The Feasibility and Effects of a Telehealth-Delivered Home-Based Prehabilitation Program for Cancer Patients during the Pandemic


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Service Design
2.3. Referral Process
2.4. Format of Prehabilitation Sessions
2.5. Intervention
2.5.1. Physical Activity
2.5.2. Nutritional Education
2.5.3. Medical Optimization Therapies
2.5.4. Psychological Support
2.6. Signposting to Wellbeing Navigation Services
2.7. Outcome Measures
2.8. Statistical Analysis
2.9. Ethical Considerations
3. Results
3.1. Feasibility
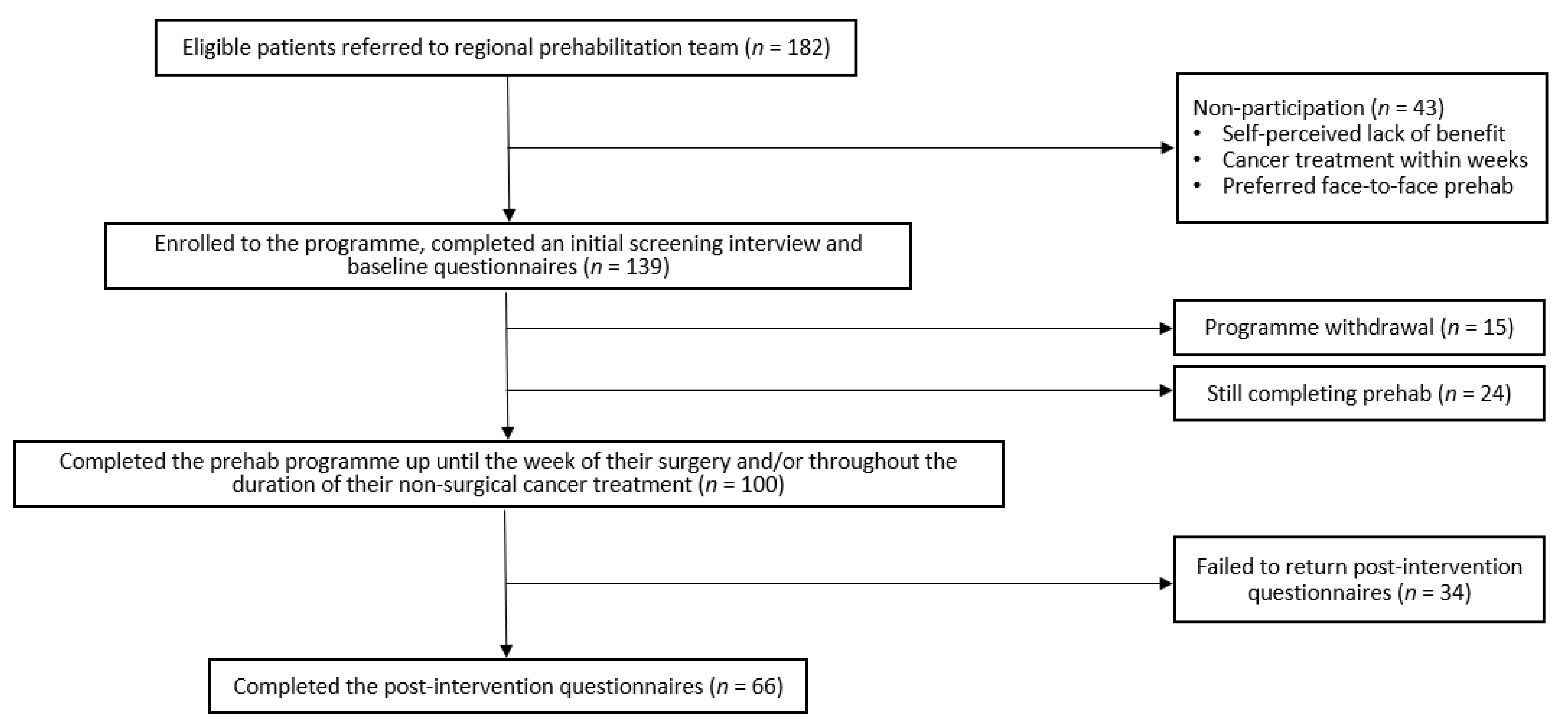
3.1.1. Recruitment Rate
3.1.2. Retention Rate
3.2. Patient Characteristics
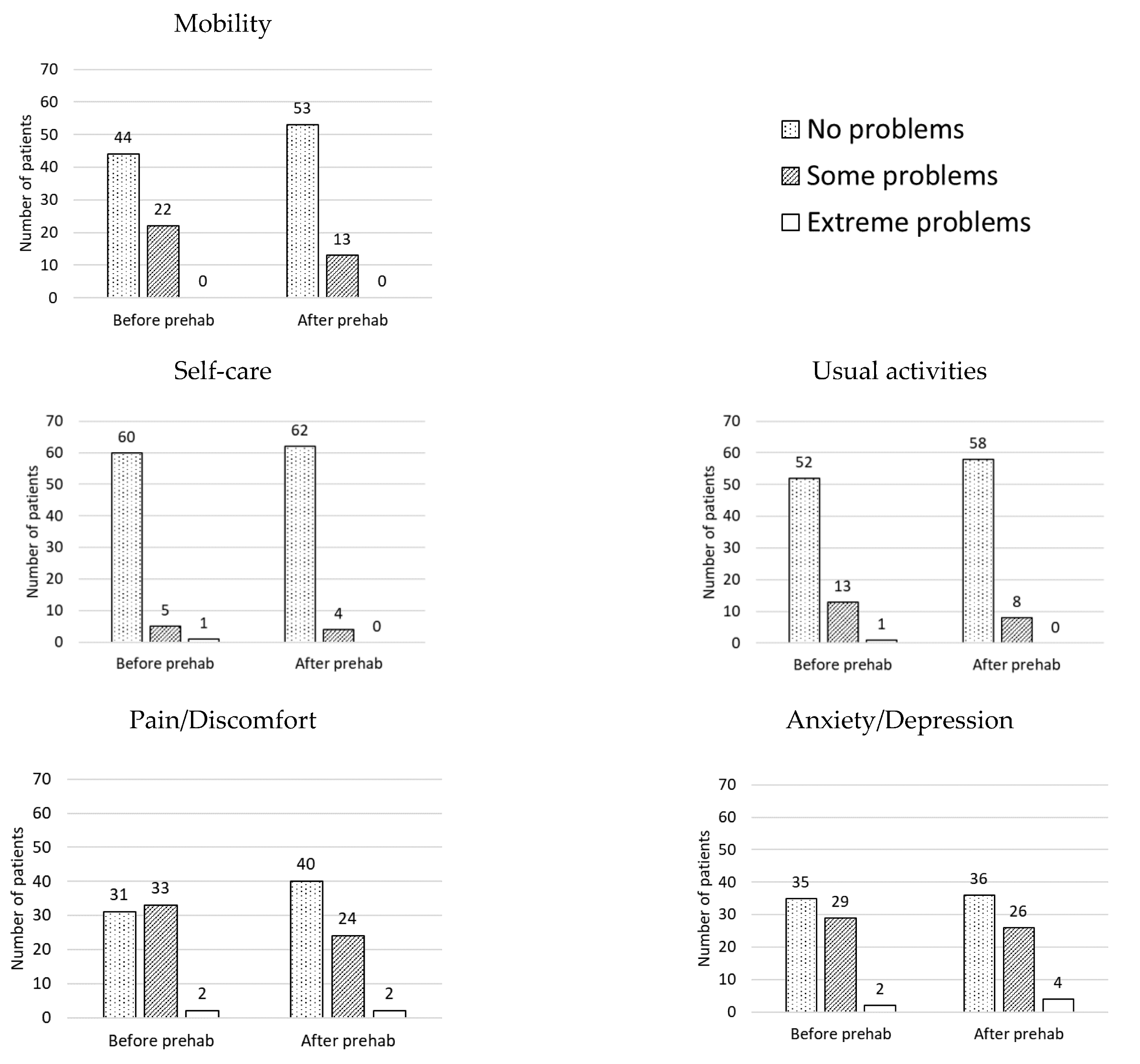
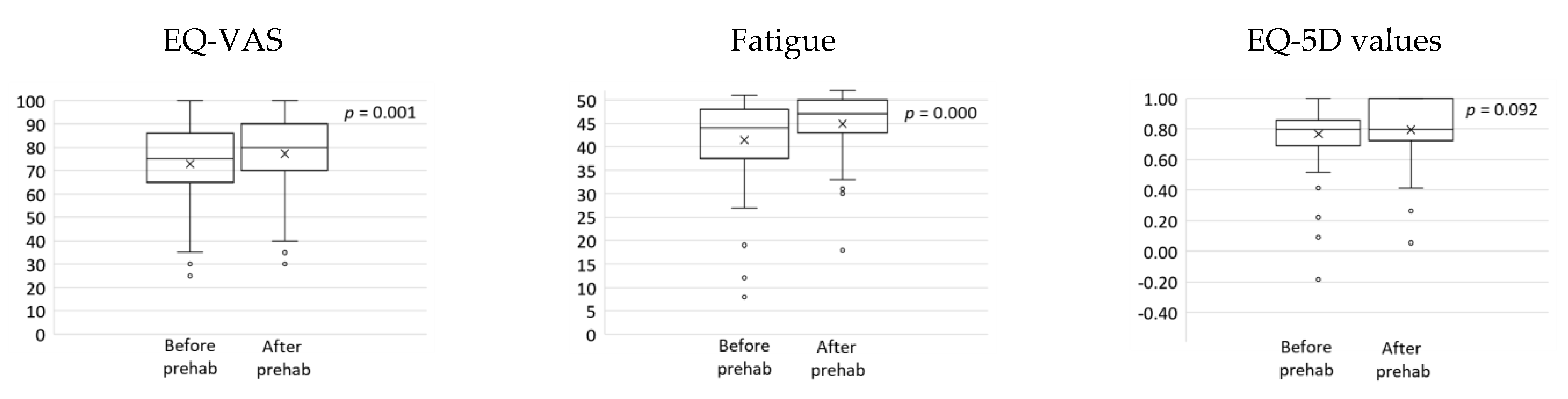
3.3. Patient-Reported Outcomes
3.4. Patient Feedback
3.4.1. Benefits
3.4.2. Challenges
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Güner, R.; Hasanoğlu, I.; Aktaş, F. COVID-19: Prevention and control measures in community. Turk. J. Med. Sci. 2020, 50, 571–577. [Google Scholar] [CrossRef] [PubMed]
- Peçanha, T.; Goessler, K.F.; Roschel, H.; Gualano, B. Social isolation during the COVID-19 pandemic can increase physical inactivity and the global burden of cardiovascular disease. Am. J. Physiol. Heart Circ. Physiol. 2020, 318, H1441–H1446. [Google Scholar] [CrossRef] [PubMed]
- Bailey, L.; Ward, M.; DiCosimo, A.; Baunta, S.; Cunningham, C.; Romero-Ortuno, R.; Kenny, R.A.; Purcell, R.; Lannon, R.; McCarroll, K.; et al. Physical and mental health of older people while cocooning during the COVID-19 pandemic. QJM Int. J. Med. 2021. [Google Scholar] [CrossRef] [PubMed]
- Laza-Cagigas, R.; Chan, S.; Sumner, D.; Rampal, T. Effects and feasibility of a prehabilitation programme incorporating a low-carbohydrate, high-fat dietary approach in patients with type 2 diabetes: A retrospective study. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 257–263. [Google Scholar] [CrossRef]
- Wu, F.; Laza-Cagigas, R.; Pagarkar, A.; Olaoke, A.; El Gammal, M.; Rampal, T. The Feasibility of Prehabilitation as Part of the Breast Cancer Treatment Pathway. PM&R 2020. [Google Scholar] [CrossRef]
- Tew, G.A.; Bedford, R.; Carr, E.; Durrand, J.W.; Gray, J.; Hackett, R.; Lloyd, S.; Peacock, S.; Taylor, S.; Yates, D.; et al. Community-based prehabilitation before elective major surgery: The PREP-WELL quality improvement project. BMJ Open Qual. 2020, 9, e000898. [Google Scholar] [CrossRef] [Green Version]
- Hijazi, Y.; Gondal, U.; Aziz, O. A systematic review of prehabilitation programs in abdominal cancer surgery. Int. J. Surg. 2017, 39, 156–162. [Google Scholar] [CrossRef]
- Hanna, K.; Ditillo, M.; Joseph, B. The role of frailty and prehabilitation in surgery. Curr. Opin. Crit. Care 2019, 25, 717–722. [Google Scholar] [CrossRef]
- Gillis, C.; Li, C.; Lee, L.; Awasthi, R.; Augustin, B.; Gamsa, A.; Liberman, A.S.; Stein, B.; Charlebois, P.; Feldman, L.S.; et al. Prehabilitation versus Rehabilitation. Anesthesiology 2014, 121, 937–947. [Google Scholar] [CrossRef]
- Minnella, E.M.; Awasthi, R.; Loiselle, S.-E.; Agnihotram, R.V.; Ferri, L.E.; Carli, F. Effect of Exercise and Nutrition Prehabilitation on Functional Capacity in Esophagogastric Cancer Surgery. JAMA Surg. 2018, 153, 1081–1089. [Google Scholar] [CrossRef] [Green Version]
- Bland, K.A.; Bigaran, A.; Campbell, K.L.; Trevaskis, M.; Zopf, E.M. Exercising in Isolation? The Role of Telehealth in Exercise Oncology during the COVID-19 Pandemic and Beyond. Phys. Ther. 2020, 100, 1713–1716. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, E.; Farahnak, P.; Franzén, E.; Nygren-Bonnier, M.; Dronkers, J.; Van Meeteren, N.; Rydwik, E. Feasibility of preoperative supervised home-based exercise in older adults undergoing colorectal cancer surgery—A randomized controlled design. PLoS ONE 2019, 14, e0219158. [Google Scholar] [CrossRef]
- Ngo-Huang, A.; Parker, N.H.; Bruera, E.; Lee, R.E.; Simpson, R.; O’Connor, D.P.; Petzel, M.Q.B.; Fontillas, R.C.; Schadler, K.; Xiao, L.; et al. Home-Based Exercise Prehabilitation During Preoperative Treatment for Pancreatic Cancer Is Associated With Improvement in Physical Function and Quality of Life. Integr. Cancer Ther. 2019, 18. [Google Scholar] [CrossRef]
- Piraux, E.; Caty, G.; Reychler, G.; Forget, P.; Deswysen, Y. Feasibility and Preliminary Effectiveness of a Tele-Prehabilitation Program in Esophagogastric Cancer Patients. J. Clin. Med. 2020, 9, 2176. [Google Scholar] [CrossRef]
- Diamond, R.; Willan, J. Coronavirus disease 2019: Achieving good mental health during social isolation. Br. J. Psychiatry 2020, 217, 408–409. [Google Scholar] [CrossRef]
- Silver, J.K. Prehabilitation could save lives in a pandemic. BMJ 2020, 369, m1386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stratton, R.J.; Hackston, A.; Longmore, D.; Dixon, R.; Price, S.; Stroud, M.; King, C.; Elia, M. Malnutrition in hospital outpatients and inpatients: Prevalence, concurrent validity and ease of use of the ‘malnutrition universal screening tool’ (‘MUST’) for adults. Br. J. Nutr. 2004, 92, 799–808. [Google Scholar] [CrossRef] [PubMed]
- GOV.UK. Physical Activity Guidelines: UK Chief Medical Officers’ Report. 2021. Available online: https://www.gov.uk/government/publications/physical-activity-guidelines-uk-chief-medical-officers-report (accessed on 24 March 2021).
- Monteiro, C.A.; Cannon, G.; Levy, R.B.; Moubarac, J.-C.; Louzada, M.L.; Rauber, F.; Khandpur, N.; Cediel, G.; Neri, D.; Martinez-Steele, E.; et al. Ultra-processed foods: What they are and how to identify them. Public Health Nutr. 2019, 22, 936–941. [Google Scholar] [CrossRef] [PubMed]
- Deer, R.; Volpi, E. Protein intake and muscle function in older adults. Curr. Opin. Clin. Nutr. Metab. Care 2015, 18, 248–253. [Google Scholar] [CrossRef] [Green Version]
- Teixeira, F.J.; Santos, H.O.; Howell, S.L.; Pimentel, G.D. Whey protein in cancer therapy: A narrative review. Pharmacol. Res. 2019, 144, 245–256. [Google Scholar] [CrossRef] [PubMed]
- Drinkaware.co.uk. UK Alcohol Unit Guidance: Chief Medical Officer’s Low Risk Drinking Guidelines. Available online: https://www.drinkaware.co.uk/facts/alcoholic-drinks-and-units/low-risk-drinking-guidelines#:~:text=UK%20alcohol%20unit%20guidance%3A%20CMOs%27%20Low%20Risk%20Drinking,on%20drinking%20in%20pregnancy%20and%20single%20occasion%20drinking (accessed on 18 April 2021).
- Thompson, A.J.; Turner, A.J. A Comparison of the EQ-5D-3L and EQ-5D-5L. PharmacoEconomics 2020, 38, 575–591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dolan, P. Modeling Valuations for EuroQol Health States. Med. Care 1997, 35, 1095–1108. [Google Scholar] [CrossRef] [PubMed]
- Hagstrom, A.; Marshall, P.W.M.; Lonsdale, C.; Cheema, B.S.; Singh, M.F.; Green, S.M. Resistance training improves fatigue and quality of life in previously sedentary breast cancer survivors: A randomised controlled trial. Eur. J. Cancer Care 2015, 25, 784–794. [Google Scholar] [CrossRef]
- NICE.org.uk. Position Statement on Use of the EQ-5D-5L Value Set for England. 2019. Available online: https://www.nice.org.uk/about/what-we-do/our-programmes/nice-guidance/technology-appraisal-guidance/eq-5d-5l (accessed on 23 May 2021).
- Ferreira, V.; Agnihotram, R.V.; Bergdahl, A.; Van Rooijen, S.J.; Awasthi, R.; Carli, F.; Scheede-Bergdahl, C. Maximizing patient adherence to prehabilitation: What do the patients say? Support. Care Cancer 2018, 26, 2717–2723. [Google Scholar] [CrossRef]
- Graley, C.E.; May, K.F.; McCoy, D.C. Postcode Lotteries in Public Health—The NHS Health Checks Programme in North West London. BMC Public Health 2011, 11, 738. [Google Scholar] [CrossRef] [Green Version]
- Robinson, A.; Oksuz, U.; Slight, R.; Slight, S.; Husband, A. Digital and Mobile Technologies to Promote Physical Health Behavior Change and Provide Psychological Support for Patients Undergoing Elective Surgery: Meta-Ethnography and Systematic Review. JMIR mHealth uHealth 2020, 8, e19237. [Google Scholar] [CrossRef]
- Sell, N.M.; Silver, J.K.; Rando, S.; Draviam, A.C.; Mina, D.S.; Qadan, M. Prehabilitation Telemedicine in Neoadjuvant Surgical Oncology Patients during the Novel COVID-19 Coronavirus Pandemic. Ann. Surg. 2020, 272, e81–e83. [Google Scholar] [CrossRef] [PubMed]
- Lambert, G.; Drummond, K.; Ferreira, V.; Carli, F. Teleprehabilitation during COVID-19 pandemic: The essentials of “what” and “how”. Support. Care Cancer 2021, 29, 551–554. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Patients’ Characteristics | N | % |
|---|---|---|
| Gender | ||
| Female | 32 | 48 |
| Male | 34 | 52 |
| Ethnicity | ||
| Asian or Asian British: Any other Asian background | 1 | 2 |
| Black, African, Caribbean, or Black British: Caribbean | 2 | 3 |
| White: Any other White background | 2 | 3 |
| White: English, Welsh, Scottish, Northern Irish or British | 61 | 92 |
| Specialty | ||
| Colorectal | 41 | 62 |
| Breast | 7 | 11 |
| Lung | 3 | 4 |
| Urology | 15 | 23 |
| Treatment | ||
| Chemo and/or radiotherapy | 7 | 11 |
| Surgery | 54 | 82 |
| Chemo and surgery | 5 | 7 |
| Duration of prehabilitation | ||
| <2 weeks | 5 | 8 |
| 2–4 weeks | 27 | 41 |
| 4–6 weeks | 12 | 18 |
| 6–8 weeks | 3 | 5 |
| ≥8 weeks | 19 | 29 |
| Counselling | ||
| Accepted | 13 | 20 |
| Declined | 53 | 80 |
| Alcohol intake | ||
| ≤14 units per week | 52 | 79 |
| >14 units per week | 14 | 21 |
| Alcohol moderation referral | ||
| Accepted | 0 | 0 |
| Declined | 14 * | 100 |
| Smoker | ||
| No | 60 | 91 |
| Yes | 6 | 9 |
| Smoking cessation referral | ||
| Accepted | 2 | 33 |
| Declined | 4 | 67 |
| High-risk of malnutrition | ||
| Yes | 3 | 5 |
| No | 63 | 95 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, F.; Rotimi, O.; Laza-Cagigas, R.; Rampal, T. The Feasibility and Effects of a Telehealth-Delivered Home-Based Prehabilitation Program for Cancer Patients during the Pandemic. Curr. Oncol. 2021, 28, 2248-2259. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol28030207
Wu F, Rotimi O, Laza-Cagigas R, Rampal T. The Feasibility and Effects of a Telehealth-Delivered Home-Based Prehabilitation Program for Cancer Patients during the Pandemic. Current Oncology. 2021; 28(3):2248-2259. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol28030207
Chicago/Turabian StyleWu, Fiona, Oloruntobi Rotimi, Roberto Laza-Cagigas, and Tarannum Rampal. 2021. "The Feasibility and Effects of a Telehealth-Delivered Home-Based Prehabilitation Program for Cancer Patients during the Pandemic" Current Oncology 28, no. 3: 2248-2259. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol28030207