Symptom Burden and Complexity in the Last 12 Months of Life among Cancer Patients Choosing Medical Assistance in Dying (MAID) in Alberta, Canada

 , ,
, ,  , , ,
, , ,
Abstract
:1. Introduction
1.1. Medical Assistance in Dying in Canada
1.2. Patient-Reported Outcomes in Cancer Care Alberta
2. Materials and Methods
2.1. Study Design
2.2. Sample and Data Collection
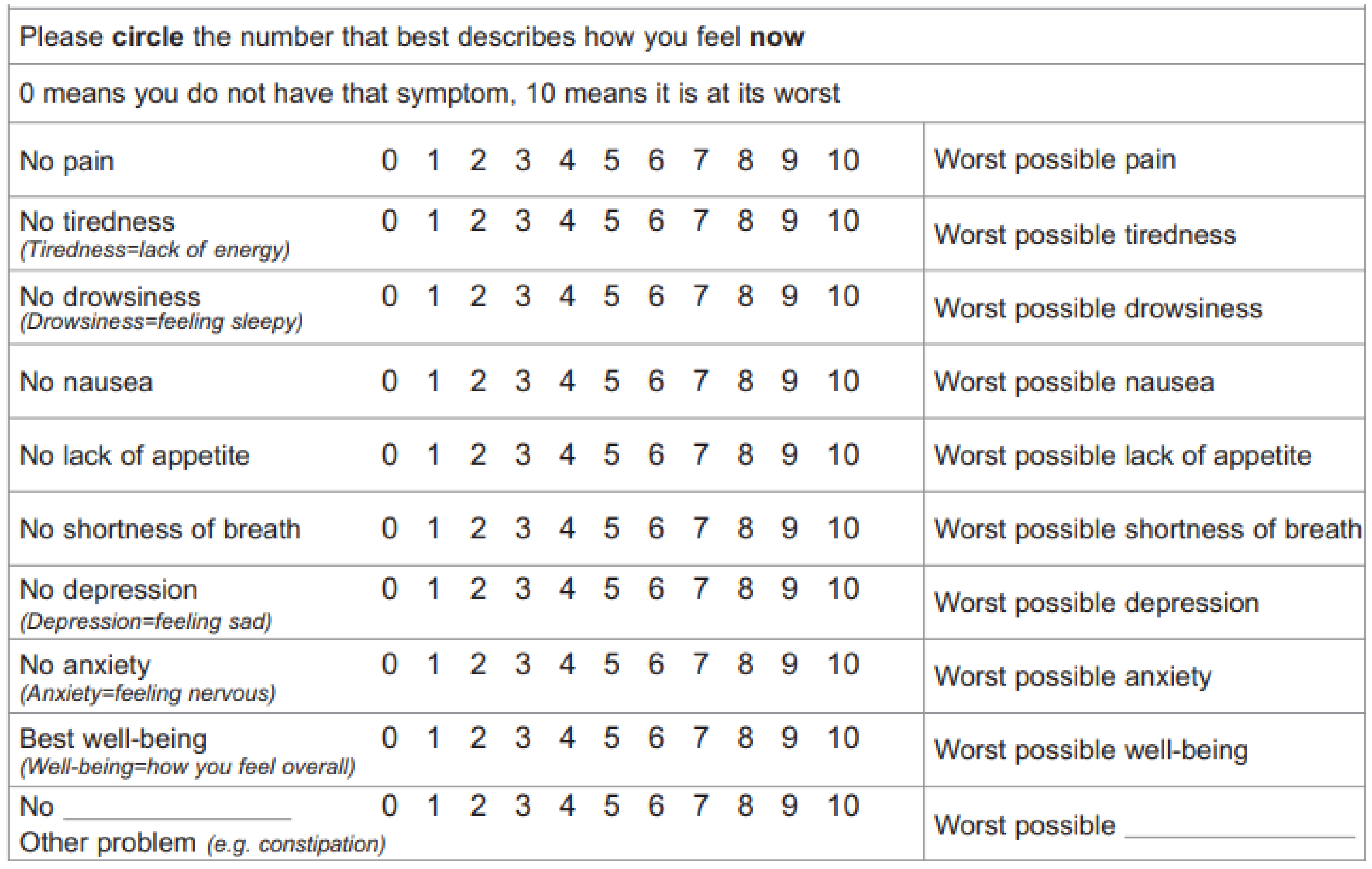
2.3. Measures
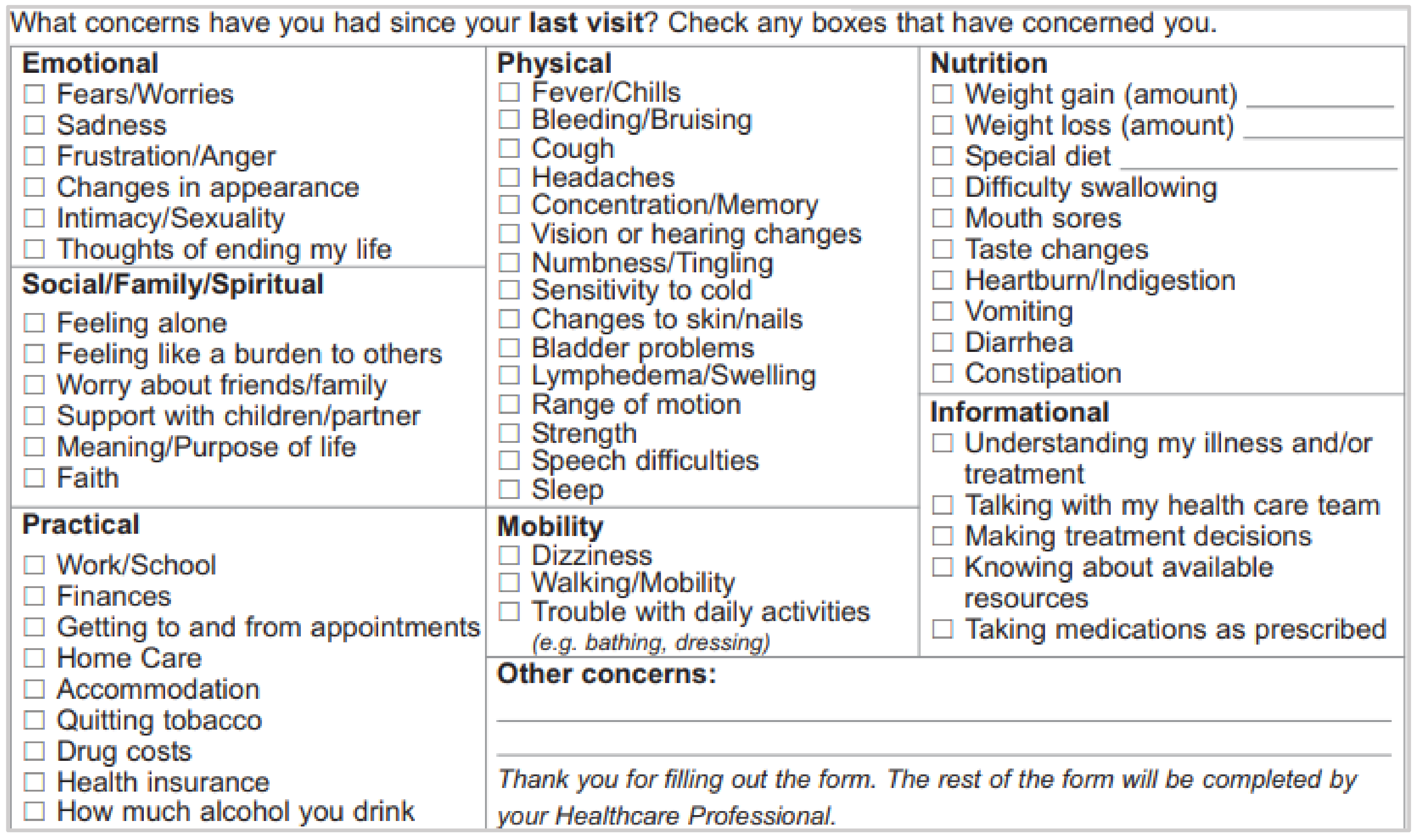
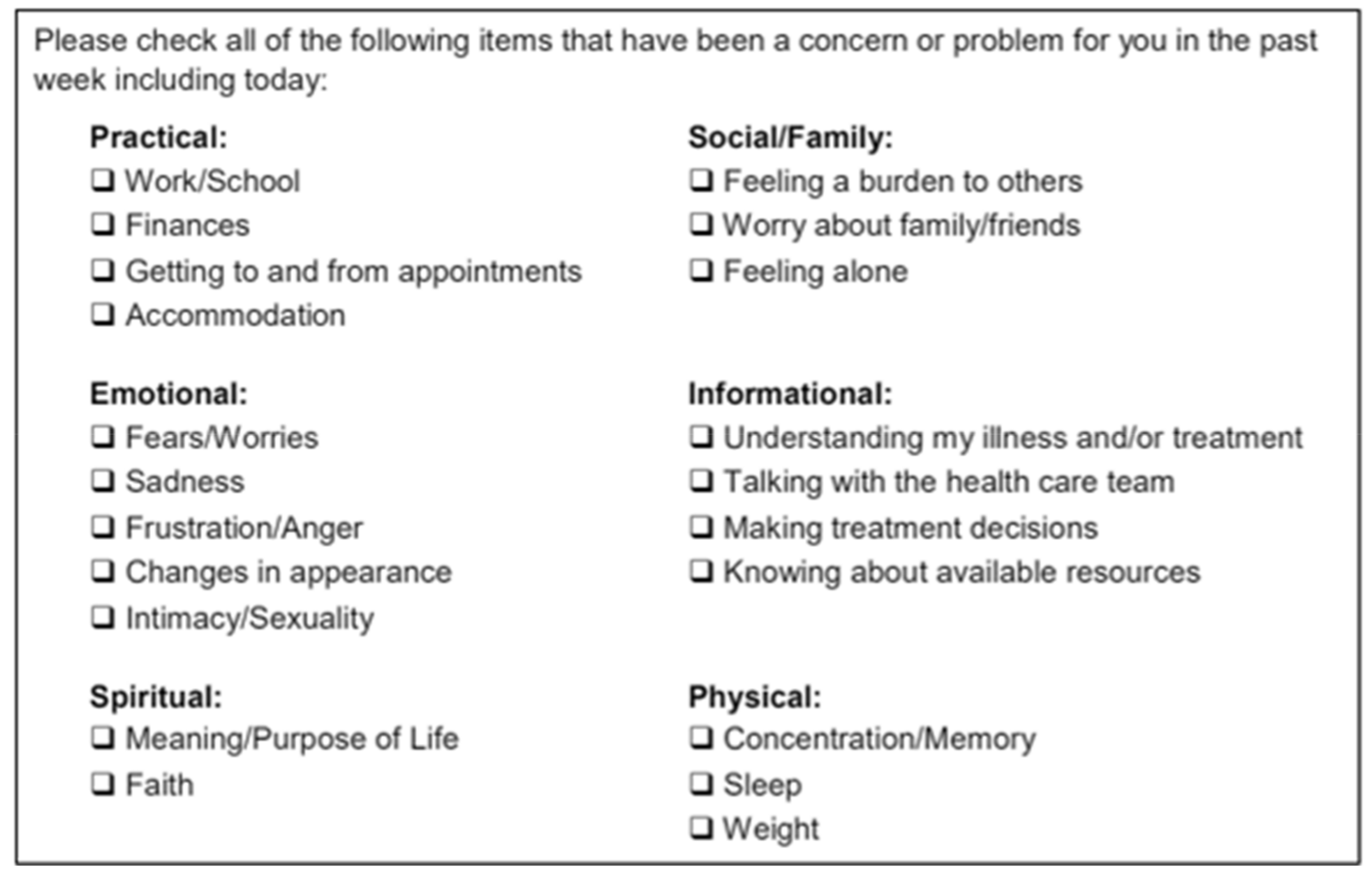
2.3.1. Patient-Reported Outcomes Questionnaire Components
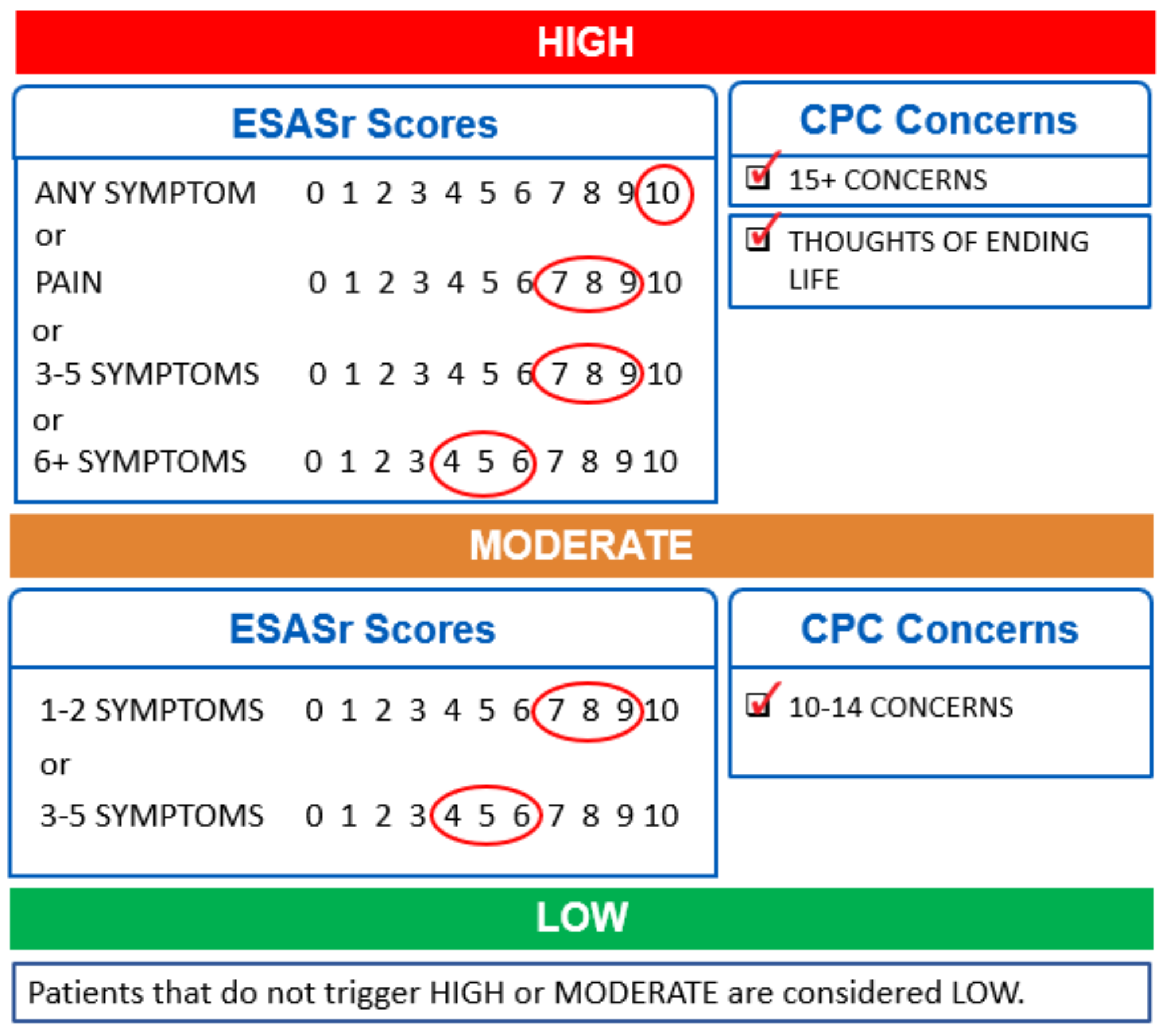
2.3.2. Symptom Complexity Level
2.4. Statistical Analyses
3. Results
3.1. Study Sample
3.2. Time between MAID Request and Provision Dates
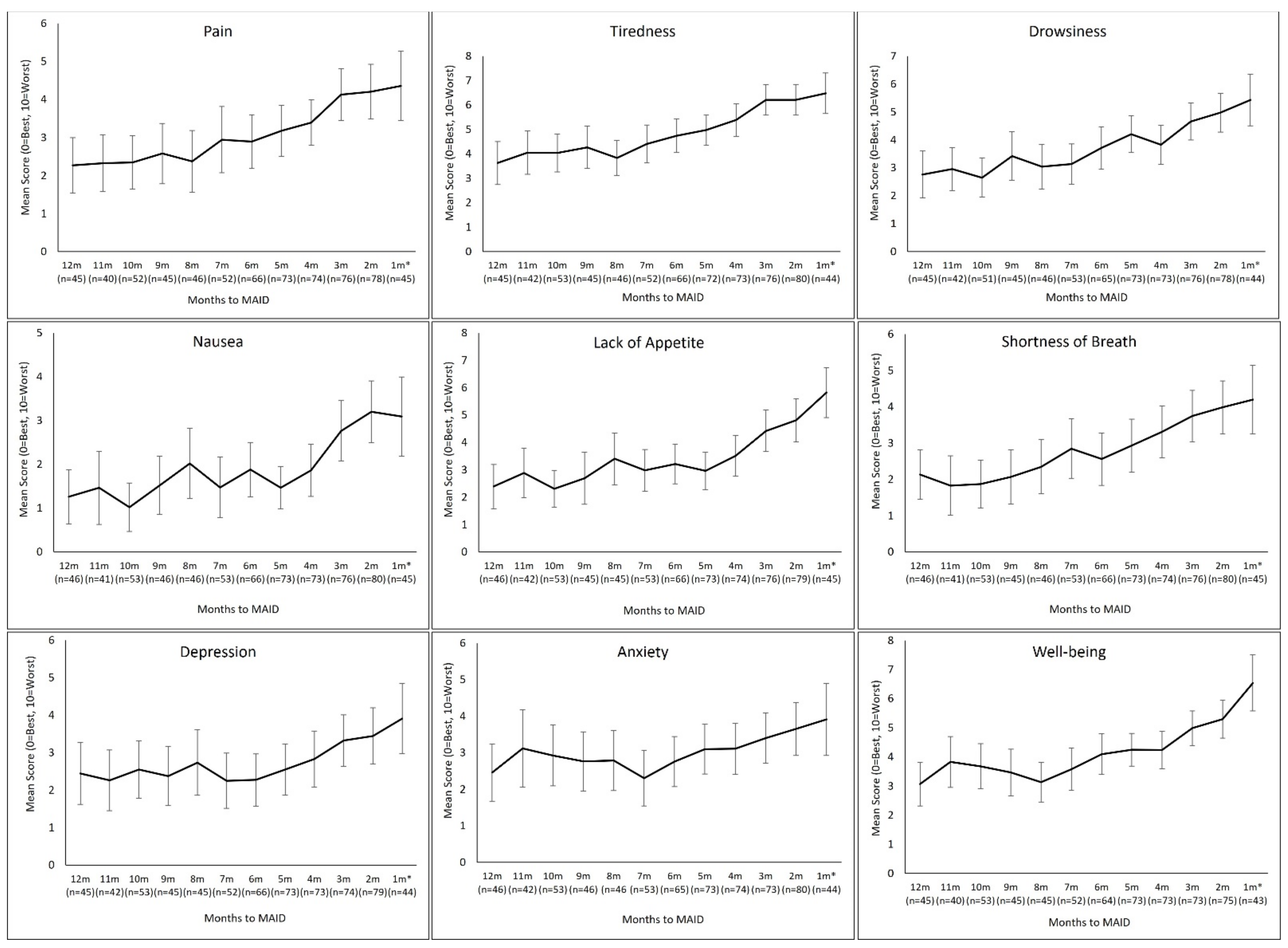
3.3. Symptom Trajectories
3.3.1. ESAS-r Trajectories
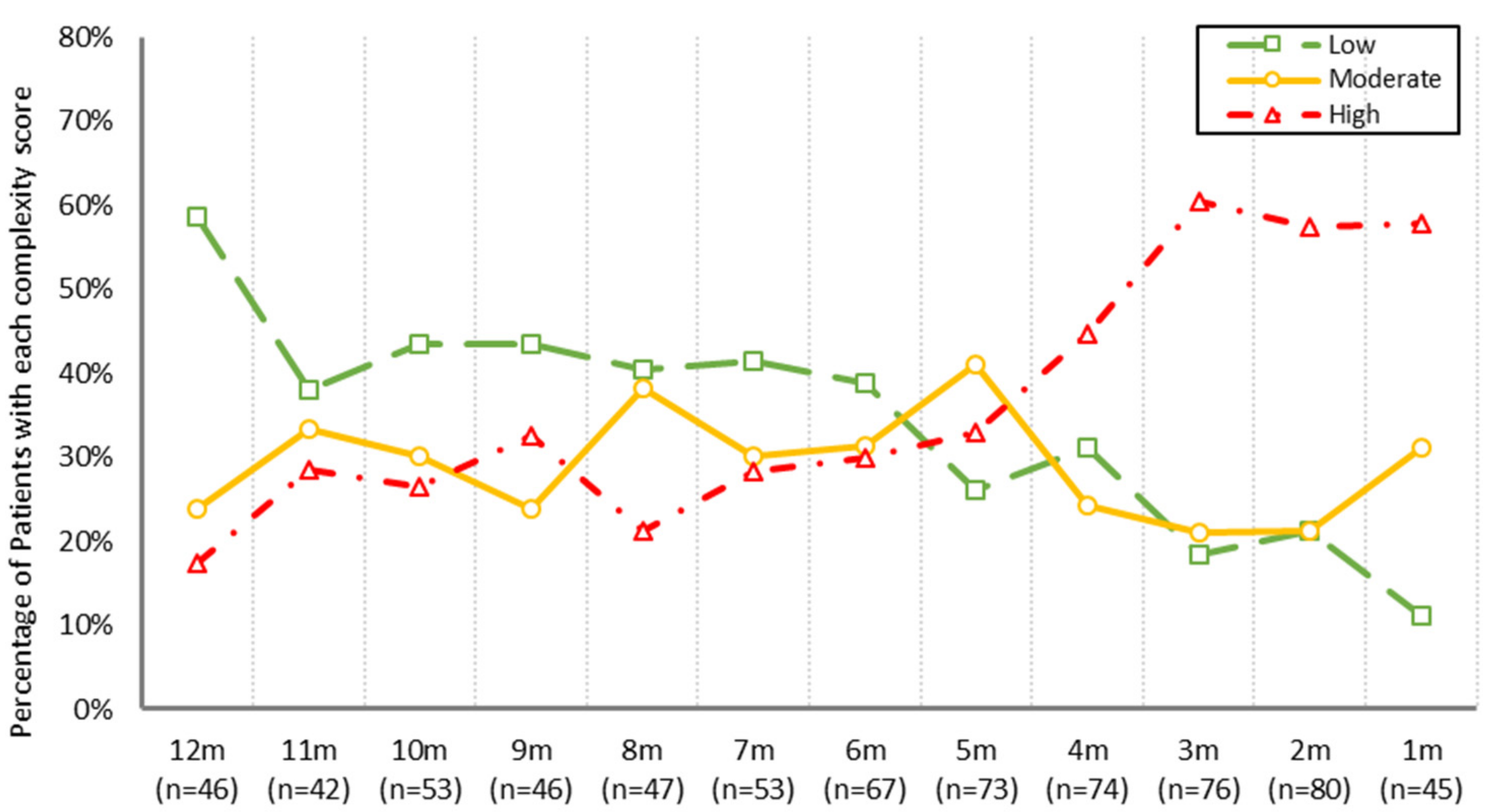
3.3.2. Symptom Complexity Level Trajectory
4. Discussion
4.1. Increased Symptom Burden and Complexity Prior to MAID Provision
4.2. Implications for Practice
4.3. Study Limitations
4.4. Future Directions for Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A



References
- Reilly, C.M.; Bruner, D.W.; Mitchell, S.A.; Minasian, L.M.; Basch, E.; Dueck, A.C.; Cella, D.; Reeve, B.B. A literature synthesis of symptom prevalence and severity in persons receiving active cancer treatment. Support. Care Cancer 2013, 21, 1525–1550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El-Jawahri, A.; Traeger, L.; Park, E.R.; Greer, J.A.; Pirl, W.; Lennes, I.T.; Jackson, V.A.; Rn, E.R.G.; Temel, J.S. Associations among prognostic understanding, quality of life, and mood in patients with advanced cancer. Cancer 2013, 120, 278–285. [Google Scholar] [CrossRef] [PubMed]
- Finlay, I. Dying and choosing. Lancet 2009, 373, 1840–1841. [Google Scholar] [CrossRef]
- Wilson, K.G.; Chochinov, H.M.; McPherson, C.; Lemay, K.; Allard, P.; Chary, S.; Gagnon, P.R.; Macmillan, K.; De Luca, M.; O’Shea, F.; et al. Suffering With Advanced Cancer. J. Clin. Oncol. 2007, 25, 1691–1697. [Google Scholar] [CrossRef]
- Nayyar, D.; Kawaguchi, S.; Mah, B. Request for medical assistance in dying after a suicide attempt in a 75-year-old man with pancreatic adenocarcinoma. Can. Med Assoc. J. 2019, 191, E838–E840. [Google Scholar] [CrossRef] [Green Version]
- Wales, J.; Isenberg, S.R.; Wegier, P.; Shapiro, J.; Cellarius, V.; Buchman, S.; Husain, A.; Khoshnood, N. Providing Medical Assistance in Dying within a Home Palliative Care Program in Toronto, Canada: An Observational Study of the First Year of Experience. J. Palliat. Med. 2018, 21, 1573–1579. [Google Scholar] [CrossRef]
- Li, M.; Shapiro, G.K.; Klein, R.; Barbeau, A.; Rydall, A.; Bell, J.A.H.; Nissim, R.; Hales, S.; Zimmermann, C.; Wong, R.K.S.; et al. Medical Assistance in Dying in patients with advanced cancer and their caregivers: A mixed methods longitudinal study protocol. BMC Palliat. Care 2021, 20, 117. [Google Scholar] [CrossRef]
- Government of Canada. Medical Assistance in Dying. Updated 2021. Available online: https://www.canada.ca/en/health-canada/services/medical-assistance-dying.html#a2 (accessed on 28 June 2021).
- Government of Canada. Canada’s New Medical Assistance in Dying (MAID) Law. Updated 2021. Available online: https://www.justice.gc.ca/eng/cj-jp/ad-am/bk-di.html (accessed on 16 August 2021).
- Health Canada. First Annual Report on Medical Assistance in Dying in Canada 2019. Updated 24 July 2020. Available online: https://www.canada.ca/en/health-canada/services/medical-assistance-dying-annual-report-2019.html#a4.1 (accessed on 2 July 2021).
- Orentlicher, D.; Pope, T.M.; Rich, B.A. Clinical Criteria for Physician Aid in Dying. J. Palliat. Med. 2016, 19, 259–262. [Google Scholar] [CrossRef] [Green Version]
- Buchbinder, M.; Brassfield, E.R.; Mishra, M. Health care providers’ experiences with implementing medical aid-in-dying in Vermont: A qualitative study. J. Gen. Intern. Med. 2019, 34, 636–641. [Google Scholar] [CrossRef] [Green Version]
- Downar, J.; Fowler, R.A.; Halko, R. Early experience with medical assistance in dying in Ontario, Canada: A cohort study. CMAJ 2020, 192, E173–E181. [Google Scholar] [CrossRef] [Green Version]
- Silvius, J.L.; Memon, A.; Arain, M. Medical Assistance in Dying: Alberta approach and policy analysis. Can. J. Aging 2019, 38, 397–406. [Google Scholar] [CrossRef]
- Government of Alberta. Population Statistics. Updated 2021. Available online: https://www.alberta.ca/population-statistics.aspx (accessed on 2 July 2021).
- Cancer Care Alberta. The 2021 Report on Cancer Statistics in Alberta. February 2021. Available online: https://public.tableau.com/profile/cancercontrol.ab#!/vizhome/The2021ReportonCancerStatisticsinAlberta/Highlights (accessed on 2 July 2021).
- Cuthbert, C.A.; Watson, L.; Xu, Y.; Boyne, D.J.; Hemmelgarn, B.R.; Cheung, W.Y. Patient-Reported Outcomes in Alberta: Rationale, Scope, and Design of a Database Initiative. Curr. Oncol. 2019, 26, 503–509. [Google Scholar] [CrossRef] [Green Version]
- Canadian Partnership against Cancer. 2012 Cancer System Performance Report. 2012. Available online: https://www.systemperformance.ca/report/performance-report-2/ (accessed on 23 February 2021).
- Watson, L.; Qi, S.; DeIure, A.; Photitai, E.; Chmielewski, L.; Smith, L. Validating a Patient-Reported Outcomes–Derived Algorithm for Classifying Symptom Complexity Levels Among Patients With Cancer. J. Natl. Compr. Cancer Netw. 2020, 18, 1518–1525. [Google Scholar] [CrossRef]
- Wilkins, R. PCCF + Version 3G User’s Guide: Automated Geographic Coding Based on the Statistics Canada Postal Code Conversions Files; Statistics Canada: Ottawa, ON, Canada, 2001. [Google Scholar]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chron. Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Deyo, R.A.; Cherkin, D.C.; Ciol, M.A. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J. Clin. Epidemiol. 1992, 45, 613–619. [Google Scholar] [CrossRef]
- Quan, H.; Sundararajan, V.; Halfon, P.; Fong, A.; Burnand, B.; Luthi, J.-C.; Saunders, L.D.; Beck, C.A.; Feasby, T.E.; Ghali, W.A. Coding Algorithms for Defining Comorbidities in ICD-9-CM and ICD-10 Administrative Data. Med. Care 2005, 43, 1130–1139. [Google Scholar] [CrossRef]
- Nekolaichuk, C.; Watanbe, S.; Beaumont, C. The Edmonton symptom assessment system: A 15-year retrospective review of validation studies. Palliat. Med. 2008, 22, 111–122. [Google Scholar] [CrossRef]
- Bultz, B.D.; Groff, S.L.; Fitch, M.; Blais, M.C.; Howes, J.; Levy, K.; Mayer, C. Implementing screening for distress, the 6th vital sign: A Canadian strategy for changing practice. Psycho-Oncology 2011, 20, 463–469. [Google Scholar] [CrossRef]
- Barbera, L.; Atzema, C.; Sutradhar, R.; Seow, H.; Howell, D.; Husain, A.; Sussman, J.; Earle, C.; Liu, Y.; Dudgeon, D. Do Patient-Reported Symptoms Predict Emergency Department Visits in Cancer Patients? A Population-Based Analysis. Ann. Emerg. Med. 2013, 61, 427–437.e5. [Google Scholar] [CrossRef]
- Singmann, H.; Kellen, D. An introduction to mixed models for experimental psychology. New Methods Cogn. Psychol. 2019, 28, 4–31. [Google Scholar]
- Molenberghs, G.; Thijs, H.; Jansen, I.; Beunckens, C.; Kenward, M.G.; Mallinckrodt, C.; Carroll, R.J. Analyzing incomplete longitudinal clinical trial data. Biostatistics 2004, 5, 445–464. [Google Scholar] [CrossRef]
- Hanley, J.A.; Negassa, A.; Edwardes, M.D.; Forrester, J.E. Statistical analysis of correlated data using generalized estimating equations: An orientation. Am. J. Epidemiol. 2003, 157, 364–375. [Google Scholar] [CrossRef]
- Hwang, S.S.; Chang, V.T.; Fairclough, D.L.; Cogswell, J.; Kasimis, B. Longitudinal quality of life in advanced cancer patients: Pilot study results from a VA medical cancer centre. JPSM 2003, 25, 225–235. [Google Scholar] [CrossRef]
- Hagelin, C.L.; Seiger, A.; Fürst, C.J. Quality of life in terminal care—With special reference to age, gender and marital status. Support Care Cancer 2006, 14, 320–328. [Google Scholar] [CrossRef]
- Morris, J.N.; Suissa, S.; Sherwood, S.; Wright, S.M.; Greer, D. Last days: A study of the quality of life of terminally ill cancer patients. J. Chronic Dis. 1986, 39, 47–62. [Google Scholar] [CrossRef]
- Cancer Care Alberta, PROs and Economic Analysis: An Exploratory Discussion. Updated 2018.
- Homsi, J.; Walsh, D.; Rivera, N.; Rybicki, L.A.; Nelson, K.A.; Legrand, S.B.; Davis, M.P.; Naughton, M.; Gvozdjan, D.; Pham, H. Symptom evaluation in palliative medicine: Patient report vs. systematic assessment. Support. Care Cancer 2006, 14, 444–453. [Google Scholar] [CrossRef]
- Sarradon-Eck, A.; Besle, S.; Adam-Troian, J.; Capodano, G.; Mancini, J. Understanding the Barriers to Introducing Early Palliative Care for Patients with Advanced Cancer: A Qualitative Study. J. Palliat. Med. 2019, 22, 508–516. [Google Scholar] [CrossRef]
- Cervantez, S.R.; Tenner, L.L.; Schmidt, S.; Aduba, I.O.; Jones, J.T.; Ali, N.; Singh-Carlson, S. Symptom burden and palliative referral disparities in an ambulatory south Texas cancer center. Front. Oncol. 2018, 8, 443. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network. NCCN Guidelines: Palliative Care. 2018. Available online: https://www.nccn.org/guidelines/guidelines-detail?category=3&id=1454 (accessed on 23 February 2022).
- Canadian Hospice Palliative Care Association. A Model to Guide Hospice Palliative Care. 2013. Available online: https://www.chpca.ca/wp-content/uploads/2019/12/norms-of-practice-eng-web.pdf (accessed on 23 February 2022).
- Falzone, L.; Salomone, S.; Libra, M. Evolution of cancer pharmacological treatments at the turn of the third millennium. Front. Pharmacol. 2018, 9, 1300. [Google Scholar] [CrossRef] [Green Version]
- Chu, C.; Anderson, R.; White, N.; Stone, P. Prognosticating for adult patients with advanced incurable cancer: A needed oncologist skill. Curr. Treat Options Oncol. 2020, 21, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiao, J.; Brenneis, C.; Ibrahim, N.; Bryan, A.; Fassbender, K. Definitions of Palliative Care Terms: A Consensus-Oriented Decision-Making Process. J. Palliat. Med. 2021, 24, 1342–1350. [Google Scholar] [CrossRef] [PubMed]
- Davis, M.P.; Bruera, E.; Morganstern, D. Early integration of palliative and supportive care in the cancer continuum: Challenges and opportunities. Am. Soc. Clin. Oncol. Educ. Book 2013, 33, 144–150. Available online: https://ascopubs.org/doi/pdfdirect/10.14694/EdBook_AM.2013.33.144 (accessed on 10 January 2022). [CrossRef] [PubMed]
- Verkissen, M.N.; Hjermstad, M.J.; Van Belle, S.; Kaasa, S.; Deliens, L.; Pardon, K. Quality of life and symptom intensity over time in people with cancer receiving palliative care: Results from the international European Palliative Care Cancer Symptom study. PLoS ONE 2019, 14, e0222988. [Google Scholar] [CrossRef]
- Watanabe, S.M.; Nekolaichuk, C.L.; Beaumont, C. The Edmonton Symptom Assessment System, a proposed tool for distress screening in cancer patients: Development and refinement. Psycho-Oncology 2012, 21, 977–985. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Full Cohort (n = 337) | Subgroup with PROs (n = 193) | Subgroup without PROs (n = 144) | p (PROs vs. No PROs) |
|---|---|---|---|---|
| Age at MAID provision (in years) | 0.000 | |||
| Mean (Min, Max, SD) | 72.6 (26, 98, 12.0) | 68.6 (26, 95, 11.5) | 78.0 (50, 98, 10.6) | |
| Sex | 0.788 | |||
| Female | 162 (48.1%) | 94 (48.7%) | 68 (47.2%) | |
| Male | 175 (51.9%) | 99 (51.3%) | 76 (52.8%) | |
| Tumour groups | 0.168 | |||
| Breast | 34 (10.1%) | 17 (8.8%) | 17 (11.8%) | |
| Gastrointestinal | 86 (25.5%) | 52 (26.9%) | 34 (23.6%) | |
| Genitourinary | 42 (12.5%) | 21 (10.9%) | 21 (14.6%) | |
| Gynecology | 32 (9.5%) | 22 (11.4%) | 10 (6.9%) | |
| Hematology | 29 (8.6%) | 20 (10.4%) | 9 (6.3%) | |
| Intrathoracic | 53 (15.7%) | 33 (17.1%) | 20 (13.9%) | |
| Other a | 61 (18.1%) | 28 (14.5%) | 33 (22.9%) | |
| CCI | 0.001 | |||
| 0 | 200 (59.3%) | 129 (66.8%) | 71 (49.3%) | |
| ≥1 | 137 (40.7%) | 64 (33.2%) | 73 (50.7%) | |
| Neighborhood income (CAD$) | 0.001 | |||
| Median | 97,230 | 103,179 | 88,517 |
| Number of Months | n | % |
|---|---|---|
| ≥10 month | 4 | 1.2 |
| 7–9 months | 6 | 1.8 |
| 4–6 months | 32 | 9.5 |
| 3 months | 15 | 4.5 |
| 2 months | 55 | 16.4 |
| 1 month a | 224 | 66.7 |
| Symptoms | Β a (95% CI) | SE b | F | p |
|---|---|---|---|---|
| Pain | 0.222 (0.160–0.284) | 0.031 | 49.9 | 0.000 |
| Tiredness | 0.250 (0.194–0.306) | 0.029 | 77.0 | 0.000 |
| Drowsiness | 0.217 (0.157–0.277) | 0.031 | 50.6 | 0.000 |
| Nausea | 0.170 (0.114–0.226) | 0.028 | 35.6 | 0.000 |
| Lack of appetite | 0.250 (0.182–0.319) | 0.035 | 52.0 | 0.000 |
| Shortness of breath | 0.168 (0.112–0.224) | 0.029 | 34.8 | 0.000 |
| Depression | 0.137 (0.082–0.193) | 0.028 | 24.0 | 0.000 |
| Anxiety | 0.060 (0.004–0.116) | 0.028 | 4.47 | 0.035 |
| Well-being | 0.223 (0.165–0.280) | 0.030 | 58.0 | 0.000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Watson, L.; Link, C.; Qi, S.; DeIure, A.; Russell, K.B.; Schulte, F.; Forbes, C.; Silvius, J.; Kelly, B.; Bultz, B.D. Symptom Burden and Complexity in the Last 12 Months of Life among Cancer Patients Choosing Medical Assistance in Dying (MAID) in Alberta, Canada. Curr. Oncol. 2022, 29, 1605-1618. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol29030135
Watson L, Link C, Qi S, DeIure A, Russell KB, Schulte F, Forbes C, Silvius J, Kelly B, Bultz BD. Symptom Burden and Complexity in the Last 12 Months of Life among Cancer Patients Choosing Medical Assistance in Dying (MAID) in Alberta, Canada. Current Oncology. 2022; 29(3):1605-1618. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol29030135
Chicago/Turabian StyleWatson, Linda, Claire Link, Siwei Qi, Andrea DeIure, K. Brooke Russell, Fiona Schulte, Caitlin Forbes, James Silvius, Brian Kelly, and Barry D. Bultz. 2022. "Symptom Burden and Complexity in the Last 12 Months of Life among Cancer Patients Choosing Medical Assistance in Dying (MAID) in Alberta, Canada" Current Oncology 29, no. 3: 1605-1618. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol29030135