The Influence of Adjuvant Chemotherapy Dose Intensity on Five-Year Outcomes in Resected Colon Cancer: A Single Centre Retrospective Analysis

Abstract
:1. Introduction
2. Methods
Statistical Analysis
3. Results
3.1. Patient Characteristics
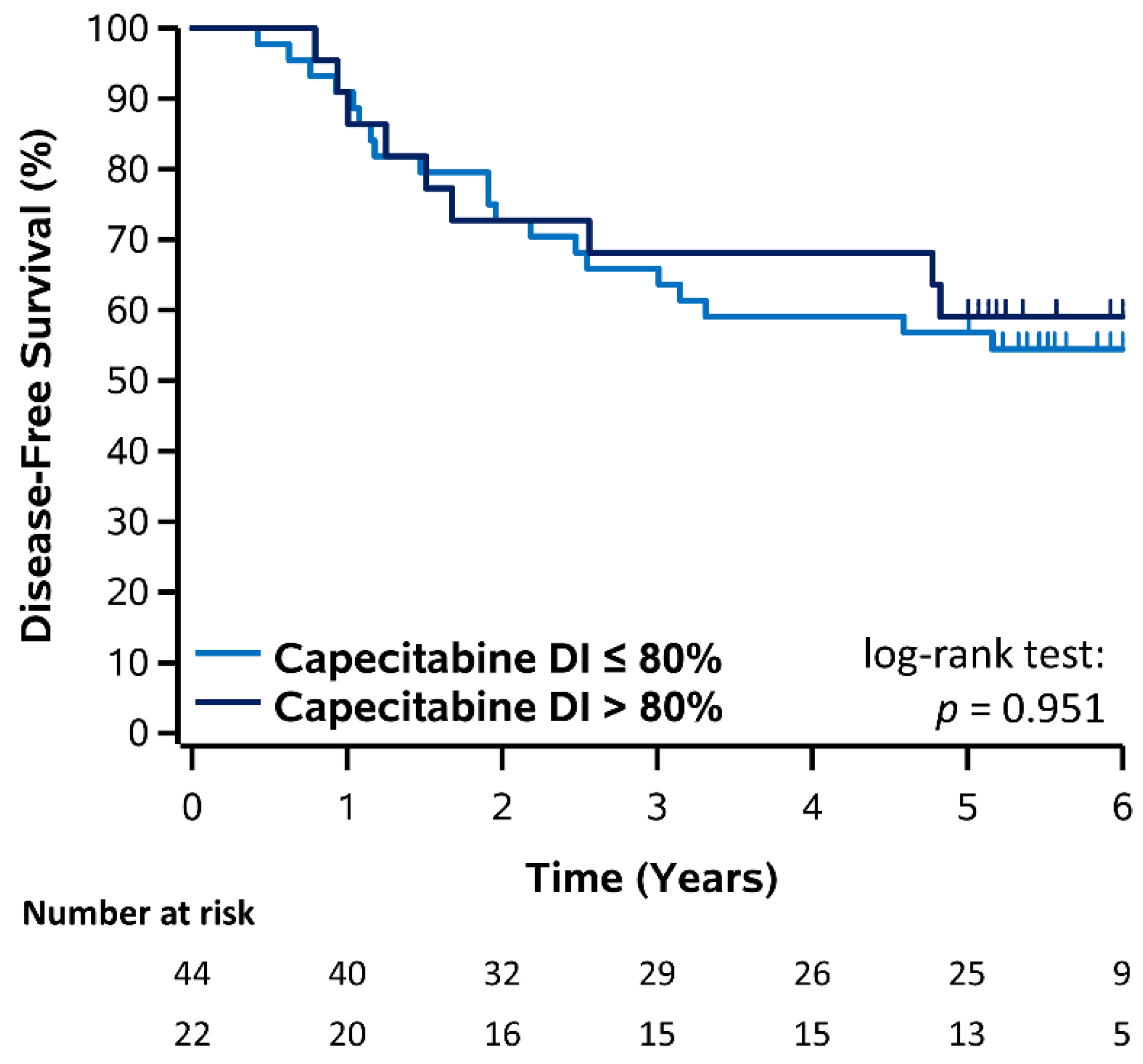
3.2. Disease-Free Survival
3.3. Overall Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Committee CCSA. Canadian Cancer Statistics 2019; Canadian Cancer Society: Toronto, ON, USA, 2019. [Google Scholar]
- Mph, K.D.M.; Nogueira, L.; Mariotto, A.B.; Rowland, J.H.; Yabroff, K.R.; Alfano, C.M.; Jemal, A.; Kramer, J.L.; Siegel, R.L. Cancer treatment and survivorship statistics, 2019. CA Cancer J. Clin. 2019, 69, 363–385. [Google Scholar]
- National Cancer Institute. SEER Cancer Statistics Factsheets: Colon and Rectum Cancer. 2013. Available online: http://seer.cancer.gov/statfacts/html/colorect.html (accessed on 12 June 2021).
- André, T.; Boni, C.; Mounedji-Boudiaf, L.; Navarro, M.; Tabernero, J.; Hickish, T.; Topham, C.; Zaninelli, M.; Clingan, P.; Bridgewater, J.; et al. Oxaliplatin, Fluorouracil, and Leucovorin as Adjuvant Treatment for Colon Cancer. N. Engl. J. Med. 2004, 350, 2343–2351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Investigators, I. Efficacy of adjuvant fluorouracil and folinic acid in colon cancer. Lancet 1995, 345, 939–944. [Google Scholar]
- Wong, S.L.; Ji, H.; Hollenbeck, B.K.; Morris, A.M.; Baser, O.; Birkmeyer, J.D. Hospital Lymph Node Examination Rates and Survival after Resection for Colon Cancer. JAMA 2007, 298, 2149–2154. [Google Scholar] [CrossRef]
- de Gramont, A.D.; Figer, A.; Seymour, M.; Homerin, M.; Hmissi, A.; Cassidy, J.; Boni, C.; Cortes-Funes, H.; Cervantes, A.; Freyer, G. Leucovorin and fluorouracil with or without oxaliplatin as first-line treatment in advanced colorectal cancer. J. Clin. Oncol. 2000, 18, 2938–2947. [Google Scholar] [CrossRef]
- Soveri, L.; Lamminmäki, A.; Hänninen, U.; Karhunen, M.; Bono, P.; Osterlund, P. Long-term neuropathy and quality of life in colorectal cancer patients treated with oxaliplatin containing adjuvant chemotherapy. Acta Oncol. 2019, 58, 398–406. [Google Scholar] [CrossRef] [Green Version]
- Goldberg, R.M.; Tabah-Fisch, I.; Bleiberg, H.; de Gramont, A.; Tournigand, C.; Andre, T.; Rothenberg, M.L.; Green, E.; Sargent, D.J. Pooled Analysis of Safety and Efficacy of Oxaliplatin Plus Fluorouracil/Leucovorin Administered Bimonthly in Elderly Patients with Colorectal Cancer. J. Clin. Oncol. 2006, 24, 4085–4091. [Google Scholar] [CrossRef]
- Neugut, A.I.; Matasar, M.; Wang, X.; McBride, R.; Jacobson, J.S.; Tsai, W.-Y.; Grann, V.R.; Hershman, D.L. Duration of Adjuvant Chemotherapy for Colon Cancer and Survival among the Elderly. J. Clin. Oncol. 2006, 24, 2368–2375. [Google Scholar] [CrossRef]
- Tournigand, C.; Cervantes, A.; Figer, A.; Lledo, G.; Flesch, M.; Buyse, M.; Mineur, L.; Carola, E.; Etienne, P.-L.; Rivera, F.; et al. OPTIMOX1: A Randomized Study of FOLFOX4 or FOLFOX7 with Oxaliplatin in a Stop-and-Go Fashion in Advanced Colorectal Cancer—A GERCOR Study. J. Clin. Oncol. 2006, 24, 394–400. [Google Scholar] [CrossRef] [Green Version]
- Morris, M.; Platell, C.; Fritschi, L.; Iacopetta, B. Failure to complete adjuvant chemotherapy is associated with adverse survival in stage III colon cancer patients. Br. J. Cancer 2007, 96, 701–707. [Google Scholar] [CrossRef] [Green Version]
- Vincent, M.D.; Breadner, D.; Soulieres, D.; Kerr, I.G.; Sanatani, M.; Kocha, W.; Klimo, P.; MacKenzie, M.J.; O’Connell, A.; Whiston, F.; et al. Phase II trial of capecitabine plus erlotinib versus capecitabine alone in patients with advanced colorectal cancer. Future Oncol. 2017, 13, 777–786. [Google Scholar] [CrossRef]
- Vincent, M.; Breadner, D.; Cripps, M.; Jonker, D.; Klimo, P.; Biagi, J.; Lam, W.; O’Connell, A.; Whiston, F.; Stitt, L.; et al. Phase I/II Trial of Dose-Reduced Capecitabine in Elderly Patients with Advanced Colorectal Cancer. Curr. Oncol. 2017, 24, 261–268. [Google Scholar] [CrossRef]
- Hryniuk, W.M. The importance of dose intensity in the outcome of chemotherapy. Important Adv. Oncol. 1988, 4, 121–141. [Google Scholar]
- Nakayama, G.; Tanaka, C.; Uehara, K.; Mashita, N.; Hayashi, N.; Kobayashi, D.; Kanda, M.; Yamada, S.; Fujii, T.; Sugimoto, H.; et al. The impact of dose/time modification in irinotecan- and oxaliplatin-based chemotherapies on outcomes in metastatic colorectal cancer. Cancer Chemother. Pharmacol. 2014, 73, 847–855. [Google Scholar] [CrossRef] [PubMed]
- Longo, D.L.; Duffey, P.; DeVita, V., Jr.; Wesley, M.; Hubbard, S.; Young, R. The calculation of actual or received dose intensity: A comparison of published methods. J. Clin. Oncol. 1991, 9, 2042–2051. [Google Scholar] [CrossRef] [PubMed]
- Hryniuk, W.; Bush, H. The importance of dose intensity in chemotherapy of metastatic breast cancer. J. Clin. Oncol. 1984, 2, 1281–1288. [Google Scholar] [CrossRef]
- Kwak, L.; Halpern, J.; Olshen, A.R.; Horning, S.J. Prognostic significance of actual dose intensity in diffuse large-cell lymphoma: Results of a tree-structured survival analysis. J. Clin. Oncol. 1990, 8, 963–977. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loibl, S.; Skacel, T.; Nekljudova, V.; Lück, H.J.; Schwenkglenks, M.; Brodowicz, T.; Zielinski, C.; Von Minckwitz, G. Evaluating the impact of Relative Total Dose Intensity (RTDI) on patients’ short and long-term outcome in taxane- and anthracycline-based chemotherapy of metastatic breast cancer—A pooled analysis. BMC Cancer 2011, 11, 131. [Google Scholar] [CrossRef] [Green Version]
- Luciani, A.; Bertuzzi, C.; Ascione, G.; Di Gennaro, E.; Bozzoni, S.; Zonato, S.; Ferrari, D.; Foa, P. Dose intensity correlate with survival in elderly patients treated with chemotherapy for advanced non-small cell lung cancer. Lung Cancer 2009, 66, 94–96. [Google Scholar] [CrossRef]
- Lyman, G.H. Impact of Chemotherapy Dose Intensity on Cancer Patient Outcomes. J. Natl. Compr. Cancer Netw. 2009, 7, 99–108. [Google Scholar] [CrossRef]
- Aspinall, S.L.; Good, C.B.; Zhao, X.; Cunningham, F.E.; Heron, B.B.; Geraci, M.; Passero, V.; Stone, R.A.; Smith, K.J.; Rogers, R.; et al. Adjuvant chemotherapy for stage III colon cancer: Relative dose intensity and survival among veterans. BMC Cancer 2015, 15, 62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ho, J.; Gill, S.; Woods, R.; Kennecke, H.F. Association of survival outcomes with dose intensity of adjuvant therapy (AT) with capecitabine for colorectal cancer (CRC). J. Clin. Oncol. 2010, 28, 3624. [Google Scholar] [CrossRef]
- Grothey, A.; Sobrero, A.F.; Shields, A.F.; Yoshino, T.; Paul, J.; Taieb, J.; Souglakos, J.; Shi, Q.; Kerr, R.; Labianca, R.; et al. Duration of Adjuvant Chemotherapy for Stage III Colon Cancer. N. Engl. J. Med. 2018, 378, 1177–1188. [Google Scholar] [CrossRef] [PubMed]
- Yoshino, T.; Yamanaka, T.; Oki, E.; Kotaka, M.; Manaka, D.; Eto, T.; Hasegawa, J.; Takagane, A.; Nakamura, M.; Kato, T. Efficacy and long-term peripheral sensory neuropathy of 3 vs. 6 months of oxaliplatin-based adjuvant chemotherapy for colon cancer: The ACHIEVE phase 3 randomized clinical trial. JAMA Oncol. 2019, 5, 1574–1581. [Google Scholar] [CrossRef]
- Schmoll, H.-J.; Twelves, C.; Sun, W.; O’Connell, M.J.; Cartwright, T.; McKenna, E.; Saif, M.; Lee, S.; Yothers, G.; Haller, D. Effect of adjuvant capecitabine or fluorouracil, with or without oxaliplatin, on survival outcomes in stage III colon cancer and the effect of oxaliplatin on post-relapse survival: A pooled analysis of individual patient data from four randomised controlled trials. Lancet Oncol. 2014, 15, 1481–1492. [Google Scholar] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | All Patients (n = 192) | Capecitabine (n = 66) | FOLFOX (n = 126) | p-Value |
|---|---|---|---|---|
| Gender—n (%) | 0.482 | |||
| Male | 98 (51.0) | 36 (54.6) | 62 (49.2) | |
| Female | 94 (49.0) | 30 (45.5) | 64 (50.8) | |
| Age—median (IQR) | 67.7 (60.5, 73.0) | 75.1 (71.7, 78.9) | 63.8 (57.5, 69.1) | <0.001 |
| Resection to discharge (days)—median (IQR) | 6 (5, 8) | 7 (6, 9) | 6 (4, 8) | 0.004 |
| Post-operative hospital re-admission—n (%) | 14 (7.3) | 8 (12.1) | 6 (4.8) | 0.080 |
| Surgery to medical oncology referral consult (days)—median (IQR) | 21 (14, 30) | 23 (15, 31) | 21 (13, 28) | 0.226 |
| Comorbidity: any—n (%) | 156 (81.3) | 59 (89.4) | 97 (77.0) | 0.036 |
| Perioperative complications—n (%) | 49 (25.5) | 25 (37.9) | 24 (19.1) | 0.005 |
| Pathological T stage—n (%) | 0.803 | |||
| T0 | 1 (0.5) | 0 (0) | 1 (0.8) | |
| T1 | 7 (3.7) | 2 (3.0) | 5 (4.0) | |
| T2 | 12 (6.3) | 3 (4.6) | 9 (7.1) | |
| T3 | 93 (48.4) | 36 (54.6) | 57 (45.2) | |
| T4 | 79 (41.2) | 25 (37.9) | 54 (42.9) | |
| Pathological N stage—n (%) | 0.605 | |||
| N0 | 30 (15.6) | 12 (18.2) | 18 (14.3) | |
| N1 | 111 (57.8) | 39 (59.1) | 72 (57.1) | |
| N2 | 51 (26.6) | 15 (22.7) | 36 (28.6) | |
| Status—n (%) | 0.083 | |||
| Alive with disease | 5 (2.6) | 2 (3.0) | 3 (2.4) | |
| Alive without disease | 129 (67.2) | 38 (57.6) | 91 (72.2) | |
| Death with disease | 43 (22.4) | 17 (25.8) | 26 (20.6) | |
| Death without disease | 15 (7.8) | 9 (13.6) | 6 (4.8) | |
| Death—n (%) | 58 (30.2) | 26 (39.4) | 32 (25.4) | 0.045 |
| Recurrence—n (%) | 59 (30.7) | 23 (34.9) | 36 (28.6) | 0.371 |
| Median follow-up (years)—median (95% CI) | 5.74 (5.52, 5.96) | 5.79 (5.46, 6.08) | 5.74 (5.45, 6.01) | 0.758 |
| 3-Year DFS (%) | 5-Year DFS (%) | Log-Rank p-Value | |||
| Dose Intensity | ≤80% | >80% | ≤80% | >80% | |
| Capecitabine | 65.9% | 68.2% | 56.8% | 59.1% | 0.951 |
| 5-FU | 80.3% | 75.3% | 67.4% | 72.9% | 0.753 |
| Oxaliplatin | 77.4% | 76.3% | 68.1% | 74.6% | 0.544 |
| 3-Year OS (%) | 5-Year OS (%) | Log-Rank p-Value | |||
| Dose Intensity | ≤80% | >80% | ≤80% | >80% | |
| Capecitabine | 81.8% | 77.3% | 68.2% | 63.6% | 0.881 |
| 5-FU | 87.7% | 85.9% | 74.8% | 77.6% | 0.700 |
| Oxaliplatin | 87.8% | 84.7% | 75.5% | 77.9% | 0.480 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lakkunarajah, S.; Breadner, D.A.; Zhang, H.; Yamanaka, E.; Warner, A.; Welch, S. The Influence of Adjuvant Chemotherapy Dose Intensity on Five-Year Outcomes in Resected Colon Cancer: A Single Centre Retrospective Analysis. Curr. Oncol. 2021, 28, 4031-4041. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol28050342
Lakkunarajah S, Breadner DA, Zhang H, Yamanaka E, Warner A, Welch S. The Influence of Adjuvant Chemotherapy Dose Intensity on Five-Year Outcomes in Resected Colon Cancer: A Single Centre Retrospective Analysis. Current Oncology. 2021; 28(5):4031-4041. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol28050342
Chicago/Turabian StyleLakkunarajah, Suganija, Daniel A. Breadner, Hanbo Zhang, Ellen Yamanaka, Andrew Warner, and Stephen Welch. 2021. "The Influence of Adjuvant Chemotherapy Dose Intensity on Five-Year Outcomes in Resected Colon Cancer: A Single Centre Retrospective Analysis" Current Oncology 28, no. 5: 4031-4041. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol28050342