Gemcitabine and Cisplatin as Neo-Adjuvant for Cholangiocarcinoma Patients Prior to Liver Transplantation: Case-Series

 , ,
, ,
Abstract
:1. Introduction
2. Methods
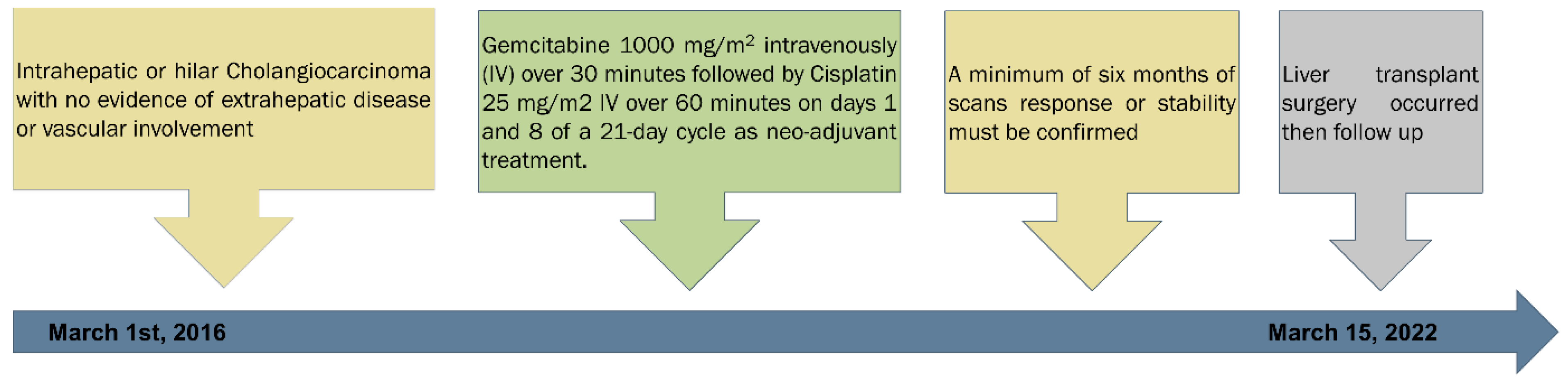
2.1. Participants
2.2. Gemcitabine plus Cisplatin as Neo-Adjuvant Treatment
2.3. Follow Up
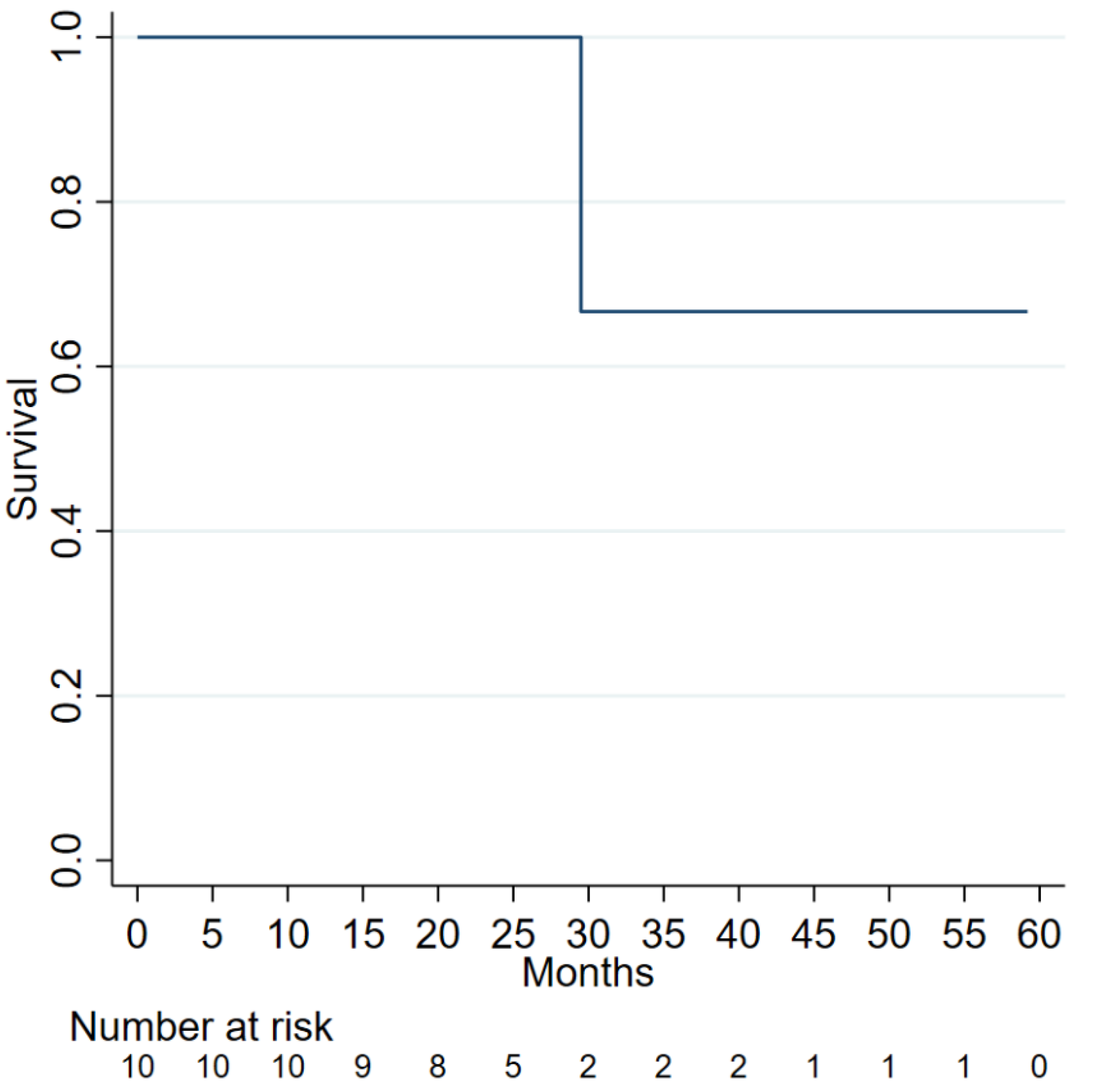
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Banales, J.M.; Cardinale, V.; Carpino, G.; Marzioni, M.; Andersen, J.B.; Invernizzi, P.; Lind, G.E.; Folseraas, T.; Forbes, S.J.; Fouassier, L.; et al. Expert consensus document: Cholangiocarcinoma: Current knowledge and future perspectives consensus statement from the European Network for the Study of Cholangiocarcinoma (ENS-CCA). Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 261–280. [Google Scholar] [CrossRef] [PubMed]
- Benson, A.B., 3rd; Abrams, T.A.; Ben-Josef, E.; Bloomston, P.M.; Botha, J.F.; Clary, B.M.; Covey, A.; Curley, S.A.; D’Angelica, M.I.; Davila, R.; et al. NCCN clinical practice guidelines in oncology: Hepatobiliary cancers. J. Natl. Compr. Cancer Netw. 2009, 7, 350–391. [Google Scholar] [CrossRef] [PubMed]
- Endo, I.; Gonen, M.; Yopp, A.C.; Dalal, K.M.; Zhou, Q.; Klimstra, D.; D’Angelica, M.; DeMatteo, R.P.; Fong, Y.; Schwartz, L.; et al. Intrahepatic cholangiocarcinoma: Rising frequency, improved survival, and determinants of outcome after resection. Ann. Surg. 2008, 248, 84–96. [Google Scholar] [CrossRef] [PubMed]
- Hyder, O.; Hatzaras, I.; Sotiropoulos, G.C.; Paul, A.; Alexandrescu, S.; Marques, H.; Pulitano, C.; Barroso, E.; Clary, B.M.; Aldrighetti, L.; et al. Recurrence after operative management of intrahepatic cholangiocarcinoma. Surgery 2013, 153, 811–818. [Google Scholar] [CrossRef]
- Spolverato, G.; Kim, Y.; Ejaz, A.; Alexandrescu, S.; Marques, H.; Aldrighetti, L.; Gamblin, T.C.; Pulitano, C.; Bauer, T.W.; Shen, F.; et al. Conditional Probability of Long-term Survival After Liver Resection for Intrahepatic Cholangiocarcinoma: A Multi-institutional Analysis of 535 Patients. JAMA Surg. 2015, 150, 538–545. [Google Scholar] [CrossRef]
- Tabrizian, P.; Jibara, G.; Hechtman, J.F.; Franssen, B.; Labow, D.M.; Schwartz, M.E.; Thung, S.N.; Sarpel, U. Outcomes following resection of intrahepatic cholangiocarcinoma. HPB 2015, 17, 344–351. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Li, J.; Xia, Y.; Gong, R.; Wang, K.; Yan, Z.; Wan, X.; Liu, G.; Wu, D.; Shi, L.; et al. Prognostic nomogram for intrahepatic cholangiocarcinoma after partial hepatectomy. J. Clin. Oncol. 2013, 31, 1188–1195. [Google Scholar] [CrossRef]
- Gupta, R.; Gupta, J. Strategies to improve survival of patients with intrahepatic cholangiocarcinoma undergoing liver transplantation. Hepatology 2017, 65, 1777–1778. [Google Scholar] [CrossRef]
- Rana, A.; Hong, J.C. Orthotopic liver transplantation in combination with neoadjuvant therapy: A new paradigm in the treatment of unresectable intrahepatic cholangiocarcinoma. Curr. Opin Gastroenterol. 2012, 28, 258–265. [Google Scholar] [CrossRef]
- Sapisochin, G.; Facciuto, M.; Rubbia-Brandt, L.; Marti, J.; Mehta, N.; Yao, F.Y.; Vibert, E.; Cherqui, D.; Grant, D.R.; Hernandez-Alejandro, R.; et al. Liver transplantation for “very early” intrahepatic cholangiocarcinoma: International retrospective study supporting a prospective assessment. Hepatology 2016, 64, 1178–1188. [Google Scholar] [CrossRef]
- Goldstein, R.M.; Stone, M.; Tillery, G.W.; Senzer, N.; Levy, M.; Husberg, B.S.; Gonwa, T.; Klintmalm, G. Is liver transplantation indicated for cholangiocarcinoma? Am. J. Surg. 1993, 166, 768–771; discussion 771–772. [Google Scholar] [CrossRef]
- Pichlmayr, R.; Weimann, A.; Oldhafer, K.J.; Schlitt, H.J.; Klempnauer, J.; Bornscheuer, A.; Chavan, A.; Schmoll, E.; Lang, H.; Tusch, G.; et al. Role of liver transplantation in the treatment of unresectable liver cancer. World J. Surg. 1995, 19, 807–813. [Google Scholar] [CrossRef] [PubMed]
- Schüle, S.; Altendorf-Hofmann, A.; Uteß, F.; Rauchfuß, F.; Freesmeyer, M.; Knösel, T.; Dittmar, Y.; Settmacher, U. Liver transplantation for hilar cholangiocarcinoma--a single-centre experience. Langenbecks Arch. Surg. 2013, 398, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Darwish Murad, S.; Kim, W.R.; Harnois, D.M.; Douglas, D.D.; Burton, J.; Kulik, L.M.; Botha, J.F.; Mezrich, J.D.; Chapman, W.C.; Schwartz, J.J.; et al. Efficacy of neoadjuvant chemoradiation, followed by liver transplantation, for perihilar cholangiocarcinoma at 12 US centers. Gastroenterology 2012, 143, 88–98.e83; quiz e14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, J.C.; Jones, C.M.; Duffy, J.P.; Petrowsky, H.; Farmer, D.G.; French, S.; Finn, R.; Durazo, F.A.; Saab, S.; Tong, M.J.; et al. Comparative analysis of resection and liver transplantation for intrahepatic and hilar cholangiocarcinoma: A 24-year experience in a single center. Arch. Surg. 2011, 146, 683–689. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marchan, E.M.; Landry, J.C. Neoadjuvant chemoradiation followed by orthotopic liver transplantation in cholangiocarcinomas: The emory experience. J. Gastrointest. Oncol. 2016, 7, 248–254. [Google Scholar] [CrossRef]
- Rea, D.J.; Heimbach, J.K.; Rosen, C.B.; Haddock, M.G.; Alberts, S.R.; Kremers, W.K.; Gores, G.J.; Nagorney, D.M. Liver transplantation with neoadjuvant chemoradiation is more effective than resection for hilar cholangiocarcinoma. Ann. Surg. 2005, 242, 451–461. [Google Scholar] [CrossRef]
- Sudan, D.; DeRoover, A.; Chinnakotla, S.; Fox, I.; Shaw, B., Jr.; McCashland, T.; Sorrell, M.; Tempero, M.; Langnas, A. Radiochemotherapy and transplantation allow long-term survival for nonresectable hilar cholangiocarcinoma. Am. J. Transpl. 2002, 2, 774–779. [Google Scholar] [CrossRef]
- Abdelrahim, M.; Esmail, A.; Abudayyeh, A.; Murakami, N.; Saharia, A.; McMillan, R.; Victor, D.; Kodali, S.; Shetty, A.; Nolte Fong, J.V.; et al. Transplant Oncology: An Evolving Field in Cancer Care. Cancers 2021, 13, 4911. [Google Scholar] [CrossRef]
- Meyer, C.G.; Penn, I.; James, L. Liver transplantation for cholangiocarcinoma: Results in 207 patients. Transplantation 2000, 69, 1633–1637. [Google Scholar] [CrossRef]
- Robles, R.; Figueras, J.; Turrión, V.S.; Margarit, C.; Moya, A.; Varo, E.; Calleja, J.; Valdivieso, A.; Valdecasas, J.C.; López, P.; et al. Spanish experience in liver transplantation for hilar and peripheral cholangiocarcinoma. Ann. Surg. 2004, 239, 265–271. [Google Scholar] [CrossRef]
- Abdelrahim, M.; Victor, D.; Esmail, A.; Kodali, S.; Graviss, E.A.; Nguyen, D.T.; Moore, L.W.; Saharia, A.; McMillan, R.; Fong, J.N.; et al. Transarterial Chemoembolization (TACE) Plus Sorafenib Compared to TACE Alone in Transplant Recipients with Hepatocellular Carcinoma: An Institution Experience. Cancers 2022, 14, 650. [Google Scholar] [CrossRef]
- Reddy, T.; Esmail, A.; Chang, J.C.; Ghobrial, R.M.; Abdelrahim, M. Utility of Cell-Free DNA Detection in Transplant Oncology. Cancers 2022, 14, 743. [Google Scholar] [CrossRef] [PubMed]
- Abdelrahim, M.; Esmail, A.; Saharia, A.; Abudayyeh, A.; Abdel-Wahab, N.; Diab, A.; Murakami, N.; Kaseb, A.O.; Chang, J.C.; Gaber, A.O.; et al. Utilization of Immunotherapy for the Treatment of Hepatocellular Carcinoma in the Peri-Transplant Setting: Transplant Oncology View. Cancers 2022, 14, 1760. [Google Scholar] [CrossRef] [PubMed]
- Renzulli, M.; Ramai, D.; Singh, J.; Sinha, S.; Brandi, N.; Ierardi, A.M.; Albertini, E.; Sacco, R.; Facciorusso, A.; Golfieri, R. Locoregional Treatments in Cholangiocarcinoma and Combined Hepatocellular Cholangiocarcinoma. Cancers 2021, 13, 3336. [Google Scholar] [CrossRef] [PubMed]
- Hastie, T.; Tibshirani, R.; Wainwright, M. Statistical Learning with Sparsity: The Lasso and Generalizations; Chapman and Hall/CRC: London, UK, 2019. [Google Scholar]
- Lasso, S. Stata Reference Manual: Release 16; Stata Press: College Station, TX, USA, 2020. [Google Scholar]
- Patel, T. Cholangiocarcinoma—Controversies and challenges. Nat. Rev. Gastroenterol. Hepatol. 2011, 8, 189–200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sapisochin, G.; de Lope, C.R.; Gastaca, M.; de Urbina, J.O.; López-Andujar, R.; Palacios, F.; Ramos, E.; Fabregat, J.; Castroagudín, J.F.; Varo, E.; et al. Intrahepatic cholangiocarcinoma or mixed hepatocellular-cholangiocarcinoma in patients undergoing liver transplantation: A Spanish matched cohort multicenter study. Ann. Surg. 2014, 259, 944–952. [Google Scholar] [CrossRef]
- Fu, B.S.; Zhang, T.; Li, H.; Yi, S.H.; Wang, G.S.; Xu, C.; Yang, Y.; Cai, C.J.; Lu, M.Q.; Chen, G.H. The role of liver transplantation for intrahepatic cholangiocarcinoma: A single-center experience. Eur. Surg. Res. 2011, 47, 218–221. [Google Scholar] [CrossRef]
- Valle, J.W.; Wasan, H.; Johnson, P.; Jones, E.; Dixon, L.; Swindell, R.; Baka, S.; Maraveyas, A.; Corrie, P.; Falk, S.; et al. Gemcitabine alone or in combination with cisplatin in patients with advanced or metastatic cholangiocarcinomas or other biliary tract tumours: A multicentre randomised phase II study—The UK ABC-01 Study. Br. J. Cancer 2009, 101, 621–627. [Google Scholar] [CrossRef]
- Kinzler, M.N.; Klasen, C.; Schulze, F.; Herrmann, E.; Schnitzbauer, A.A.; Trojan, J.; Zeuzem, S.; Wild, P.J.; Walter, D. Impact of Liver Fibrosis on Survival of Patients with Intrahepatic Cholangiocarcinoma Receiving Gemcitabine-Based Chemotherapy. J. Clin. Med. 2022, 11, 2057. [Google Scholar] [CrossRef]
- Hayashi, A.; Misumi, K.; Shibahara, J.; Arita, J.; Sakamoto, Y.; Hasegawa, K.; Kokudo, N.; Fukayama, M. Distinct Clinicopathologic and Genetic Features of 2 Histologic Subtypes of Intrahepatic Cholangiocarcinoma. Am. J. Surg. Pathol. 2016, 40, 1021–1030. [Google Scholar] [CrossRef] [PubMed]
- Jain, A.; Kwong, L.N.; Javle, M. Genomic Profiling of Biliary Tract Cancers and Implications for Clinical Practice. Curr. Treat. Options Oncol. 2016, 17, 58. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Ross, J.S. The potential role of comprehensive genomic profiling to guide targeted therapy for patients with biliary cancer. Therap. Adv. Gastroenterol. 2017, 10, 507–520. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Patients ID | Sex | Native Liver Diagnosis | Treatment Duration- Days | Days to Transplant | Recurrence or Rejection | Days to The Date of Recurrence or Rejection | Days to The Last Follow up | Days to Death |
|---|---|---|---|---|---|---|---|---|
| 1 | Female | HCCA | 603 | 8 | No | 813 | ||
| 2 | Male | IHCCA | 149 | 5 | Yes | 603 | 871 | 885 |
| 3 | Male | IHCCA | 250 | 20 | No | 824 | ||
| 4 | Male | IHCCA | 120 | 369 | No | 967 | ||
| 5 | Male | IHCCA | 83 | 472 | No | 1405 | ||
| 6 | Male | HCCA | 161 | 64 | No | 418 | ||
| 7 | Male | HCCA | 201 | 5 | No | 812 | ||
| 8 | Male | IHCCA | 206 | 79 | No | 831 | ||
| 9 | Male | IHCCA | 77 | 445 | No | 1834 | ||
| 10 | Female | IHCCA | 200 | 113 | No | 870 |
| The Basic Characteristics of the Included Patients Who Received Gemcitabine Plus Cisplatin as a Neo-Adjuvant Treatment for Cholangiocarcinoma Prior to Liver Transplantation | |
|---|---|
| Total | |
| N = 10 | |
| Age | |
| 62.71 (60.02–71.87) | |
| Gender | |
| Female | 2 (20.00) |
| Male | 8 (80.00) |
| Race | |
| Asian | 1 (10.00) |
| Black | 1 (10.00) |
| Caucasian | 8 (80.00) |
| Ethnicity | |
| Hispanic or Latino | 2 (20.00) |
| Not Hispanic or Latino | 8 (80.00) |
| Recurrence or rejection | |
| Yes | 1 (10.00) |
| no | 9 (90.00) |
| Recurrent time | 612.00 (612.00–612.00) |
| Days for GIM/CIS | 181.00 (120.00–250.00) |
| Death | |
| 0 | 9 (90.00) |
| 1 | 1 (10.00) |
| Follow-up time (days) | |
| 851.00 (813.00–967.00) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abdelrahim, M.; Al-Rawi, H.; Esmail, A.; Xu, J.; Umoru, G.; Ibnshamsah, F.; Abudayyeh, A.; Victor, D.; Saharia, A.; McMillan, R.; et al. Gemcitabine and Cisplatin as Neo-Adjuvant for Cholangiocarcinoma Patients Prior to Liver Transplantation: Case-Series. Curr. Oncol. 2022, 29, 3585-3594. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol29050290
Abdelrahim M, Al-Rawi H, Esmail A, Xu J, Umoru G, Ibnshamsah F, Abudayyeh A, Victor D, Saharia A, McMillan R, et al. Gemcitabine and Cisplatin as Neo-Adjuvant for Cholangiocarcinoma Patients Prior to Liver Transplantation: Case-Series. Current Oncology. 2022; 29(5):3585-3594. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol29050290
Chicago/Turabian StyleAbdelrahim, Maen, Hadeel Al-Rawi, Abdullah Esmail, Jiaqiong Xu, Godsfavour Umoru, Fahad Ibnshamsah, Ala Abudayyeh, David Victor, Ashish Saharia, Robert McMillan, and et al. 2022. "Gemcitabine and Cisplatin as Neo-Adjuvant for Cholangiocarcinoma Patients Prior to Liver Transplantation: Case-Series" Current Oncology 29, no. 5: 3585-3594. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol29050290