
3D Printed Customized Facemask for Maxillary Protraction in the Early Treatment of a Class III Malocclusion: Proof-of-Concept Clinical Case

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
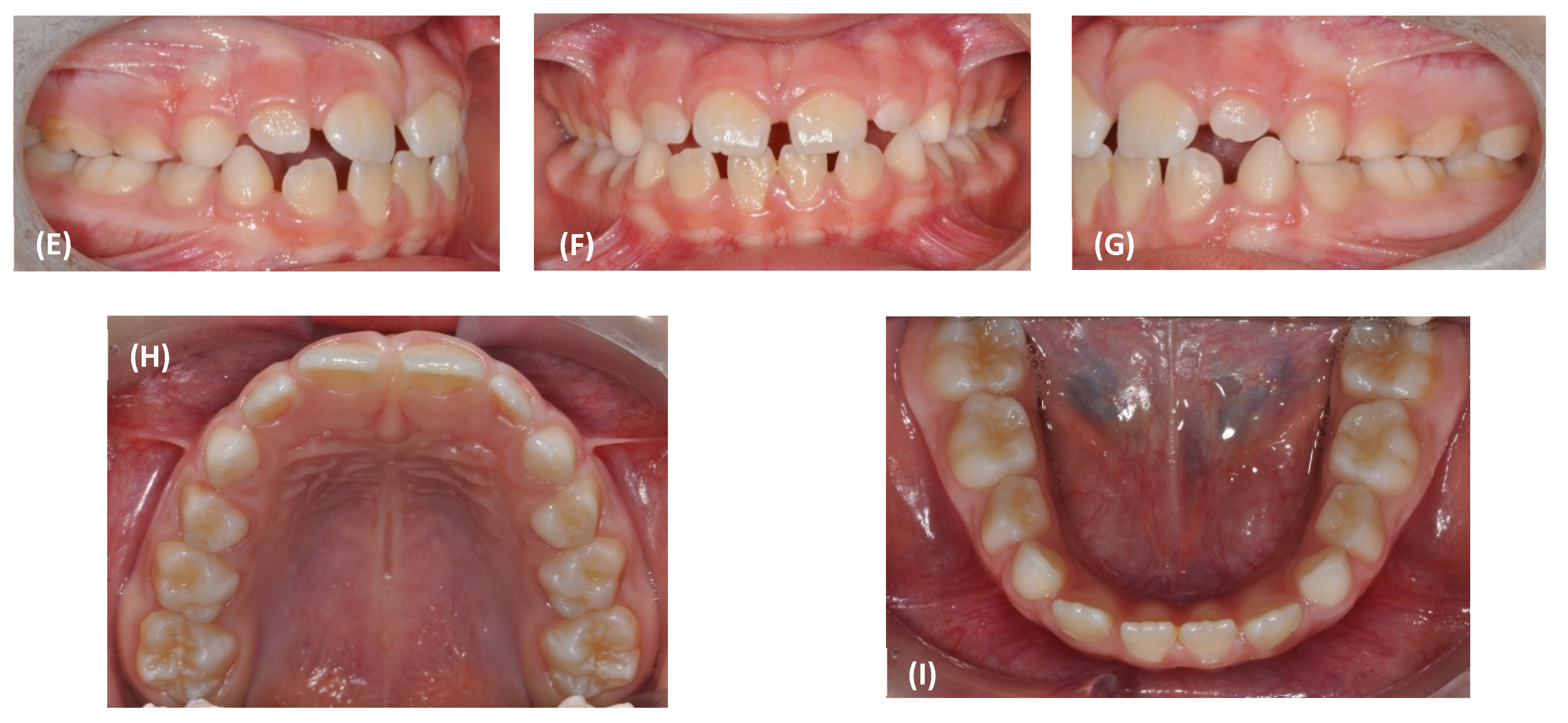
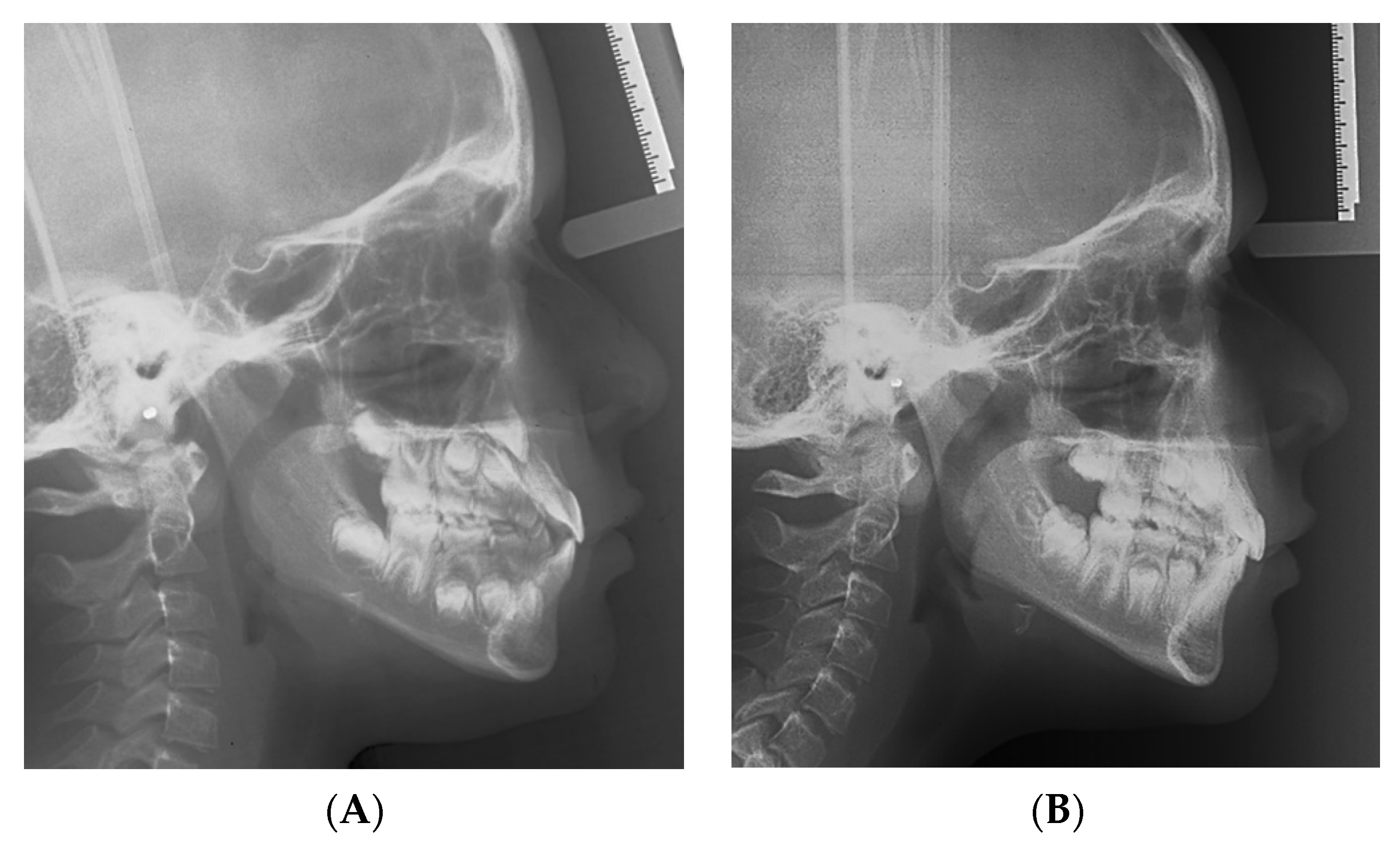
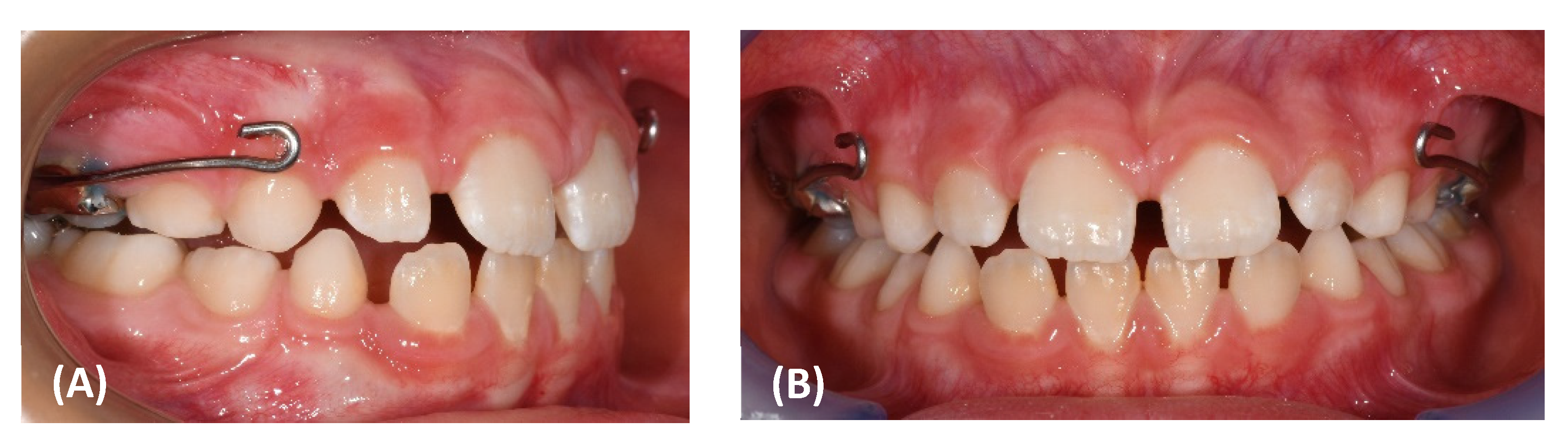
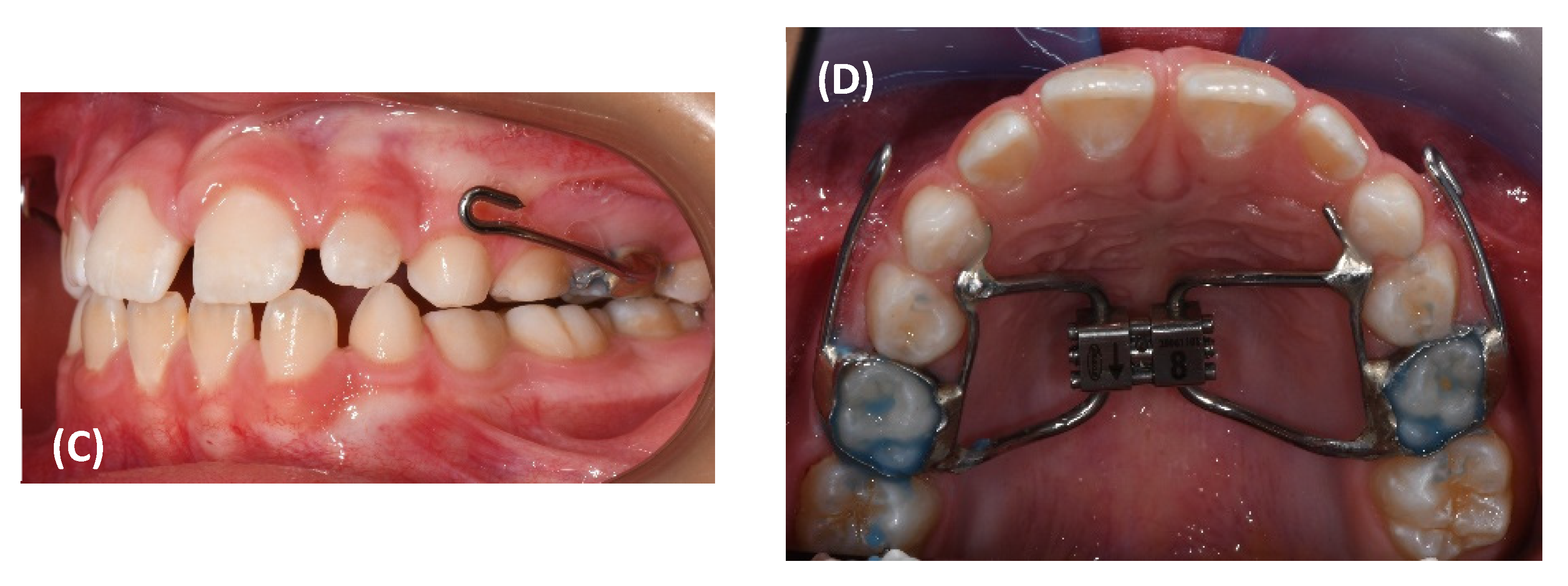
3. Results
4. Discussion
5. Conclusions
6. Patents
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Woon, S.C.; Thiruvenkatachari, B. Early orthodontic treatment for Class III malocclusion: A systematic review and meta-analysis. Am. J. Orthod. Dentofac. Orthop. 2017, 151, 28–52. [Google Scholar] [CrossRef] [PubMed]
- Mandall, N.; Cousley, R.; DiBiase, A.; Dyer, F.; Littlewood, S.; Mattick, R.; Nute, S.J.; Doherty, B.; Stivaros, N.; McDowall, R.; et al. Early class III protraction facemask treatment reduces the need for orthognathic surgery: A multi-centre, two-arm parallel randomized, controlled trial. J. Orthod. 2016, 43, 164–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Angelieri, F.; Franchi, L.; Cevidanes, L.H.S.; Hino, C.T.; Nguyen, T.; McNamara, J.A., Jr. Zygomaticomaxillary suture maturation: A predictor of maxillary protraction? Part I—A classification method. Orthod. Craniofac. Res. 2017, 20, 85–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Angelieri, F.; Ruellas, A.C.; Yatabe, M.S.; Cevidanes, L.H.S.; Franchi, L.; Toyama-Hino, C.; De Clerck, H.J.; Nguyen, T.; McNamara, J.A., Jr. Zygomaticomaxillary suture maturation: Part II—The influence of sutural maturation on the response to maxillary protraction. Orthod. Craniofac. Res. 2017, 20, 152–163. [Google Scholar] [CrossRef] [Green Version]
- Franchi, L.; Baccetti, T.; McNamara, J.A. Postpubertal assessment of treatment timing for maxillary expansion and protraction therapy followed by fixed appliances. Am. J. Orthod. Dentofac. Orthop. 2004, 126, 555–568. [Google Scholar] [CrossRef]
- Watkinson, S.; Harrison, J.E.; Furness, S.; Worthington, H.V. Orthodontic treatment for prominent lower front teeth (Class III malocclusion) in children. Cochrane Database Syst. Rev. 2013, 30, CD003451. [Google Scholar] [CrossRef] [Green Version]
- Zhang, W.; Qu, H.C.; Yu, M.; Zhang, Y. The effects of maxillary protraction with or without rapid maxillary expansion and age factors in treating Class III malocclusion: A Meta-Analysis. PLoS ONE 2015, 10, e0130096. [Google Scholar] [CrossRef] [Green Version]
- Smyth, R.S.D.; Ryan, F.S. Early treatment of class III malocclusion with facemask. Evid. Based Dent. 2017, 22, 107–108. [Google Scholar] [CrossRef]
- Foersch, M.; Jacobs, C.; Wriedt, S.; Hechtner, M.; Wehrbein, H. Effectiveness of maxillary protraction using facemask with or without maxillary expansion: A systematic review and meta-analysis. Clin. Oral Investig. 2015, 19, 1181–1192. [Google Scholar] [CrossRef]
- Cordasco, G.; Matarese, G.; Rustico, L.; Fastuca, S.; Caprioglio, A.; Lindauer, S.J.; Nucera, R. Efficacy of orthopedic treatment with protraction facemask on skeletal Class III malocclusion: A systematic review and meta-analysis. Orthod. Craniofac. Res. 2014, 17, 133–143. [Google Scholar] [CrossRef]
- Yepes, E.; Quintero, P.; Rueda, Z.V.; Pedroza, A. Optimal force for maxillary protraction facemask therapy in the early treatment of class III malocclusion. Eur. J. Orthod. 2014, 36, 586–594. [Google Scholar] [CrossRef] [PubMed]
- Stocker, B.; Willmann, J.H.; Wilmes, B.; Vasudavan, S.; Drescher, D. Wear-time recording during early Class III facemask treatment using TheraMon chip technology. Am. J. Orthod. Dentofac. Orthop. 2016, 150, 533–540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abu Alhaija, E.S.; Karajeh, M.A. Acceptability and attractiveness of intra- and extra-oral orthodontic appliances. Int. J. Orthod. 2013, 24, 11–17. [Google Scholar]
- Arreghini, A.; Trigila, S.; Lombardo, L.; Siciliani, G. Objective assessment of compliance with intra- and extraoral removable appliances. Angle Orthod. 2017, 87, 88–95. [Google Scholar] [CrossRef] [PubMed]
- Ierardo, G.; Luzzi, V.; Vozza, I.; Polimeni, A.; Bossù, M. Skin irritation from a facial mask in Class III malocclusion: Evaluation of individual silicone chin cups in a group of 100 children. Minerva Stomatol. 2018, 67, 45–48. [Google Scholar] [CrossRef]
- Cacciatore, G.; Poletti, L.; Ghislanzoni, L.H. A chairside customized chin cup. J. Clin. Orthod. 2013, 47, 352. [Google Scholar]
- Turley, P.K. Orthopedic correction of Class III malocclusion with palatal expansion and custom protraction headgear. J. Clin. Orthod. 1988, 22, 314–325. [Google Scholar]
- Orton, H.S.; Noar, J.H.; Smith, A.J. The customized facemask. J. Clin. Orthod. 1992, 26, 230–235. [Google Scholar]
- Available online: https://www.blender.org (accessed on 27 February 2022).
- Available online: https://www.shapeways.com (accessed on 27 February 2022).
- Masucci, C.; Franchi, L.; Defraia, E.; Mucedero, M.; Cozza, P.; Baccetti, T. Stability of rapid maxillary expansion and facemask therapy: A long-term controlled study. Am. J. Orthod. Dentofac. Orthop. 2011, 140, 493–500. [Google Scholar] [CrossRef] [Green Version]
- D’Ettorre, G.; Farronato, M.; Candida, E.; Quinzi, V.; Grippaudo, C. A comparison between stereophotogrammetry and smartphone structured light technology for three-dimensional face scanning. Angle Orthod. 2022, 92, 358–363. [Google Scholar] [CrossRef]
- Liu, J.; Zhang, C.; Cai, R.; Yao, Y.; Zhao, Z.; Liao, W. Accuracy of 3-dimensional stereophotogrammetry: Comparison of the 3dMD and Bellus3D facial scanning systems with one another and with direct anthropometry. Am. J. Orthod. Dentofac. Orthop. 2021, 160, 862–871. [Google Scholar] [CrossRef] [PubMed]
- Ortensi, L.; Fisichella, M.L.; Ortensi, M.; Grande, F.; Pellegrino, G.; Ferri, A.; La Rosa, G.R.; Pedullà, E. A comparison of accuracy between three different facial detection systems for prosthodontic esthetic preview: A single-blinded in vitro study. Minerva Dent. Oral Sci. 2021. [Google Scholar] [CrossRef] [PubMed]
- Gallardo, Y.N.R.; Salazar-Gamarra, R.; Bohner, L.; De Oliveira, J.I.; Dib, L.L.; Sesma, N. Evaluation of the 3D error of 2 face-scanning systems: An in vitro analysis. J. Prosthet. Dent. 2021, S0022-3913(21)00368-1. [Google Scholar] [CrossRef] [PubMed]
- Sarul, M.; Nahajowski, M.; Gawin, G.; Antoszewska-Smith, J. Does daily wear time of Twin Block reliably predict its efficiency of class II treatment? J. Orofac. Orthop. 2022, 83, 195–204. [Google Scholar] [CrossRef] [PubMed]
- Sarul, M.; Antoszewska-Smith, J.; Park, H.S. Self-perception of smile attractiveness as a reliable predictor of increased patient compliance with an orthodontist. Adv. Clin. Exp. Med. 2019, 28, 1633–1638. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://formlabs-media.formlabs.com/datasheets/2001432-TDS-ENUS-0.pdf (accessed on 27 February 2022).
- Available online: https://silipos.com/products/gel-squares/ (accessed on 27 February 2022).
- Mangal, U.; Seo, J.Y.; Yu, J.; Kwon, J.S.; Choi, S.H. Incorporating aminated nanodiamonds to improve the mechanical properties of 3D-Printed resin-based biomedical Appliances. Nanomaterials 2020, 10, 827. [Google Scholar] [CrossRef]
- Han, X.; Yang, D.; Yang, C.; Spintzyk, S.; Scheideler, L.; Li, P.; Li, D.; Geis-Gerstorfer, J.; Rupp, F. Carbon fiber reinforced PEEK composites based on 3D-Printing technology for orthopedic and dental applications. J. Clin. Med. 2019, 12, 240. [Google Scholar] [CrossRef] [Green Version]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Normal Values | Pretreatment | Posttreatment |
|---|---|---|---|
| Angular degrees | |||
| SNA | 82 | 87.7 | 89.6 |
| SNB | 80 | 85.3 | 83.5 |
| ANB | 2 | 2.5 | 6.2 |
| SN to Palatal Plane | 8 | 9.6 | 9.6 |
| SN to Mand. Plane | 32 | 33.3 | 33.5 |
| Co-Go-Me | 125 | 136.1 | 130 |
| Upper Inc. to Palatal Pl | 110 | 119 | 113.6 |
| Lower Inc. to Mand. Pl. | 90 | 87.5 | 91.8 |
| Linear, mm | |||
| Wits | 0 | −6.3 | −3.1 |
| Overjet | 2.5 | 0.4 | 2.7 |
| Overbite | 2.5 | 1.1 | 3.6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Franchi, L.; Vichi, A.; Marti, P.; Lampus, F.; Guercio, S.; Recupero, A.; Giuntini, V.; Goracci, C. 3D Printed Customized Facemask for Maxillary Protraction in the Early Treatment of a Class III Malocclusion: Proof-of-Concept Clinical Case. Materials 2022, 15, 3747. https://0-doi-org.brum.beds.ac.uk/10.3390/ma15113747
Franchi L, Vichi A, Marti P, Lampus F, Guercio S, Recupero A, Giuntini V, Goracci C. 3D Printed Customized Facemask for Maxillary Protraction in the Early Treatment of a Class III Malocclusion: Proof-of-Concept Clinical Case. Materials. 2022; 15(11):3747. https://0-doi-org.brum.beds.ac.uk/10.3390/ma15113747
Chicago/Turabian StyleFranchi, Lorenzo, Alessandro Vichi, Patrizia Marti, Flavio Lampus, Simone Guercio, Annamaria Recupero, Veronica Giuntini, and Cecilia Goracci. 2022. "3D Printed Customized Facemask for Maxillary Protraction in the Early Treatment of a Class III Malocclusion: Proof-of-Concept Clinical Case" Materials 15, no. 11: 3747. https://0-doi-org.brum.beds.ac.uk/10.3390/ma15113747