
Resistance to Fracture of Lithium Disilicate Feldspathic Restorations Manufactured Using a CAD/CAM System and Crystallized with Different Thermal Units and Programs

 ,
, 
 and
and
Abstract
:1. Introduction
2. Materials and Methods
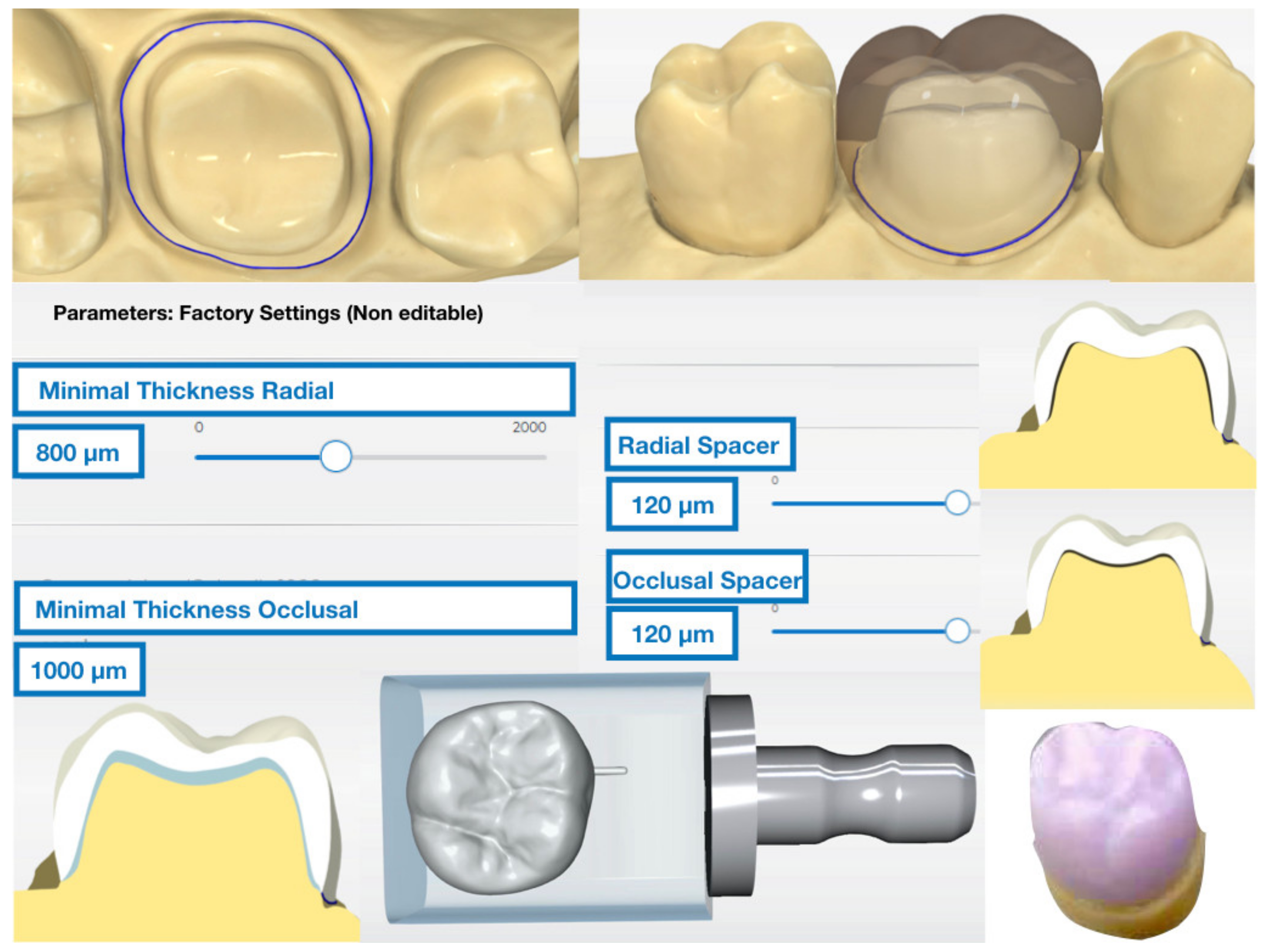
2.1. Crown Design
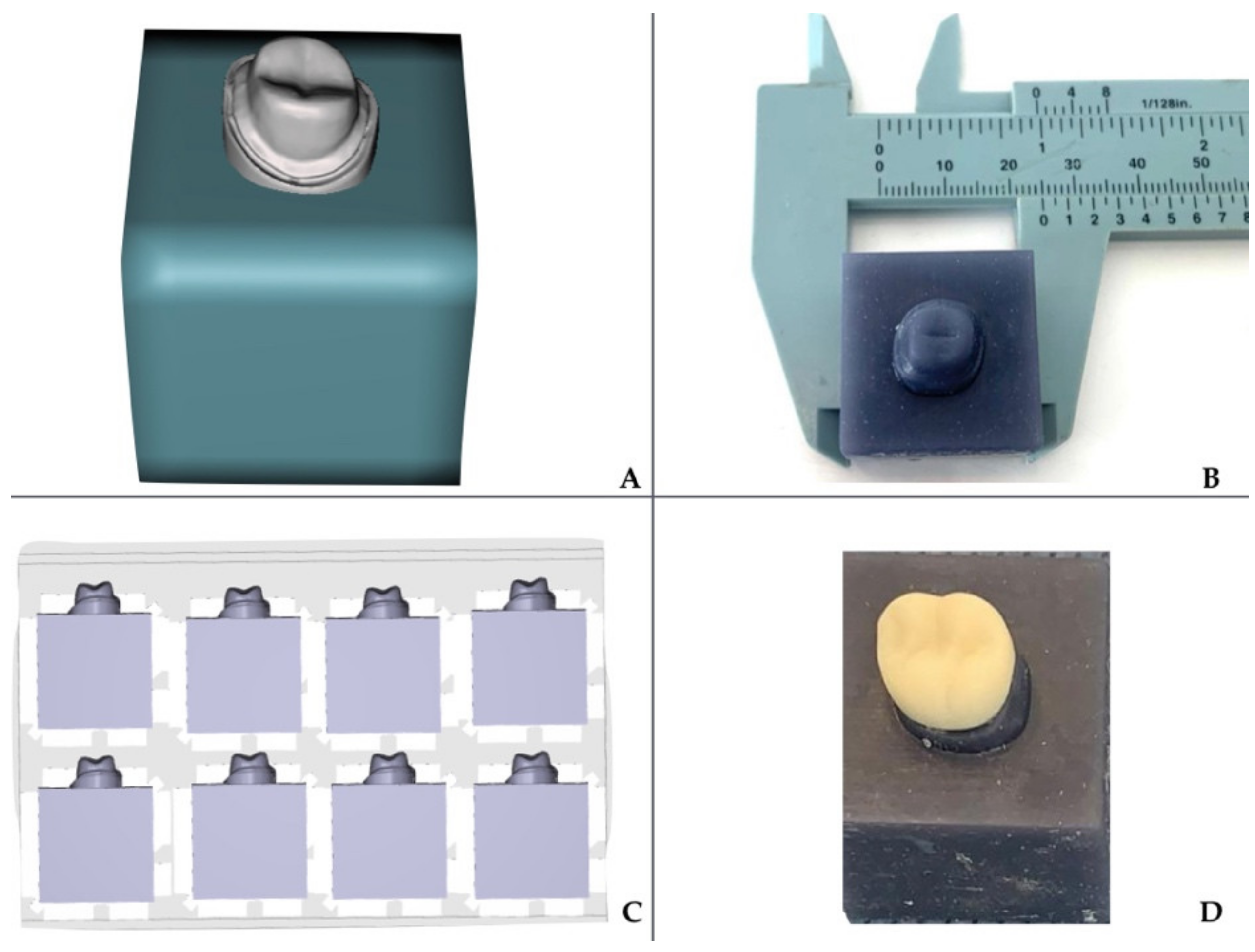
2.2. Fabrication of CAD/CAM Abutments and Restorations
2.3. Thermocycling of the Restorations
2.4. Crystallization Process of the Restorations
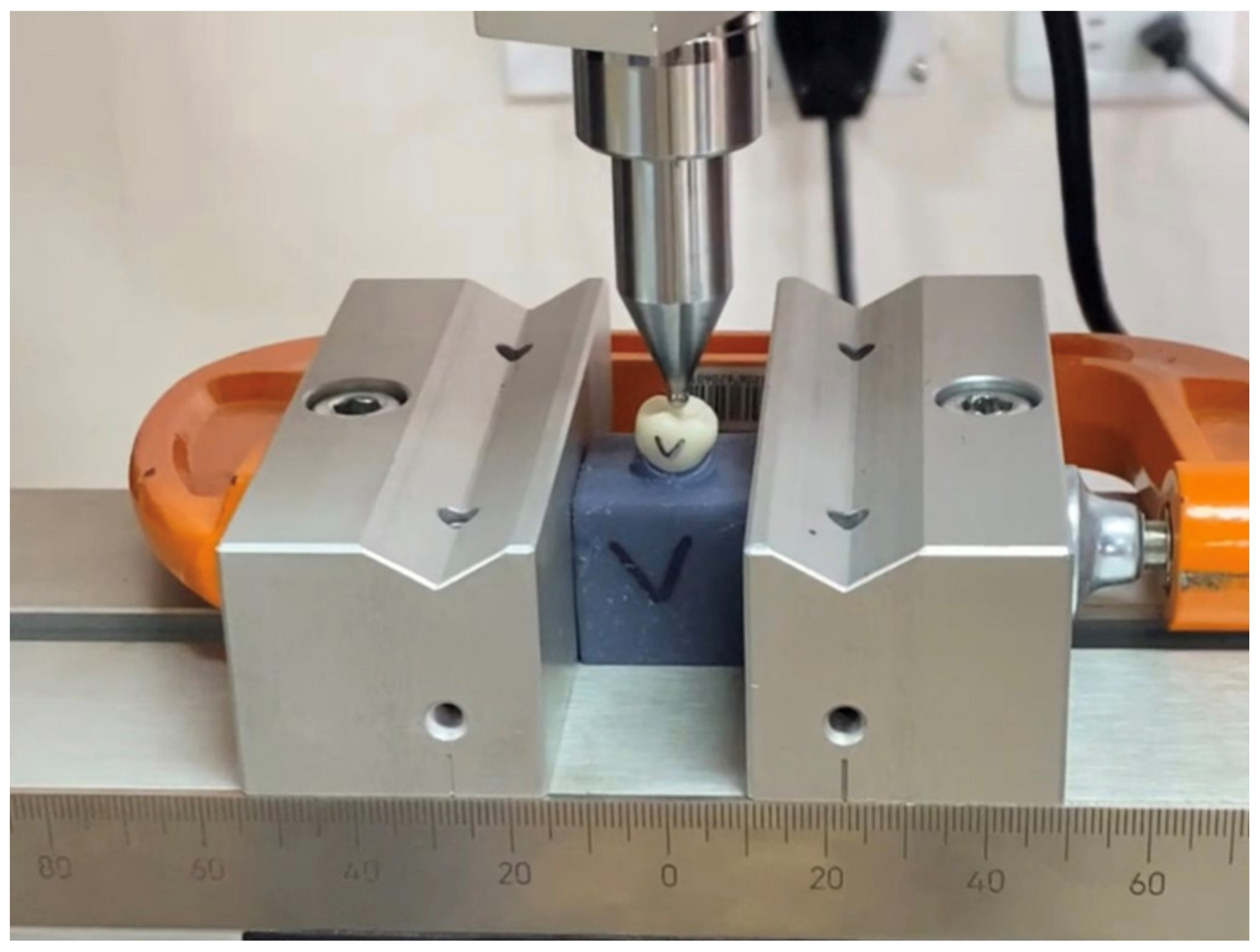
2.5. Fracture Loading of the Restorations
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Moörmann, W.H. The evolution of the CEREC system. J. Am. Dent. Assoc. 2006, 137, 7–13. [Google Scholar]
- Conrad, H.J.; Seong, W.-J.; Pesun, I.J. Current ceramic materials and systems with clinical recommendations: A systematic review. J. Prosthet. Dent. 2007, 98, 389–404. [Google Scholar] [CrossRef]
- Peampring, C.; Sanohkan, S. Effect of Thermocycling on Flexural Strength and Weibull Statistics of Machinable Glass–Ceramic and Composite Resin. J. Indian Prosthodont. Soc. 2013, 14, 376–380. [Google Scholar] [CrossRef]
- Miyazaki, T.; Hotta, Y. CAD/CAM systems available for the fabrication of crown and bridge restorations. Aust. Dent. J. 2011, 56, 97–106. [Google Scholar] [CrossRef]
- Ivoclar-Vivadent AG. IPS Emax CAD, Laboratory Instructions for Use; Ivoclar-Vivadent Technical: Schaan, Liechtenstein, 2009; pp. 1–68. [Google Scholar]
- Ferrari, M.; Mangano, F.G.; Leone, R.; Sorrentino, R. Digitally oriented materials: Focus on lithium disilicate ceramics. Int. J. Dent. 2016, 2016, 1–10. [Google Scholar] [CrossRef]
- Li, R.W.K.; Chow, T.W.; Matinlinna, J.P. Ceramic dental biomaterials and CAD/CAM technology: State of the art. J. Prosthodont. Res. 2014, 58, 208–216. [Google Scholar] [CrossRef] [Green Version]
- Denry, I.; Holloway, J.A. Ceramics for Dental Applications: A Review. Materials 2010, 3, 351–368. [Google Scholar] [CrossRef] [Green Version]
- Ivoclar-Vivadent™ Technical. Programat P310 Instructions for use; Ivoclar-Vivadent AG: Schaan, Liechtenstein, 2019; pp. 1–68. Available online: https://asia.ivoclarvivadent.com/en-as/all-products/programat-p310 (accessed on 28 February 2021).
- Dentsply-Sirona™. Operating Instructions CEREC Speed Fire™.; Sirona Dental Inc.: Bensheim, Germany, 2016; pp. 1–56. Available online: https://www.dentsplysirona.com/en/explore/cerec/cerec-speedfire.html (accessed on 3 March 2021).
- Lohbauer, U.; Bell, R.; Abdalla, A.; Goetz, F.; Hurle, K. Effect of sintering parameters on phase evolution and strength of dental lithium silicate glass-ceramics. Dent. Mater. 2019, 35, 1360–1369. [Google Scholar] [CrossRef]
- Riquieri, H.; Monteiro, J.B.; Viegas, D.C.; Campos, T.M.B.; de Melo, R.M.; Saavedra, G.D.S.F.A. Impact of crystallization firing process on the microstructure and flexural strength of zirconia-reinforced lithium silicate glass-ceramics. Dent. Mater. 2018, 34, 1483–1491. [Google Scholar] [CrossRef] [Green Version]
- Nejatidanesh, F.; Azadbakht, K.; Savabi, O.; Sharifi, M.; Shirani, M. Effect of repeated firing on the translucency of CAD-CAM monolithic glass-ceramics. J. Prosthet. Dent. 2020, 123, 530–e1. [Google Scholar] [CrossRef]
- Gold, S.A.; Ferracane, J.L.; Da Costa, J. Effect of Crystallization Firing on Marginal Gap of CAD/CAM Fabricated Lithium Disilicate Crowns. J. Prosthodont. 2017, 27, 63–66. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.H.; Oh, S.; Uhm, S.H. Effect of the Crystallization Process on the Marginal and Internal Gaps of Lithium Disilicate CAD/CAM Crowns. Biomed. Res. Int. 2016, 2016, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Willard, A.; Chu, G. The science and application of IPS e. Max dental ceramic. Kaohsiung J. Med. Sci. 2018, 34, 238–242. [Google Scholar] [CrossRef] [Green Version]
- Mörmann, W.H.; Brandestini, M.; Lutz, F. The Cerec system: Computer-assisted preparation of direct ceramic inlays in 1 setting. Quintessenz 1987, 38, 457–470. [Google Scholar] [PubMed]
- Mörmann, W.H.; Brandestini, M.; Lutz, F.; Barbakow, F.; Götsch, T. CAD-CAM Ceramic Inlays and Onlays: A Case Report after 3 years in Place. J. Am. Dent. Assoc. 1990, 120, 517–520. [Google Scholar] [CrossRef] [PubMed]
- Lien, W.; Roberts, H.W.; Platt, J.A.; Vandewalle, K.S.; Hill, T.J.; Chu, T.-M.G. Microstructural evolution and physical behavior of a lithium disilicate glass–ceramic. Dent. Mater. 2015, 31, 928–940. [Google Scholar] [CrossRef]
- Yuan, J.C.C.; Barão, V.A.R.; Wee, A.G.; Alfaro, M.F.; Afshari, F.S.; Sukotjo, C. Effect of brushing and thermocycling on the shade and surface roughness of CAD-CAM ceramic restorations. J. Prosthet. Dent. 2017, 119, 1000–1006. [Google Scholar] [CrossRef]
- Alves, M.F.R.P.; Simba, B.G.; Campos, L.Q.B.; Ferreira, I.; Santos, C. Influence of heat-treatment protocols on mechanical behavior of lithium silicate dental ceramics. Int. J. Appl. Ceram. Technol. 2019, 16, 1920–1931. [Google Scholar] [CrossRef]
- Belli, R.; Lohbauer, U.; Goetz-Neunhoeffer, F.; Hurle, K. Crack-healing during two-stage crystallization of biomedical lithium (di)silicate glass-ceramics. Dent. Mater. 2019, 35, 1130–1145. [Google Scholar] [CrossRef]
- Alao, A.-R.; Stoll, R.; Song, X.-F.; Abbott, J.R.; Zhang, Y.; Abduo, J.; Yin, L. Fracture, roughness and phase transformation in CAD/CAM milling and subsequent surface treatments of lithium metasilicate/disilicate glass-ceramics. J. Mech. Behav. Biomed. Mater. 2017, 74, 251–260. [Google Scholar] [CrossRef]
- Giordano, R. Materials for chairside CAD/CAM–produced restorations. J. Am. Dent. Assoc. 2006, 137, 14S–21S. [Google Scholar] [CrossRef] [PubMed]
- Romanyk, D.L.; Guo, Y.; Rae, N.; Veldhuis, S.; Sirovica, S.; Fleming, G.J.; Addison, O. Strength-limiting damage and its mitigation in CAD-CAM zirconia-reinforced lithium-silicate ceramics machined in a fully crystallized state. Dent. Mater. 2020, 36, 1557–1565. [Google Scholar] [CrossRef]
- Wiedenmann, F.; Böhm, D.; Eichberger, M.; Edelhoff, D.; Stawarczyk, B. Influence of different surface treatments on two-body wear and fracture load of monolithic CAD/CAM ceramics. Clin. Oral Investig. 2020, 24, 3049–3060. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Lee, S.-J.; Park, J.S.; Ryu, J.J. Fracture Load of Monolithic CAD/CAM Lithium Disilicate Ceramic Crowns and Veneered Zirconia Crowns as a Posterior Implant Restoration. Implant. Dent. 2013, 22, 66–70. [Google Scholar] [CrossRef] [PubMed]
- Furtado de Mendonca, A.; Shahmoradi, M.; Gouvêa, C.V.D.; De Souza, G.M.; Ellakwa, A. Microstructural and Mechanical Characterization of CAD/CAM Materials for Monolithic Dental Restorations. J. Prosthodont. 2019, 28, 587–594. [Google Scholar] [CrossRef]
- Aziz, A.; El-Mowafy, O.; Tenenbaum, H.C.; Lawrence, H.P.; Shokati, B. Clinical performance of chairside monolithic lithium disilicate glass-ceramic CAD-CAM crowns. J. Esthet. Restor. Dent. 2019, 31, 613–619. [Google Scholar] [CrossRef] [PubMed]
- Badawy, R.; El-Mowafy, O.; Tam, L.E. Fracture toughness of chairside CAD/CAM materials–Alternative loading approach for compact tension test. Dent. Mater. 2016, 32, 847–852. [Google Scholar] [CrossRef]
- Sieper, K.; Wille, S.; Kern, M. Fracture strength of lithium disilicate crowns compared to polymer-infiltrated ceramic-network and zirconia reinforced lithium silicate crowns. J. Mech. Behav. Biomed. Mater. 2017, 74, 342–348. [Google Scholar] [CrossRef]
- Altier, M.; Erol, F.; Yildirim, G.; Dalkilic, E.E. Fracture resistance and failure modes of lithium disilicate or composite endocrowns. Niger. J. Clin. Pract. 2018, 21, 821–826. [Google Scholar]
- Dmd, S.E.C.; Dds, A.C.P.; Wang, J.; Knoernschild, K.L.; Campbell, S.; Yang, B. Fracture Resistance of Various Thickness e.max CAD Lithium Disilicate Crowns Cemented on Different Supporting Substrates: An In Vitro Study. J. Prosthodont. 2019, 28, 997–1004. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Furnace | Manufacturer | Crystallization Programs |
|---|---|---|
| Programat P310 | Ivoclar-Vivadent™/Liechtenstein | Group A, Normal Firing (NF) final temperature 850 °C/approximately 23 min 50 s Group B, Fast Firing (FF) final temperature of 870 °C/15 min 10 s |
| Speed Fire | Dentsply-Sirona™/Bensheim, Germany | Group C, SpeedFire (SF) final temperature 797 °C/approximately 24 min |
| Groups | Sum Square | Gl | Mean Square | F | Sig. |
|---|---|---|---|---|---|
| Inter-groups | 101077.700 | 2 | 50538.85 | 8.699 | 0.001 |
| Intra-groups | 331141.965 | 57 | 5809.50 | - | - |
| Total | 432219.665 | 59 | - | - | - |
| Furnace Type | Group | Mean Difference (I–J) | Sig. | C. I. 95% | |
|---|---|---|---|---|---|
| Lower Limit | Upper Limit | ||||
| Normal Firing | Fast Firing | 32.80 | 0.537 | −26.64 | 92.25 |
| Speed Fire | 98.70 * | 0.000 | 39.25 | 158.15 | |
| Fast Firing | Normal Firing | −32.80 | 0.537 | −92.25 | 26.64 |
| Speed Fire | 65.90 * | 0.025 | 6.44 | 125.35 | |
| Speed Fire | Normal Firing | −98.70 * | 0.000 | −158.15 | −39.25 |
| Fast Firing | −65.90 * | 0.025 | −125.35 | −6.44 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abad-Coronel, C.; Ordoñez Balladares, A.; Fajardo, J.I.; Martín Biedma, B.J. Resistance to Fracture of Lithium Disilicate Feldspathic Restorations Manufactured Using a CAD/CAM System and Crystallized with Different Thermal Units and Programs. Materials 2021, 14, 3215. https://0-doi-org.brum.beds.ac.uk/10.3390/ma14123215
Abad-Coronel C, Ordoñez Balladares A, Fajardo JI, Martín Biedma BJ. Resistance to Fracture of Lithium Disilicate Feldspathic Restorations Manufactured Using a CAD/CAM System and Crystallized with Different Thermal Units and Programs. Materials. 2021; 14(12):3215. https://0-doi-org.brum.beds.ac.uk/10.3390/ma14123215
Chicago/Turabian StyleAbad-Coronel, Cristian, Andrea Ordoñez Balladares, Jorge I. Fajardo, and Benjamín José Martín Biedma. 2021. "Resistance to Fracture of Lithium Disilicate Feldspathic Restorations Manufactured Using a CAD/CAM System and Crystallized with Different Thermal Units and Programs" Materials 14, no. 12: 3215. https://0-doi-org.brum.beds.ac.uk/10.3390/ma14123215