Uncommon EGFR Compound Mutations in Non-Small Cell Lung Cancer (NSCLC): A Systematic Review of Available Evidence

 , ,
, ,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
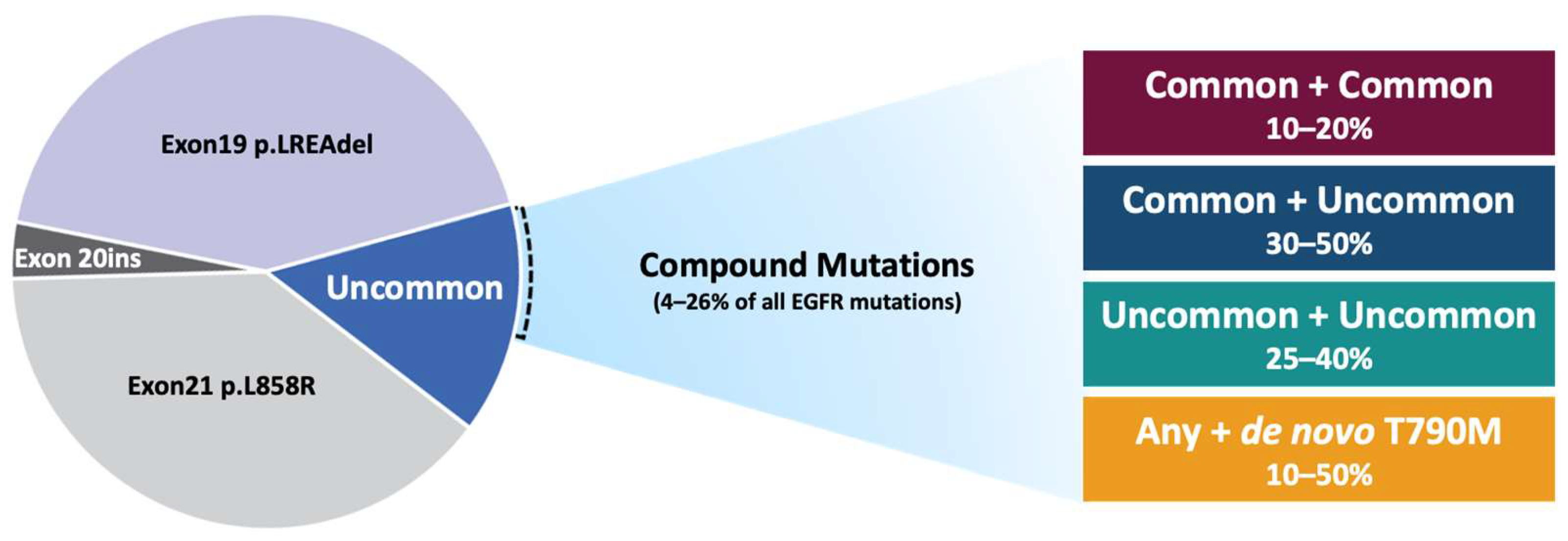
3.1. Prevalence and Distribution of EGFR Compound Mutations
3.2. Preclinical Data on EGFR Compound Mutations
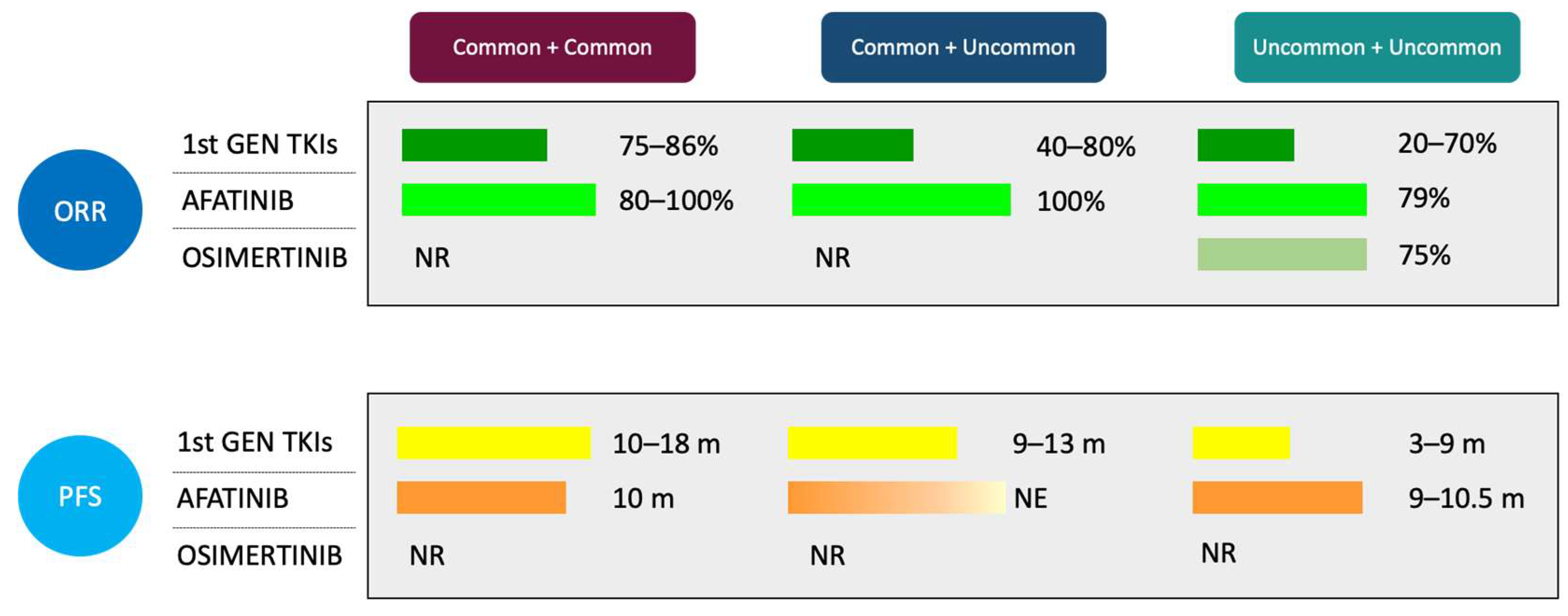
3.3. Clinical Outcomes of NSCLC Patients Harboring EGFR Compound Mutations
3.3.1. First-Generation EGFR-TKIs in Compound EGFR Mutations
3.3.2. Second-Generation EGFR-TKIs in Compound EGFR Mutations
3.3.3. Third-Generation EGFR TKIs in Compound EGFR Mutations
3.3.4. Exon 20 p.T790M EGFR Compound Mutations
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
References
- Yang, J.C.; Sequist, L.V.; Geater, S.L.; Tsai, C.M.; Mok, T.S.; Schuler, M.; Yamamoto, N.; Yu, C.J.; Ou, S.H.; Zhou, C.; et al. Clinical activity of afatinib in patients with advanced non-small-cell lung cancer harbouring uncommon EGFR mutations: A combined post-hoc analysis of LUX-Lung 2, LUX-Lung 3, and LUX-Lung 6. Lancet Oncol. 2015, 16, 830–838. [Google Scholar] [CrossRef]
- Cho, J.H.; Lim, S.H.; An, H.J.; Kim, K.H.; Park, K.U.; Kang, E.J.; Choi, Y.H.; Ahn, M.S.; Lee, M.H.; Sun, J.M.; et al. Osimertinib for Patients With Non-Small-Cell Lung Cancer Harboring Uncommon EGFR Mutations: A Multicenter, Open-Label, Phase II Trial (KCSG-LU15-09). J. Clin. Oncol. 2020, 38, 488–495. [Google Scholar] [CrossRef]
- Passaro, A.; Mok, T.; Peters, S.; Popat, S.; Ahn, M.-J.; de Marinis, F. Recent Advances on the Role of EGFR Tyrosine Kinase Inhibitors in the Management of NSCLC With Uncommon, Non Exon 20 Insertions, EGFR Mutations. J. Thorac. Oncol. 2020, 16, 764–773. [Google Scholar] [CrossRef] [PubMed]
- Tu, H.Y.; Ke, E.E.; Yang, J.J.; Sun, Y.L.; Yan, H.H.; Zheng, M.Y.; Bai, X.Y.; Wang, Z.; Su, J.; Chen, Z.H.; et al. A comprehensive review of uncommon EGFR mutations in patients with non-small cell lung cancer. Lung Cancer 2017, 114, 96–102. [Google Scholar] [CrossRef]
- Passaro, A.; de Marinis, F.; Tu, H.Y.; Laktionov, K.K.; Feng, J.; Poltoratskiy, A.; Zhao, J.; Tan, E.H.; Gottfried, M.; Lee, V.; et al. Afatinib in EGFR TKI-Naïve Patients with Locally Advanced or Metastatic EGFR Mutation-Positive Non-Small Cell Lung Cancer: A Pooled Analysis of Three Phase IIIb Studies. Front. Oncol. 2021, 11, 709877. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Syahruddin, E.; Wulandari, L.; Sri Muktiati, N.; Rima, A.; Soeroso, N.; Ermayanti, S.; Levi, M.; Hidajat, H.; Widjajahakim, G.; Utomo, A.R.H. Uncommon EGFR mutations in cytological specimens of 1,874 newly diagnosed Indonesian lung cancer patients. Lung Cancer 2018, 9, 25–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zaini, J.; Syahruddin, E.; Yunus, M.; Andarini, S.L.; Hudoyo, A.; Masykura, N.; Yasril, R.; Ridwanuloh, A.; Hidajat, H.; Nurwidya, F.; et al. Evaluation of PCR-HRM, RFLP, and direct sequencing as simple and cost-effective methods to detect common EGFR mutations in plasma cell-free DNA of non-small cell lung cancer patients. Cancer Rep. 2019, 2, e1159. [Google Scholar] [CrossRef] [PubMed]
- Jing, C.; Mao, X.; Wang, Z.; Sun, K.; Ma, R.; Wu, J.; Cao, H. Next-generation sequencing-based detection of EGFR, KRAS, BRAF, NRAS, PIK3CA, Her-2 and TP53 mutations in patients with non-small cell lung cancer. Mol. Med. Rep. 2018, 18, 2191–2197. [Google Scholar] [CrossRef]
- Namba, K.; Tomida, S.; Matsubara, T.; Takahashi, Y.; Kurihara, E.; Ogoshi, Y.; Yoshioka, T.; Takeda, T.; Torigoe, H.; Sato, H.; et al. Application of amplicon-based targeted sequencing with the molecular barcoding system to detect uncommon minor EGFR mutations in patients with treatment-naïve lung adenocarcinoma. BMC Cancer 2019, 19, 175. [Google Scholar] [CrossRef] [PubMed]
- Mao, L.; Zhao, W.; Li, X.; Zhang, S.; Zhou, C.; Zhou, D.; Ou, X.; Xu, Y.; Tang, Y.; Ou, X.; et al. Mutation Spectrum of EGFR from 21,324 Chinese Patients with Non-Small Cell Lung Cancer (NSCLC) Successfully Tested by Multiple Methods in a CAP-Accredited Laboratory. Pathol. Oncol. Res. 2021, 27, 602726. [Google Scholar] [CrossRef]
- Zhou, Y.; Ge, F.; Du, Y.; Li, Q.; Cai, J.; Liu, X.; Guo, Y.; Shen, Z.; Duan, L.; Huang, Z.; et al. Unique Profile of Driver Gene Mutations in Patients With Non-Small-Cell Lung Cancer in Qujing City, Yunnan Province, Southwest China. Front. Oncol. 2021, 11, 1121. [Google Scholar]
- Shi Yeen, T.N.; Pathmanathan, R.; Shiran, M.S.; Ahmad Zaid, F.A.; Cheah, Y.K. Detection of epidermal growth factor receptor mutations in formalin fixed paraffin embedded biopsies in Malaysian non-small cell lung cancer patients. J. Biomed. Sci. 2013, 20, 22. [Google Scholar] [CrossRef] [Green Version]
- Wen, S.; Dai, L.; Wang, L.; Wang, W.; Wu, D.; Wang, K.; He, Z.; Wang, A.; Chen, H.; Zhang, P.; et al. Genomic Signature of Driver Genes Identified by Target Next-Generation Sequencing in Chinese Non-Small Cell Lung Cancer. Oncologist 2019, 24, e1070–e1081. [Google Scholar] [CrossRef] [Green Version]
- Evans, M.; O’Sullivan, B.; Smith, M.; Hughes, F.; Mullis, T.; Trim, N.; Taniere, P. Large-Scale EGFR Mutation Testing in Clinical Practice: Analysis of a Series of 18,920 Non-Small Cell Lung Cancer Cases. Pathol. Oncol. Res. 2019, 25, 1401–1409. [Google Scholar] [CrossRef]
- Martin, J.; Lehmann, A.; Klauschen, F.; Hummel, M.; Lenze, D.; Grohé, C.; Tessmer, A.; Gottschalk, J.; Schmidt, B.; Pau, H.W.; et al. Clinical Impact of Rare and Compound Mutations of Epidermal Growth Factor Receptor in Patients With Non-Small-Cell Lung Cancer. Clin. Lung Cancer 2019, 20, 350–362.e4. [Google Scholar] [CrossRef]
- Sousa, A.C.; Silveira, C.; Janeiro, A.; Malveiro, S.; Oliveira, A.R.; Felizardo, M.; Nogueira, F.; Teixeira, E.; Martins, J.; Carmo-Fonseca, M. Detection of rare and novel EGFR mutations in NSCLC patients: Implications for treatment-decision. Lung Cancer 2020, 139, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, T.; Kohsaka, S.; Takamochi, K.; Hara, K.; Kishikawa, S.; Sano, K.; Takahashi, F.; Suehara, Y.; Saito, T.; Takahashi, K.; et al. Clinicopathological characteristics of lung adenocarcinoma with compound EGFR mutations. Hum. Pathol. 2020, 103, 42–51. [Google Scholar] [CrossRef] [PubMed]
- Bar, J.; Kian, W.; Wolner, M.; Derijcke, S.; Girard, N.; Rottenberg, Y.; Dudnik, E.; Metro, G.; Hochmair, M.J.; Aboubakar, F.; et al. 1206P UNcommon EGFR mutations: International Case series on efficacy of Osimertinib in Real-life practice in first-liNe setting (UNICORN). Ann. Oncol. 2021, 32, S961–S962. [Google Scholar] [CrossRef]
- Miura, S.; Hsia, T.-C.; Hung, J.-Y.; Jung, H.A.; Shih, J.-Y.; Yang, T.-Y.; Park, C.-K.; Lee, S.H.; Okamoto, T.; Ahn, H.K.; et al. Abstract LB138: UpSwinG: Real-world, non-interventional cohort study on TKI activity in patients (pts) with EGFR mutation-positive (EGFRm+) NSCLC with uncommon mutations. Cancer Res. 2021, 81, LB138. [Google Scholar]
- Burnett, H.; Emich, H.; Carroll, C.; Stapleton, N.; Mahadevia, P.; Li, T. Epidemiological and clinical burden of EGFR Exon 20 insertion in advanced non-small cell lung cancer: A systematic literature review. PLoS ONE 2021, 16, e0247620. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Xu, X.; Cai, J.; Ning, J.; Wery, J.P.; Li, Q.X. NSCLC harboring EGFR exon-20 insertions after the regulatory C-helix of kinase domain responds poorly to known EGFR inhibitors. Int. J. Cancer 2016, 139, 171–176. [Google Scholar] [CrossRef] [Green Version]
- Bazhenova, L.; Min Yang m, A.; Viteri, S.; Bauml, J.M.; Ignatius Ou, S.-H.; Gadgeel, S.M.; Manuel Trigo, J.; Backenroth, D.; Li, T.; Londhe, A.; et al. Comparative Clinical Outcomes for Patients With Advanced NSCLC Harboring EGFR Exon 20 Insertion Mutations and Common EGFR Mutations. Lung Cancer 2021, 162, 154–161. [Google Scholar] [CrossRef]
- Tam, I.Y.; Leung, E.L.; Tin, V.P.; Chua, D.T.; Sihoe, A.D.; Cheng, L.C.; Chung, L.P.; Wong, M.P. Double EGFR mutants containing rare EGFR mutant types show reduced in vitro response to gefitinib compared with common activating missense mutations. Mol. Cancer 2009, 8, 2142–2151. [Google Scholar] [CrossRef] [Green Version]
- Kimura, S.; Tanaka, K.; Harada, T.; Liu, R.; Shibahara, D.; Kawano, Y.; Nakanishi, Y.; Okamoto, I. Sensitivity of epidermal growth factor receptor with single or double uncommon mutations to afatinib confirmed by a visual assay. Cancer Sci. 2018, 109, 3657–3661. [Google Scholar] [CrossRef] [PubMed]
- Gristina, V.; Malapelle, U.; Galvano, A.; Pisapia, P.; Pepe, F.; Rolfo, C.; Tortorici, S.; Bazan, V.; Troncone, G.; Russo, A. The significance of epidermal growth factor receptor uncommon mutations in non-small cell lung cancer: A systematic review and critical appraisal. Cancer Treat. Rev. 2020, 85, 101994. [Google Scholar] [CrossRef] [PubMed]
- Floc’h, N.; Lim, S.; Bickerton, S.; Ahmed, A.; Orme, J.; Urosevic, J.; Martin, M.J.; Cross, D.A.E.; Cho, B.C.; Smith, P.D. Osimertinib, an Irreversible Next-Generation EGFR Tyrosine Kinase Inhibitor, Exerts Antitumor Activity in Various Preclinical NSCLC Models Harboring the Uncommon EGFR Mutations G719X or L861Q or S768I. Mol. Cancer 2020, 19, 2298–2307. [Google Scholar] [CrossRef]
- Kohsaka, S.; Nagano, M.; Ueno, T.; Suehara, Y.; Hayashi, T.; Shimada, N.; Takahashi, K.; Suzuki, K.; Takamochi, K.; Takahashi, F.; et al. A method of high-throughput functional evaluation of EGFR gene variants of unknown significance in cancer. Sci. Transl. Med. 2017, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akula, S.; Kamasani, S.; Sivan, S.K.; Manga, V.; Vudem, D.R.; Kancha, R.K. Computational Analysis of Epidermal Growth Factor Receptor Mutations Predicts Differential Drug Sensitivity Profiles toward Kinase Inhibitors. J. Thorac. Oncol. 2018, 13, 721–726. [Google Scholar] [CrossRef] [Green Version]
- Peng, L.; Song, Z.-G.; Jiao, S.-C. Efficacy analysis of tyrosine kinase inhibitors on rare non-small cell lung cancer patients harboring complex EGFR mutations. Sci. Rep. 2014, 4, 6104. [Google Scholar] [CrossRef] [Green Version]
- Li, H.; Wang, C.; Wang, Z.; Hu, Y.; Zhang, G.; Zhang, M.; Zheng, X.; Zhang, X.; Yang, J.; Ma, Z.; et al. Efficacy and long-term survival of advanced lung adenocarcinoma patients with uncommon EGFR mutations treated with 1st generation EGFR-TKIs compared with chemotherapy as first-line therapy. Lung Cancer 2019, 130, 42–49. [Google Scholar] [CrossRef]
- Rossi, S.; Damiano, P.; Toschi, L.; Finocchiaro, G.; Giordano, L.; Marinello, A.; Bria, E.; D’Argento, E.; Santoro, A. Uncommon single and compound EGFR mutations: Clinical outcomes of a heterogeneous subgroup of NSCLC. Curr. Probl. Cancer 2021, 100787. [Google Scholar] [CrossRef] [PubMed]
- Passaro, A.; Prelaj, A.; Bonanno, L.; Tiseo, M.; Tuzi, A.; Proto, C.; Chiari, R.; Rocco, D.; Genova, C.; Sini, C.; et al. Activity of EGFR TKIs in Caucasian Patients With NSCLC Harboring Potentially Sensitive Uncommon EGFR Mutations. Clin. Lung Cancer 2019, 20, e186–e194. [Google Scholar] [CrossRef] [PubMed]
- Moran, T.; Taus, A.; Arriola, E.; Aguado, C.; Dómine, M.; Rueda, A.G.; Calles, A.; Cedrés, S.; Viñolas, N.; Isla, D.; et al. Clinical Activity of Afatinib in Patients With Non-Small-Cell Lung Cancer Harboring Uncommon EGFR Mutations: A Spanish Retrospective Multicenter Study. Clin. Lung Cancer 2020, 21, 428–436.e2. [Google Scholar] [CrossRef]
- Chen, K.; Yu, X.; Wang, H.; Huang, Z.; Xu, Y.; Gong, L.; Fan, Y. Uncommon mutation types of epidermal growth factor receptor and response to EGFR tyrosine kinase inhibitors in Chinese non-small cell lung cancer patients. Cancer Chemother. Pharm. 2017, 80, 1179–1187. [Google Scholar] [CrossRef] [PubMed]
- Lei, L.; Wang, W.X.; Zhu, Y.C.; Li, J.L.; Fang, Y.; Wang, H.; Zhuang, W.; Zhang, Y.B.; Wang, L.P.; Fang, M.Y.; et al. Real-world efficacy and potential mechanism of resistance of icotinib in Asian advanced non-small cell lung cancer with EGFR uncommon mutations: A multi-center study. Cancer Med. 2020, 9, 12–18. [Google Scholar] [CrossRef]
- Xu, J.; Jin, B.; Chu, T.; Dong, X.; Yang, H.; Zhang, Y.; Wu, D.; Lou, Y.; Zhang, X.; Wang, H.; et al. EGFR tyrosine kinase inhibitor (TKI) in patients with advanced non-small cell lung cancer (NSCLC) harboring uncommon EGFR mutations: A real-world study in China. Lung Cancer 2016, 96, 87–92. [Google Scholar] [CrossRef]
- Jung, H.A.; Park, S.; Sun, J.M.; Lee, S.H.; Ahn, J.S.; Ahn, M.J.; Park, K. Treatment and Outcomes of Metastatic Non-Small-Cell Lung Cancer Harboring Uncommon EGFR Mutations: Are They Different from Those with Common EGFR Mutations? Biology 2020, 9, 326. [Google Scholar] [CrossRef]
- Peng, L.; Song, Z.; Jiao, S. Comparison of uncommon EGFR exon 21 L858R compound mutations with single mutation. Onco Targets 2015, 8, 905–910. [Google Scholar]
- Wu, S.G.; Chang, Y.L.; Hsu, Y.C.; Wu, J.Y.; Yang, C.H.; Yu, C.J.; Tsai, M.F.; Shih, J.Y.; Yang, P.C. Good response to gefitinib in lung adenocarcinoma of complex epidermal growth factor receptor (EGFR) mutations with the classical mutation pattern. Oncologist 2008, 13, 1276–1284. [Google Scholar] [CrossRef] [Green Version]
- Hata, A.; Yoshioka, H.; Fujita, S.; Kunimasa, K.; Kaji, R.; Imai, Y.; Tomii, K.; Iwasaku, M.; Nishiyama, A.; Ishida, T.; et al. Complex mutations in the epidermal growth factor receptor gene in non-small cell lung cancer. J. Thorac. Oncol. 2010, 5, 1524–1528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kobayashi, S.; Canepa, H.M.; Bailey, A.S.; Nakayama, S.; Yamaguchi, N.; Goldstein, M.A.; Huberman, M.S.; Costa, D.B. Compound EGFR mutations and response to EGFR tyrosine kinase inhibitors. J. Thorac. Oncol. 2013, 8, 45–51. [Google Scholar] [CrossRef] [Green Version]
- Wu, J.Y.; Yu, C.J.; Chang, Y.C.; Yang, C.H.; Shih, J.Y.; Yang, P.C. Effectiveness of tyrosine kinase inhibitors on “uncommon” epidermal growth factor receptor mutations of unknown clinical significance in non-small cell lung cancer. Clin. Cancer Res. 2011, 17, 3812–3821. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, B.; Wang, S.; Qian, J.; Yang, W.; Qian, F.; Lu, J.; Zhang, Y.; Qiao, R.; Han, B. Complex epidermal growth factor receptor mutations and their responses to tyrosine kinase inhibitors in previously untreated advanced lung adenocarcinomas. Cancer 2018, 124, 2399–2406. [Google Scholar] [CrossRef] [Green Version]
- Tan, J.; Hu, C.; Deng, P.; Wan, R.; Cao, L.; Li, M.; Yang, H.; Gu, Q.; An, J.; Jiang, J. The Predictive Values of Advanced Non-Small Cell Lung Cancer Patients Harboring Uncommon EGFR Mutations-The Mutation Patterns, Use of Different Generations of EGFR-TKIs, and Concurrent Genetic Alterations. Front. Oncol. 2021, 11, 646577. [Google Scholar] [CrossRef]
- Yang, J.C.-H.; Schuler, M.; Popat, S.; Miura, S.; Heeke, S.; Park, K.; Märten, A.; Kim, E.S. Afatinib for the Treatment of NSCLC Harboring Uncommon EGFR Mutations: A Database of 693 Cases. J. Thorac. Oncol. 2020, 15, 803–815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, S.G.; Yu, C.J.; Yang, J.C.; Shih, J.Y. The effectiveness of afatinib in patients with lung adenocarcinoma harboring complex epidermal growth factor receptor mutation. Adv. Med. Oncol. 2020, 12, 1758835920946156. [Google Scholar] [CrossRef]
- Li, H.S.; Yang, G.J.; Wang, Y. Case Report: Dacomitinib May Not Benefit Patients Who Develop Rare Compound Mutations After Later-Line Osimertinib Treatment. Front. Oncol. 2021, 11, 649843. [Google Scholar] [CrossRef]
- Ji, J.; Aredo, J.V.; Piper-Vallillo, A.; Huppert, L.; Rotow, J.K.; Husain, H.; Stewart, S.L.; Cobb, R.; Wakelee, H.A.; Blakely, C.M.; et al. Osimertinib in non-small cell lung cancer (NSCLC) with atypical EGFR activating mutations: A retrospective multicenter study. J. Clin. Oncol. 2020, 38, 9570. [Google Scholar] [CrossRef]
- Su, K.Y.; Chen, H.Y.; Li, K.C.; Kuo, M.L.; Yang, J.C.; Chan, W.K.; Ho, B.C.; Chang, G.C.; Shih, J.Y.; Yu, S.L.; et al. Pretreatment epidermal growth factor receptor (EGFR) T790M mutation predicts shorter EGFR tyrosine kinase inhibitor response duration in patients with non-small-cell lung cancer. J. Clin. Oncol. 2012, 30, 433–440. [Google Scholar] [CrossRef] [Green Version]
- Singh, V.; Nambirajan, A.; Malik, P.S.; Thulkar, S.; Pandey, R.M.; Luthra, K.; Arava, S.; Ray, R.; Mohan, A.; Jain, D. Spectrum of uncommon and compound epidermal growth factor receptor mutations in non-small-cell lung carcinomas with treatment response and outcome analysis: A study from India. Lung Cancer 2020, 149, 53–60. [Google Scholar] [CrossRef]
- Lin, Y.T.; Tsai, T.H.; Wu, S.G.; Liu, Y.N.; Yu, C.J.; Shih, J.Y. Complex EGFR mutations with secondary T790M mutation confer shorter osimertinib progression-free survival and overall survival in advanced non-small cell lung cancer. Lung Cancer 2020, 145, 1–9. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study | Region | Patients Screened (N) | Testing Method | EGFR Mut Rate | EGFR Compound Mut Rate |
|---|---|---|---|---|---|
| (N, %) | (N, % of EGFR Mut) | ||||
| Syahruddin et al., 2018 [7] | Indonesian | 1779 | PCR HRM | 791 (44.4) | 154 (19.5) |
| RFLP | |||||
| Zaini et al., 2019 [8] | Indonesian | 116 | PCR HRM | 69 (63.2) | 18 (26) |
| RFLP | |||||
| Jing et al., 2018 [9] | China | 112 | NGS | 58 (51.8) | 11 (18.9) |
| Mao et al., 2021 [11] | China | 21,324 | NGS + qPCR + Sanger | 9,621 (47.5) | 642 (6.7) |
| Wen et al., 2019 [14] | China | 1200 | NGS | 571(47.6) | 87 (15.3) |
| Zhou et al., 2021 [12] | SW China | 2146 | ARMS-PCR | 346 (46) Q | 151 (43.6) Q |
| (Q vs. non-Q) | 710 (51) non-Q | 74 (10.4) non-Q | |||
| Namba et al., 2019 [10] | Japan | 531 | MBS | 64 (n.e.) 1 | 8 (12.5) |
| Shi et al., 2013 [13] | Malaysia | 484 | ARMS + HRM | 221 (45.7) | 9 (4) |
| Evans et al., 2019 [15] | EU | 17,782 | qPCR | 1,737 (10.7) | 79 (4.9) |
| Sousa et al., 2020 [17] | EU | 1228 | Sanger | 252 (20.5) | 19 (7.5) |
| Martin et al., 2019 [16] | EU | 2906 | Sanger | 408 (14) | 22 (5.4) |
| Methodology | Advantages | Disadvantages |
|---|---|---|
| RT-PCR |
|
|
| dPCR |
|
|
| NGS |
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Attili, I.; Passaro, A.; Pisapia, P.; Malapelle, U.; de Marinis, F. Uncommon EGFR Compound Mutations in Non-Small Cell Lung Cancer (NSCLC): A Systematic Review of Available Evidence. Curr. Oncol. 2022, 29, 255-266. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol29010024
Attili I, Passaro A, Pisapia P, Malapelle U, de Marinis F. Uncommon EGFR Compound Mutations in Non-Small Cell Lung Cancer (NSCLC): A Systematic Review of Available Evidence. Current Oncology. 2022; 29(1):255-266. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol29010024
Chicago/Turabian StyleAttili, Ilaria, Antonio Passaro, Pasquale Pisapia, Umberto Malapelle, and Filippo de Marinis. 2022. "Uncommon EGFR Compound Mutations in Non-Small Cell Lung Cancer (NSCLC): A Systematic Review of Available Evidence" Current Oncology 29, no. 1: 255-266. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol29010024