Accuracy of Three Impression Materials on the Totally Edentulous Maxilla: In Vitro/In Silico Comparative Analysis


 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Preparation of the Reference Typodont
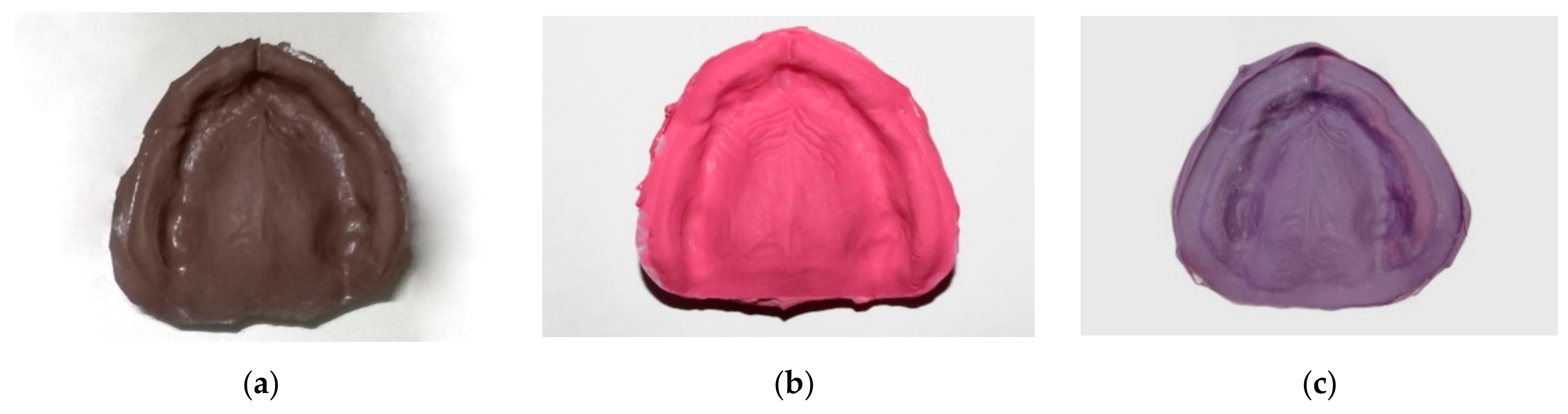
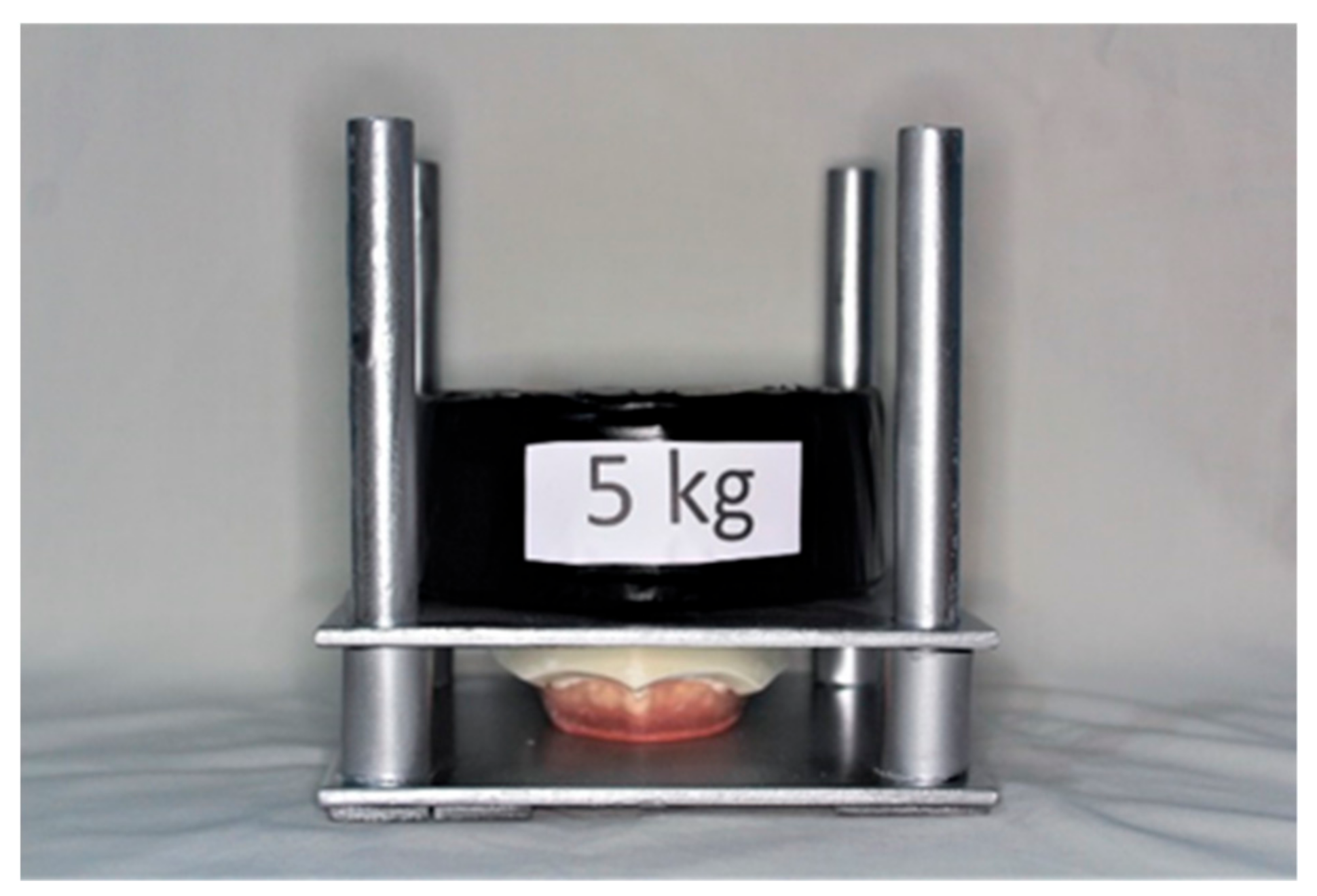
2.2. Conventional Impression Procedure
- Polysulfide: manual mixing time = 50 s (mixing ratio 1:1); material placement into the tray and impression making = 20 s; removal of the impression tray from the tester = 15 min from the beginning of mixing;
- Polyvinyl siloxane: for initial use, a small amount of material was extruded for 5 s and then discarded; the extruded material was deleted, then it was mounted on the mixing tip; auto-mixing (mixing ratio 1:1); material placement into the tray and impression making = 30 s; removal of the impression tray from the tester = 15 min from the beginning of mixing;
- Polyether: for initial use, a small amount of material was extruded for 5 s and then discarded; auto-mixing (mixing ratio 5:1, 300 ml of base paste and 60 ml of catalyst paste); material placement into the tray and impression making = 30 s; removal of the impression tray from the tester = 15 min from the beginning of mixing.
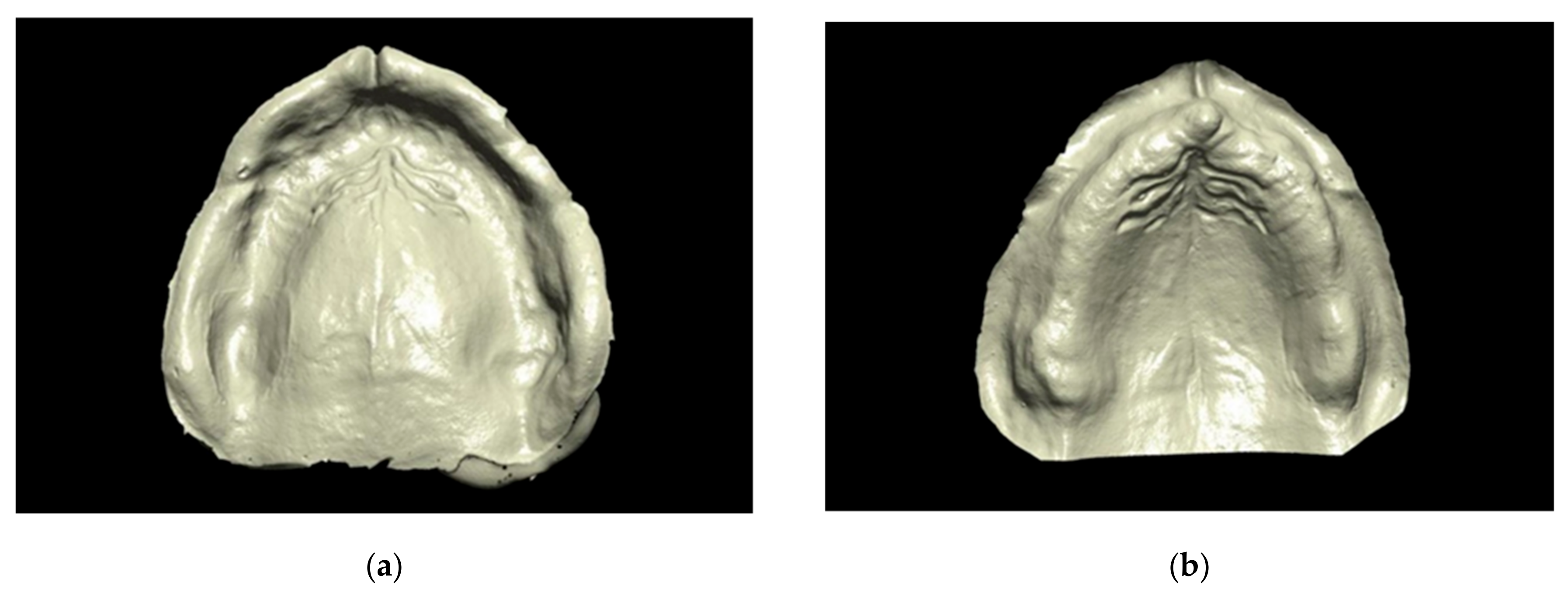
2.3. Digitization of the Conventional Impressions
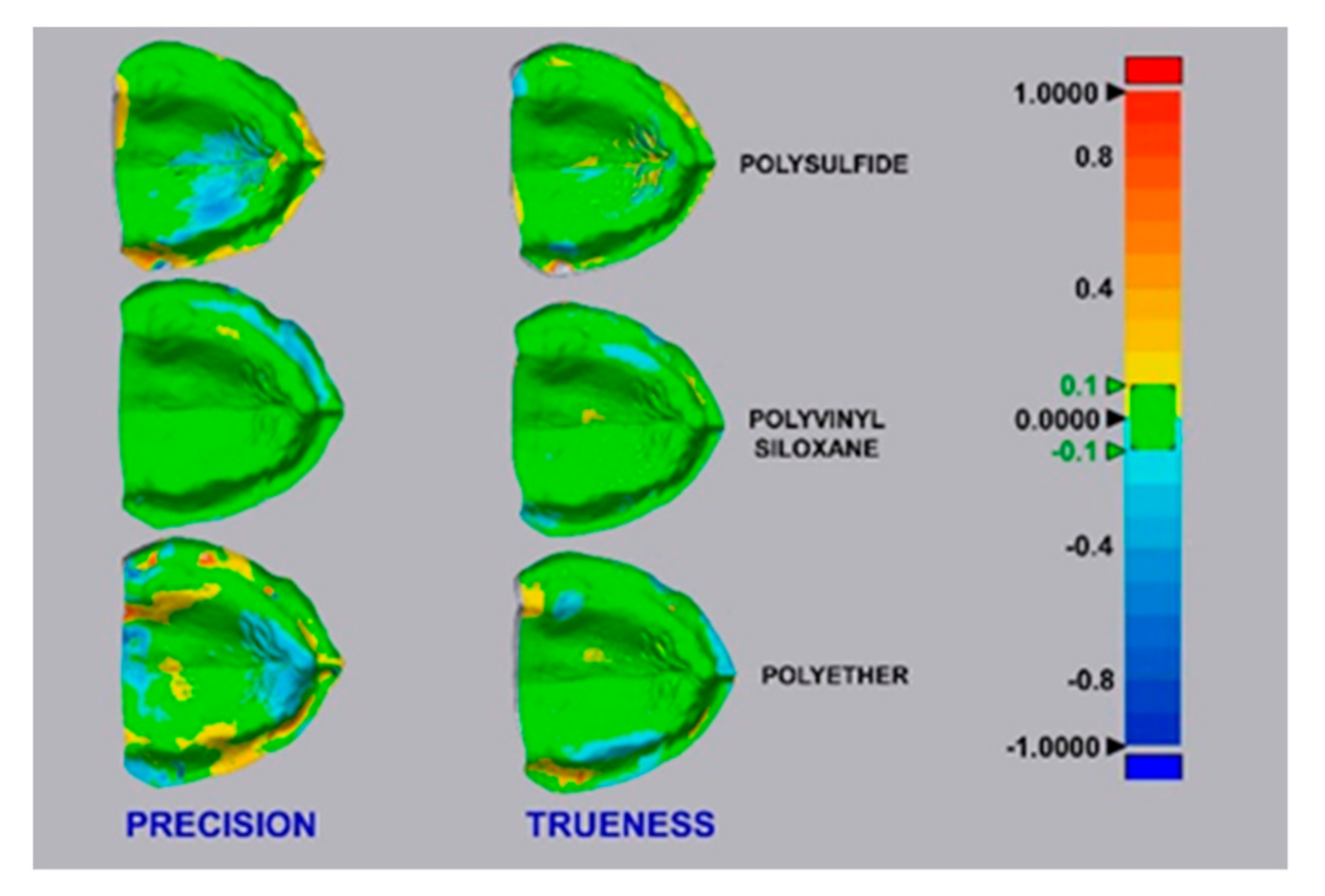
2.4. Digital Analysis
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Available online: https://www.encyclopedia.com/education/encyclopedias-almanacs-transcripts-and-maps/edentulism (accessed on 3 December 2019).
- Emami, E.; de Souza, R.F.; Kabawat, M.; Feine, J.S. The impact of edentulism on oral and general health. Int. J. Dent. 2013, 2013, 498305. [Google Scholar] [CrossRef] [PubMed]
- Cunha-Cruz, J.; Hujoel, P.P.; Nadanovsky, P. Secular trends in socio-economic disparities in edentulism: USA, 1972–2001. J. Dent. Res. 2007, 86, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Allen, J. Artificial Dentures. Am. J. Dent. Sci. 1860, 10, 16–20. [Google Scholar] [PubMed]
- Allen, J. Artificial Dentures. Am. J. Dent. Sci. 1860, 10, 239–242. [Google Scholar]
- Lemos, M.M.C.; Zanin, L.; Jorge, M.L.R.; Florio, F.M. Oral health conditions and self-perception among edentulous individuals with different prosthetic status. Braz. J. Oral Sci. 2013, 12, 5–10. [Google Scholar]
- Rameez, M.; Razi, S.S.; Farhan, F.; Kumar, B.; Rashid, H. Clinical implications of elastomeric impression materials used for complete denture construction. Dent. Med. Res. 2018, 6, 19–23. [Google Scholar]
- Page, H.L. Mucostatics—A practical comparison. TIC 1947, 4, 2–10. [Google Scholar]
- Boucher, C.O. Impressions for complete dentures. J. Am. Dent. Assoc. 1943, 30, 14–25. [Google Scholar] [CrossRef]
- Boucher, C.O. A critical analysis of mid-century impression techniques for full dentures. J. Prosthet. Dent. 1951, 1, 472–491. [Google Scholar] [CrossRef]
- Rashid, H.; Vohra, F.A.; Haidry, T.Z.; Devi, G. Stabilizing mandibular complete dentures using the neutral zone impression technique. J. Pak. Dent. Assoc. 2013, 22, 154–159. [Google Scholar]
- Drago, C.J. A retrospective comparison of two definitive impression techniques and their associated postinsertion adjustments in complete denture prosthodontics. J. Prosthodont. 2003, 12, 192–197. [Google Scholar] [CrossRef]
- McCord, J.F.; Grant, A.A. Impression making. Br. Dent. J. 2000, 188, 484–492. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H. Improved digital impressions of edentulous areas. J. Prosthet. Dent. 2017, 117, 448–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fang, J.H.; An, X.; Jeong, S.M.; Choi, B.H. Digital intraoral scanning technique for edentulous jaws. J. Prosthet. Dent. 2018, 119, 733–735. [Google Scholar] [CrossRef]
- Goodacre, B.J.; Goodacre, C.J.; Baba, N.Z. Using Intraoral Scanning to Capture Complete Denture Impressions, Tooth Positions, and Centric Relation Records. Int. J. Prosthodont. 2018, 31, 377–381. [Google Scholar] [CrossRef]
- Fang, Y.; Fang, J.H.; Jeong, S.M.; Choi, B.H. A Technique for Digital Impression and Bite Registration for a Single Edentulous Arch. J. Prosthodont. 2019, 28, 519–523. [Google Scholar] [CrossRef]
- Fang, J.H.; An, X.; Jeong, SM.; Choi, BH. Development of complete dentures based on digital intraoral impressions-Case report. J. Prosthodont. Res. 2018, 62, 116–120. [Google Scholar] [CrossRef]
- Chebib, N.; Kalberer, N.; Srinivasan, M.; Maniewicz, S.; Perneger, T.; Müller, F. Edentulous jaw impression techniques: An in vivo comparison of trueness. J. Prosthet. Dent. 2019, 121, 623–630. [Google Scholar] [CrossRef]
- Jain, A.R.; Dhanraj, M. A clinical review of spacer design for conventional complete denture. Biol. Med. 2016, 8, 5. [Google Scholar] [CrossRef] [Green Version]
- Passamonti, G. Relationship between the two arches and its effect in the diagnosis and treatment of complete denture prosthesis. Quintessence Int. Dent. Dig. 1979, 10, 37–51. [Google Scholar]
- Moore, R.J.; Watts, J.T.; Hood, J.A.; Burritt, D.J. Intra-oral temperature variation over 24 hours. Eur. J. Orthod. 1999, 21, 249–261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gonçalves, F.S.; Popoff, D.A.; Castro, C.D.; Silva, G.C.; Magalhães, C.S.; Moreira, A.N. Dimensional stability of elastomeric impression materials: A critical review of the literature. Eur. J. Prosthodont. Restor. Dent. 2011, 19, 163–166. [Google Scholar] [PubMed]
- Mandelli, F.; Gherlone, E.; Gastaldi, G.; Ferrari, M. Evaluation of the accuracy of extraoral laboratory scanners with a single-tooth abutment model: A 3D analysis. J. Prosth. Res. 2017, 61, 363–370. [Google Scholar] [CrossRef] [PubMed]
- Imburgia, M.; Logozzo, S.; Hauschild, U.; Veronesi, G.; Mangano, C.; Mangano, F.G. Accuracy of four intraoral scanners in oral implantology: A comparative in vitro study. BMC Oral Health 2017, 17, 92. [Google Scholar] [CrossRef] [PubMed]
- International Organization for Standardization. ISO 5725-1. Accuracy (trueness and precision) of measurement methods and results Part 1: General principles and definitions. Stat. Methods Qual. Control 1994, 2, 9–29. [Google Scholar]
- Sim, J.Y.; Jang, Y.; Kim, W.C.; Kim, H.Y.; Lee, D.H.; Kim, J.H. Comparing the accuracy (trueness and precision) of models of fixed dental prostheses fabricated by digital and conventional workflows. J. Prosthodont. Res. 2019, 63, 25–30. [Google Scholar] [CrossRef]
- Marino, G.; Canton, A.; Marino, A. Moderno Trattato di Protesi Mobile Completa, 1st ed.; Edizioni Martina: Bologna, Italy, 2014; pp. 34–38. [Google Scholar]
- Utz, K.H. Abformung zahnloser Kiefer. In Totalprothesen, 4th ed.; Koeck, B., Ed.; Elsevier: Munich, Germany, 2005; pp. 57–94. [Google Scholar]
- Regis, R.R.; Alves, C.C.; Rocha, S.S.; Negreiros, W.A.; Freitas-Pontes, K.M. The importance of a two-step impression procedure for complete denture fabrication: A systematic review of the literature. J. Oral Rehabil. 2016, 43, 771–777. [Google Scholar] [CrossRef]
- Lo Russo, L.; Salamini, A. Removable complete digital dentures: A workflow that integrates open technologies. J. Prosthet. Dent. 2018, 119, 727–732. [Google Scholar] [CrossRef]
- Lo Russo, L.; Salamini, A. Single-arch digital removable complete denture: A workflow that starts from the intraoral scan. J. Prosthet. Dent. 2018, 120, 20–24. [Google Scholar] [CrossRef]
- Mangano, F.; Gandolfi, A.; Luongo, G.; Logozzo, S. Intraoral scanners in dentistry: A review of the current literature. BMC Oral Health 2017, 17, 149. [Google Scholar] [CrossRef] [Green Version]
- Bilgin, M.S.; Baytaroğlu, E.N.; Erdem, A.; Dilber, E. A review of computer-aided design/computer-aided manufacture techniques for removable denture fabrication. Eur. J. Dent. 2016, 10, 286–291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- AlHelal, A.; AlRumaih, H.S.; Kattadiyil, M.T.; Baba, N.Z.; Goodacre, C.J. Comparison of retention between maxillary milled and conventional denture bases: A clinical study. J. Prosthet. Dent. 2017, 117, 233–238. [Google Scholar] [CrossRef] [PubMed]
- McLaughlin, J.B.; Ramos, V., Jr.; Dickinson, D.P. Comparison of Fit of Dentures Fabricated by Traditional Techniques Versus CAD/CAM Technology. J. Prosthodont. 2019, 28, 428–435. [Google Scholar] [CrossRef] [PubMed]
- Bidra, A.S.; Taylor, T.D.; Agar, J.R. Computer-aided technology for fabricating complete dentures: Systematic review of historical background, current status, and future perspectives. J. Prosthet. Dent. 2013, 109, 361–366. [Google Scholar] [CrossRef]
- Patzelt, S.B.; Vonau, S.; Stampf, S.; Att, W. Assessing the feasibility and accuracy of digitizing edentulous jaws. J. Am. Dent. Assoc. 2013, 144, 914–920. [Google Scholar] [CrossRef]
- Jeong, I.D.; Lee, J.J.; Jeon, J.H.; Kim, J.H.; Kim, H.Y.; Kim, W.C. Accuracy of complete- arch model using an intraoral video scanner: An in vitro study. J. Prosthet. Dent. 2016, 115, 755–759. [Google Scholar] [CrossRef]
- Peng, L.; Chen, L.; Harris, B.T.; Bhandari, B.; Morton, D.; Lin, W.S. Accuracy and reproducibility of virtual edentulous casts created by laboratory impression scan protocols. J. Prosthet. Dent. 2018, 120, 389–395. [Google Scholar] [CrossRef]
- Nedelcu, R.; Olsson, P.; Nyström, I.; Rydén, J.; Thor, A. Accuracy and precision of 3 intraoral scanners and accuracy of conventional impressions: A novel in vivo analysis method. J. Dent. 2018, 69, 110–118. [Google Scholar] [CrossRef]
- Patzelt, S.B.; Emmanouilidi, A.; Stampf, S.; Strub, J.R.; Att, W. Accuracy of full-arch scans using intraoral scanners. Clin. Oral Investig. 2014, 18, 1687–1694. [Google Scholar] [CrossRef]
- Spoto, G. Materiali e Tecnologie Odontostomatologiche, 2nd ed.; Ariesdue: Milan, Italy, 2013; pp. 169–174. [Google Scholar]
- Craig, R.G.; Robert, G. Restorative Dental Materials, 11th ed.; Elsevier: Amsterdam, The Netherlands, 2002; p. 12. [Google Scholar]
- Rubel, B.S. Impression materials: A comparative review of impression materials most commonly used in restorative dentistry. Dent. Clin. North Am. 2007, 51, 629–642. [Google Scholar] [CrossRef]
- Giordano, R. Impression materials: Basic properties. Gen. Dent. 2000, 48, 510–516. [Google Scholar] [PubMed]
- Marino, G.; Canton, A. La Protesi Parziale Rimovibile Dalla Teoria Alla Pratica, 1st ed.; Edizioni Martina: Bologna, Italy, 2002; pp. 6–7. [Google Scholar]
- Reich, S.; Gozdowski, S.; Trentzsch, L.; Frankenberger, R.; Lohbauer, U. Marginal fit of heatpressed vs. CAD/CAM processed all-ceramic onlays using a milling unit prototype. Oper. Dent. 2008, 33, 644–650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ushiwata, O.; de Moraes, J.V. Method for marginal measurements of restorations: Accessory device for toolmakers microscope. J. Prosthet. Dent. 2000, 83, 362–366. [Google Scholar] [CrossRef]
- Heboyan, A.G. Marginal and internal fit of fixed prosthodontic constructions: A literature review. Int. J. Dent. Res. Rev. 2019, 2, 19. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
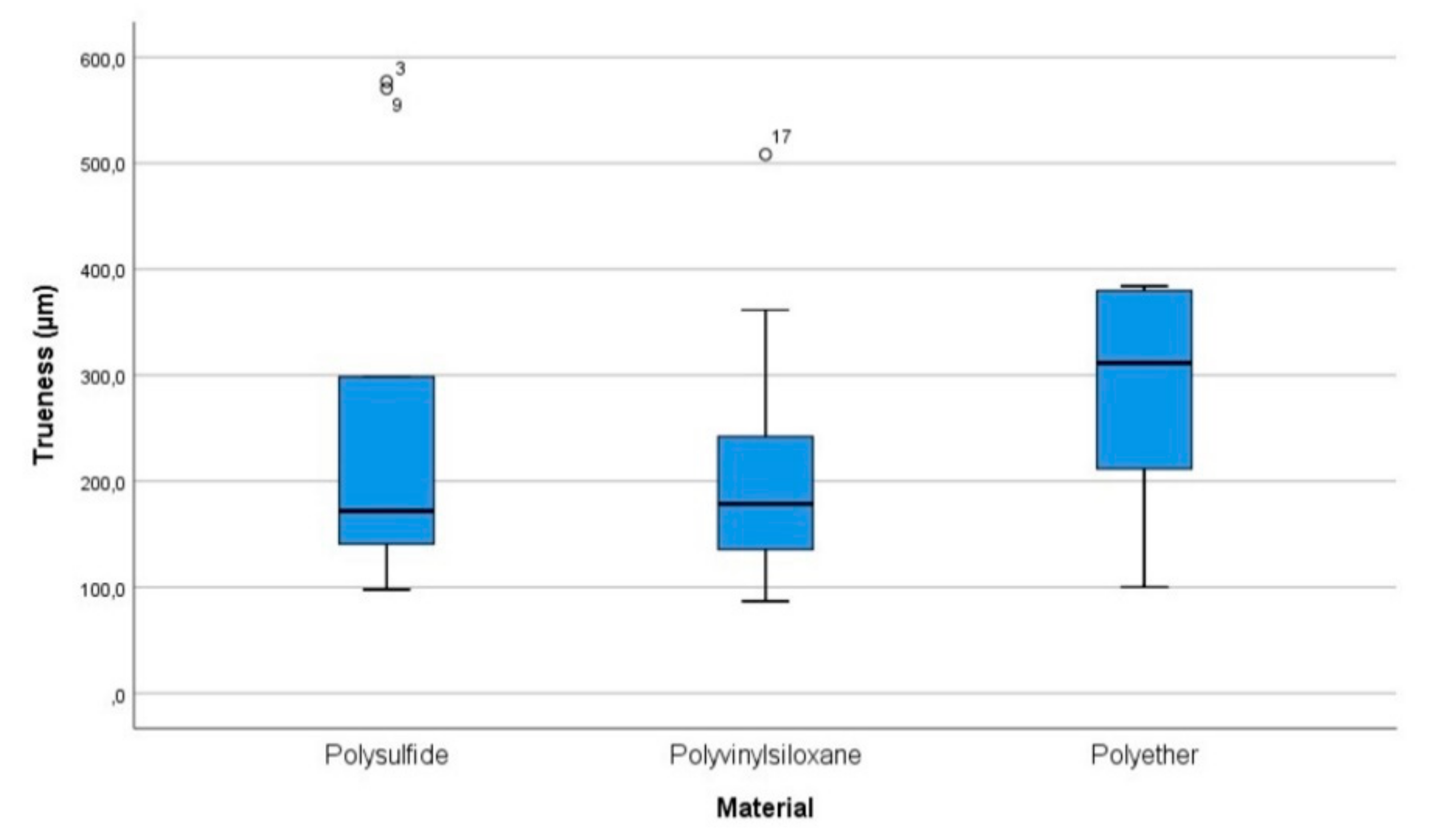
| Material Scanned | Lower-Upper Bound (95% CI) | Mean | Standard Error |
|---|---|---|---|
| polysulfide | 121.3–378.5 | 249.9 | 56.8531 |
| polyvinyl siloxane | 123.1–310.6 | 216.8 | 41.4459 |
| polyether | 219.9–362.3 | 291.1 | 31.4736 |
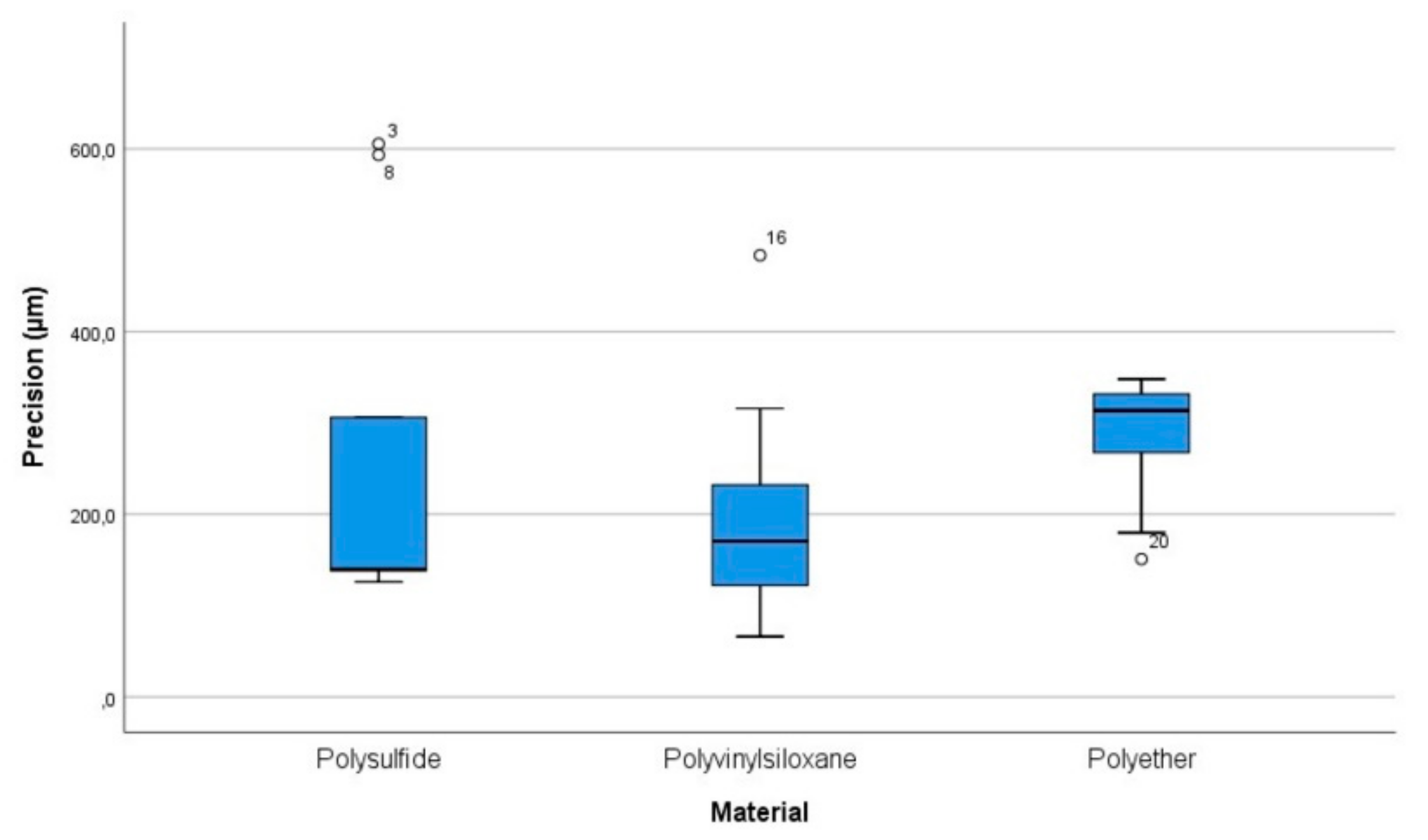
| Material Scanned | Lower-Upper Bound (95% CI) | Mean | Standard Error |
|---|---|---|---|
| polysulfide | 108.8–415 | 261.9 | 66.4043 |
| polyvinyl siloxane | 111.9–306.8 | 209.4 | 42.2547 |
| polyether | 227.9–338.1 | 283 | 23.8969 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zarone, F.; Ruggiero, G.; Di Mauro, M.I.; Spagnuolo, G.; Ferrari, M.; Sorrentino, R. Accuracy of Three Impression Materials on the Totally Edentulous Maxilla: In Vitro/In Silico Comparative Analysis. Materials 2020, 13, 515. https://0-doi-org.brum.beds.ac.uk/10.3390/ma13030515
Zarone F, Ruggiero G, Di Mauro MI, Spagnuolo G, Ferrari M, Sorrentino R. Accuracy of Three Impression Materials on the Totally Edentulous Maxilla: In Vitro/In Silico Comparative Analysis. Materials. 2020; 13(3):515. https://0-doi-org.brum.beds.ac.uk/10.3390/ma13030515
Chicago/Turabian StyleZarone, Fernando, Gennaro Ruggiero, Maria Irene Di Mauro, Gianrico Spagnuolo, Marco Ferrari, and Roberto Sorrentino. 2020. "Accuracy of Three Impression Materials on the Totally Edentulous Maxilla: In Vitro/In Silico Comparative Analysis" Materials 13, no. 3: 515. https://0-doi-org.brum.beds.ac.uk/10.3390/ma13030515