SOX2 and Bcl-2 as a Novel Prognostic Value in Hepatocellular Carcinoma Progression

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Tissue Samples
2.2. Total RNA Extraction and cDNA Synthesis
2.3. Gene Expression Analysis Using qRT-PCR
2.4. Statistical Analysis
3. Results
3.1. Demographic and Clinical Characteristics of the Patients
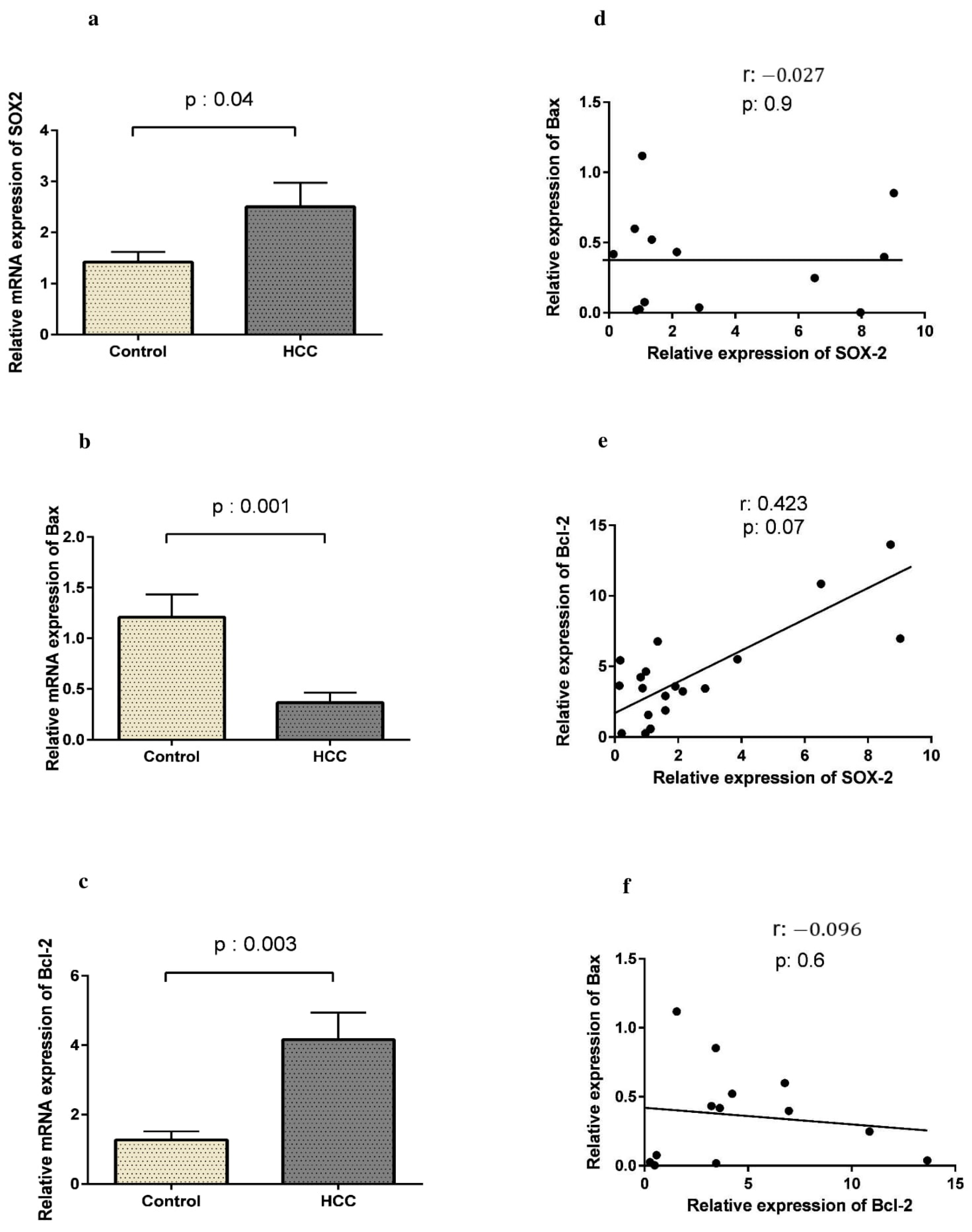
3.2. SOX2 Is Up-Regulated in HCC Along with Bcl-2
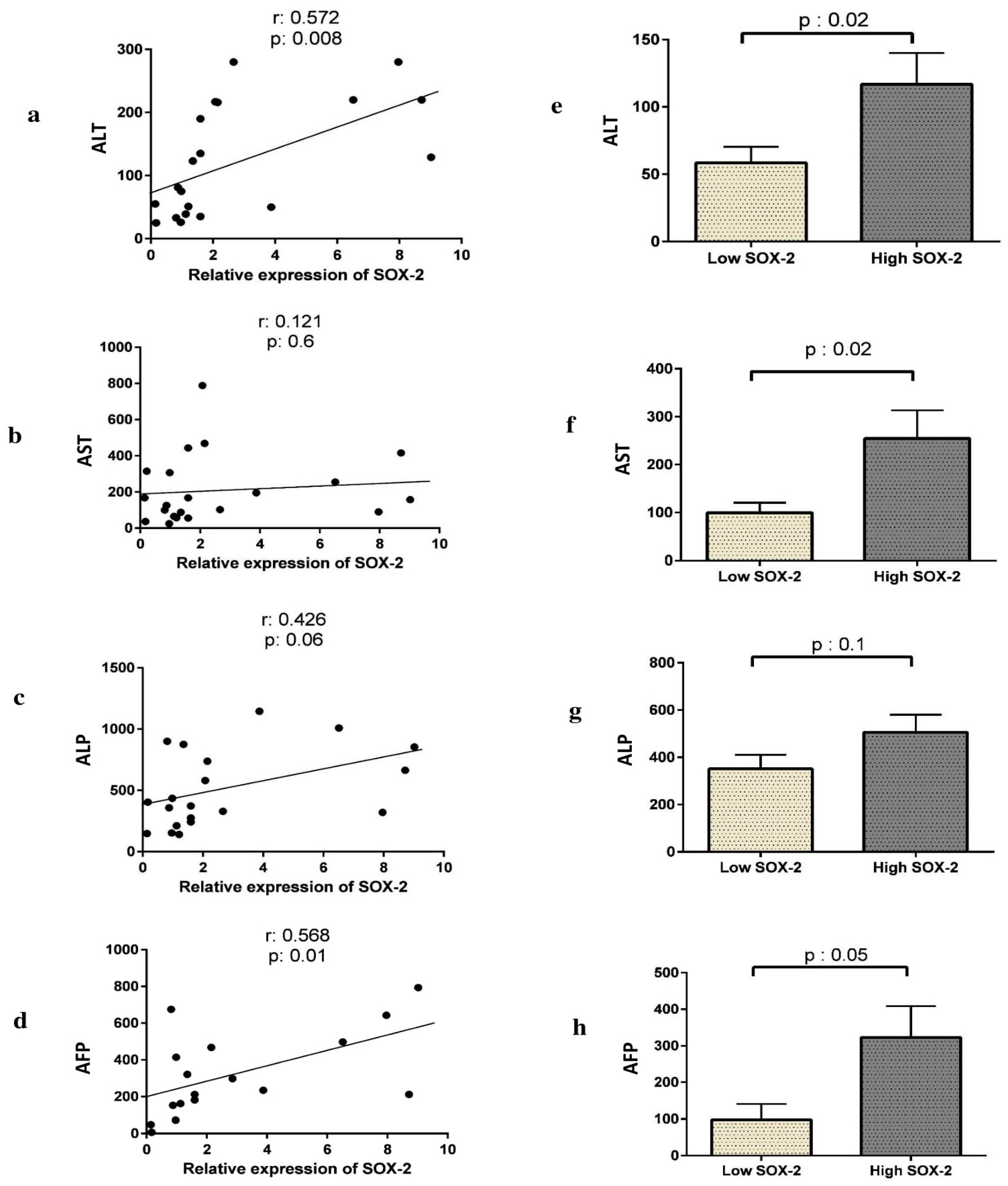
3.3. The Expression of SOX2, Bax, or Bcl-2 Correlates with Liver Enzyme Activity and AFP Levels in HCC Patients
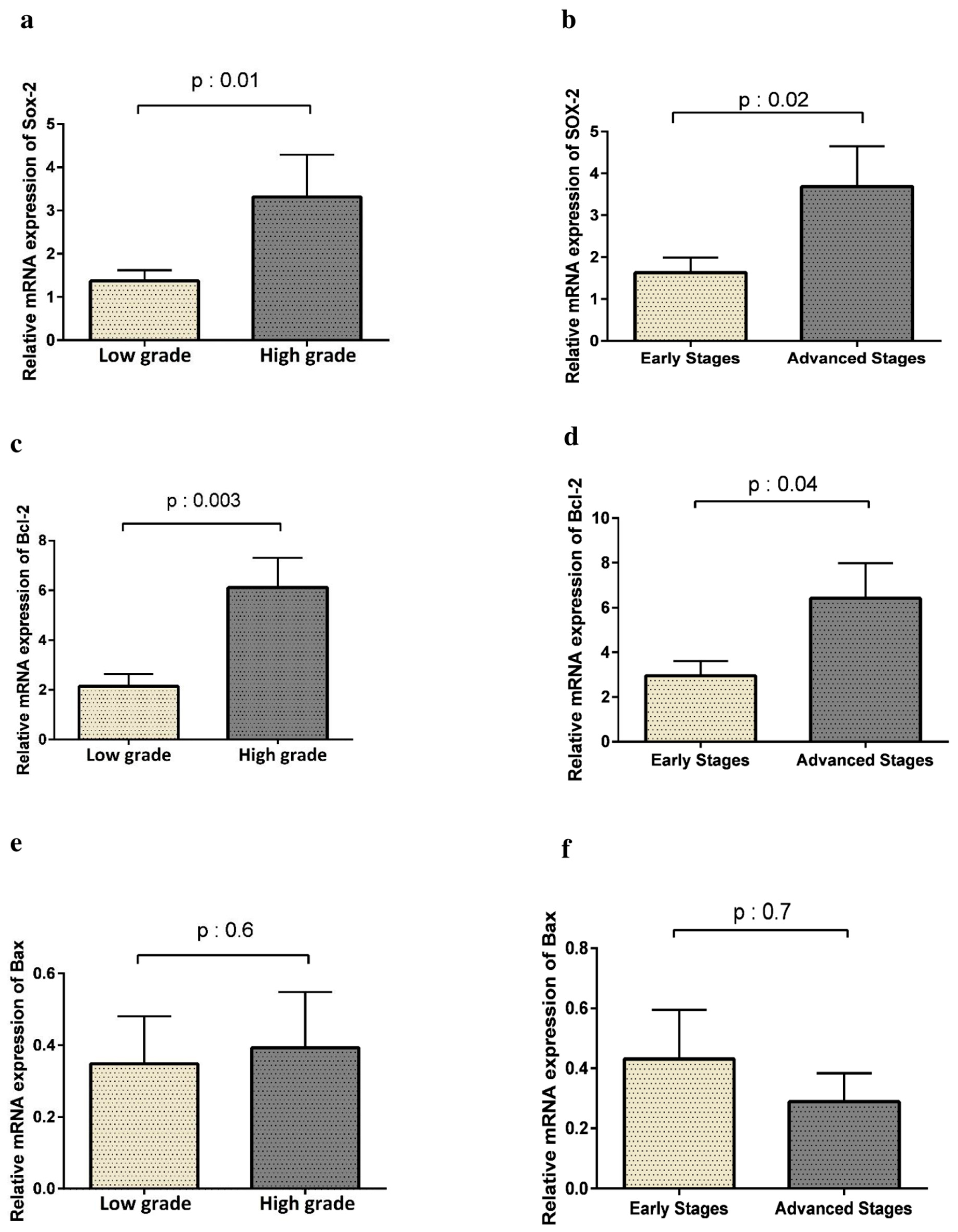
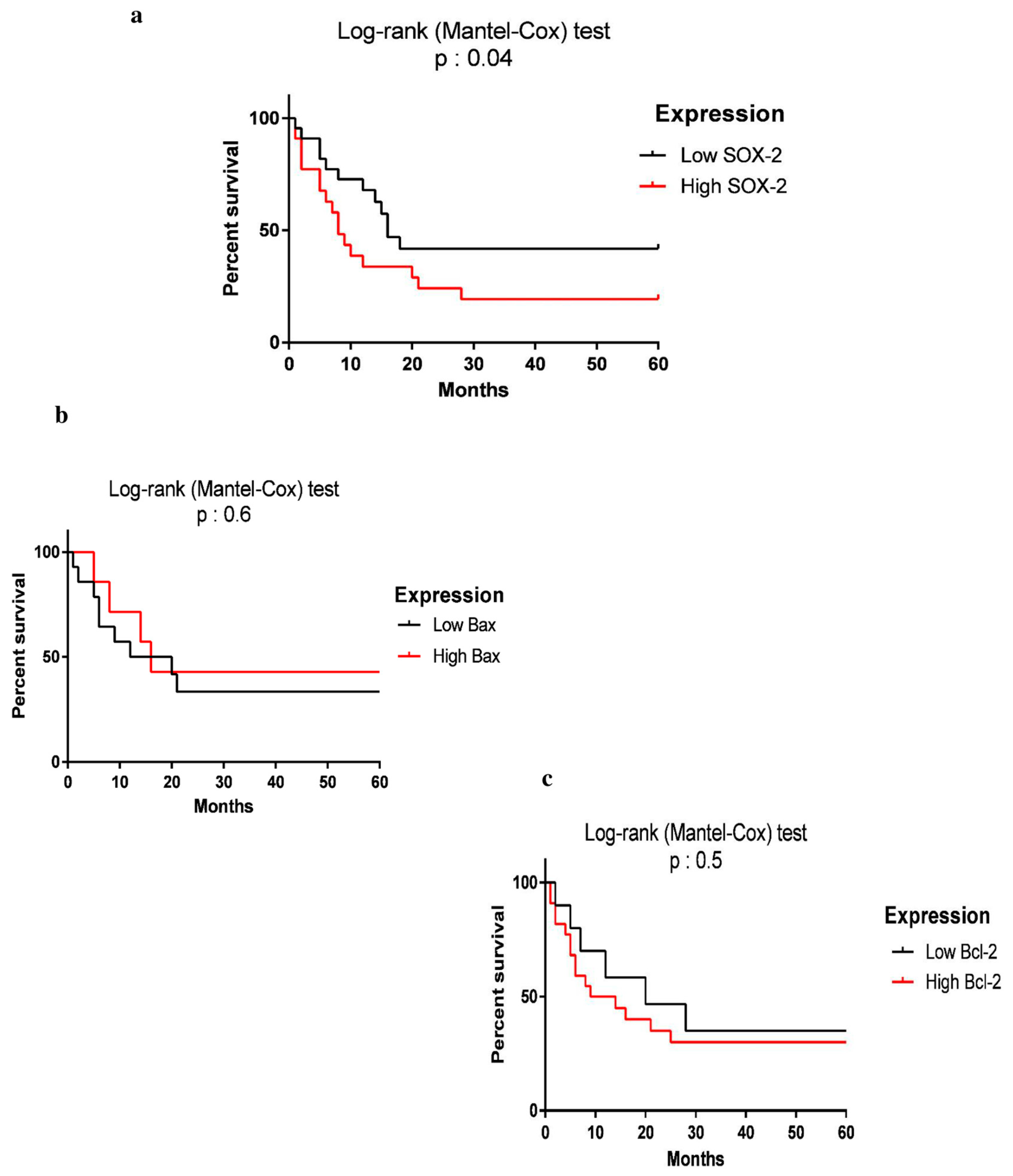
3.4. SOX2 Expression Is Correlated with Tumor Progression and Lower Survival Rate
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Avila, M.A.; Berasain, C.; Sangro, B.; Prieto, J. New therapies for hepatocellular carcinoma. Oncogene 2006, 25, 3866–3884. [Google Scholar] [CrossRef] [Green Version]
- Ali, N.; Allam, H.; May, R.; Sureban, S.M.; Bronze, M.S.; Bader, T.; Umar, S.; Anant, S.; Houchen, C.W. Hepatitis C virus-induced cancer stem cell-like signatures in cell culture and murine tumor xenografts. J. Virol. 2011, 85, 12292–12303. [Google Scholar] [CrossRef] [Green Version]
- Assadollahi, V.; Gholami, M.; Zendedel, A.; Afsartala, Z.; Jahanmardi, F. Comparison of Oct4, Sox2 and Nanog Expression in Pancreatic Cancer Cell Lines and Human Pancreatic Tumor. Zahedan J. Res. Med. Sci. 2015, 17, e5186. [Google Scholar] [CrossRef] [Green Version]
- Sun, C.; Sun, L.; Li, Y.; Kang, X.; Zhang, S.; Liu, Y. Sox2 expression predicts poor survival of hepatocellular carcinoma patients and it promotes liver cancer cell invasion by activating Slug. Med. Oncol. 2013, 30, 503. [Google Scholar] [CrossRef] [PubMed]
- Ma, S.; Chan, K.W.; Hu, L.; Lee, T.K.W.; Wo, J.Y.H.; Ng, I.O.L.; Zheng, B.J.; Guan, X.Y. Identification and characterization of tumorigenic liver cancer stem/progenitor cells. Gastroenterology 2007, 132, 2542–2556. [Google Scholar] [CrossRef]
- Leis, O.; Eguiara, A.; Lopez-Arribillaga, E.; Alberdi, M.; Hernandez-Garcia, S.; Elorriaga, K.; Pandiella, A.; Rezola, R.; Martin, A. Sox2 expression in breast tumours and activation in breast cancer stem cells. Oncogene 2012, 31, 1354–1365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yin, C.; Lin, Y.; Zhang, X.; Chen, Y.X.; Zeng, X.; Yue, H.Y.; Hou, J.L.; Deng, X.; Zhang, J.P.; Han, Z.G. Differentiation therapy of hepatocellular carcinoma in mice with recombinant adenovirus carrying hepatocyte nuclear factor-4α gene. Hepatology 2008, 48, 1528–1539. [Google Scholar] [CrossRef]
- Jung, K.; Wang, P.; Gupta, N.; Gopal, K.; Wu, F.; Ye, X.; Alshareef, A.; Bigras, G.; McMullen, T.P.; Abdulkarim, B.S. Profiling gene promoter occupancy of Sox2 in two phenotypically distinct breast cancer cell subsets using chromatin immunoprecipitation and genome-wide promoter microarrays. Breast Cancer Res. 2014, 16, 470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, F.; Ye, X.; Wang, P.; Jung, K.; Wu, C.; Douglas, D.; Kneteman, N.; Bigras, G.; Ma, Y.; Lai, R. Sox2 suppresses the invasiveness of breast cancer cells via a mechanism that is dependent on Twist1 and the status of Sox2 transcription activity. BMC Cancer 2013, 13, 317. [Google Scholar] [CrossRef] [Green Version]
- Yu, B.; Cai, H.; Xu, Z.; Xu, T.; Zou, Q.; Gu, M. Expressions of stem cell transcription factors Nanog and Oct4 in renal cell carcinoma tissues and clinical significance. Artif. Cells Nanomed. Biotechnol. 2016, 44, 1818–1823. [Google Scholar] [CrossRef] [Green Version]
- Wang, Q.; He, W.; Lu, C.; Wang, Z.; Wang, J.; Giercksky, K.E.; Nesland, J.M.; Suo, Z. Oct3/4 and Sox2 are significantly associated with an unfavorable clinical outcome in human esophageal squamous cell carcinoma. Anticancer Res. 2009, 29, 1233–1241. [Google Scholar]
- Rassouli, F.B.; Matin, M.M.; Bahrami, A.R.; Ghaffarzadegan, K.; Sisakhtnezhad, S.; Cheshomi, H.; Abbasi, F. SOX2 expression in gastrointestinal cancers of Iranian patients. Int. J. Biol. Markers 2014, 30, e315–e320. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Ji, X.; Chen, J.; Yan, D.; Zhang, Z.; Wang, Q.; Xi, X.; Feng, Y. SOX2 enhances the migration and invasion of ovarian cancer cells via Src kinase. PLoS ONE 2014, 9, e99594. [Google Scholar]
- Osman, N.A.; Khalil, A.I.; Yousef, R.K. The Clinical and Prognostic Implications of Pluripotent Stem Cell Markers Expression and Their Correlation with the WNT signal pathway in Hepatocellular Carcinoma. Asian Pac. J. Cancer Prev. 2020, 21, 2961–2970. [Google Scholar] [CrossRef]
- Xia, Y.; Tang, G.; Chen, Y.; Wang, C.; Guo, M.; Xu, T.; Zhao, M.; Zhou, Y. Tumor-targeted delivery of siRNA to silence Sox2 gene expression enhances therapeutic response in hepatocellular carcinoma. Bioact. Mater. 2021, 6, 1330–1340. [Google Scholar] [CrossRef]
- Liu, H.; Zhang, L.; Chen, S.; Wang, Z.; Huang, F.; Wang, D. The role and significance of Bcl-2 and Bax in the hepatic carcinoma. Int. J. Morphol 2012, 30, 1466–1473. [Google Scholar]
- Guo, X.-Z.; Shao, X.-D.; Liu, M.-P.; Xu, J.-H.; Ren, L.-N.; Zhao, J.-J.; Li, H.-Y.; Wang, D. Effect of bax, bcl-2 and bcl-xL on regulating apoptosis in tissues of normal liver and hepatocellular carcinoma. World J. Gastroenterol. 2002, 8, 1059. [Google Scholar] [CrossRef]
- Do Seon Song, S.H.B. Changes of guidelines diagnosing hepatocellular carcinoma during the last ten-year period. Clin. Mol. Hepatol. 2012, 18, 258. [Google Scholar] [CrossRef]
- Wittekind, C. Pitfalls in der Klassifikation von Lebertumoren. Der. Pathol. 2006, 27, 289–293. [Google Scholar] [CrossRef]
- Subramaniam, S.; Kelley, R.K.; Venook, A.P. A review of hepatocellular carcinoma (HCC) staging systems. Chin. Clin. Oncol. 2013, 2, 33. [Google Scholar] [CrossRef] [PubMed]
- Barros-Oliveira, M.d.C.; Costa-Silva, D.R.; Campos-Verdes, L.C.; Pereira, R.d.O.; Silva, R.A.; Moura-Borges, P.d.T.; Sousa, E.B.; Pinho-Sobral, A.L.; Lopes-Costa, P.V.; Dos Santos, A.R.; et al. CYP19A1 gene expression in the peripheral blood of Brazilian women with breast cancer relapse. BMC Cancer 2020, 20, 480. [Google Scholar] [CrossRef] [PubMed]
- Basati, G.; Mohammadpour, H.; Razavi, A.E. Association of high expression levels of SOX2, NANOG, and OCT4 in gastric cancer tumor tissues with progression and poor prognosis. J. Gastrointest. Cancer 2020, 51, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Hussenet, T.; Dali, S.; Exinger, J.; Monga, B.; Jost, B.; Dembelé, D.; Martinet, N.; Thibault, C.; Huelsken, J.; Brambilla, E.; et al. SOX2 is an oncogene activated by recurrent 3q26. 3 amplifications in human lung squamous cell carcinomas. PLoS ONE 2010, 5, e8960. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruiz, G.; Valencia-González, H.A.; Pérez-Montiel, D.; Muñoz, F.; Ocadiz-Delgado, R.; Fernández-Retana, J.; Pérez-Plasencia, C.; Reséndis-Antonio, O.; Gariglio, P.; García-Carrancá, A. Genes Involved in the Transcriptional Regulation of Pluripotency Are Expressed in Malignant Tumors of the Uterine Cervix and Can Induce Tumorigenic Capacity in a Nontumorigenic Cell Line. Stem Cells Int. 2019, 2019, 7683817. [Google Scholar] [CrossRef]
- Annovazzi, L.; Mellai, M.; Caldera, V.; Valente, G.; Schiffer, D. SOX2 expression and amplification in gliomas and glioma cell lines. Cancer Genom. Proteom. 2011, 8, 139–147. [Google Scholar]
- Herreros-Villanueva, M.; Zhang, J.; Koenig, A.; Abel, E.; Smyrk, T.C.; Bamlet, W.; De Narvajas, A.A.; Gomez, T.; Simeone, D.; Bujanda, L. SOX2 promotes dedifferentiation and imparts stem cell-like features to pancreatic cancer cells. Oncogenesis 2013, 2, e61. [Google Scholar] [CrossRef]
- Boumahdi, S.; Driessens, G.; Lapouge, G.; Rorive, S.; Nassar, D.; Le Mercier, M.; Delatte, B.; Caauwe, A.; Lenglez, S.; Nkusi, E. SOX2 controls tumour initiation and cancer stem-cell functions in squamous-cell carcinoma. Nature 2014, 511, 246–250. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Qin, B.; Li, F.; Xu, S.; Wang, S.; Li, L. Clinicopathological significance of Sox2 expression in patients with breast cancer: A meta-analysis. Int. J. Clin. Exp. Med. 2015, 8, 22382. [Google Scholar] [PubMed]
- Chen, Y.; Shi, L.; Zhang, L.; Li, R.; Liang, J.; Yu, W.; Sun, L.; Yang, X.; Wang, Y.; Zhang, Y.; et al. The molecular mechanism governing the oncogenic potential of SOX2 in breast cancer. J. Biol. Chem. 2008, 283, 17969–17978. [Google Scholar] [CrossRef] [Green Version]
- Song, K.; Hao, J.; Ge, Z.; Chen, P. Clinical and Survival Impact of Sex-Determining Region Y-Box 2 in Colorectal Cancer: An Integrated Analysis of the Immunohistochemical Study and Bioinformatics Analysis. J. Oncol. 2020, 2020, 3761535. [Google Scholar] [CrossRef]
- Liu, K.; Lin, B.; Zhao, M.; Yang, X.; Chen, M.; Gao, A.; Liu, F.; Que, J.; Lan, X. The multiple roles for Sox2 in stem cell maintenance and tumorigenesis. Cell. Signal. 2013, 25, 1264–1271. [Google Scholar] [CrossRef] [Green Version]
- Liu, L.; Liu, C.; Zhang, Q.; Shen, J.; Zhang, H.; Shan, J.; Duan, G.; Guo, D.; Chen, X.; Cheng, J. SIRT1-mediated transcriptional regulation of SOX2 is important for self-renewal of liver cancer stem cells. Hepatology 2016, 64, 814–827. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wuebben, E.L.; Rizzino, A. The dark side of SOX2: Cancer-a comprehensive overview. Oncotarget 2017, 8, 44917. [Google Scholar] [CrossRef] [Green Version]
- Conway, K.; Edmiston, S.N.; Tse, C.-K.; Bryant, C.; Kuan, P.F.; Hair, B.Y.; Parrish, E.A.; May, R.; Swift-Scanlan, T. Racial variation in breast tumor promoter methylation in the Carolina Breast Cancer Study. Cancer Epidemiol. Prev. Biomark. 2015, 24, 921–930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stretch, C.; Khan, S.; Asgarian, N.; Eisner, R.; Vaisipour, S.; Damaraju, S.; Graham, K.; Bathe, O.F.; Steed, H.; Greiner, R.; et al. Effects of sample size on differential gene expression, rank order and prediction accuracy of a gene signature. PLoS ONE 2013, 8, e65380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, X.; Meng, J.; Xu, H.; Niu, J. Alpha-fetoprotein to transaminase ratio is related to higher diagnostic efficacy for hepatocellular carcinoma. Medicine 2019, 98, e15414. [Google Scholar] [CrossRef]
- Ding, Y.; Liu, K.; Xu, Y.; Zhao, Q.; Lou, S.; Xiang, X.; Yan, L.; Cao, Z.; Xie, Q.; Zhu, C.; et al. Combination of inflammatory score/liver function and AFP improves the diagnostic accuracy of HBV-related hepatocellular carcinoma. Cancer Med. 2020, 9, 3057–3069. [Google Scholar] [CrossRef] [Green Version]
- Kotsafti, A.; Farinati, F.; Cardin, R.; Cillo, U.; Nitti, D.; Bortolami, M. Autophagy and apoptosis-related genes in chronic liver disease and hepatocellular carcinoma. BMC Gastroenterol. 2012, 12, 118. [Google Scholar] [CrossRef] [Green Version]
- Garcia, E.; Lawson, D.; Cotsonis, G.; Cohen, C. Hepatocellular carcinoma and markers of apoptosis (bcl-2, bax, bcl-x): Prognostic significance. Appl. Immunohistochem. Mol. Morphol. 2002, 10, 210–217. [Google Scholar] [CrossRef]
- Moul, J.W.; Bettencourt, M.-C.; Sesterhenn, I.A.; Mostofi, F.; McLeod, D.G.; Srivastava, S.; Bauer, J.J. Protein expression of p53, bcl-2, and KI-67 (MIB-1) as prognostic biomarkers in patients with surgically treated, clinically localized prostate cancer. Surgery 1996, 120, 159–167. [Google Scholar] [CrossRef]
- Lohmann, C.M.; League, A.A.; Clark, W.S.; Lawson, D.; DeRose, P.B.; Cohen, C. Bcl-2: Bax and Bcl-2: Bcl-x ratios by image cytometric quantitation of immunohistochemical expression in ovarian carcinoma: Correlation with prognosis. Cytom. Part A 2000, 42, 61–66. [Google Scholar] [CrossRef]
- Chou, Y.T.; Lee, C.C.; Hsiao, S.H.; Lin, S.E.; Lin, S.C.; Chung, C.H.; Chung, C.H.; Kao, Y.R.; Wang, Y.H.; Chen, C.T.; et al. The emerging role of SOX2 in cell proliferation and survival and its crosstalk with oncogenic signaling in lung cancer. Stem Cells 2013, 31, 2607–2619. [Google Scholar] [CrossRef] [PubMed]
- Walton, M.; Whysong, D.; O’connor, P.; Hockenbery, D.; Korsmeyer, S.; Kohn, K. Constitutive expression of human Bcl-2 modulates nitrogen mustard and camptothecin induced apoptosis. Cancer Res. 1993, 53, 1853–1861. [Google Scholar]
- Ikeguchi, M.; Hirooka, Y.; Kaibara, N. Quantitative analysis of apoptosis-related gene expression in hepatocellular carcinoma. Cancer 2002, 95, 1938–1945. [Google Scholar] [CrossRef] [PubMed]
- Williams, N.G.; Roberts, T.M. Signal transduction pathways involving the Raf proto-oncogene. Cancer Metastasis Rev. 1994, 13, 105–116. [Google Scholar] [CrossRef]
- Tomasson, M.H. Cancer stem cells: A guide for skeptics. J. Cell. Biochem. 2009, 106, 745–749. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Yang, Y.; Xing, D. Bcl-2 and Bcl-xL play important roles in the crosstalk between autophagy and apoptosis. FEBS J. 2011, 278, 403–413. [Google Scholar] [CrossRef] [PubMed]
- Chung, J.H.; Jung, H.R.; Jung, A.R.; Lee, Y.C.; Kong, M.; Lee, J.-S.; Eun, Y.-G. SOX2 activation predicts prognosis in patients with head and neck squamous cell carcinoma. Sci. Rep. 2018, 8, 1677. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saigusa, S.; Tanaka, K.; Toiyama, Y.; Yokoe, T.; Okugawa, Y.; Ioue, Y.; Miki, C.; Kusunoki, M. Correlation of CD133, OCT4, and SOX2 in rectal cancer and their association with distant recurrence after chemoradiotherapy. Ann. Surg. Oncol. 2009, 16, 3488–3498. [Google Scholar] [CrossRef]
- Lu, Y.; Futtner, C.; Rock, J.R.; Xu, X.; Whitworth, W.; Hogan, B.L.; Onaitis, M.W. Evidence that SOX2 overexpression is oncogenic in the lung. PLoS ONE 2010, 5, e11022. [Google Scholar] [CrossRef]
- Han, S.; Huang, T.; Wu, X.; Wang, X.; Liu, S.; Yang, W.; Shi, Q.; Li, H.; Hou, F. Prognostic value of CD133 and SOX2 in advanced cancer. J. Oncol. 2019, 2019, 3905817. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Wang, J.; Xu, Z.; Ahmad, A.; Li, E.; Wang, Y.; Qin, S.; Wang, Q. Expression of sox2 and oct4 and their clinical significance in human non-small-cell lung cancer. Int. J. Mol. Sci. 2012, 13, 7663–7675. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; Huang, Y.; Huang, Y.; Chen, J.; Wang, S.; Zhou, J. The prognostic value of SOX2 expression in non-small cell lung cancer: A meta-analysis. PLoS ONE 2013, 8, e71140. [Google Scholar] [CrossRef]
- Javaeed, A.; Ghauri, S.K. Metastatic potential and prognostic significance of SOX2: A meta-analysis. World J. Clin. Oncol. 2019, 10, 234. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.W.; Cho, H.; Choi, C.H.; Ylaya, K.; Chung, J.-Y.; Kim, J.-H.; Hewitt, S.M. Clinical significance of OCT4 and SOX2 protein expression in cervical cancer. BMC Cancer 2015, 15, 1015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamashita, T.; Kaneko, S. Orchestration of hepatocellular carcinoma development by diverse liver cancer stem cells. J. Gastroenterol. 2014, 49, 1105–1110. [Google Scholar] [CrossRef] [PubMed]
- Novak, D.; Hüser, L.; Elton, J.J.; Umansky, V.; Altevogt, P.; Utikal, J. SOX2 in development and cancer biology. Semin. Cancer Biol. 2019, 67, 74–82. [Google Scholar] [CrossRef]
- Hu, Y.; Fu, L. Targeting cancer stem cells: A new therapy to cure cancer patients. Am. J. Cancer Res. 2012, 2, 340. [Google Scholar] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Target Gene | Sequence (5′–3′) | Accession Number | Amplicon Size (bps) | |
|---|---|---|---|---|
| SOX2 | Forward Reverse | TTGTCGGAGACGGAGAAG GGCAGCGTGTACTTATCC | NM_003106.4 | 140 |
| Bax | Forward Reverse | TGGCAGCTGACATGTTTTCTGAC TCACCCAACCACCCTGGTCTT | NM_001291430.2 | 195 |
| Bcl-2 | Forward Reverse | TCGCCCTGTGGATGACTGA CAGAGACAGCCAGGAGAAATCA | NM_000633.3 | 134 |
| GAPDH | Forward Reverse | GGTGGTCTCCTCTGACTTCAACA GTTGCTGTAGCAAATTCGTTGT | NM_001357943.2 | 126 |
| Parameter | HCC (n = 53) | Control (n = 44) | p-Value |
|---|---|---|---|
| Age | 55.43 ± 1.870 | 50.53 ± 1.709 | 0.06 |
| Gender | 0.819 | ||
| Male | 40 (75.47%) | 25(56.8%) | |
| Female | 13 (24.53%) | 19 (43.2%) | |
| AST a (IU/L) | 197 ± 34.04 | 79.8 ± 41.97 | 0.039 * |
| ALT b (IU/L) | 93.53 ± 17.04 | 41.72 ± 10.26 | 0.0407 * |
| ALP c (IU/L) | 565.8 ± 107.0 | 264.6 ± 38.42 | 0.05 * |
| Triglyceride (mg/dL) | 107.7 ± 31.0 | 141.8 ± 30.78 | 0.459 |
| Cholesterol (mg/dL) | 199.5 ± 61.87 | 180 ± 18.64 | 0.7882 |
| HDL d (mg/dL) | 41.83 ± 6.237 | 36.5 ± 7.762 | 0.6055 |
| LDL e (mg/dL) | 171.4 ± 77.95 | 93.67 ± 21.88 | 0.4877 |
| PLT f (×1000/mm3) | 172.4 ± 13.11 | 216.8 ± 24.11 | 0.0842 |
| Parameter | PhaseI (%) | PhaseII (%) | PhaseIII (%) | PhaseIV (%) |
|---|---|---|---|---|
| Tumor grade | 35.8 | 35.9 | 20.75 | 7.55 |
| Clinical stage | 60.41 | 8.33 | 4.2 | 27.06 |
| Parameter | HBV-Related HCC | HCV-Related HCC | ||||
|---|---|---|---|---|---|---|
| HBV-Positive (n = 17) | HBV-Negative (n = 26) | p-Value | HCV-Positive (n = 7) | HCV-Negative (n = 36) | p-Value | |
| SOX2 | 2.608 ± 3.049 | 2.751± 2.664 | 0.9 | 1.744± 1.539 | 2.882 ± 2.911 | 0.4 |
| Bcl-2 | 5.703 ± 4.849 | 3.336 ± 2.220 | 0.4 | 6.162 ± 4.845 | 3.482 ± 2.649 | 0.1 |
| Bax | 0.284 ± 0.237 | 0.501 ± 0.430 | 0.3 | 0.705 ± 0.371 | 0.371 ± 0.380 | 0.2 |
| AST a | 218.3 ± 193.4 | 190.5 ± 205.9 | 0.7 | 238.3 ± 212.0 | 208.5 ± 210.4 | 0.5 |
| ALT b | 87.80 ± 75.71 | 96.65 ± 113.6 | 0.8 | 69.50 ± 34.35 | 97.69 ± 106.3 | 0.7 |
| ALP c | 696.9 ± 897.7 | 466.7 ± 242.0 | 0.7 | 722.2 ± 368.5 | 532.9 ± 654.4 | 0.07 |
| AFP d | 415.7 ± 427.2 | 140.5 ± 204.2 | 0.1 | 195.0 ± 186.5 | 4906 ± 21244 | 0.5 |
| Survival | 9.308± 6.762 | 9.167 ± 8.140 | 0.8 | 8.500 ± 5.802 | 8.962 ± 7.681 | 0.8 |
| Correlation | Relative Expression of Bax | Relative Expression of Bcl-2 | ||
|---|---|---|---|---|
| p-Value | Correlation Coefficient | p-Value | Correlation Coefficient | |
| AST | 0.1 | −0.384 | 0.1 | 0.326 |
| ALT | 0.5 | −0.187 | 0.02 * | 0.486 |
| AFP | 0.03 * | 0.593 | 0.1 | 0.320 |
| ALP | 0.3 | −0.291 | 0.01 * | 0.537 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hosseini-khah, Z.; Babaei, M.R.; Tehrani, M.; Cucchiarini, M.; Madry, H.; Ajami, A.; Rakhshani, N.; Rafiei, A.; Nikbin, B. SOX2 and Bcl-2 as a Novel Prognostic Value in Hepatocellular Carcinoma Progression. Curr. Oncol. 2021, 28, 3015-3029. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol28040264
Hosseini-khah Z, Babaei MR, Tehrani M, Cucchiarini M, Madry H, Ajami A, Rakhshani N, Rafiei A, Nikbin B. SOX2 and Bcl-2 as a Novel Prognostic Value in Hepatocellular Carcinoma Progression. Current Oncology. 2021; 28(4):3015-3029. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol28040264
Chicago/Turabian StyleHosseini-khah, Zahra, Mohammad Reza Babaei, Mohsen Tehrani, Magali Cucchiarini, Henning Madry, Abolghasem Ajami, Nasser Rakhshani, Alireza Rafiei, and Behrooz Nikbin. 2021. "SOX2 and Bcl-2 as a Novel Prognostic Value in Hepatocellular Carcinoma Progression" Current Oncology 28, no. 4: 3015-3029. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol28040264