
The Analysis of Polyethylene Hip Joint Endoprostheses Strength Parameters Changes after Use inside the Human Body

 ,
,  , , , , , , , , and
, , , , , , , , and
Abstract
:1. Introduction
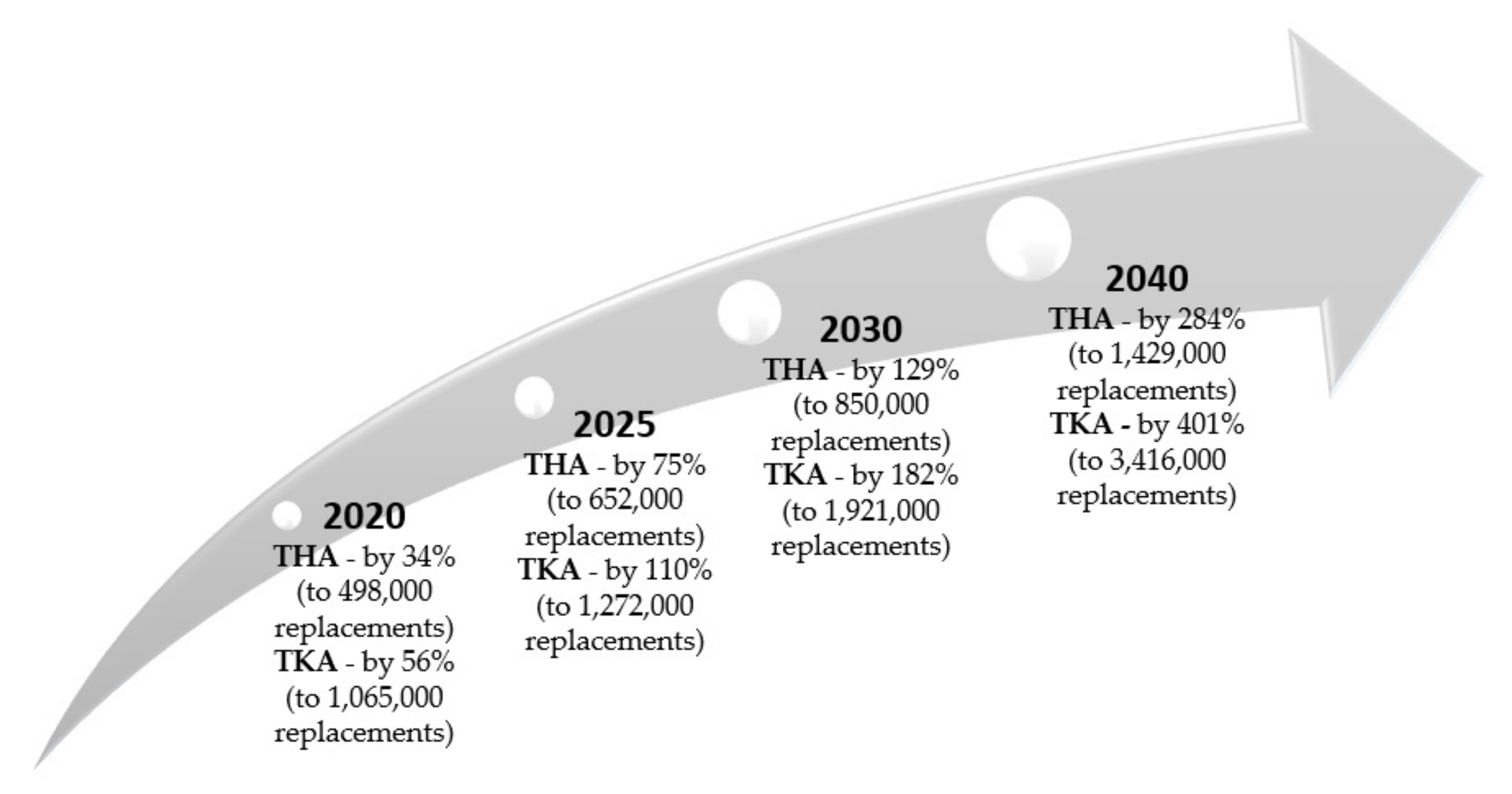
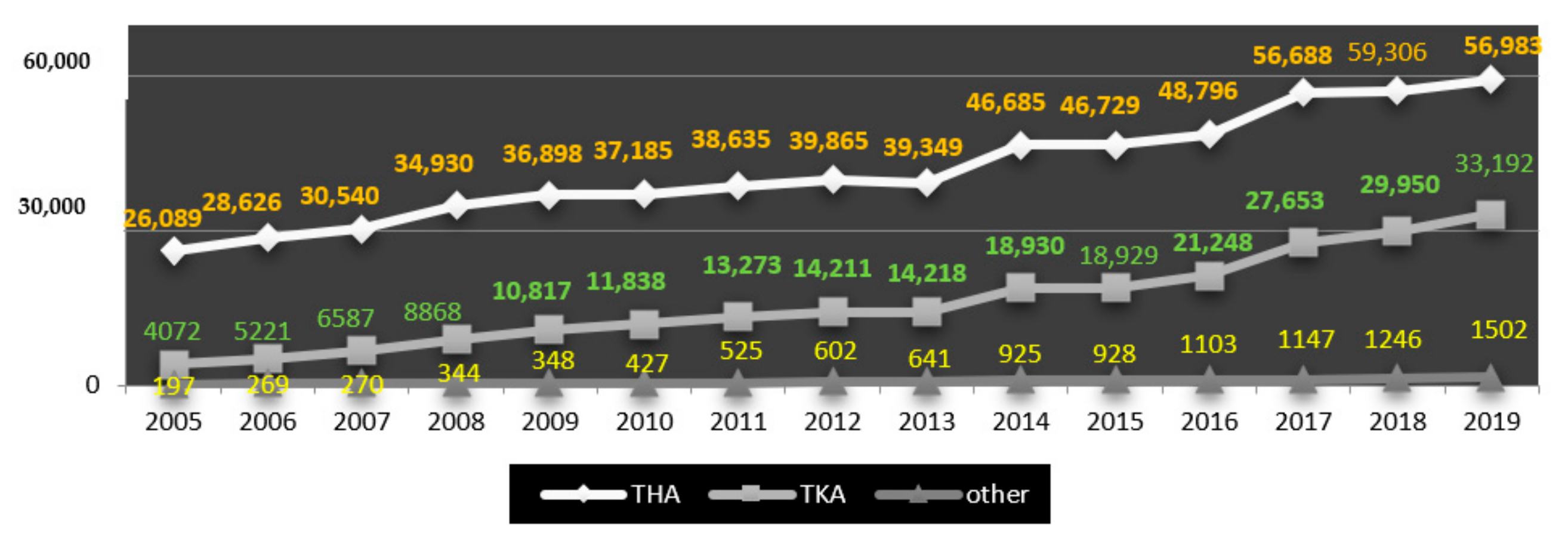
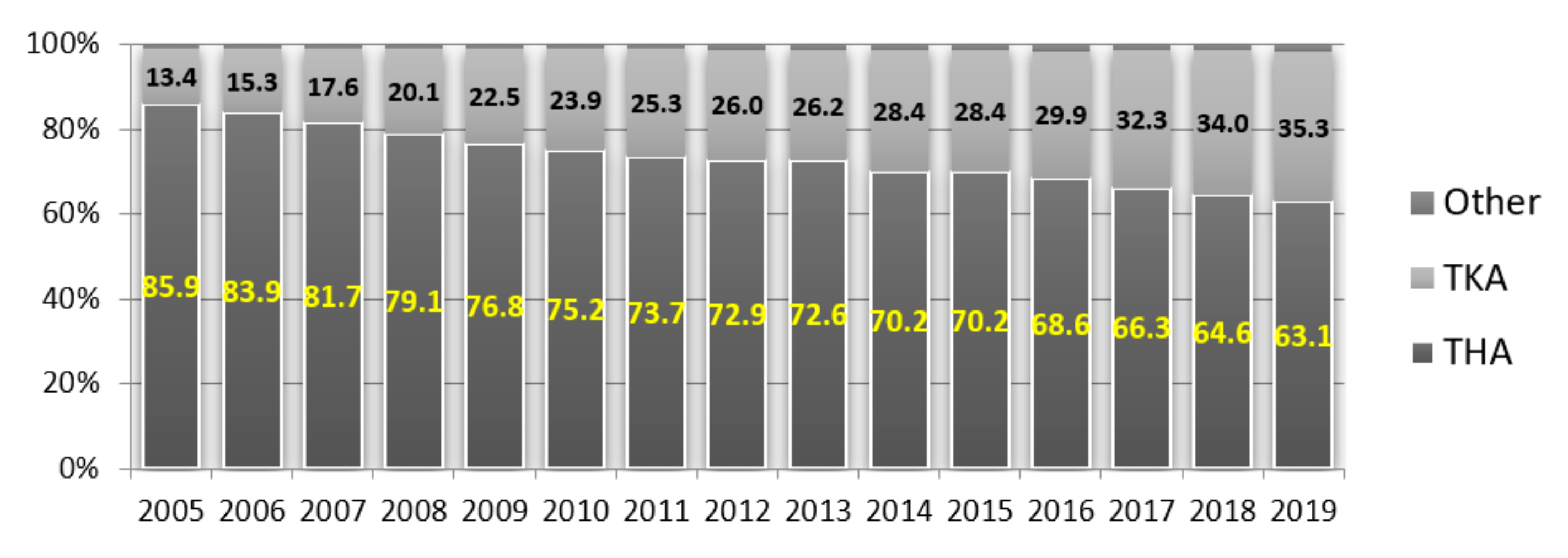
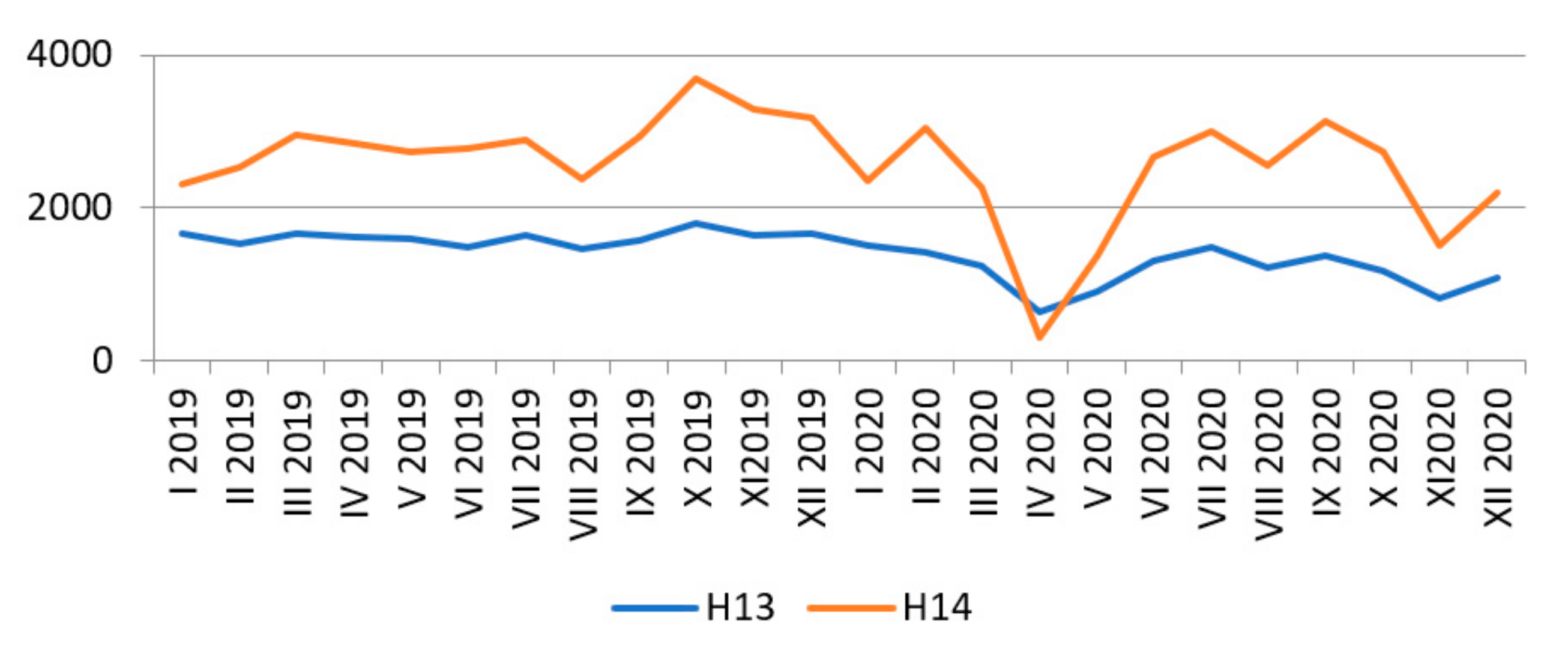
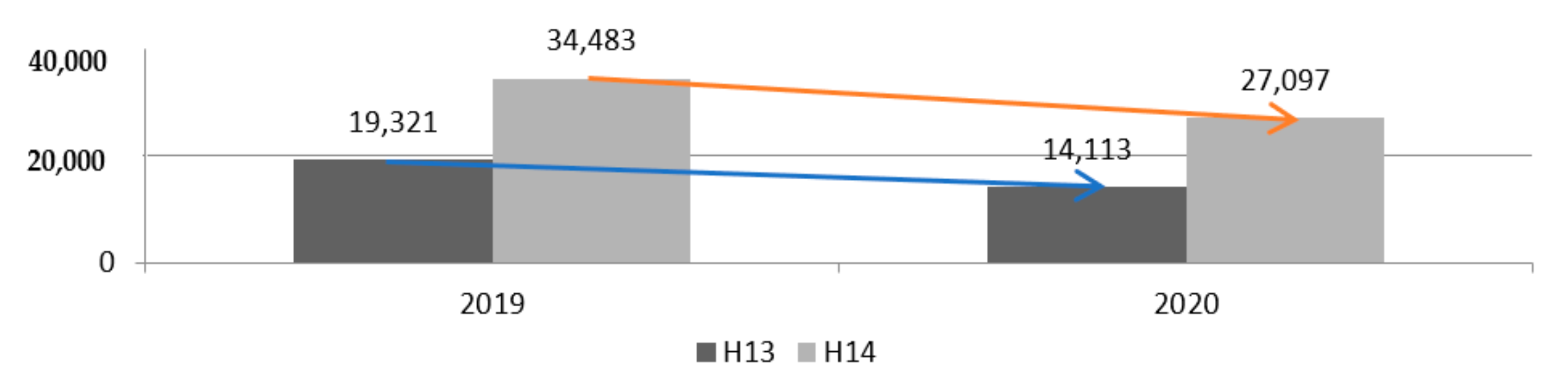
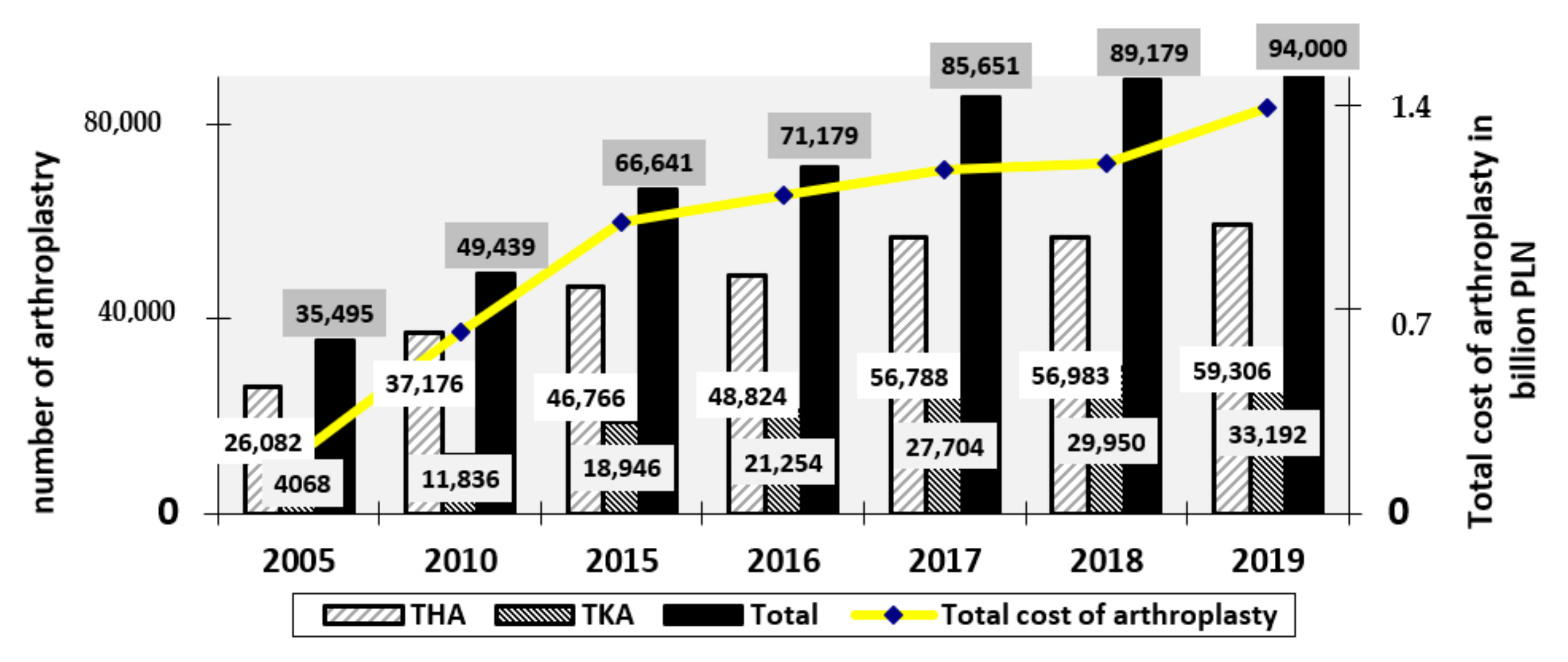
2. Statistical Evaluation of the Number of Surgeries and Costs of Hip-Joint Replacement in Poland
3. Materials and Methods
3.1. Aim and Scope of Research
3.2. Methodology of Experimental Research
- phase transitions of polymers;
- physical changes: glass transition temperature Tg, melting point temperature Tm;
- composition of mixtures and copolymers;
- thermal decomposition of Td (destruction temperature) of polymers, oxidation and combustion;
- heat of: crystallisation, polymerisation, dissolution, absorption and desorption;
- enthalpy of melting and degree of crystallinity.
- —sample mass;
- —specific heat at constant pressure (heat capacity per unit mass);
- —heat supplied or discharged to the system per unit time;
- —heating or cooling speed.
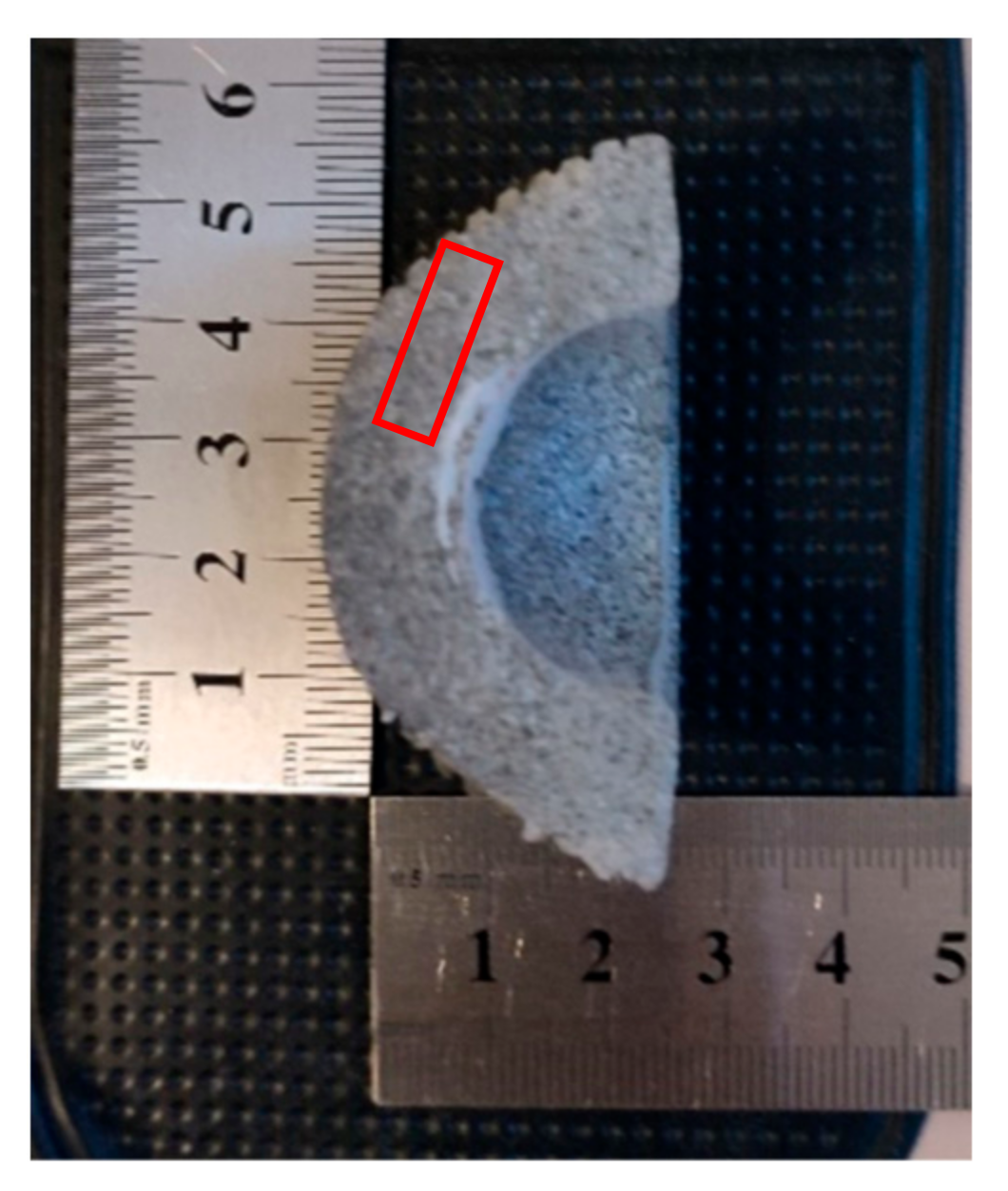
3.3. Materials and Their Preparation
4. Results
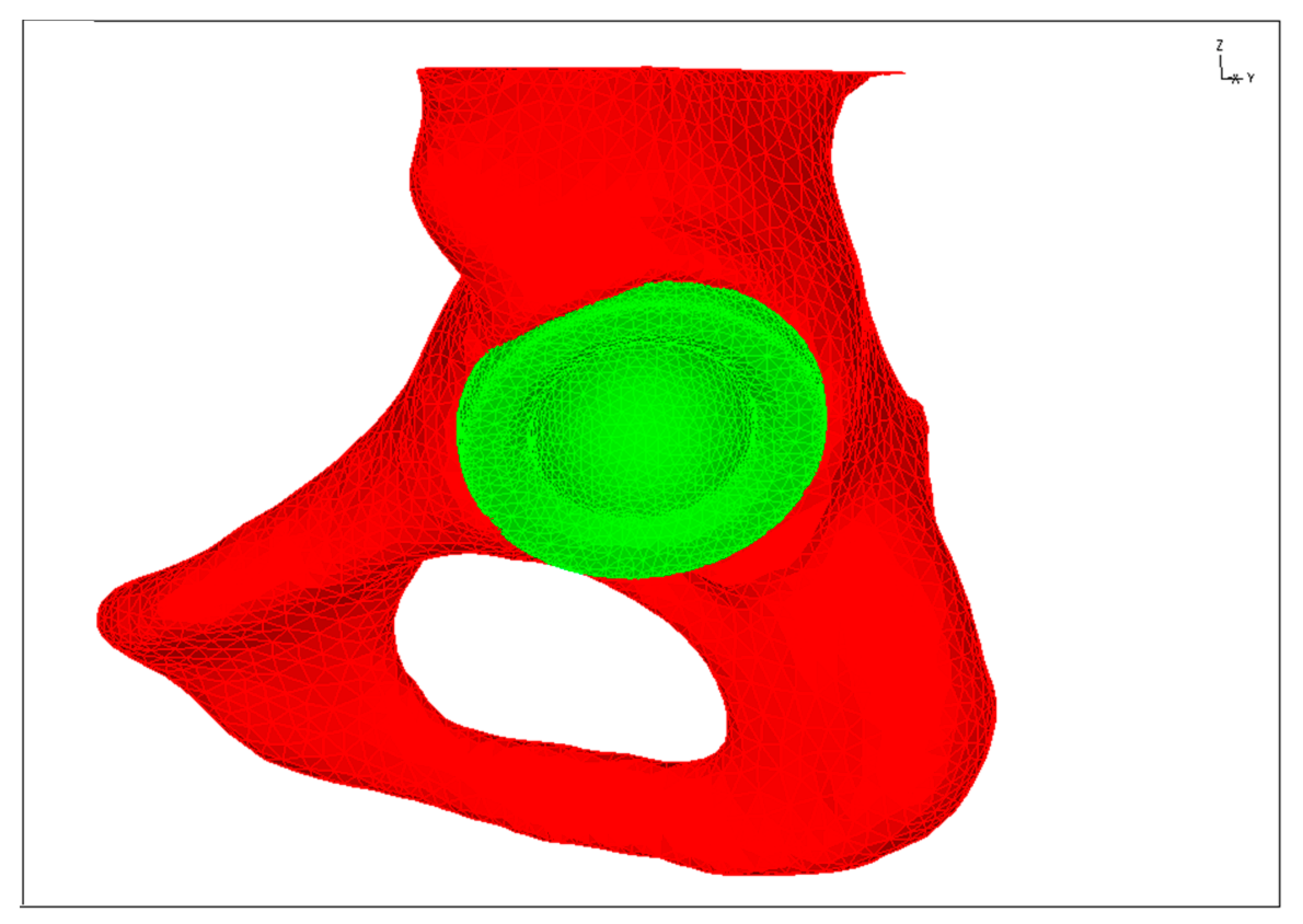
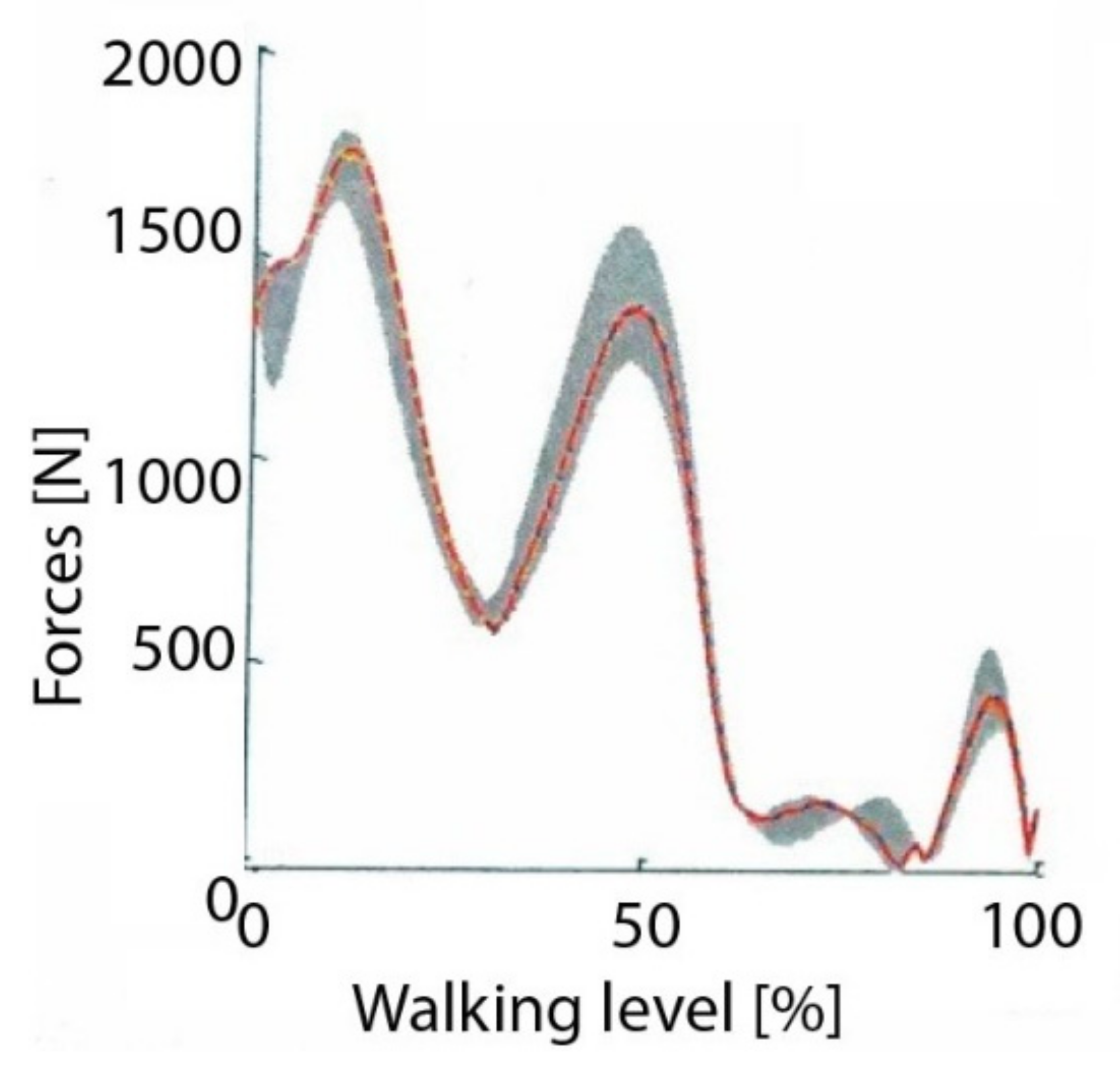
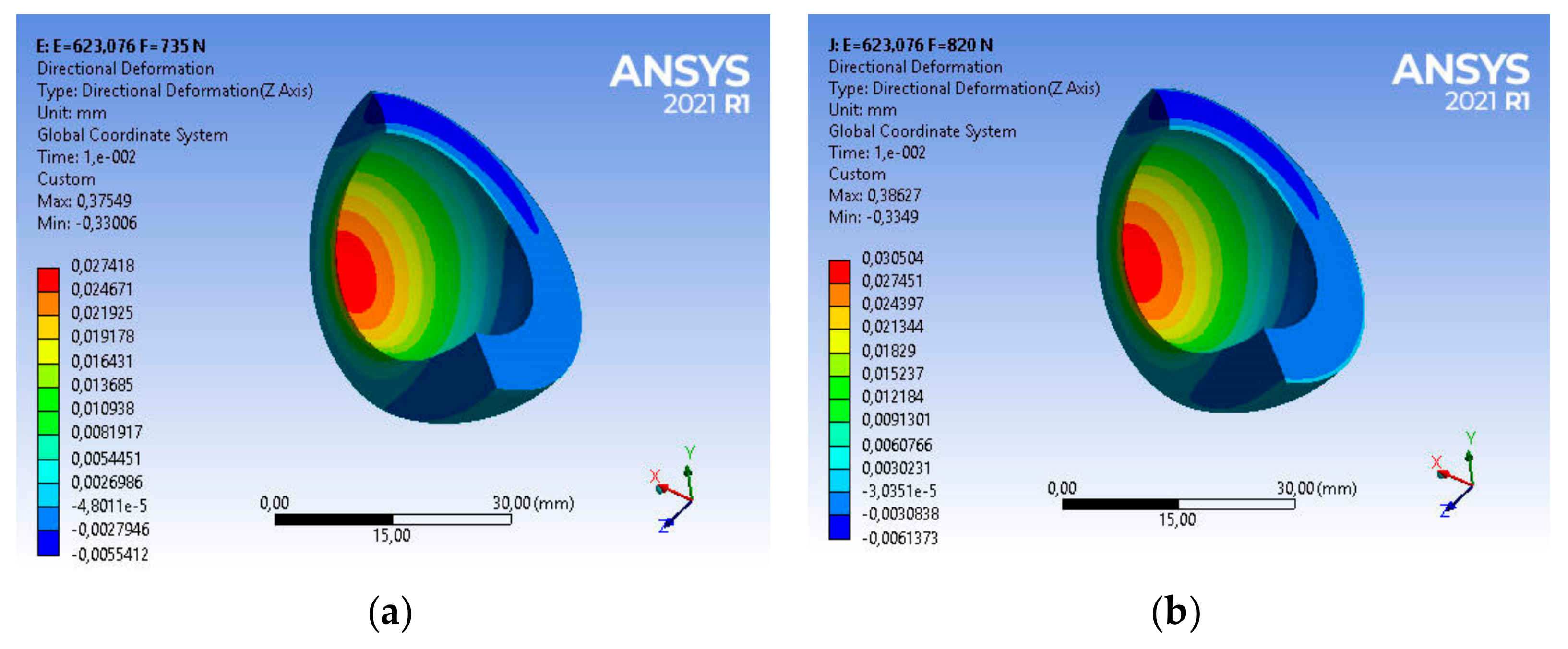
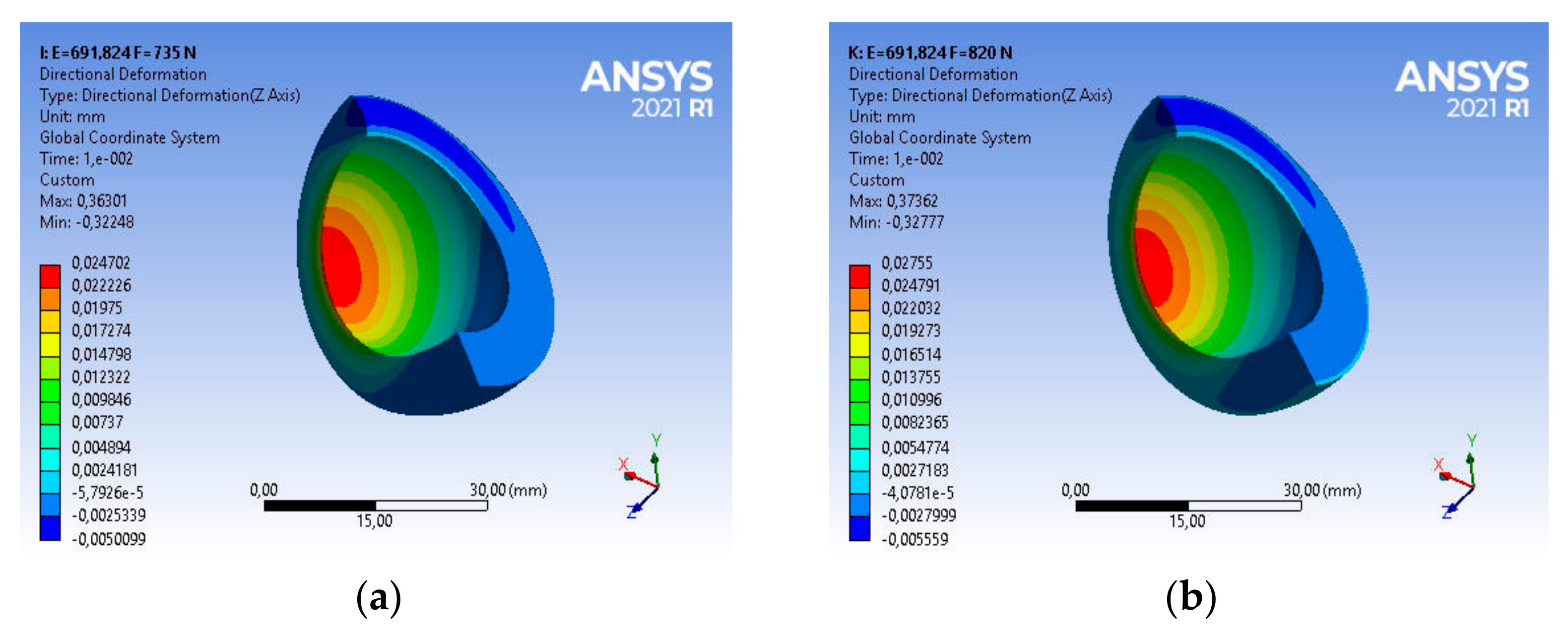
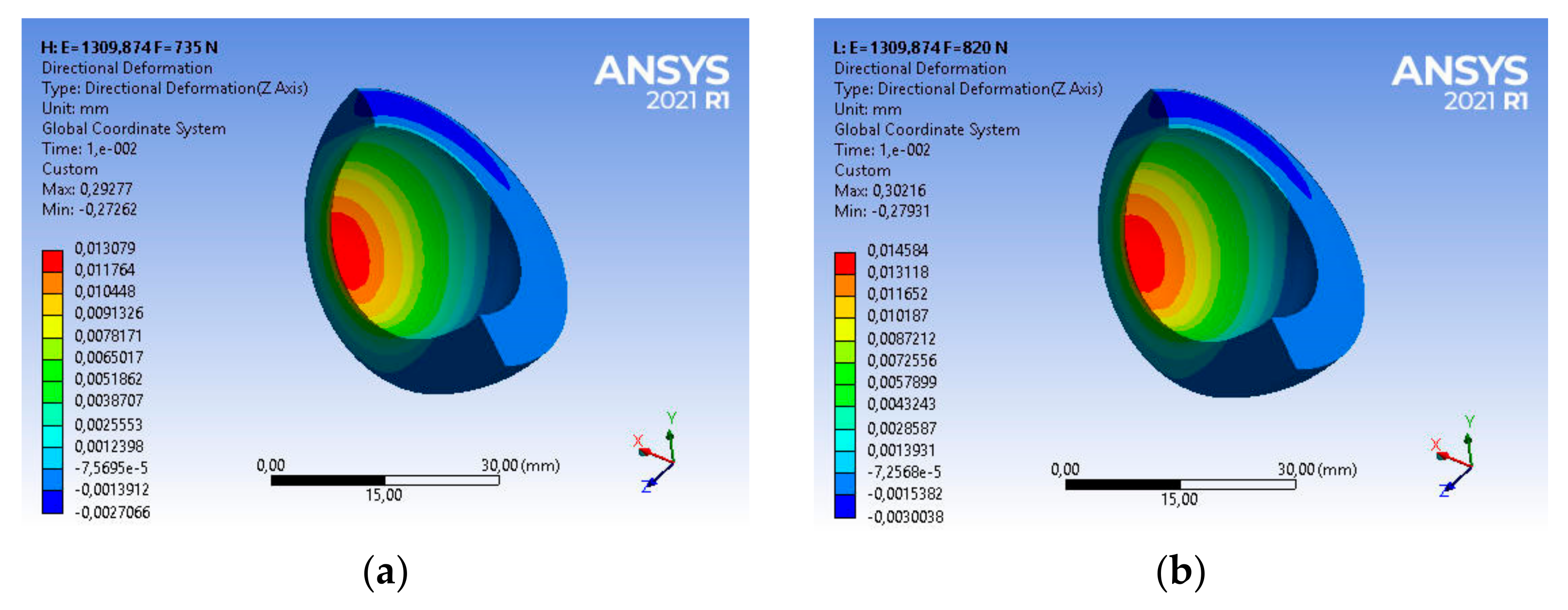
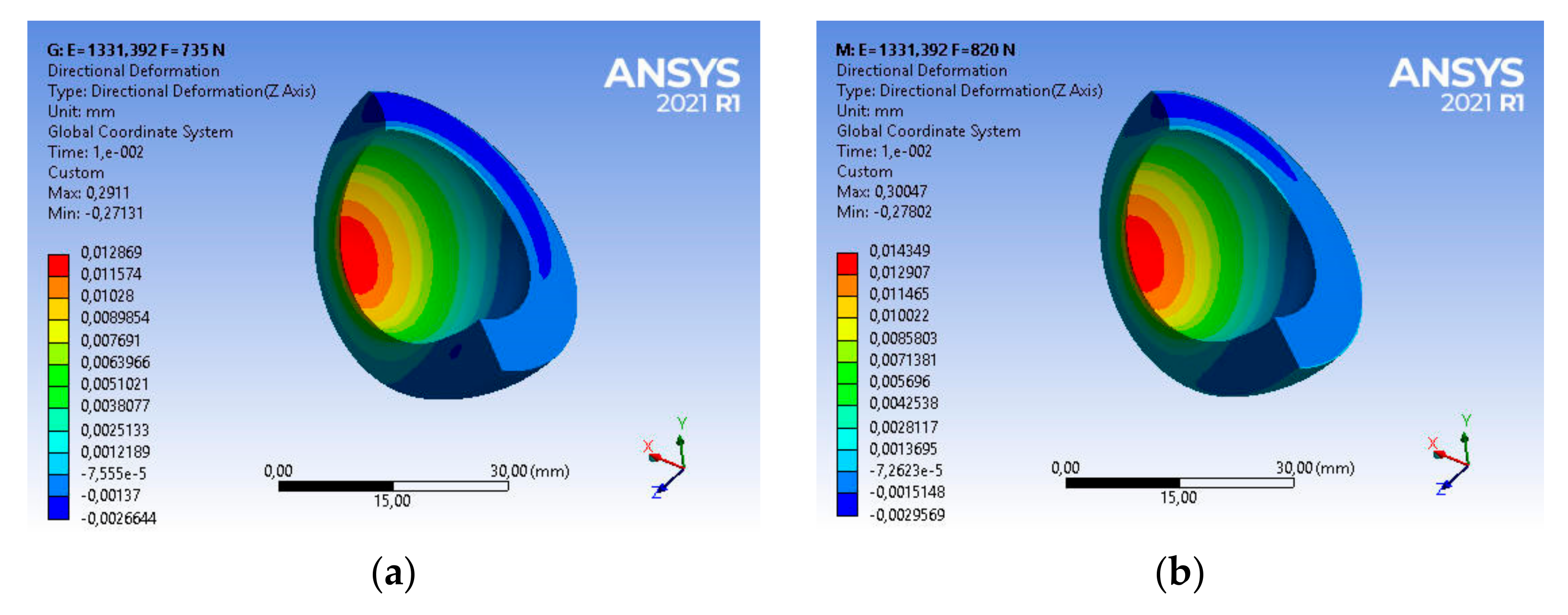
4.1. Results of Numerical Research
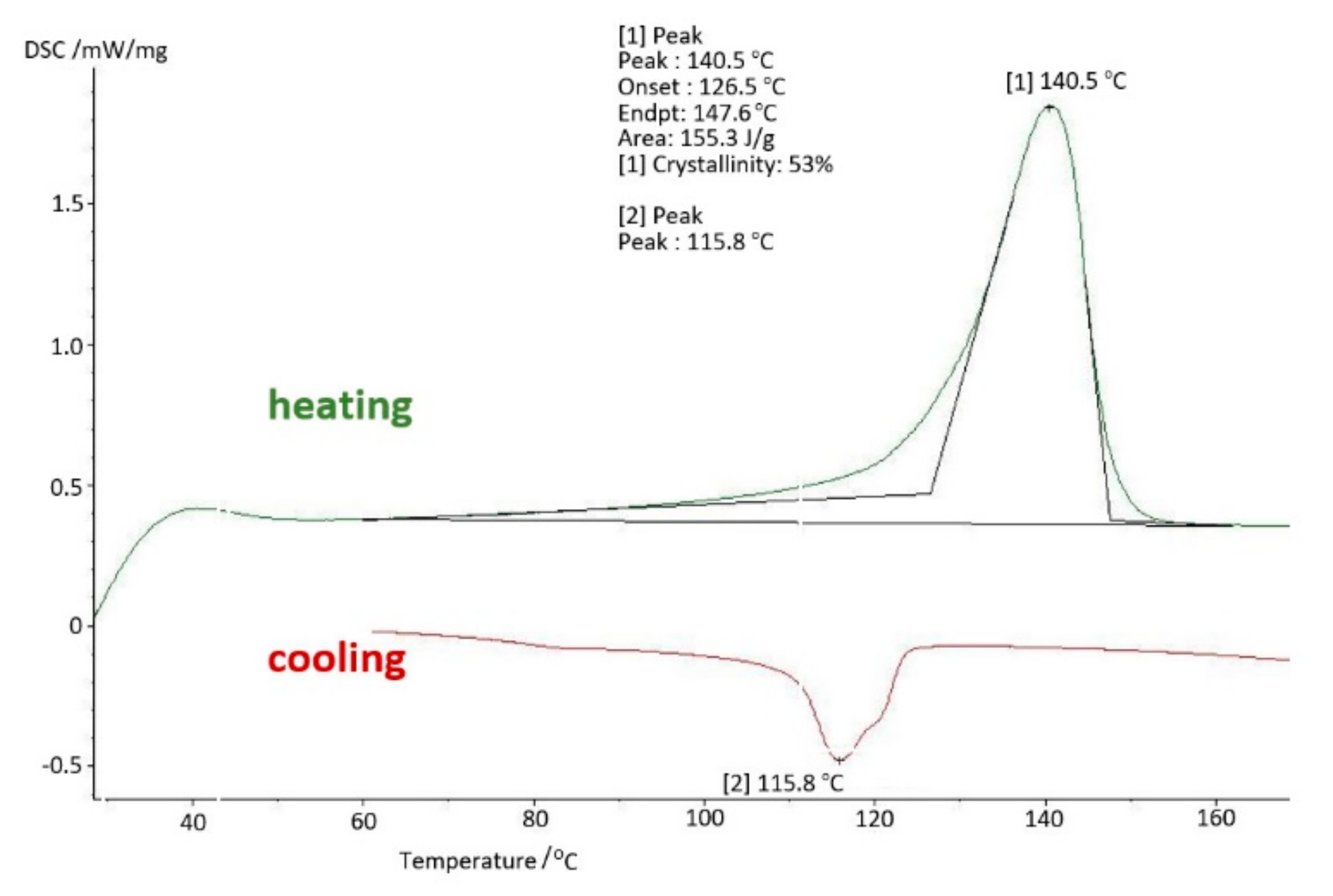
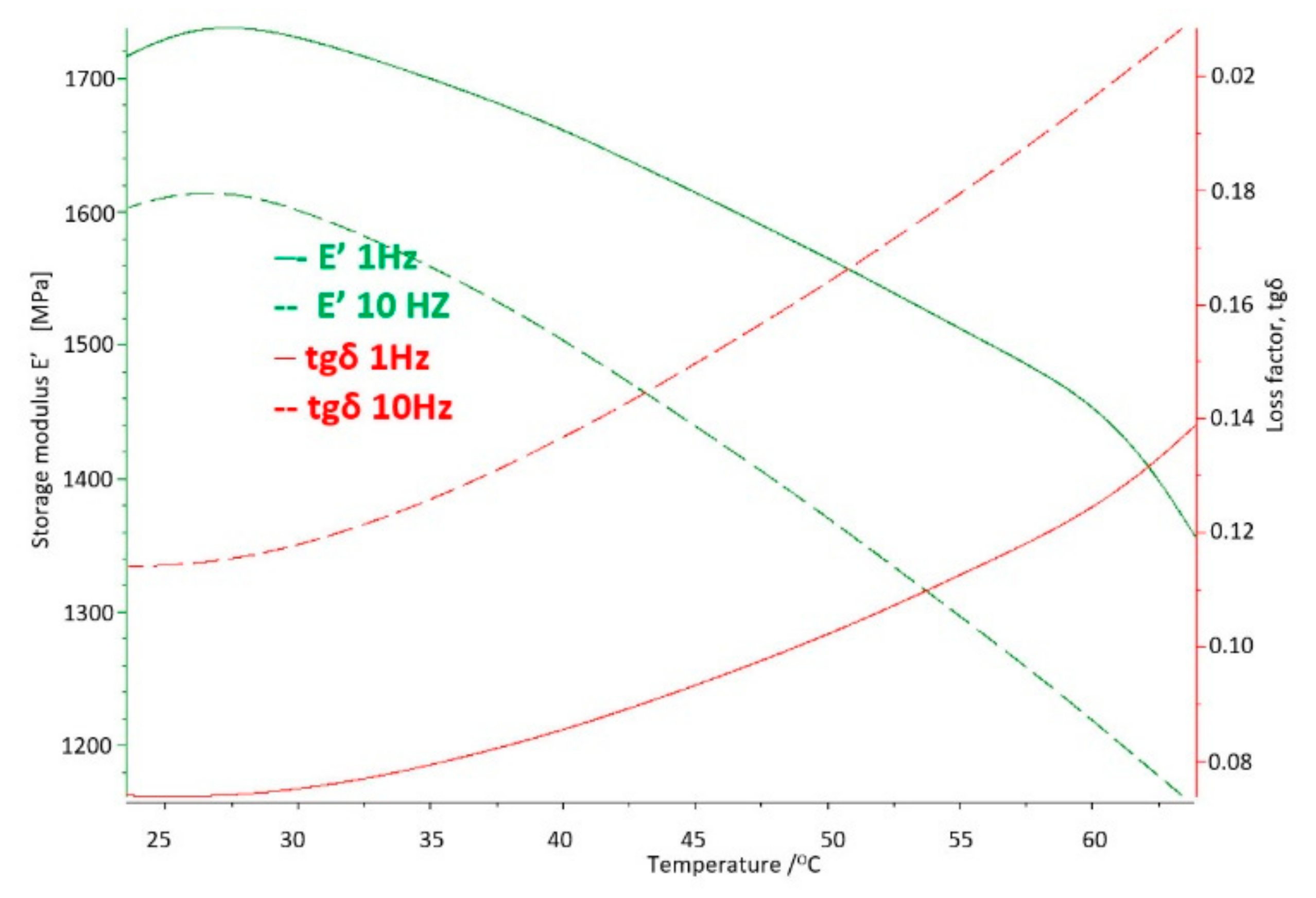
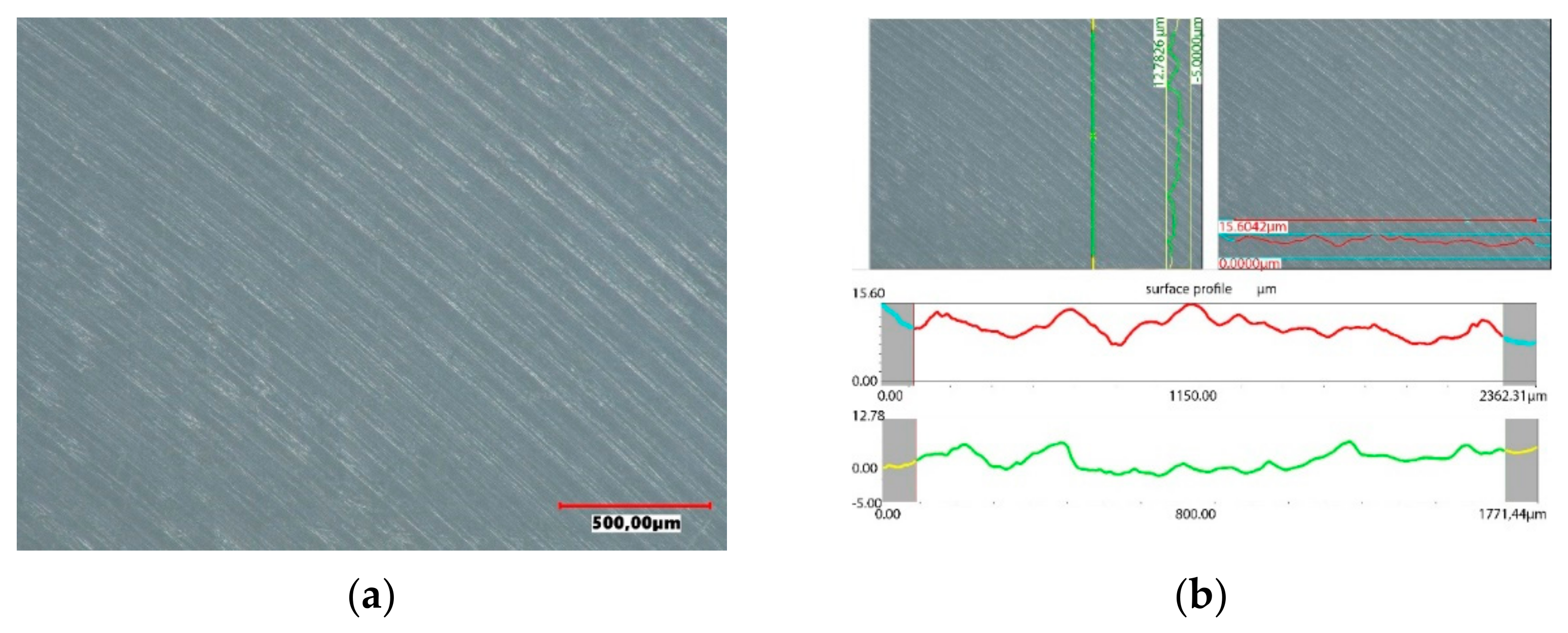
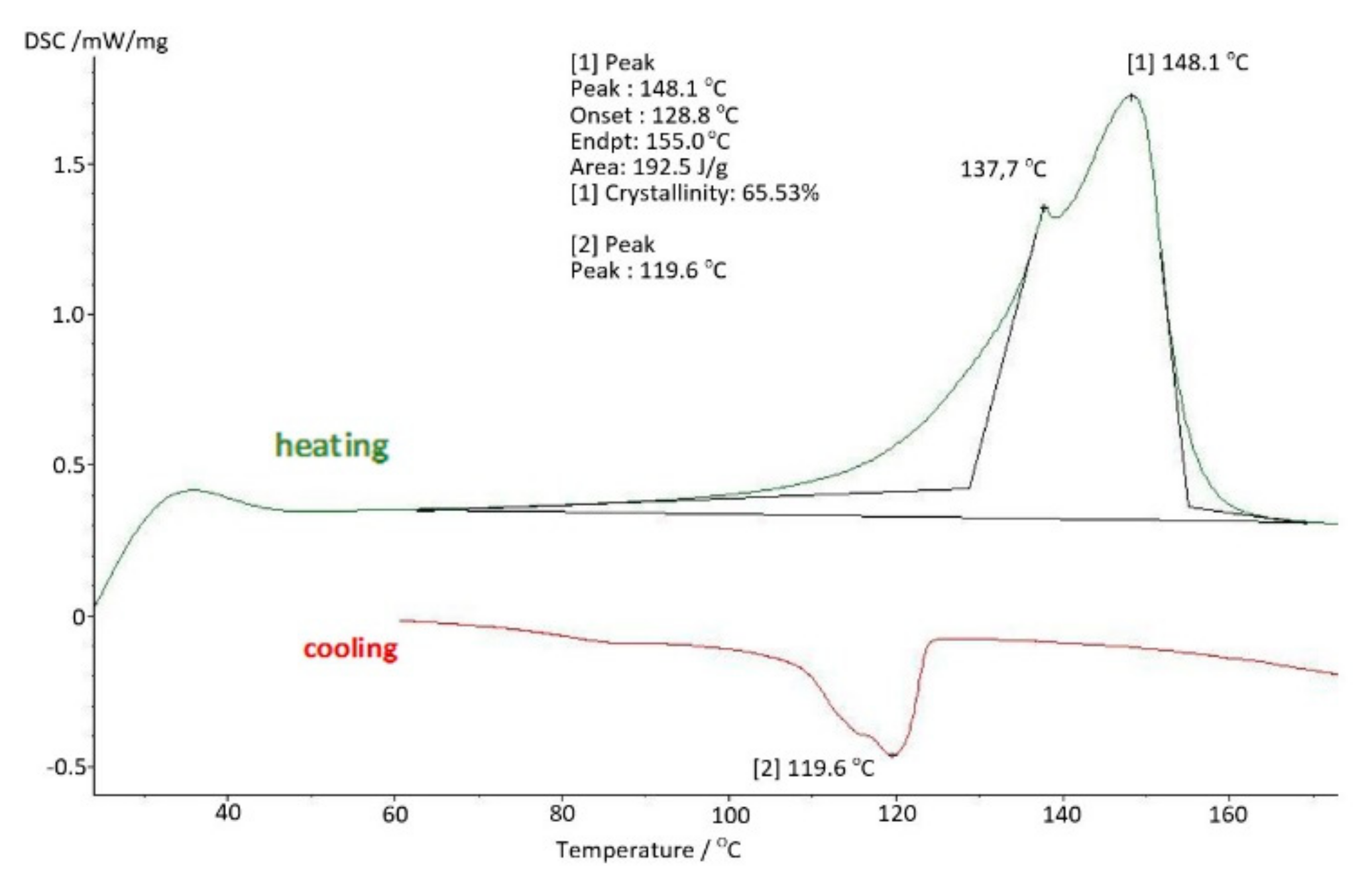
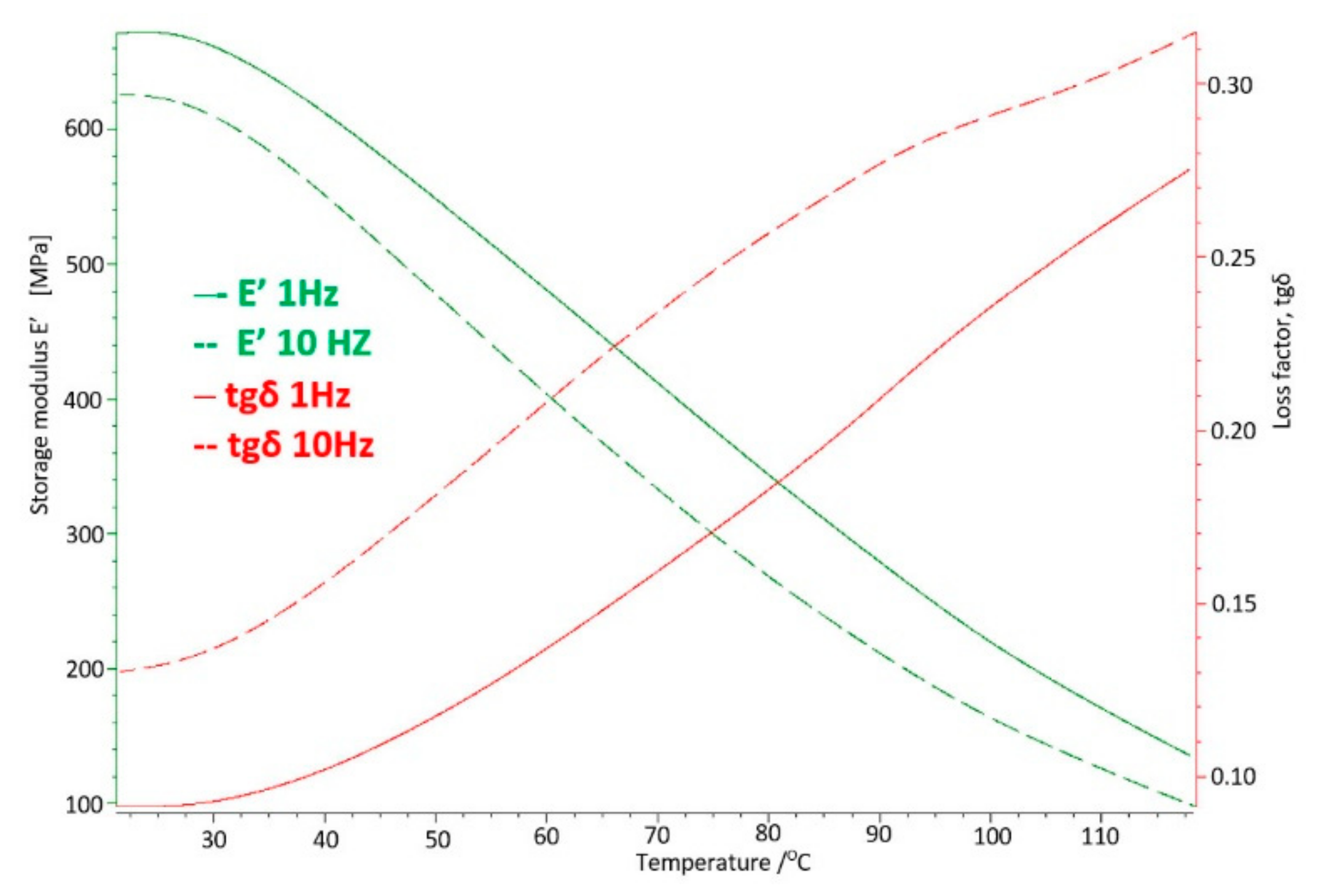
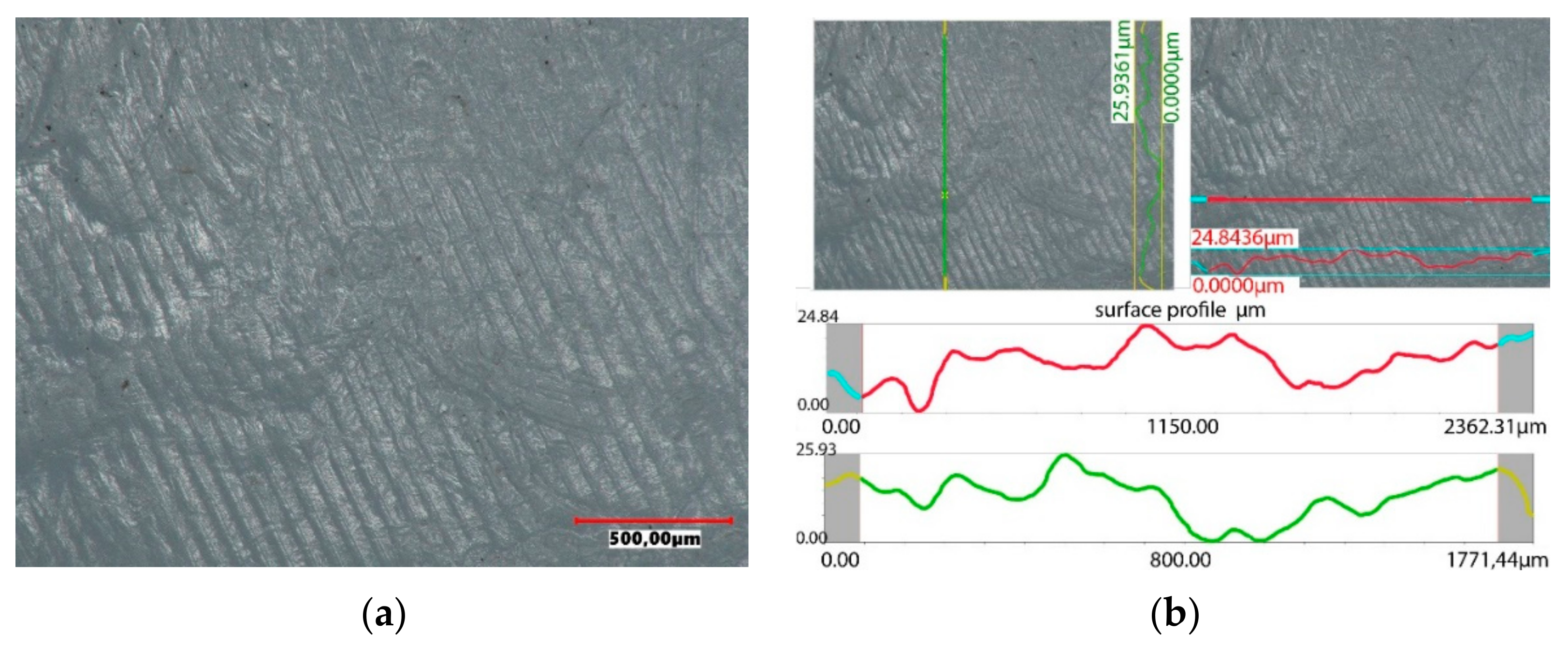
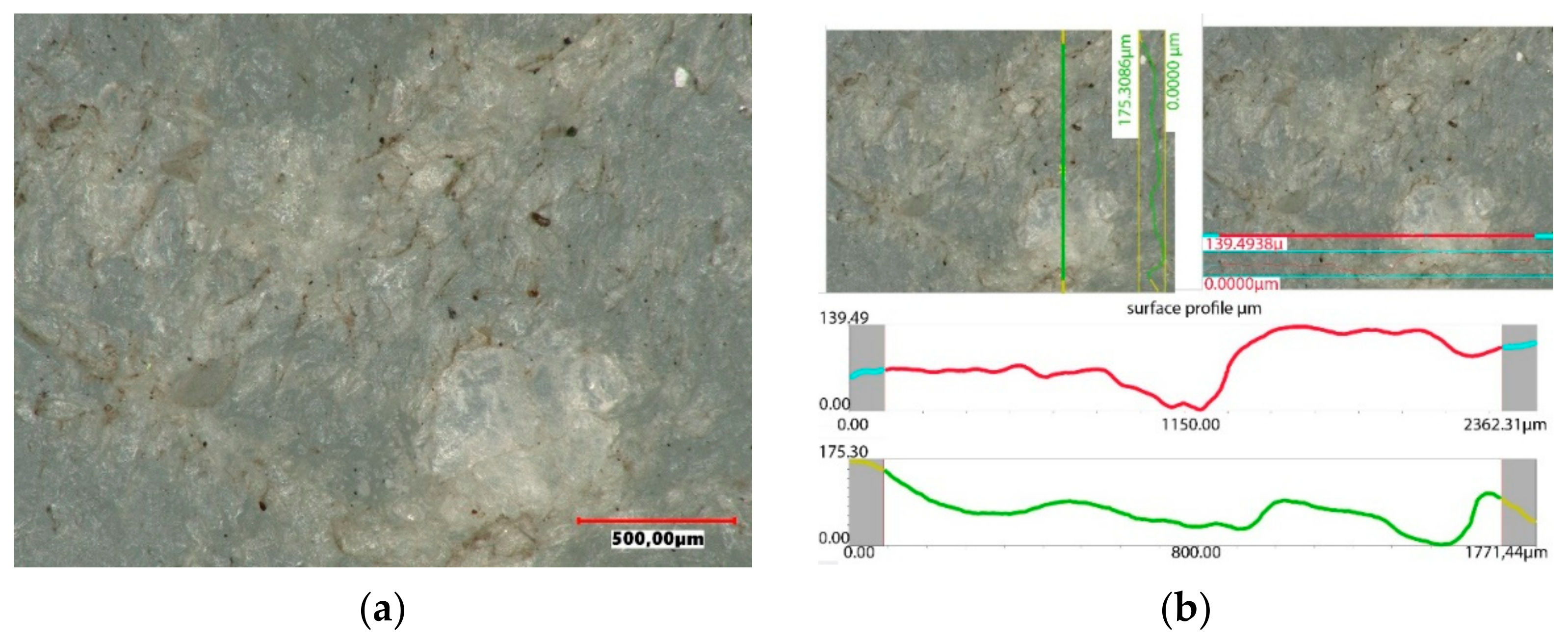
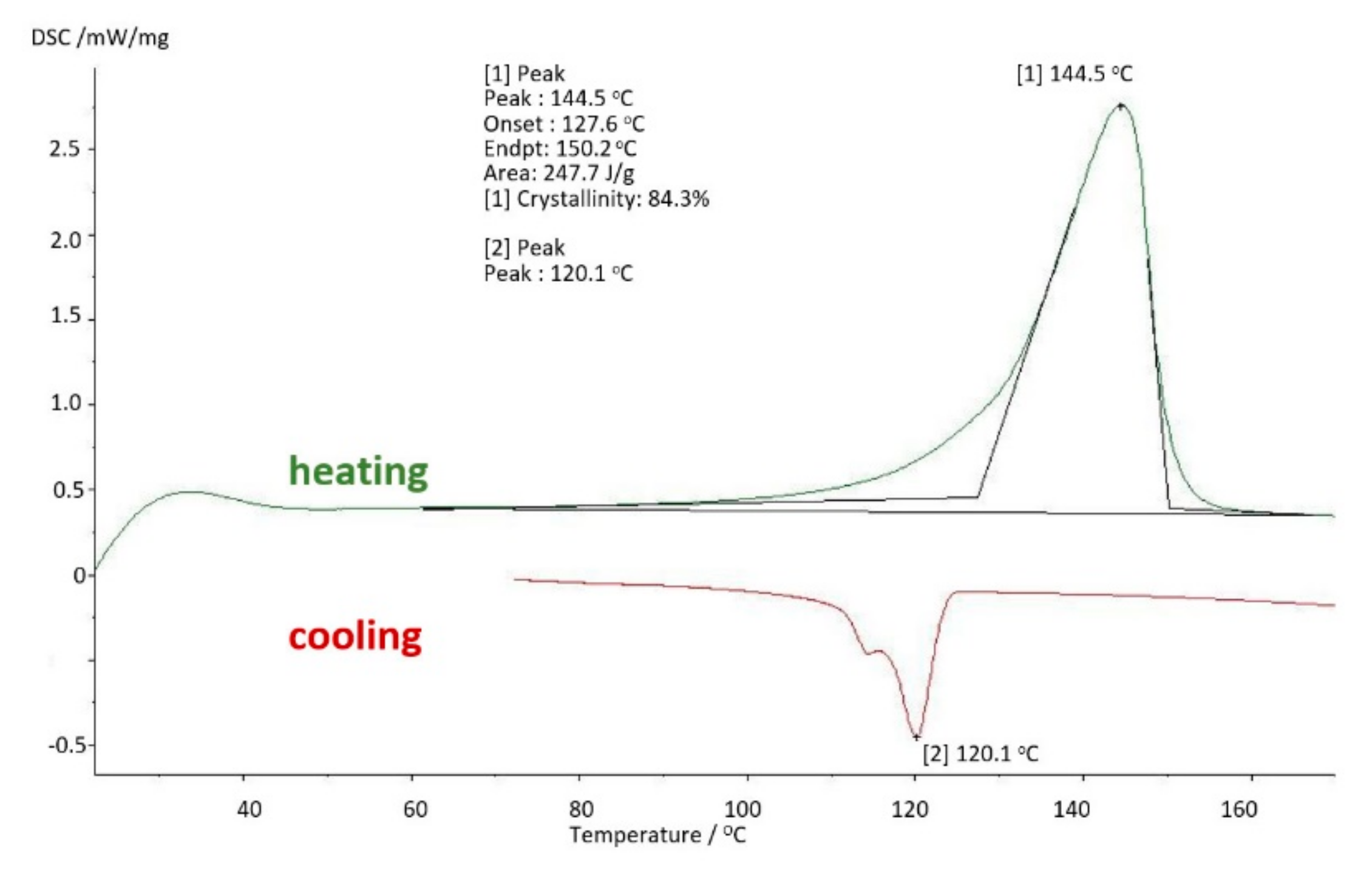
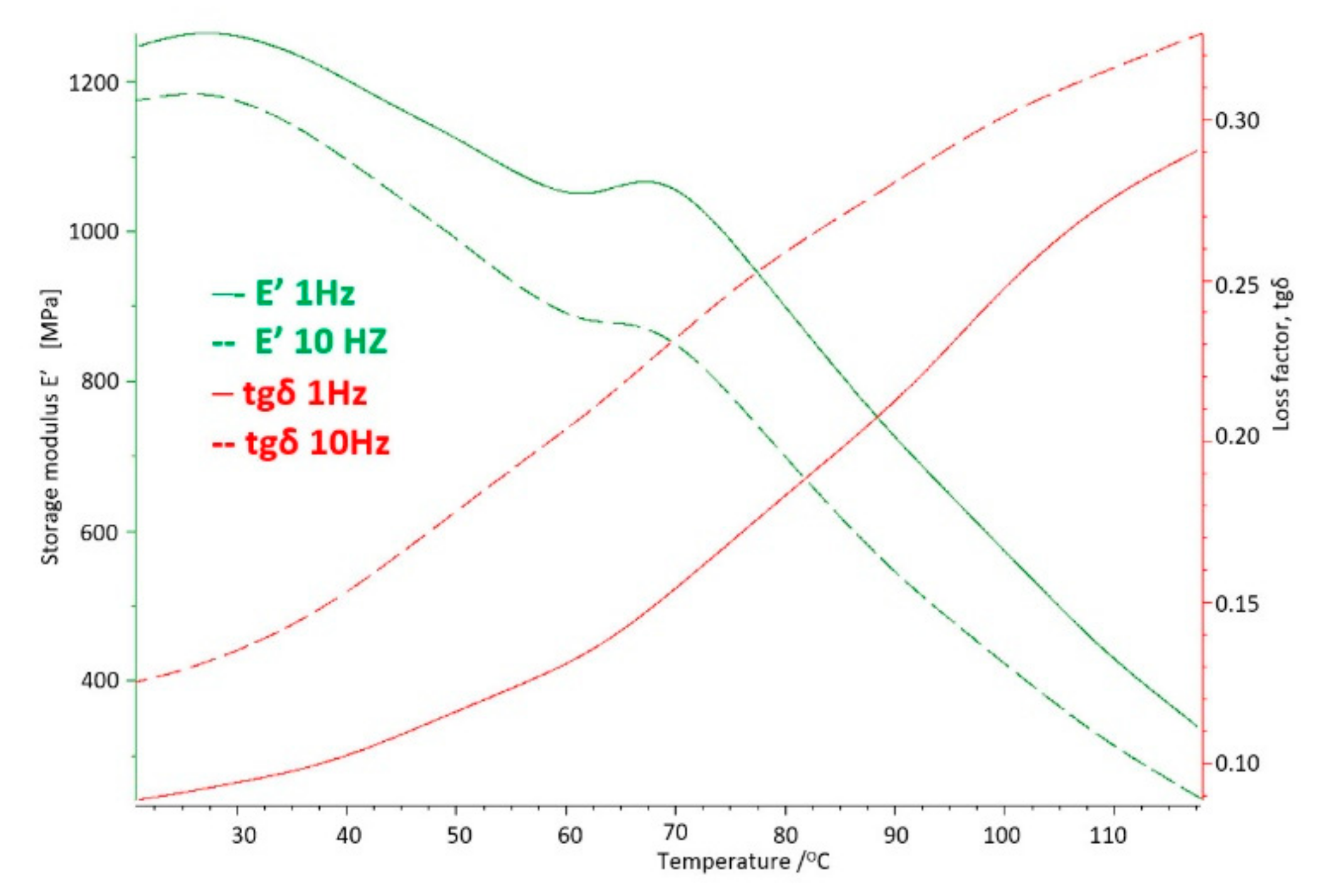
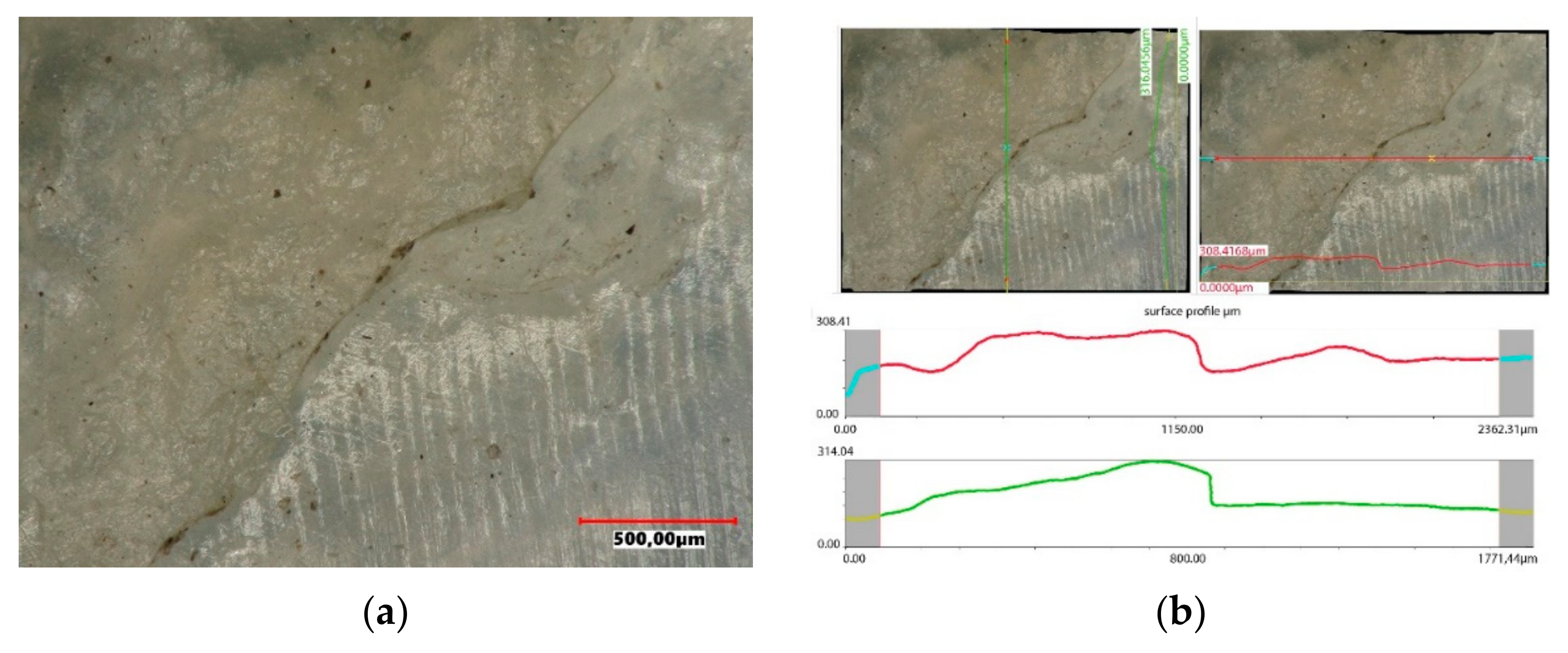
4.2. Research Results
- temperature range: RT up to 65 or 110 °C;
- heating rate: 2 K/min;
- strains amplitude: 120 µm;
- dynamic force: 5.2 [N];
- static force: 0.05 [N];
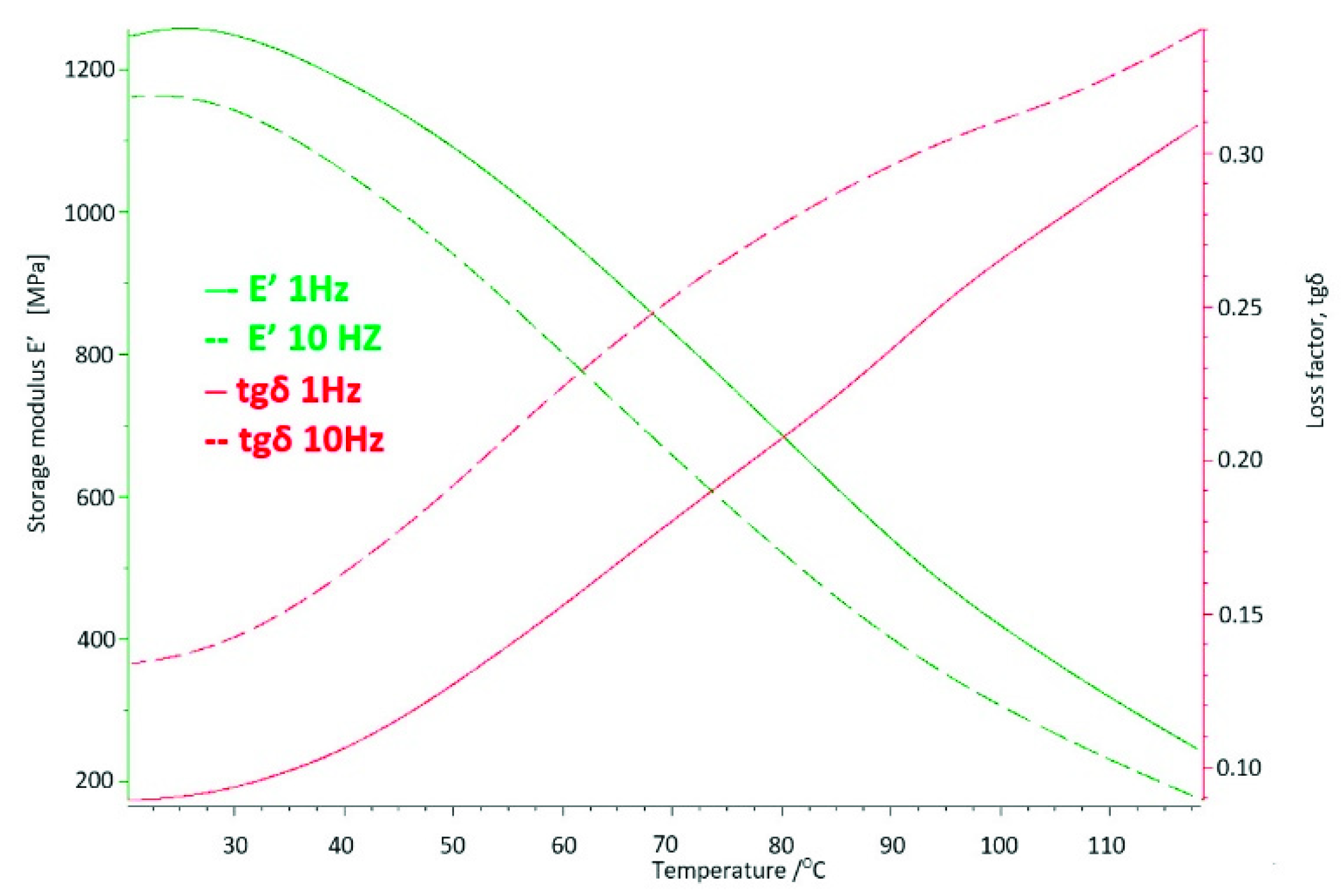
- frequency: 1 and 10 Hz.
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Santiago, M.S.; Aidar, F.J.; dos Santos Moraes, T.L.; de Farias Neto, J.P.; Vieira Filho, M.C.; de Vasconcelos, D.P.; Leite, V.S.; Doria, F.M.; Sobral Porto, E.; Albuquerque Madruga, R.E.T.T.; et al. The management between comorbidities and pain level with physical activity in individuals with hip osteoarthritis with surgical indication: A cross-sectional study. Medicina 2021, 57, 890. [Google Scholar] [CrossRef] [PubMed]
- Murphy, N.J.; Eyles, J.P.; Hunter, D.J. Hip osteoarthritis: Etiopathogenesis and implications for management. Adv. Ther. 2016, 33, 1921–1946. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szarek, A. Biomechaniczne i Biomateriałowe Determinanty Aseptycznego Obluzowania Endoprotez Stawu Biodrowego Człowieka; Wydawnictwo Politechniki Częstochowskiej: Częstochowa, Poland, 2015. [Google Scholar]
- Stone, R.C.; Baker, J. Painful Choices: A Qualitative exploration of facilitators and barriers to active lifestyles among adults with osteoarthritis. J. Appl. Gerontol. 2017, 36, 1091–1116. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, R.B.; Salles, M.J. Outcomes and risk factors in prosthetic joint infections by multidrug-resistant gram-negative bacteria: A retrospective cohort study. Antibiotics 2021, 10, 340. [Google Scholar] [CrossRef] [PubMed]
- Niemczewska-Wójcik, M.; Piekoszewski, W. The surface topography of a metallic femoral head and its influence on the wear mechanism of a polymeric acetabulum. Arch. Civ. Mech. Eng. 2017, 17, 307–317. [Google Scholar] [CrossRef]
- Miura, Y.; Hasegawa, M.; Sudo, A.; Pezzotti, G.; Puppulin, L. In-vivo degradation of middle-term highly cross-linked and remelted polyethylene cups: Modification induced by creep, wear and oxidation. J. Mech. Behav. Biomed. Mater. 2015, 51, 13–24. [Google Scholar] [CrossRef] [PubMed]
- Mordal, K.; Szarek, A. Analysis of stresses and strains distribution of polyethylene cups in hip joint endoprosthesis at various articular joints and friction conditions. Arch. Metall. Mater. 2021, 66, 523–530. [Google Scholar]
- Nabrdalik, M.; Sobociński, M. Modeling and computing of stress and strain distribution in uhmw polyethylene elements of chosen artificial human joints. Pol. J. Chem. Technol. 2020, 22, 1–8. [Google Scholar] [CrossRef]
- Prodinger, P.M.; Lazic, I.; Horas, K.; Burgkart, R.; von Eisenhart-Rothe, R.; Weissenberger, M.; Rudert, M. Revision arthroplasty through the direct anterior approach using an asymmetric acetabular component. J. Clin. Med. 2020, 9, 3031. [Google Scholar] [CrossRef] [PubMed]
- Mederake, M.; Hofmann, U.K.; Fink, B. New technique for custom-made spacers in septic two-stage revision of total hip arthroplasties. Antibiotics 2021, 10, 1073. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Renz, N.; Trampuz, A. Management of periprosthetic joint infection. Hip Pelvis 2018, 30, 138–146. [Google Scholar] [CrossRef] [PubMed]
- Choudhurya, D.; Ranušac, M.; Fleminga, R.A.; Vrbkad, M.; Křupkad, I.; Teetere, M.G.; Gossa, J.; Zoua, M. Mechanical wear and oxidative degradation analysis of retrieved ultra high molecular weight polyethylene acetabular cups. J. Mech. Behav. Biomed. Mater. 2018, 79, 314–323. [Google Scholar] [CrossRef] [PubMed]
- Nabrdalik, M.; Sobociński, M. Modeling of stress and strain distribution in uhmwpe elements of knee and hip human joints. Acta Phys. Pol. A 2020, 138, 224–227. [Google Scholar] [CrossRef]
- Kunal, A.; Singh, A.K. Magnetorheological finishing of UHMWPE acetabular cup surface and its performance analysis. Mater. Manuf. Process. 2020, 14, 1631–1649. [Google Scholar]
- Szarek, A. Mechanical Destruction of Joints Implants. Izdatel’stvo Nauka i Obrazovanie; Publishing House Education and Science s.r.o.: Prague, Czech Republic; Dniepr, Ukraine, 2018. [Google Scholar]
- Cook, M.J.; Sorial, A.K.; Lunt, M.; Board, T.N.; O’Neill, T.W. Effect of timing and duration of statin exposure on risk of hip or knee revision arthroplasty: A population-based cohort study. J. Rheumatol. 2020, 47, 441–448. [Google Scholar] [CrossRef] [PubMed]
- Singh, J.A.; Yu, S.; Chen, L.; Cleveland, J.D. Rates of total joint replacement in the United States: Future projections to 2020–2040 using the National Inpatient Sample. J. Rheumatol. 2019, 46, 1134–1140. [Google Scholar] [CrossRef] [PubMed]
- Szarek, A.; Stradomski, G.; Łukomska-Szarek, J.; Rydz, D.; Wolański, W.; Joszko, K. Wear morphology on the surfaces of cocrmo unicompartmental knee joint endoprostheses as elements of metal-metal friction nodes. Materials 2020, 13, 2689. [Google Scholar] [CrossRef] [PubMed]
- NFZ. Endoprotezoplastyka Stawowa W 2012. Available online: https://www.nfz.gov.pl/download/gfx/nfz/pl/defaultstronaopisowa/349/5/1/2013_05_07_endoprotezy_2012_analiza.pdf (accessed on 5 April 2020).
- NFZ. Realizacja Świadczeń Endoprotezoplastyki Stawowej W 2013. Available online: https://www.nfz.gov.pl/download/gfx/nfz/pl/defaultstronaopisowa/349/1/1/2014_06_02_endoprotezoplastyka_2013.pdf (accessed on 19 November 2021).
- NFZ. Realizacja Świadczeń Endoprotezoplastyki Stawowej W 2014. Available online: https://www.nfz.gov.pl/download/gfx/nfz/pl/defaultstronaopisowa/349/26/1/realizacja_swiadczen_endoprotezoplastyki_stawowej_w_2014_r..pdf (accessed on 19 November 2021).
- NFZ. Realizacja Świadczeń Endoprotezoplastyki Stawowej W 2015. Available online: https://www.nfz.gov.pl/download/gfx/nfz/pl/defaultstronaopisowa/349/30/1/cbe_za_2015.pdf (accessed on 19 November 2021).
- NFZ. Realizacja Świadczeń Endoprotezoplastyki Stawowej W 2016. Available online: https://www.nfz.gov.pl/download/gfx/nfz/pl/defaultstronaopisowa/349/34/1/cbe_za_2016.pdf (accessed on 19 November 2021).
- NFZ. Realizacja Świadczeń Endoprotezoplastyki Stawowej W 2017. Available online: https://www.nfz.gov.pl/download/gfx/nfz/pl/defaultstronaopisowa/349/38/1/realizacja_swiadczen_endoprotezoplastyki_stawowej_w_2017_r.pdf (accessed on 19 November 2021).
- NFZ. Realizacja Świadczeń Endoprotezoplastyki Stawowej W 2018. Available online: https://www.nfz.gov.pl/download/gfx/nfz/pl/defaultstronaopisowa/349/46/1/cbe_za_2018.pdf (accessed on 5 November 2021).
- NFZ. Realizacja Świadczeń Endoprotezoplastyki Stawowej W 2019. Available online: https://www.nfz.gov.pl/download/gfx/nfz/pl/defaultstronaopisowa/349/47/1/realizacja_swiadczen_endoprotezoplastyki_stawowej_w_2019r.docx (accessed on 19 November 2021).
- „Niecovidowe” Efekty COVID-19: Endoprotezoplastyka Biodra–Hospitalizacje. Available online: http://pharmamarket.pl/niecovidowe-efekty-covid-19-endoprotezoplastyka-biodra-liczba-i-wartosc-hospitalizacji/ (accessed on 5 November 2021).
- NFZ. Realizacja Świadczeń Endoprotezoplastyki Stawowej W 2020. Available online: https://www.nfz.gov.pl/download/gfx/nfz/pl/defaultstronaopisowa/349/57/1/cbe_na_strone_2020.docx (accessed on 5 November 2021).
- NBP Exchange Rates. Available online: https://www.money.pl/pieniadze/nbp/srednie/?date=2005-12-30 (accessed on 18 August 2021).
- NBP Exchange Rates. Available online: https://www.money.pl/pieniadze/nbp/srednie/?date=2019-12-30 (accessed on 18 August 2021).
- Jurkojć, J.; Michnik, R.; Pauk, J. Identyfication of muscle forces acting in lower limbs with the use of planar and spatial mathematical model. J. Vibroengineering 2009, 11, 566–570. [Google Scholar]
- Kusz, D.; Wojciechowski, P.; Cielinski, L.S.; Iwaniak, A.; Jurkojc, J.; Gasiorek, D. Stress distribution around TKR implant: Are lab results consistent with observational studies. Acta Bioeng. Biomech. 2008, 10, 21–26. [Google Scholar] [PubMed]



























{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Voivodeship in Poland | Number of Hip Arthroplasty in 2020 | Total Number of Arthroplasty in 2020 |
|---|---|---|
| Lower Silesia | 3557 | 5368 |
| Kuyavian-Pomeranian Voivodeship | 2259 | 3395 |
| Lublin | 2286 | 3288 |
| Lubuskie | 1365 | 2179 |
| Lodzkie | 3269 | 5212 |
| Lesser Poland | 4390 | 7131 |
| Masovian Voivodeship | 6771 | 10,599 |
| Opole Province | 1147 | 1715 |
| Podkarpackie Province | 2527 | 3840 |
| Podlasie | 1147 | 1902 |
| Pomeranian | 2458 | 3749 |
| Silesian | 4502 | 6930 |
| Świętokrzyskie Province | 1587 | 2549 |
| Warmia-Masuria Province | 1786 | 2764 |
| Greater Poland | 4816 | 7670 |
| West Pomeranian | 2391 | 3736 |
| Time of Use in the Body | DMTA Studies | DSC Studies | |||
|---|---|---|---|---|---|
| E′ 1 Hz 40 °C, [MPa] | tgδ 1 Hz 40 °C | Melting Point, Tm °C | Enthalpy of Melting, [J/g] | Degree of Crystallinity, K% | |
| Base sample | 528 | 0.13 | 140.8 | 155.3 | 53 |
| 4 years | 557 | 0.16 | 148.1 | 192.5 | 65.53 |
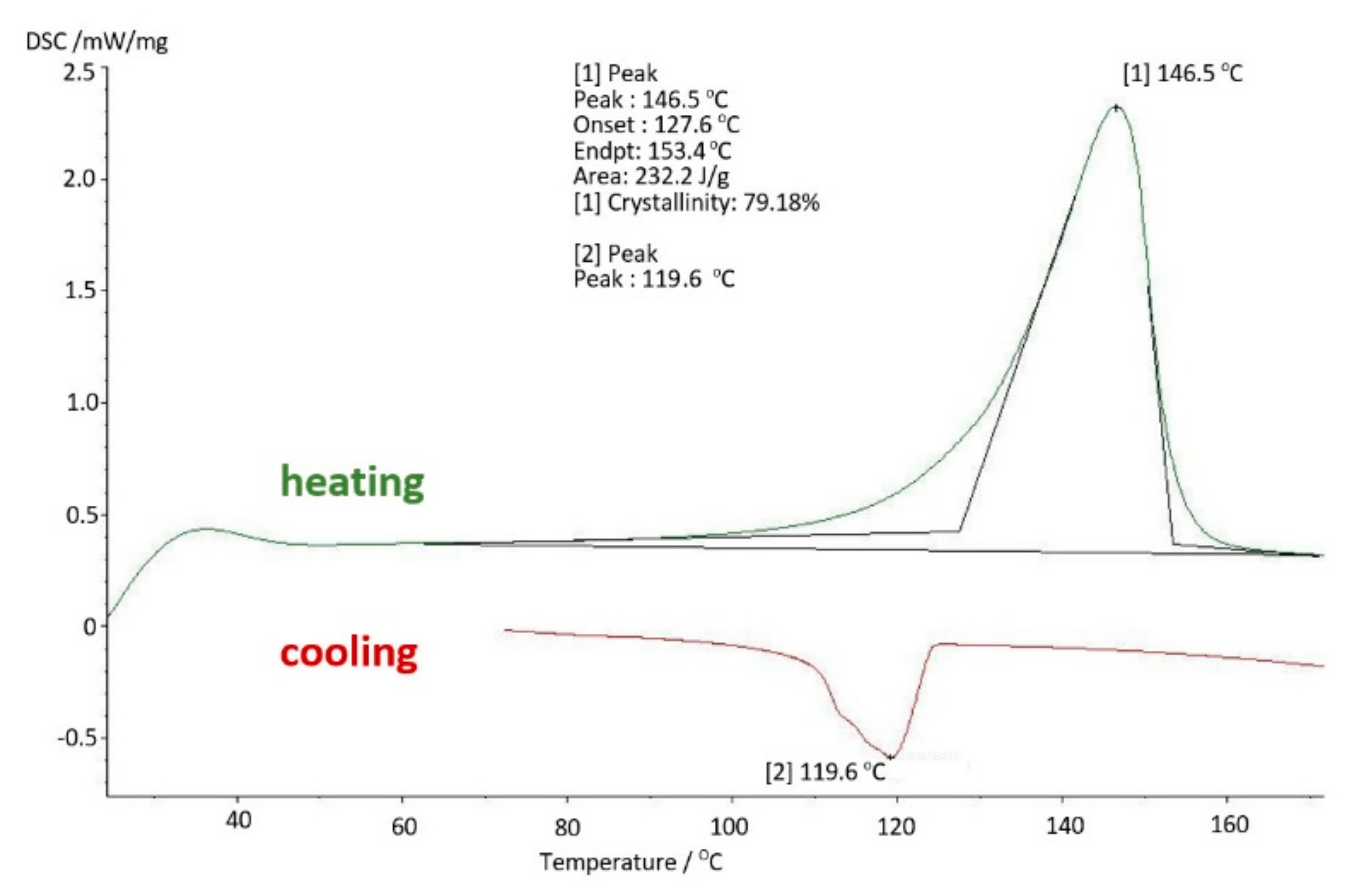
| 8 years | 1164 | 0.17 | 146.5 | 232.2 | 79.18 |
| 10 years | 1101 | 0.15 | 144.5 | 247.7 | 84.3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szarek, A.; Postawa, P.; Stachowiak, T.; Paszta, P.; Redutko, J.; Mordal, K.; Kalwik, A.; Łukomska-Szarek, J.; Gzik, M.; Joszko, K.; et al. The Analysis of Polyethylene Hip Joint Endoprostheses Strength Parameters Changes after Use inside the Human Body. Materials 2021, 14, 7091. https://0-doi-org.brum.beds.ac.uk/10.3390/ma14227091
Szarek A, Postawa P, Stachowiak T, Paszta P, Redutko J, Mordal K, Kalwik A, Łukomska-Szarek J, Gzik M, Joszko K, et al. The Analysis of Polyethylene Hip Joint Endoprostheses Strength Parameters Changes after Use inside the Human Body. Materials. 2021; 14(22):7091. https://0-doi-org.brum.beds.ac.uk/10.3390/ma14227091
Chicago/Turabian StyleSzarek, Arkadiusz, Przemysław Postawa, Tomasz Stachowiak, Piotr Paszta, Joanna Redutko, Katarzyna Mordal, Aleksandra Kalwik, Justyna Łukomska-Szarek, Marek Gzik, Kamil Joszko, and et al. 2021. "The Analysis of Polyethylene Hip Joint Endoprostheses Strength Parameters Changes after Use inside the Human Body" Materials 14, no. 22: 7091. https://0-doi-org.brum.beds.ac.uk/10.3390/ma14227091