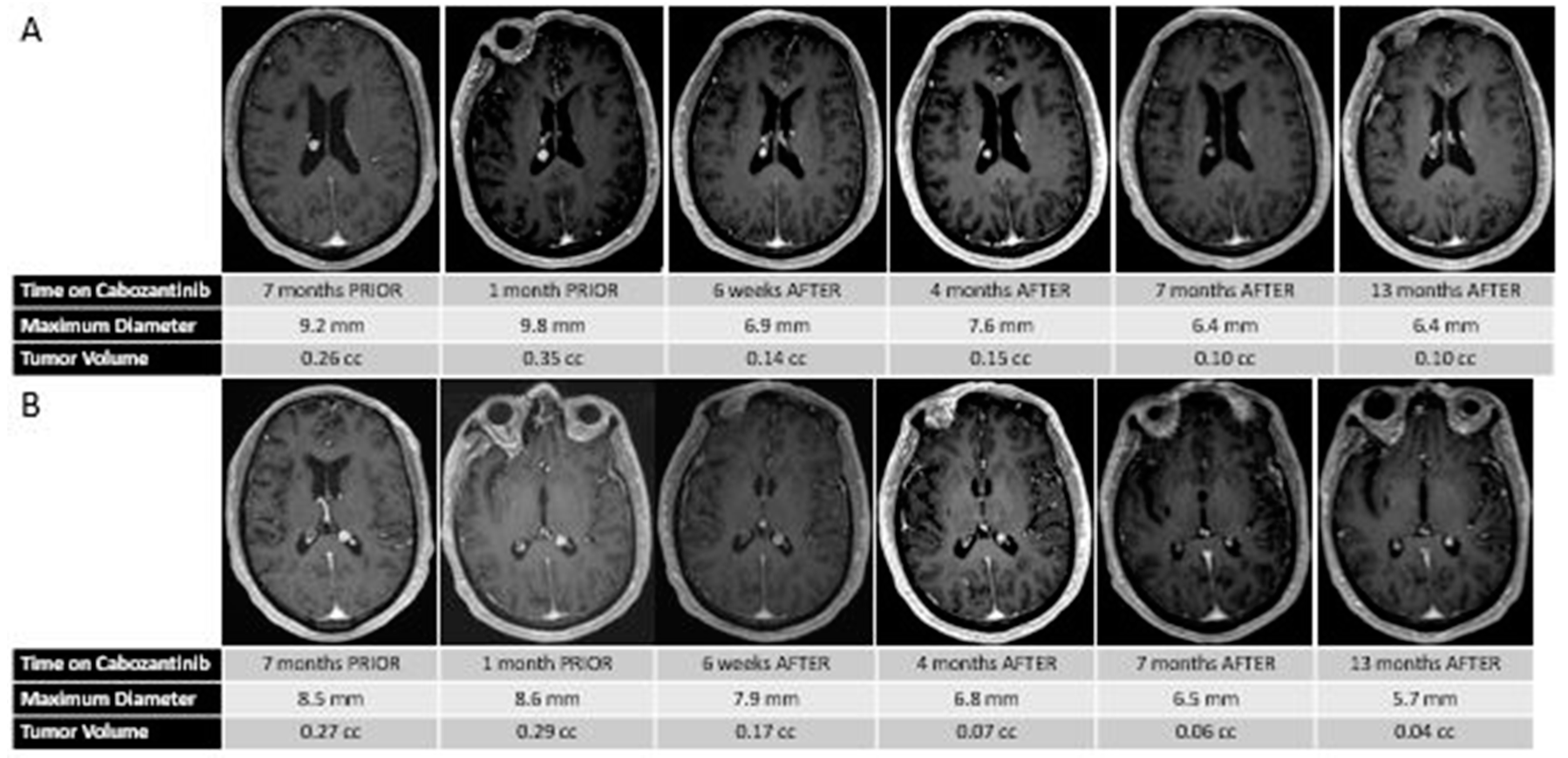
2. Case Report
3. Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jääskeläinen, J.; Haltia, M.; Servo, A. Atypical and anaplastic meningiomas: Radiology, surgery, radiotherapy, and outcome. Surg. Neurol. 1986, 25, 233–242. [Google Scholar] [CrossRef]
- Rogers, C.L.; Perry, A.; Pugh, S.; Vogelbaum, M.A.; Brachman, D.; McMillan, W.; Jenrette, J.; Barani, I.; Shrieve, D.; Sloan, A.; et al. Pathology concordance levels for meningioma classification and grading in NRG Oncology RTOG Trial 0539. Neuro Oncol. 2016, 18, 565–574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rogers, C.L.; Won, M.; Vogelbaum, M.A.; Perry, A.; Ashby, L.S.; Modi, J.M.; Alleman, A.M.; Galvin, J.; Fogh, S.E.; Youssef, E.; et al. High-risk meningioma: Initial outcomes from NRG Oncology/RTOG 0539. Int. J. Radiat. Oncol. 2020, 106, 790–799. [Google Scholar] [CrossRef] [PubMed]
- Sherman, W.J.; Raizer, J.J. Medical management of meningiomas. CNS Oncol. 2013, 2, 161–170. [Google Scholar] [CrossRef]
- Preusser, M.; Brastianos, P.K.; Mawrin, C. Advances in meningioma genetics: Novel therapeutic opportunities. Nat. Rev. Neurol. 2018, 14, 106–115. [Google Scholar] [CrossRef] [PubMed]
- Yun, S.; Koh, J.M.; Lee, K.S.; Seo, A.N.; Nam, K.H.; Choe, G. Expression of c-MET in Invasive Meningioma. J. Pathol. Transl. Med. 2015, 49, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Dasanu, C.A.; Samara, Y.; Codreanu, I.; Limonadi, F.M.; Hamid, O.; Alvarez-Argote, J. Systemic therapy for relapsed/refractory meningioma: Is there potential for antiangiogenic agents? J. Oncol. Pharm. Pract. 2019, 25, 638–647. [Google Scholar] [CrossRef]
- Reszec, J.; Hermanowicz, A.; Rutkowski, R.; Turek, G.; Mariak, Z.; Chyczewski, L. Expression of MMP-9 and VEGF in meningiomas and their correlation with peritumoral brain edema. Biomed Res. Int. 2015, 2015, 646853. [Google Scholar] [CrossRef] [PubMed]
- Franke, A.; Skelton IV, W.; Woody, L.; Bregy, A.; Shah, A.; Vakharia, K.; Komotar, R. Role of bevacizumab for treatment-refractory meningiomas: A systematic analysis and literature review. Surg. Neurol. Int. 2018, 9, 133. [Google Scholar]
- Kaley, T.J.; Wen, P.; Schiff, D.; Ligon, K.; Haidar, S.; Karimi, S.; Lassman, A.B.; Nolan, C.P.; De Angelis, L.M.; Gavrilovic, I.; et al. Phase II trial of sunitinib for recurrent and progressive atypical and anaplastic meningioma. Neuro Oncol. 2015, 17, 116–121. [Google Scholar] [CrossRef] [Green Version]
- Shih, K.C.; Chowdhary, S.; Rosenblatt, P.; Weir, A.B.; Shepard, G.C.; Williams, J.T.; Shastry, M.; Burris, H.A.; Hainsworth, J.D. A phase II trial of bevacizumab and everolimus as treatment for patients with refractory, progressive intracranial meningioma. J. Neurooncol. 2016, 129, 281–288. [Google Scholar] [CrossRef] [PubMed]
- Raizer, J.J.; Grimm, S.A.; Rademaker, A.; Chandler, J.P.; Muro, K.; Helenowski, I.; Rice, L.; McCarthy, K.; Johnston, S.K.; Mrugala, M.M.; et al. A phase II trial of PTK787/ZK 222584 in recurrent or progressive radiation and surgery refractory meningiomas. J. Neurooncol. 2014, 117, 93–101. [Google Scholar] [CrossRef]
- Yakes, F.M.; Chen, J.; Tan, J.; Yamaguchi, K.; Shi, Y.; Yu, P.; Qian, F.; Chu, F.; Bentzien, F.; Cancilla, B.; et al. Cabozantinib (XL184), a Novel MET and VEGFR2 Inhibitor, Simultaneously Suppresses Metastasis, Angiogenesis, and Tumor Growth. Mol. Cancer Ther. 2011, 10, 2298–2308. [Google Scholar] [CrossRef] [Green Version]
- Puchner, M.J.A.; Hans, V.H.; Harati, A.; Lohmann, F.; Glas, M.; Herrlinger, U. Bevacizumab-induced regression of anaplastic meningioma. Ann. Oncol. 2010, 21, 2445–2446. [Google Scholar] [CrossRef] [PubMed]
- Goutagny, S.; Raymond, E.; Sterkers, O.; Colombani, J.M.; Kalamarides, M. Radiographic regression of cranial meningioma in a NF2 patient treated by bevacizumab. Ann. Oncol. 2011, 22, 990–991. [Google Scholar] [CrossRef] [PubMed]
- Lou, E.; Sumrall, A.L.; Turner, S.; Peters, K.B.; Desjardins, A.; Vredenburgh, J.J.; McLendon, R.E.; Herndon, J.E.; McSherry, F.; Norfleet, J.; et al. Bevacizumab therapy for adults with recurrent/progressive meningioma: A retrospective series. J. Neurooncol. 2012, 109, 63–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nayak, L.; Iwamoto, F.M.; Rudnick, J.D.; Norden, A.D.; Lee, E.Q.; Drappatz, J.; Omuro, A.; Kaley, T.J. Atypical and anaplastic meningiomas treated with bevacizumab. J. Neurooncol. 2012, 109, 187–193. [Google Scholar] [CrossRef]
- Nunes, F.P.; Merker, V.L.; Jennings, D.; Caruso, P.A.; di Tomaso, E.; Muzikansky, A.; Barker, F.G.; Stemmer-Rachamimov, A.; Plotkin, S.R. Bevacizumab Treatment for Meningiomas in NF2: A Retrospective Analysis of 15 Patients. PLoS ONE 2013, 8, e59941. [Google Scholar] [CrossRef] [Green Version]
- Hawasli, A.H.; Rubin, J.B.; Tran, D.D.; Adkins, D.R.; Waheed, S.; Hullar, T.E.; Gutmann, D.H.; Evans, J.; Leonard, J.R.; Zipfel, G.J.; et al. Antiangiogenic agents for nonmalignant brain tumors. J. Neurol. Surg. Part B Skull Base 2013, 74, 136–141. [Google Scholar] [CrossRef] [Green Version]
- Alanin, M.C.; Klausen, C.; Caye-Thomasen, P.; Thomsen, C.; Fugleholm, K.; Poulsgaard, L.; Lassen, U.; Mau-Sorensen, M.; Hofland, K.F. Effect of bevacizumab on intracranial meningiomas in patients with neurofibromatosis type 2—A retrospective case series. Int. J. Neurosci. 2016, 126, 1002–1006. [Google Scholar] [CrossRef] [PubMed]
- Furtner, J.; Schöpf, V.; Seystahl, K.; Le Rhun, E.; Rudà, R.; Roelcke, U.; Koeppen, S.; Berghoff, A.S.; Marosi, C.; Clement, P.; et al. Kinetics of tumor size and peritumoral brain edema before, during, and after systemic therapy in recurrent WHO grade II or III meningioma. Neuro. Oncol. 2016, 18, 401–407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grimm, S.A.; Kumthekar, P.; Chamberlain, M.C.; Schiff, D.; Wen, P.Y.; Iwamoto, F.M.; Reardon, D.A.; Purow, B.; Raizer, J.J. Phase II trial of bevacizumab in patients with surgery and radiation refractory progressive meningioma. J. Clin. Oncol. 2015, 33, 2055. [Google Scholar] [CrossRef]
- Chevreau, C.; Ravaud, A.; Escudier, B.; Amela, E.; Delva, R.; Rolland, F.; Tosi, D.; Oudard, S.; Blanc, E.; Ferlay, C.; et al. A Phase II Trial of Sunitinib in Patients With Renal Cell Cancer and Untreated Brain Metastases. Clin. Genitourin. Cancer 2014, 12, 50–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pàez-Ribes, M.; Allen, E.; Hudock, J.; Takeda, T.; Okuyama, H.; Viñals, F.; Inoue, M.; Bergers, G.; Hanahan, D.; Casanovas, O. Antiangiogenic Therapy Elicits Malignant Progression of Tumors to Increased Local Invasion and Distant Metastasis. Cancer Cell 2009, 15, 220–231. [Google Scholar] [CrossRef] [Green Version]
- Elisei, R.; Schlumberger, M.J.; Müller, S.P.; Schöffski, P.; Brose, M.S.; Shah, M.H.; Licitra, L.; Jarzab, B.; Medvedev, V.; Kreissl, M.C.; et al. Cabozantinib in Progressive Medullary Thyroid Cancer. J. Clin. Oncol. 2013, 31, 3639–3646. [Google Scholar] [CrossRef] [Green Version]
- Choueiri, T.K.; Escudier, B.; Powles, T.; Tannir, N.M.; Mainwaring, P.N.; Rini, B.I.; Hammers, H.J.; Donskov, F.; Roth, B.J.; Peltola, K.; et al. Cabozantinib versus everolimus in advanced renal cell carcinoma (METEOR): Final results from a randomised, open-label, phase 3 trial. Lancet Oncol. 2016, 17, 917–927. [Google Scholar] [CrossRef] [Green Version]
- Cloughesy, T.F.; Drappatz, J.; De Groot, J.; Prados, M.D.; Reardon, D.A.; Schiff, D.; Chamberlain, M.; Mikkelsen, T.; Desjardins, A.; Ping, J.; et al. Phase II study of cabozantinib in patients with progressive glioblastoma: Subset analysis of patients with prior antiangiogenic therapy. Neuro Oncol. 2018, 20, 259–267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wen, P.Y.; Drappatz, J.; De Groot, J.; Prados, M.D.; Reardon, D.A.; Schiff, D.; Chamberlain, M.; Mikkelsen, T.; Desjardins, A.; Holland, J.; et al. Phase II study of cabozantinib in patients with progressive glioblastoma: Subset analysis of patients naive to antiangiogenic therapy. Neuro Oncol. 2018, 20, 249–258. [Google Scholar] [CrossRef] [PubMed]
- Hassaneen, W.; Suki, D.; Salaskar, A.L.; Wildrick, D.M.; Lang, F.F.; Fuller, G.N.; Sawaya, R. Surgical management of lateral-ventricle metastases: Report of 29 cases in a single-institution experience. J. Neurosurg. 2010, 112, 1046–1055. [Google Scholar] [CrossRef] [PubMed]
- Wasita, B.; Sakamoto, M.; Mizushima, M.; Kurosaki, M.; Watanabe, T. Choroid plexus metastasis from papillary thyroid carcinoma presenting with intraventricular hemorrhage: Case report. Neurosurgery 2010, 66, E1213–E1214. [Google Scholar] [CrossRef] [PubMed]
- Arneth, B. Update on the types and usage of liquid biopsies in the clinical setting: A systematic review. BMC Cancer 2018, 18, 527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mattox, A.K.; Yan, H.; Bettegowda, C. The potential of cerebrospinal fluid-based liquid biopsy approaches in CNS tumors. Neuro Oncol. 2019, 21, 1509–1518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhi, F.; Shao, N.; Li, B.; Xue, L.; Deng, D.; Xu, Y.; Lan, Q.; Peng, Y.; Yang, Y. A serum 6-miRNA panel as a novel non-invasive biomarker for meningioma. Sci. Rep. 2016, 6, 32067. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barciszewska, A.-M. Total DNA methylation as a biomarker of DNA damage and tumor malignancy in intracranial meningiomas. BMC Cancer 2020, 20, 509. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author and Year | Studied Drug | Mechanism of Action | Study Type | Number of Patients | Prior Surgery | Prior RT * | WHO Grade Inclusion | PFS 6 ** |
|---|---|---|---|---|---|---|---|---|
| Puchner et al., 2010 [14] | Bevacizumab | Anti-VEGF antibody | Case report | 1 | 1 | 1 | III | NA |
| Goutagny et al., 2011 [15] | Bevacizumab | Anti-VEGF antibody | Case report | 1 | NA | NA | NA | NA |
| Lou et al., 2012 [16] | Bevacizumab | Anti-VEGF antibody | Retrospective | 14 | 14 | 11 | I,II,III | 86% |
| Nayak et al., 2012 [17] | Bevacizumab | Anti-VEGF antibody | Retrospective | 15 | 15 | 15 | II,III | 44% |
| Nunes et al., 2013 [18] | Bevacizumab | Anti-VEGF antibody | Retrospective | 15 | NA | NA | NA | 93% |
| Hawasli et al., 2013 [19] | Bevacizumab, Pazopanib | Anti-VEGF antibody, TKI | Retrospective | 10 | 9 | 5 | NA | NA |
| Raizer et al., 2014 [12] | Vatalanib | VEGFR + PDGFR TKI | Phase II | 17 | 16 | 12 | I,II,III | 60% |
| Alanin et al., 2015 [20] | Bevacizumab | Anti-VEGF antibody | Retrospective | 7 | NA | NA | NA | NA |
| Kaley et al., 2015 [10] | Sunitinib | VEGFR + PDGFR TKI | Phase II | 36 | 36 | 35 | II,III | 42% |
| Furtner et al., 2015 [21] | Bevacizumab | Anti-VEGF antibody | Retrospective | 5 | NA | NA | II,III | NA |
| Grimm et al., 2015 [22] | Bevacizumab | Anti-VEGF antibody | Phase II | 40 | 40 | 40 | I,II,III | 27% |
| Shih et al., 2016 [11] | Bevacizumab, Everolimus | Anti-VEGF antibody | Phase II | 17 | 16 | 12 | I,II,III | 69% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kotecha, R.; Tonse, R.; Appel, H.; Odia, Y.; Kotecha, R.R.; Rabinowits, G.; Mehta, M.P. Regression of Intracranial Meningiomas Following Treatment with Cabozantinib. Curr. Oncol. 2021, 28, 1537-1543. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol28020145
Kotecha R, Tonse R, Appel H, Odia Y, Kotecha RR, Rabinowits G, Mehta MP. Regression of Intracranial Meningiomas Following Treatment with Cabozantinib. Current Oncology. 2021; 28(2):1537-1543. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol28020145
Chicago/Turabian StyleKotecha, Rupesh, Raees Tonse, Haley Appel, Yazmin Odia, Ritesh R. Kotecha, Guilherme Rabinowits, and Minesh P. Mehta. 2021. "Regression of Intracranial Meningiomas Following Treatment with Cabozantinib" Current Oncology 28, no. 2: 1537-1543. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol28020145