
Sustained Release of Bone Morphogenetic Protein-2 through Alginate Microbeads Enhances Bone Regeneration in Rabbit Tibial Metaphyseal Defect Model



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
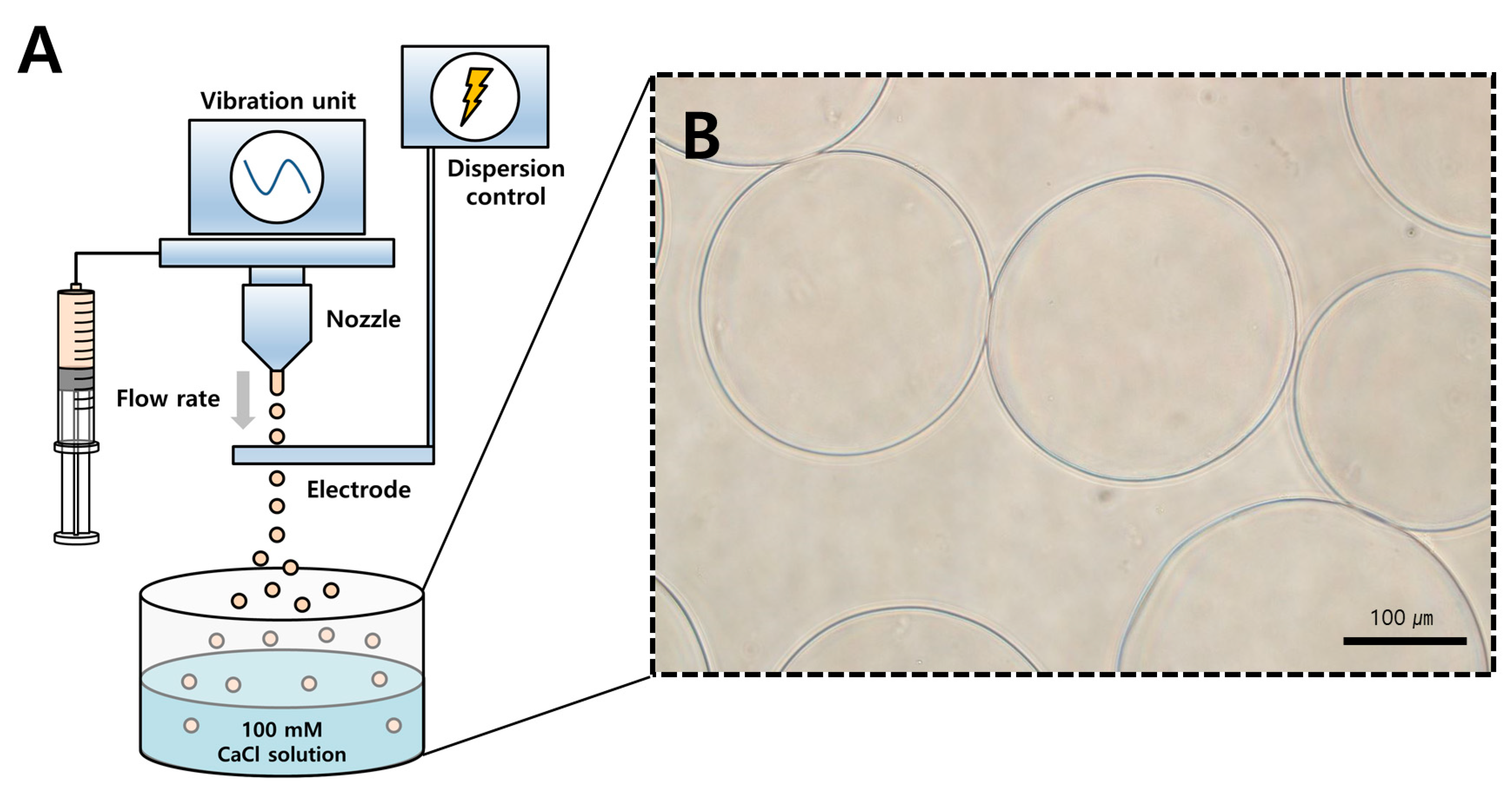
2.1. Preparation of Alginate Microbeads Loaded with BMP-2
2.2. Morphology and Encapsulation Efficiency
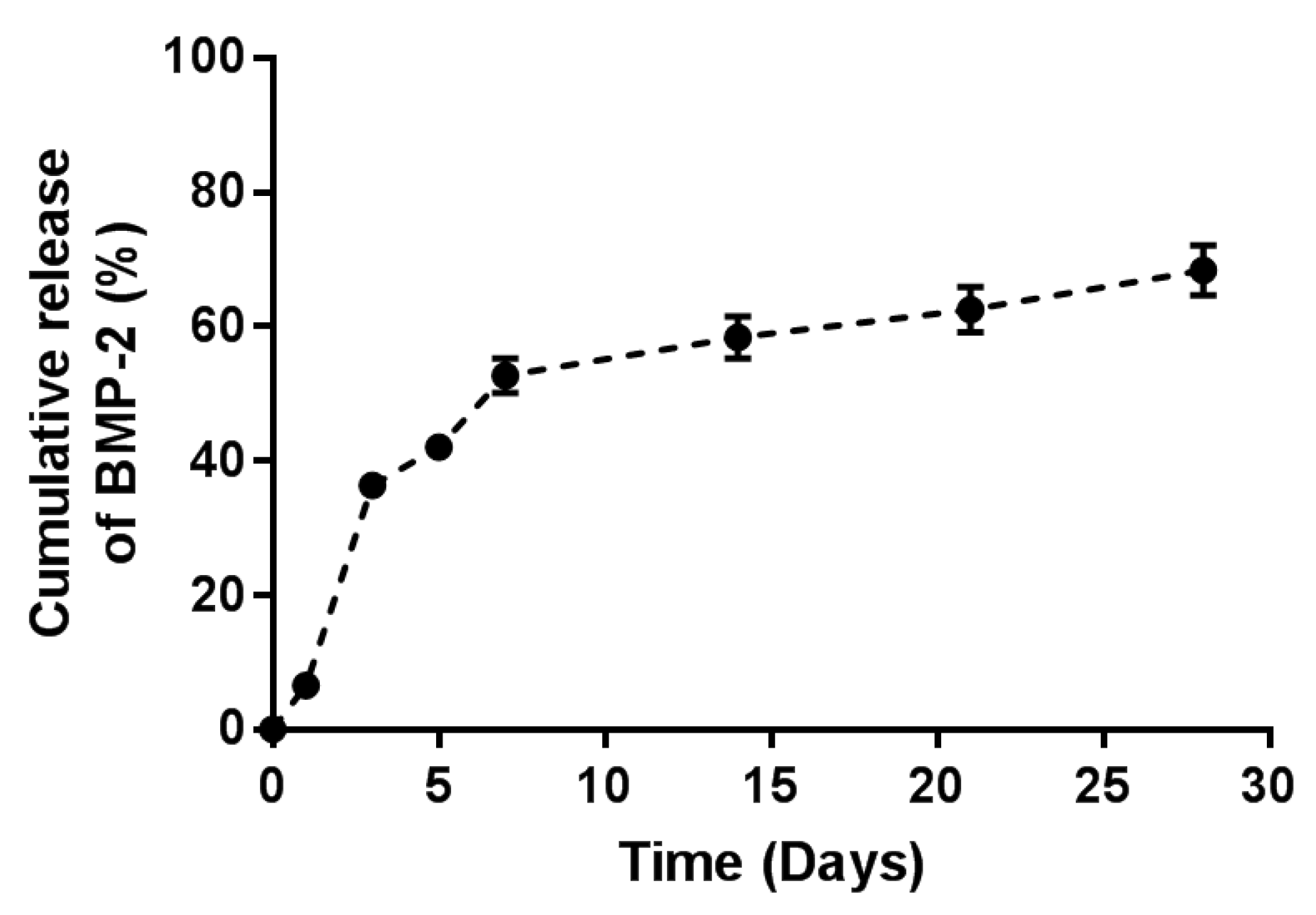
2.3. In Vitro BMP-2 Release Kinetics from Alginate Microbeads
2.4. Experimental Animals
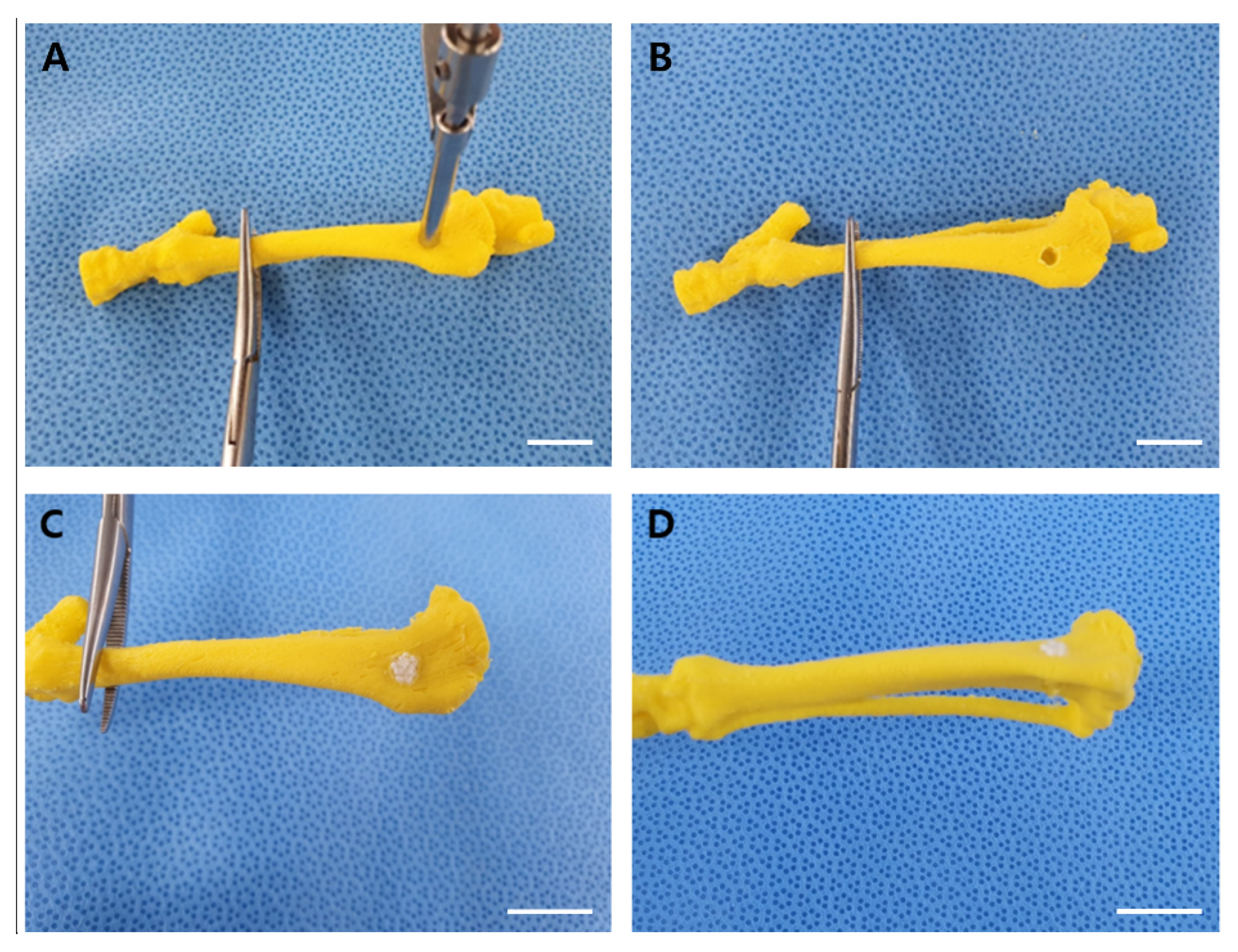
2.5. Rabbit Tibial Metaphyseal Defect Model for Bone Regeneration
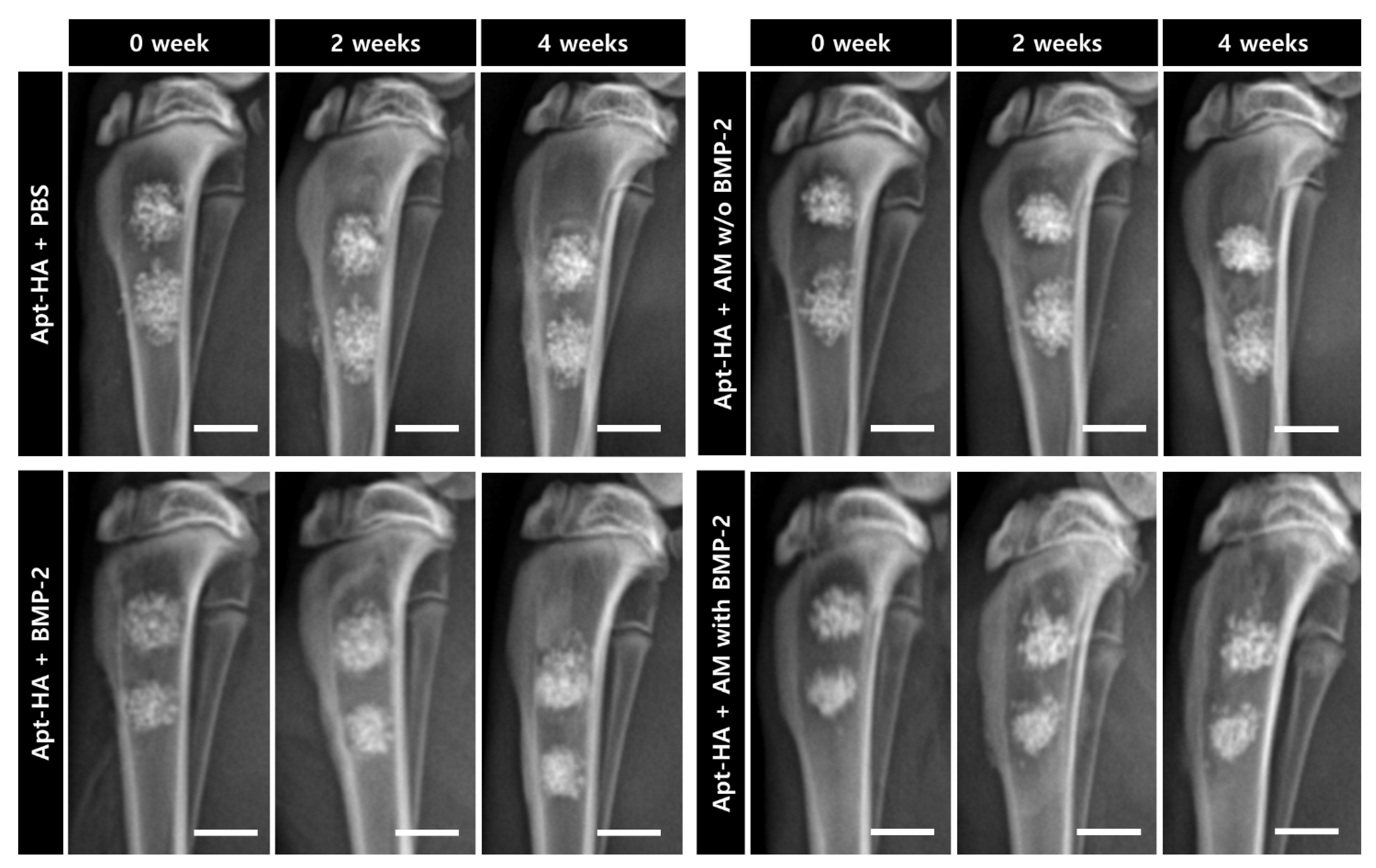
2.6. Radiographic Assessment
2.7. Micro-Computed Tomography Analysis
2.8. Histological and Histomorphometric Analyses
2.9. Statistical Analysis
3. Results
3.1. Morphology and EE
3.2. Controlled Release of BMP-2
3.3. Radiographic Finding and Evaluation
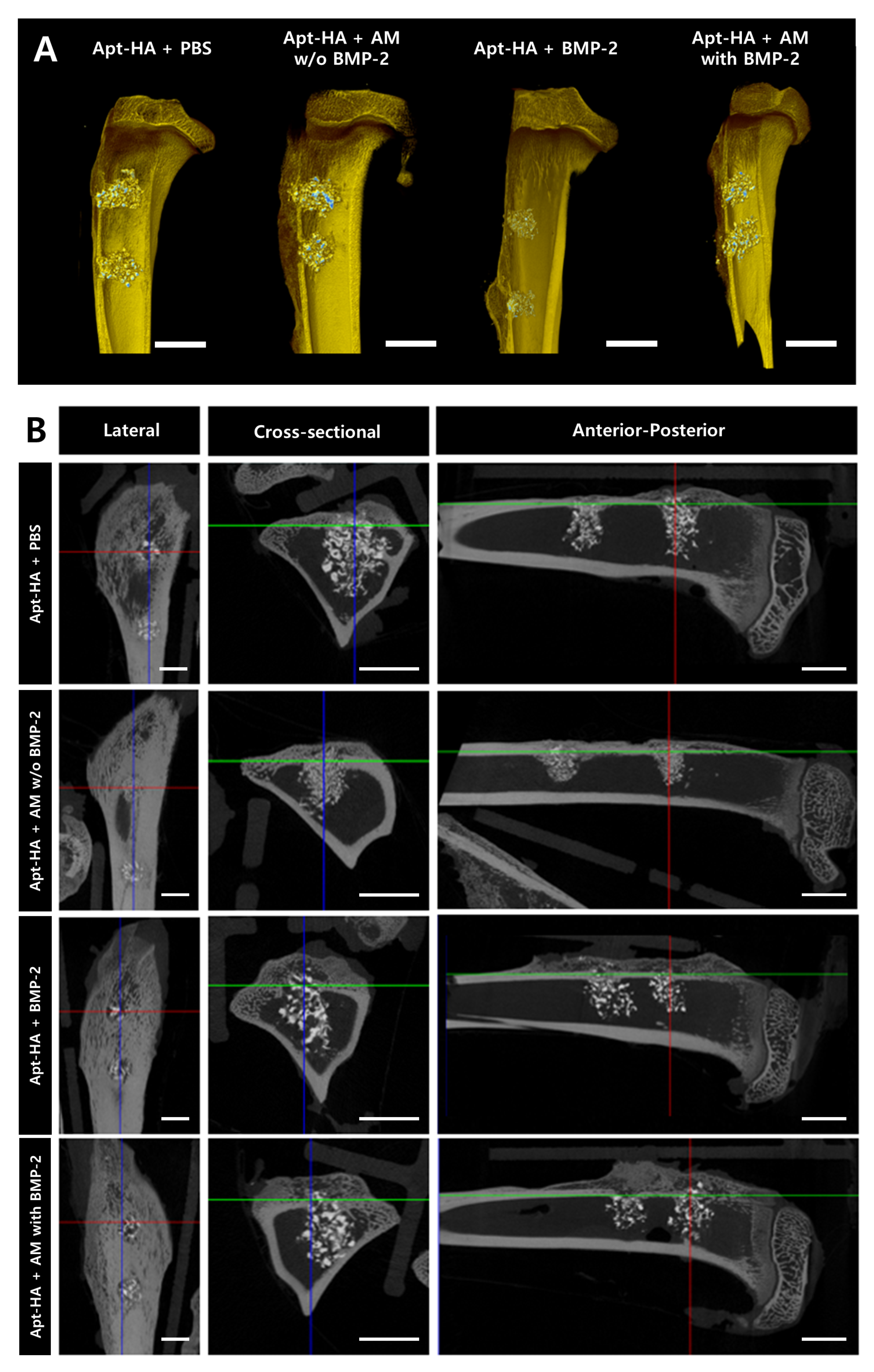
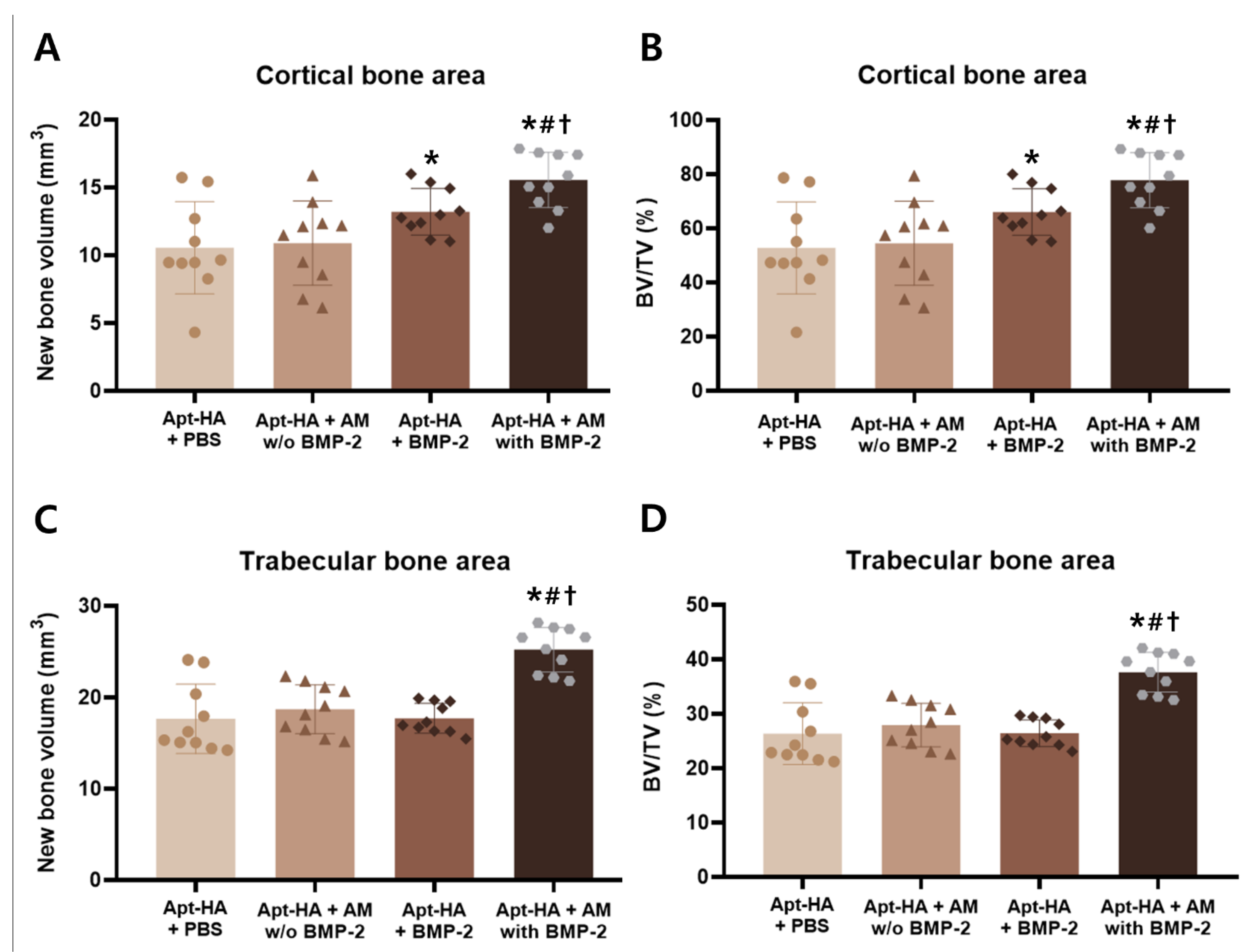
3.4. Micro-CT Analysis
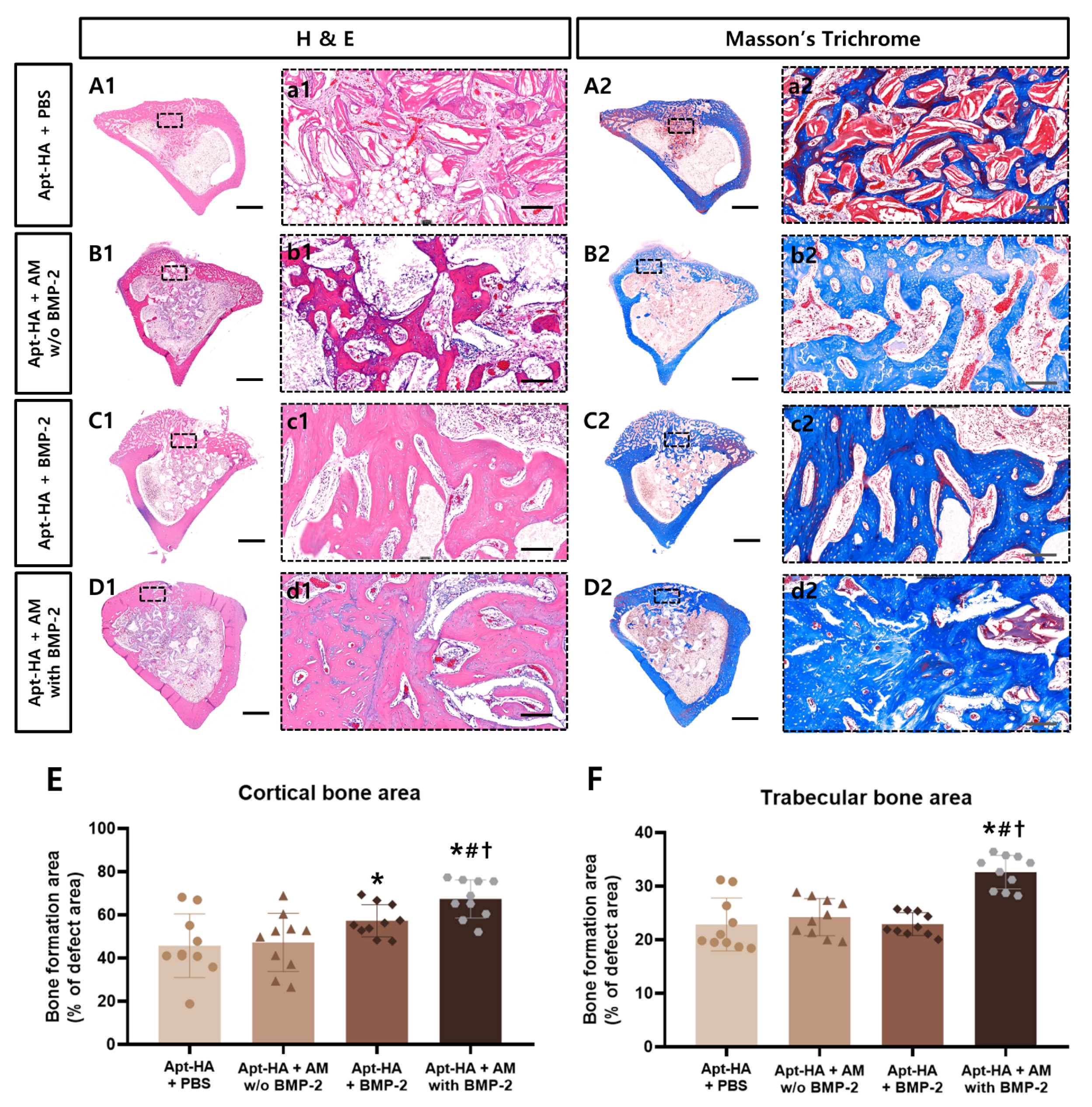
3.5. Histological and Histomorphometric Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Martino, M.M.; Briquez, P.S.; Maruyama, K.; Hubbell, J.A. Extracellular matrix-inspired growth factor delivery systems for bone regeneration. Adv. Drug Deliv. Rev. 2015, 94, 41–52. [Google Scholar] [CrossRef] [PubMed]
- Mauffrey, C.; Barlow, B.T.; Smith, W. Management of segmental bone defects. JAAOS-J. Am. Acad. Orthop. Surg. 2015, 23, 143–153. [Google Scholar]
- Shin, S.R.; Tornetta, P., III. Donor site morbidity after anterior iliac bone graft harvesting. J. Orthop. Trauma 2016, 30, 340–343. [Google Scholar]
- Suda, A.J.; Schamberger, C.T.; Viergutz, T. Donor site complications following anterior iliac crest bone graft for treatment of distal radius fractures. Arch. Orthop. Trauma Surg. 2018, 139, 423–428. [Google Scholar] [CrossRef]
- Tuchman, A.; Brodke, D.S.; Youssef, J.A.; Meisel, H.-J.; Dettori, J.R.; Park, J.-B.; Yoon, S.T.; Wang, J.C. Iliac Crest Bone Graft versus Local Autograft or Allograft for Lumbar Spinal Fusion: A Systematic Review. Glob. Spine J. 2016, 6, 592–606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dang, M.; Saunders, L.; Niu, X.; Fan, Y.; Ma, P.X. Biomimetic delivery of signals for bone tissue engineering. Bone Res. 2018, 6, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Raina, D.B.; Isaksson, H.; Hettwer, W.; Kumar, A.; Lidgren, L.; Tägil, M. A Biphasic Calcium Sulphate/Hydroxyapatite Carrier Containing Bone Morphogenic Protein-2 and Zoledronic Acid Generates Bone. Sci. Rep. 2016, 6, 26033. [Google Scholar] [CrossRef] [Green Version]
- Son, J.; Kim, J.; Lee, K.; Hwang, J.; Choi, Y.; Seo, Y.; Jeon, H.; Kang, H.C.; Woo, H.-M.; Kang, B.-J.; et al. DNA aptamer immobilized hydroxyapatite for enhancing angiogenesis and bone regeneration. Acta Biomater. 2019, 99, 469–478. [Google Scholar] [CrossRef]
- Poynton, A.R.; Lane, J.M. Safety Profile for the Clinical Use of Bone Morphogenetic Proteins in the Spine. Spine 2002, 27, S40–S48. [Google Scholar] [CrossRef]
- Lee, K.-B.; Taghavi, C.E.; Song, K.-J.; Sintuu, C.; Yoo, J.H.; Keorochana, G.; Tzeng, S.-T.; Fei, Z.; Liao, J.-C.; Wang, J.C. Inflammatory Characteristics of rhBMP-2 In Vitro and in an In Vivo Rodent Model. Spine 2011, 36, E149–E154. [Google Scholar] [CrossRef]
- Zara, J.N.; Siu, R.K.; Zhang, X.; Shen, J.; Ngo, R.; Lee, M.; Li, W.; Chiang, M.; Chung, J.; Kwak, J.; et al. High Doses of Bone Morphogenetic Protein 2 Induce Structurally Abnormal Bone and Inflammation In Vivo. Tissue Eng. Part A 2011, 17, 1389–1399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agrawal, V.; Sinha, M. A review on carrier systems for bone morphogenetic protein-2. J. Biomed. Mater. Res. Part B Appl. Biomater. 2017, 105, 904–925. [Google Scholar] [CrossRef] [PubMed]
- Gombotz, W.R.; Wee, S.F. Protein release from alginate matrices. Adv. Drug Deliv. Rev. 2012, 64, 194–205. [Google Scholar] [CrossRef]
- Gu, F.; Amsden, B.; Neufeld, R. Sustained delivery of vascular endothelial growth factor with alginate beads. J. Control. Release 2004, 96, 463–472. [Google Scholar] [CrossRef]
- Lee, Y.H.; Lee, B.-W.; Jung, Y.C.; Yoon, B.-I.; Woo, H.-M.; Kang, B.-J. Application of alginate microbeads as a carrier of bone morphogenetic protein-2 for bone regeneration. J. Biomed. Mater. Res. Part B Appl. Biomater. 2019, 107, 286–294. [Google Scholar] [CrossRef]
- Koh, E.; Jung, Y.C.; Woo, H.-M.; Kang, B.-J. Injectable alginate-microencapsulated canine adipose tissue-derived mesenchymal stem cells for enhanced viable cell retention. J. Veter. Med. Sci. 2017, 79, 492–501. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.; Yang, H.J.; Cho, T.H.; Lee, S.E.; Park, Y.D.; Kim, H.M.; Kim, I.S.; Seo, Y.-K.; Hwang, S.J.; Kim, S.J. Enhanced regeneration of rabbit mandibular defects through a combined treatment of electrical stimulation and rhBMP-2 application. Med. Biol. Eng. Comput. 2013, 51, 1339–1348. [Google Scholar] [CrossRef]
- Jeon, O.; Song, S.J.; Kang, S.-W.; Putnam, A.J.; Kim, B.-S. Enhancement of ectopic bone formation by bone morphogenetic protein-2 released from a heparin-conjugated poly(l-lactic-co-glycolic acid) scaffold. Biomaterials 2007, 28, 2763–2771. [Google Scholar] [CrossRef]
- Zhao, B.; Katagiri, T.; Toyoda, H.; Takada, T.; Yanai, T.; Fukuda, T.; Chung, U.-I.; Koike, T.; Takaoka, K.; Kamijo, R. Heparin Potentiates the in Vivo Ectopic Bone Formation Induced by Bone Morphogenetic Protein-2. J. Biol. Chem. 2006, 281, 23246–23253. [Google Scholar] [CrossRef] [Green Version]
- Krishnan, L.; Priddy, L.B.; Esancy, C.; Klosterhoff, B.S.; Stevens, H.Y.; Tran, L.; Guldberg, R.E. Delivery vehicle effects on bone regeneration and heterotopic ossification induced by high dose BMP-2. Acta Biomater. 2017, 49, 101–112. [Google Scholar] [CrossRef] [Green Version]
- Makvandi, P.; Ghomi, M.; Padil, V.V.T.; Shalchy, F.; Ashrafizadeh, M.; Askarinejad, S.; Pourreza, N.; Zarrabi, A.; Zare, E.N.; Kooti, M.; et al. Biofabricated Nanostructures and Their Composites in Regenerative Medicine. ACS Appl. Nano Mater. 2020, 3, 6210–6238. [Google Scholar] [CrossRef]
- Li, B.; Yoshii, T.; Hafeman, A.E.; Nyman, J.S.; Wenke, J.C.; Guelcherab, S.A. The effects of rhBMP-2 released from biodegradable polyurethane/microsphere composite scaffolds on new bone formation in rat femora. Biomaterials 2009, 30, 6768–6779. [Google Scholar] [CrossRef] [PubMed]
- Harper, B.A.; Barbut, S.; Lim, L.-T.; Marcone, M.F. Effect of Various Gelling Cations on the Physical Properties of “Wet” Alginate Films. J. Food Sci. 2014, 79, E562–E567. [Google Scholar] [CrossRef]
- Almeida, P.F.; Almeida, A. Cross-linked alginate–gelatine beads: A new matrix for controlled release of pindolol. J. Control. Release 2004, 97, 431–439. [Google Scholar] [CrossRef] [PubMed]
- Balmayor, E.R.; Feichtinger, G.A.; Azevedo, H.S.; Van Griensven, M.; Reis, R.L. Starch-poly-є-caprolactone Microparticles Reduce the Needed Amount of BMP-2. Clin. Orthop. Relat. Res. 2009, 467, 3138–3148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, D.; Wufuer, M.; Kim, I.; Choi, T.H.; Kim, B.J.; Jung, H.G.; Jeon, B.; Lee, G.; Jeon, O.H.; Chang, H.; et al. Sequential dual-drug delivery of BMP-2 and alendronate from hydroxyapatite-collagen scaffolds for enhanced bone regeneration. Sci. Rep. 2021, 11. [Google Scholar] [CrossRef]
- Kempen, D.H.R.; Yaszemski, M.J.; Heijink, A.; Hefferan, T.E.; Creemers, L.; Britson, J.; Maran, A.; Classic, K.L.; Dhert, W.J.A.; Lu, L. Non-invasive monitoring of BMP-2 retention and bone formation in composites for bone tissue engineering using SPECT/CT and scintillation probes. J. Control. Release 2009, 134, 169–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, N.; Lalwani, D.; Gollmer, S.; Injeti, E.; Sari, Y.; Nesamony, J. Development and evaluation of a calcium alginate based oral ceftriaxone sodium formulation. Prog. Biomater. 2016, 5, 117–133. [Google Scholar] [CrossRef] [Green Version]
- Yeo, Y.; Park, K. Control of encapsulation efficiency and initial burst in polymeric microparticle systems. Arch. Pharmacal Res. 2004, 27, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Stubbs, D.; Deakin, M.; Chapman-Sheath, P.; Bruce, W.; Debes, J.; Gillies, R.; Walsh, W. In vivo evaluation of resorbable bone graft substitutes in a rabbit tibial defect model. Biomaterials 2004, 25, 5037–5044. [Google Scholar] [CrossRef] [PubMed]
- Milgrom, C.; Gildadi, M.; Simkin, A.; Rand, N.; Kedem, R.; Kashtan, H.; Stein, M.; Gomori, M. The area moment of inertia of the tibia: A risk factor for stress fractures. J. Biomech. 1989, 22, 1243–1248. [Google Scholar] [CrossRef]
- Maquer, G.B.; Musy, S.N.; Wandel, J.; Gross, T.; Zysset, P.K. Bone volume fraction and fabric anisotropy are better determinants of trabecular bone stiffness than other mor-phological variables. J. Bone Miner. Res. 2015, 30, 1000–1008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kempen, D.H.; Lu, L.; Heijink, A.; Hefferan, T.E.; Creemers, L.B.; Maran, A.; Yaszemski, M.J.; Dhert, W.J. Effect of local sequential VEGF and BMP-2 delivery on ectopic and orthotopic bone regeneration. Biomaterials 2009, 30, 2816–2825. [Google Scholar] [CrossRef]
- Zhang, W.; Wang, X.; Wang, S.; Zhao, J.; Xu, L.; Zhu, C.; Zeng, D.; Chen, J.; Zhang, Z.; Kaplan, D.L.; et al. The use of injectable sonication-induced silk hydrogel for VEGF165 and BMP-2 delivery for elevation of the maxil-lary sinus floor. Biomaterials 2011, 32, 9415–9424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, S.; Chen, J.; Yu, Y.; Dai, K.; Wang, J.; Liu, C. Accelerated Bone Regenerative Efficiency by Regulating Sequential Release of BMP-2 and VEGF and Synergism with Sulfated Chitosan. ACS Biomater. Sci. Eng. 2019, 5, 1944–1955. [Google Scholar] [CrossRef] [PubMed]
- Peng, H.; Usas, A.; Olshanski, A.; Ho, A.M.; Gearhart, B.; Cooper, G.M.; Huard, J. VEGF Improves, Whereas sFlt1 Inhibits, BMP2-Induced Bone Formation and Bone Healing Through Modulation of Angiogenesis. J. Bone Miner. Res. 2005, 20, 2017–2027. [Google Scholar] [CrossRef]
- Liu, T.; Gao, Y.; Sakamoto, K.; Minamizato, T.; Furukawa, K.; Tsukazaki, T.; Shibata, Y.; Bessho, K.; Komori, T.; Yamaguchi, A. BMP-2 promotes differentiation of osteoblasts and chondroblasts inRunx2-deficient cell lines. J. Cell. Physiol. 2007, 211, 728–735. [Google Scholar] [CrossRef] [PubMed]
- Caetano-Lopes, J.; Canhao, H.; Fonseca, J.E. Osteoblasts and bone formation. Acta Reum. Port. 2007, 32, 2. [Google Scholar]
- Hankenson, K.D.; Dishowitz, M.; Gray, C.; Schenker, M. Angiogenesis in bone regeneration. Injury 2011, 42, 556–561. [Google Scholar] [CrossRef] [Green Version]







Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.; Lee, S.; Choi, Y.; Choi, J.; Kang, B.-J. Sustained Release of Bone Morphogenetic Protein-2 through Alginate Microbeads Enhances Bone Regeneration in Rabbit Tibial Metaphyseal Defect Model. Materials 2021, 14, 2600. https://0-doi-org.brum.beds.ac.uk/10.3390/ma14102600
Kim J, Lee S, Choi Y, Choi J, Kang B-J. Sustained Release of Bone Morphogenetic Protein-2 through Alginate Microbeads Enhances Bone Regeneration in Rabbit Tibial Metaphyseal Defect Model. Materials. 2021; 14(10):2600. https://0-doi-org.brum.beds.ac.uk/10.3390/ma14102600
Chicago/Turabian StyleKim, Junhyung, Seoyun Lee, Yonghyun Choi, Jonghoon Choi, and Byung-Jae Kang. 2021. "Sustained Release of Bone Morphogenetic Protein-2 through Alginate Microbeads Enhances Bone Regeneration in Rabbit Tibial Metaphyseal Defect Model" Materials 14, no. 10: 2600. https://0-doi-org.brum.beds.ac.uk/10.3390/ma14102600