In Vitro Physico-Chemical Characterization and Standardized In Vivo Evaluation of Biocompatibility of a New Synthetic Membrane for Guided Bone Regeneration


 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Control Membrane
2.2. Physico-Chemical Characterization of Experimental Membranes
2.3. Animal Characterization and Experimental Group
2.4. Surgical Procedure and Production of Samples
3. Results
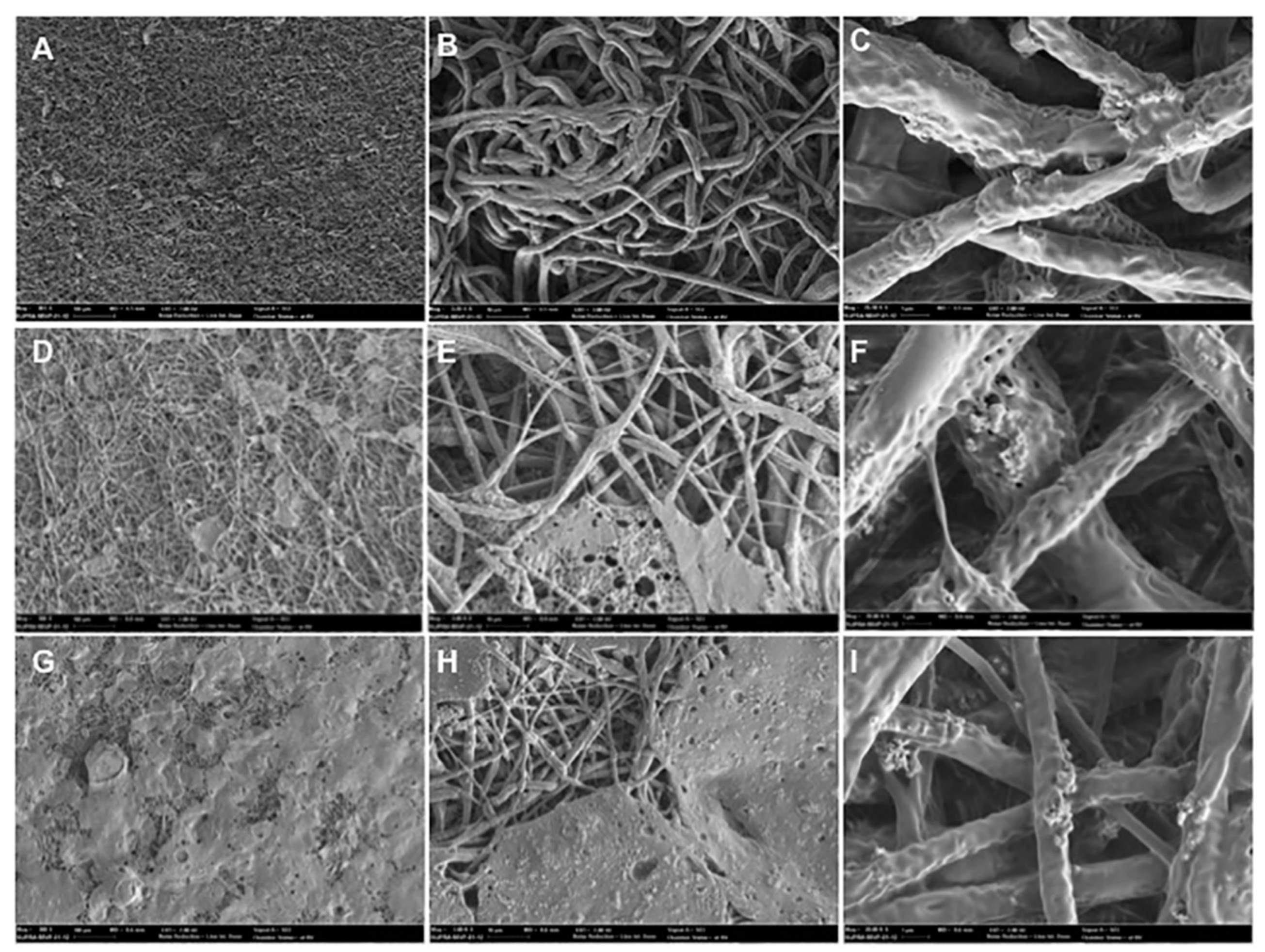
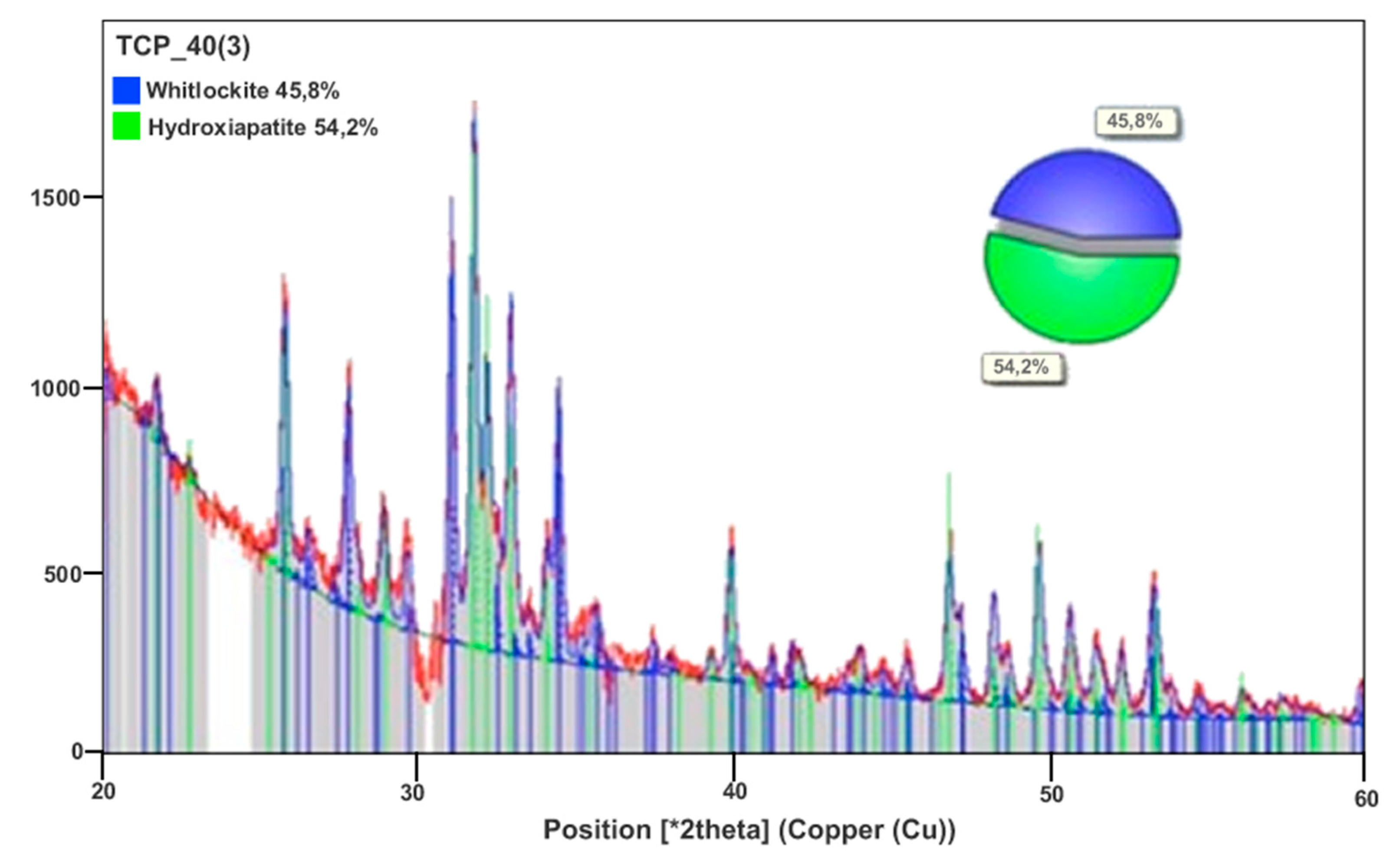
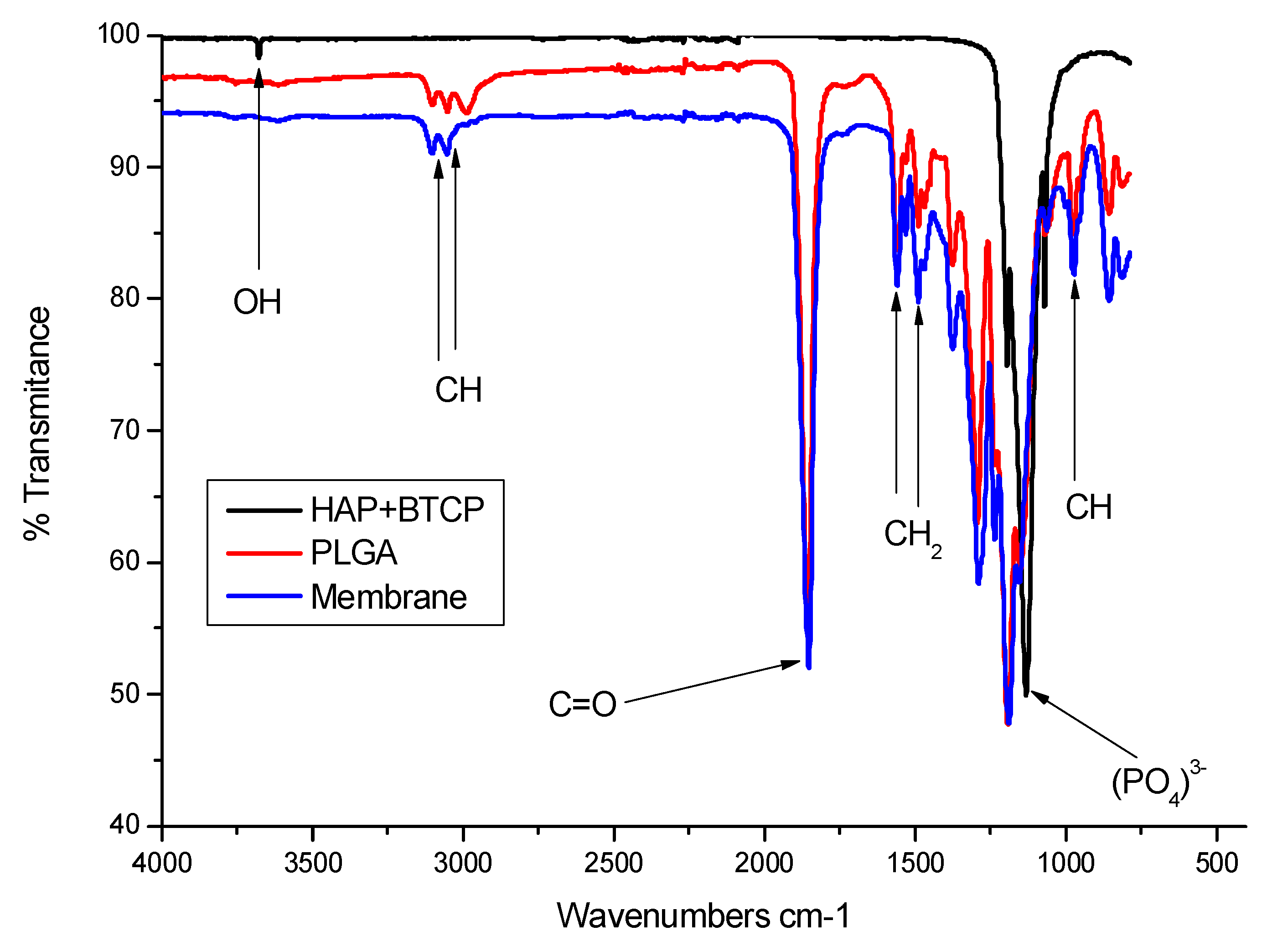
3.1. Structure and Characteristics of the PLGA Membrane
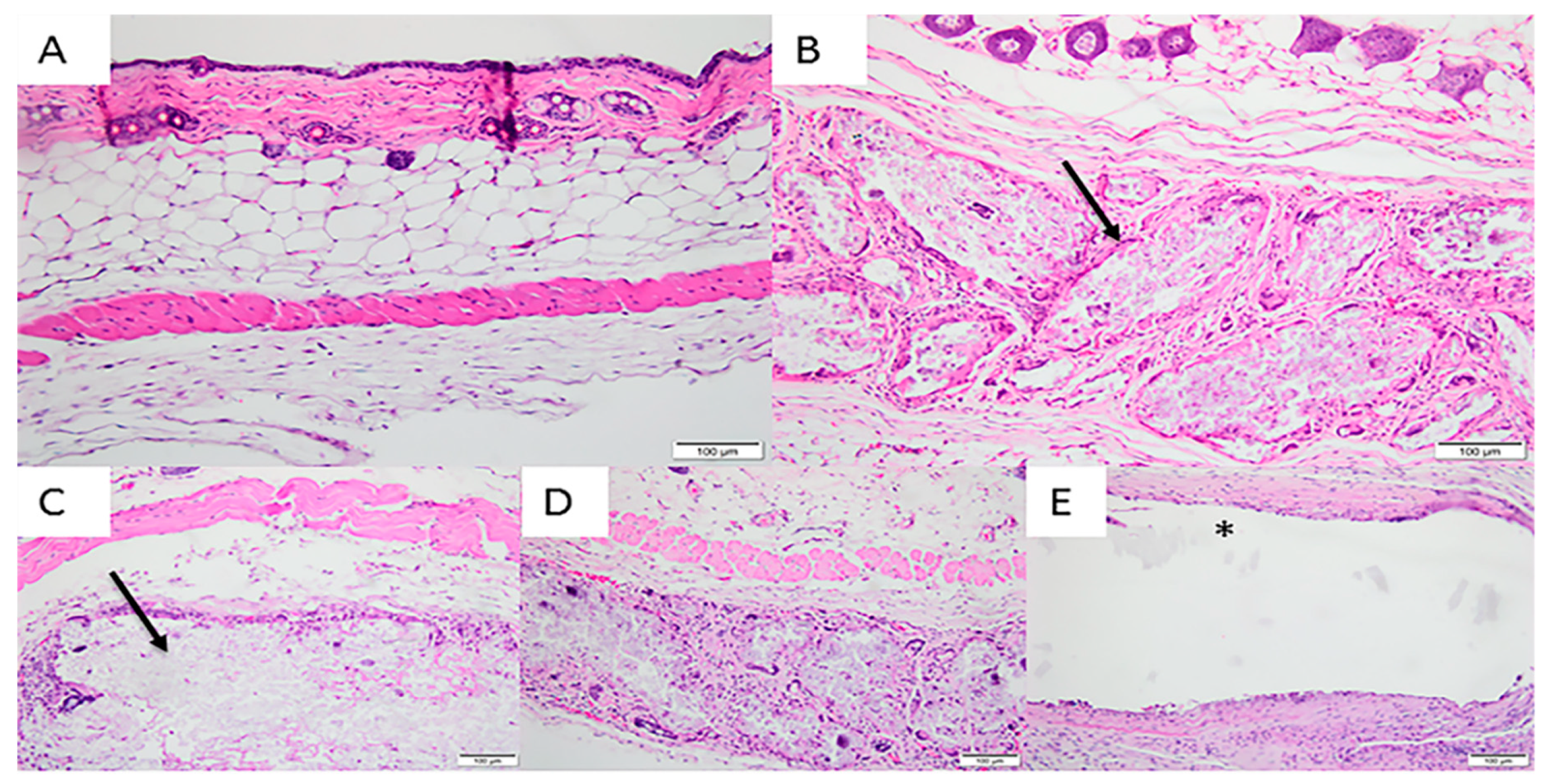
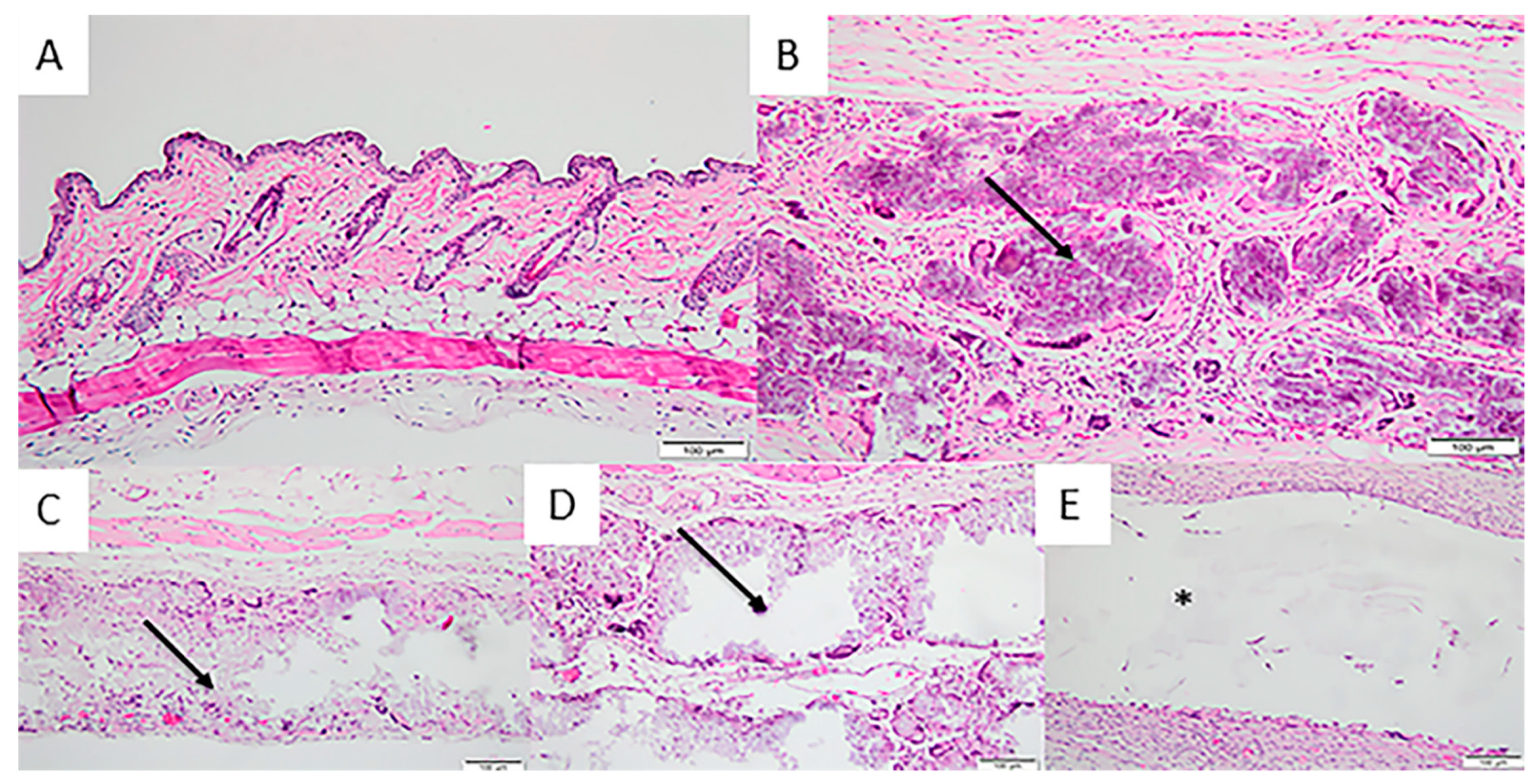
3.2. In Vivo Implantation
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Melcher, A.H. On the repair potential of periodontal tissues. J. Periodontol. 1976, 47, 256–260. [Google Scholar] [CrossRef] [PubMed]
- Arunjaroensuk, S.; Panmekiate, S.; Pimkhaokham, A. The Stability of Augmented Bone Between Two Different Membranes Used for Guided Bone Regeneration Simultaneous with Dental Implant Placement in the Esthetic Zone. Int. J. Oral Maxillofac. Implants 2017, 33, 206–216. [Google Scholar] [CrossRef] [PubMed]
- Benic, G.I.; Hammerle, C.H. Horizontal bone augmentation by means of guided bone regeneration. Periodontology 2000 2014, 66, 13–40. [Google Scholar] [CrossRef]
- Schwarz, F.; Herten, M.; Ferrari, D.; Wieland, M.; Schmitz, L.; Engelhardt, E.; Becker, J. Guided bone regeneration at dehiscence-type defects using biphasic hydroxyapatite + beta tricalcium phosphate (Bone Ceramic®) or a collagen-coated natural bone mineral (BioOss Collagen®): An immunohistochemical study in dogs. Int. J. Oral Maxillofac. Surg. 2007, 36, 1198–1206. [Google Scholar] [CrossRef]
- Guda, T.; Walker, J.A.; Singleton, B.M.; Hernandez, J.W.; Son, J.S.; Kim, S.G.; Oh, D.S.; Appleford, M.R.; Ong, J.L.; Wenke, J.C. Guided bone regeneration in long-bone defects with a structural hydroxyapatite graft and collagen membrane. Tissue Eng. Part A 2013, 19, 1879–1888. [Google Scholar] [CrossRef]
- Peng, S.W.; Li, C.W.; Chiu, I.M.; Wang, G.J. Nerve guidance conduit with a hybrid structure of a PLGA microfibrous bundle wrapped in a micro/nanostructured membrane. Int. J. Nanomed. 2017, 11, 421–432. [Google Scholar] [CrossRef] [PubMed]
- Shao, H.J.; Chen, C.S.; Lee, I.C.; Wang, J.H.; Young, T.H. Designing a three-dimensional expanded polytetrafluoroethylene-poly(lactic-co-glycolic acid) scaffold for tissue engineering. Artif. Organs 2009, 33, 309–317. [Google Scholar] [CrossRef] [PubMed]
- Mao, D.; Li, Q.; Bai, N.; Dong, H.; Li, D. Porous stable poly(lactic acid)/ethyl cellulose/hydroxyapatite composite scaffolds prepared by a combined method for bone regeneration. Carbohydr. Polym. 2018, 15, 104–111. [Google Scholar] [CrossRef]
- Lee, S.W.; Kim, S.G. Membranes for the Guided Bone Regeneration. Maxillofac. Plast. Reconstr. Surg. 2014, 36, 239–246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lv, Q.; Deng, M.; Ulery, B.D.; Nair, L.S.; Laurencin, C.T. Nano-ceramic composite scaffolds for bioreactor-based bone engineering. Clin. Orthop. Relat. Res. 2013, 8, 2422–2433. [Google Scholar] [CrossRef] [PubMed]
- Hartgerink, J.D.; Beniash, E.; Stupp, S.I. Self-assembly and mineralization of peptide-amphiphile nanofibers. Science 2001, 5547, 1684–1688. [Google Scholar] [CrossRef]
- Murphy, W.L.; Mooney, D.J. Bioinspired growth of crystalline carbonate apatite on biodegradable polymer substrata. J. Am. Chem. Soc. 2002, 9, 1910–1917. [Google Scholar] [CrossRef]
- Barrère, F.; Layrolle, P.; Van Blitterswijk, C.A.; De Groot, K. Biomimetic coatingson titanium: A crystal growth study of octacalcium phosphate. J. Mater. Sci. Mater. Med. 2001, 6, 529–534. [Google Scholar] [CrossRef]
- Fu, L.; Wang, Z.; Dong, S.; Cai, Y.; Ni, Y.; Zhang, T.; Wang, L.; Zhou, Y. Bilayer Poly(Lactic-co-glycolic acid)/Nano-Hydroxyapatite Membrane with Barrier Function and Osteogenesis Promotion for Guided Bone Regeneration. Materials 2017, 3, 257. [Google Scholar] [CrossRef]
- Balmain, N.; Legros, R.; Bonel, G. X-ray diffraction of calcined bone tissue: A reliable method for the determination of bone Ca/Pmolar ratio. Calcif. Tissue Int. 1982, 34, s93–s98. [Google Scholar]
- Sanaei-Rad, P.; Jafarzadeh Kashi, T.S.; Seyedjafari, E.; Soleimani, M. Enhancement of stem cell differentiation to osteogenic lineage on hydroxyapatite-coated hybrid PLGA/gelatin nanofiber scaffolds. Biologicals 2016, 44, 511–516. [Google Scholar] [CrossRef]
- Tan, H.Y.; Widjaja, E.; Boey, F.; Loo, S.C. Spectroscopy techniques for analyzing the hydrolysis of PLGA and PLLA. J. Biomed. Mater. Res. B Appl. Biomater. 2009, 1, 433–440. [Google Scholar] [CrossRef]
- Jin, Q.; Wang, X.M.; Wang, X.F.; Li, X.D.; Ma, J.F. The efficacy of collagen-hydroxyapatite composite membrane on bone regeneration. Hua Xi Kou Qiang Yi Xue Za Zhi 2011, 29, 21–26. [Google Scholar]
- Buser, D.; Dula, K.; Hirt, H.P.; Schenk, R.K. Lateral ridge augmentation using autografts and barrier membranes: A clinical study with 40 partially edentulous patients. J. Oral Maxillofac. Surg. 1996, 54, 420–432. [Google Scholar] [CrossRef]
- Hwang, K.S.; Choi, J.W.; Kim, J.H.; Chung, H.Y.; Jin, S.; Shim, J.H.; Yun, W.S.; Jeong, C.M.; Huh, J.B. Comparative Efficacies of Collagen-Based 3D Printed PCL/PLGA/beta-TCP Composite Block Bone Grafts and Biphasic Calcium Phosphate Bone Substitute for Bone Regeneration. Materials 2017, 10, 421. [Google Scholar] [CrossRef]
- Chen, G.; Xia, Y.; Lu, X.; Zhou, X.; Zhang, F.; Gu, N. Effects of surface functionalization of PLGA membranes for guided bone regeneration on proliferation and behavior of osteoblasts. J. Biomed. Mater. Res. A 2013, 101, 44–53. [Google Scholar] [CrossRef]
- Knecht, S.; Erggelet, C.; Endres, M.; Sittinger, M.; Kaps, C.; Stussi, E. Mechanical testing of fixation techniques for scaffold-based tissue-engineered grafts. J. Biomed. Mater. Res. B Appl. Biomater. 2007, 83, 50–57. [Google Scholar] [CrossRef]
- Deng, X.L.; Sui, G.; Zhao, M.L.; Chen, G.Q.; Yang, X.P. Poly(L-lactic acid)/hydroxyapatite hybrid nanofibrous scaffolds prepared by electrospinning. J. Biomater. Sci. Polym. Ed. 2007, 18, 117–130. [Google Scholar] [CrossRef]
- Seyedjafari, E.; Soleimani, M.; Ghaemi, N.; Shabani, I. Nanohydroxyapatite-coated electrospun poly(l-lactide) nanofibers enhance osteogenic differentiation of stem cells and induce ectopic bone formation. Biomacromolecules 2010, 8, 3118–3125. [Google Scholar] [CrossRef]
- Minabe, M. A critical review of the biologic rationale for guided tissue regeneration. J. Periodontol. 1991, 62, 171–179. [Google Scholar] [CrossRef]
- Oliveira, R.C.; Menezes, R.; Cestari, T.M.; Taga, E.M.; Taga, R.; Buzalaf, M.A.R.; Granjeiro, J.M. Tissue response to a membrane of demineralized bovine cortical bone implanted in the subcutaneous tissue of rats. Braz. Dent. J. 2004, 15, 3–8. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Carbon % | Hydrogen% | Nitrogen % | |
|---|---|---|---|
| 1 | 39.5 | 4.7 | 0.1 |
| 2 | 39.2 | 4.3 | 0.1 |
| Mean | 39.4 | 4.5 | 0.1 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
da Costa Pereira, L.; de Almeida Barros Mourão, C.F.; Neves Novellino Alves, A.T.; Figueiredo de Brito Resende, R.; Pinheiro Guedes de Uzeda, M.J.; Granjeiro, J.M.; Seabra Louro, R.; Diuana Calasans-Maia, M. In Vitro Physico-Chemical Characterization and Standardized In Vivo Evaluation of Biocompatibility of a New Synthetic Membrane for Guided Bone Regeneration. Materials 2019, 12, 1186. https://0-doi-org.brum.beds.ac.uk/10.3390/ma12071186
da Costa Pereira L, de Almeida Barros Mourão CF, Neves Novellino Alves AT, Figueiredo de Brito Resende R, Pinheiro Guedes de Uzeda MJ, Granjeiro JM, Seabra Louro R, Diuana Calasans-Maia M. In Vitro Physico-Chemical Characterization and Standardized In Vivo Evaluation of Biocompatibility of a New Synthetic Membrane for Guided Bone Regeneration. Materials. 2019; 12(7):1186. https://0-doi-org.brum.beds.ac.uk/10.3390/ma12071186
Chicago/Turabian Styleda Costa Pereira, Lívia, Carlos Fernando de Almeida Barros Mourão, Adriana Terezinha Neves Novellino Alves, Rodrigo Figueiredo de Brito Resende, Marcelo José Pinheiro Guedes de Uzeda, José Mauro Granjeiro, Rafael Seabra Louro, and Mônica Diuana Calasans-Maia. 2019. "In Vitro Physico-Chemical Characterization and Standardized In Vivo Evaluation of Biocompatibility of a New Synthetic Membrane for Guided Bone Regeneration" Materials 12, no. 7: 1186. https://0-doi-org.brum.beds.ac.uk/10.3390/ma12071186