
Effectiveness of Two Different Fluoride-Based Agents in the Treatment of Dentin Hypersensitivity: A Prospective Clinical Trial


 ,
,  , ,
, ,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patient Selection
2.3. Criteria of Inclusion and Exclusion
2.4. Diagnosis of DH
2.5. Group Division and Fluoride-Based Agent Application
2.6. Measurement of the DH Level
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Favaro Zeola, L.; Soares, P.V.; Cunha-Cruz, J. Prevalence of dentin hypersensitivity: Systematic review and meta-analysis. J. Dent. 2019, 81, 1–6. [Google Scholar] [CrossRef]
- Holland, G.R.; Narhi, M.N.; Addy, M.; Gangarosa, L.; Orchardson, R. Guidelines for the design and conduct of clinical trials on dentine hypersensitivity. J. Clin. Periodontol. 1997, 24, 808–813. [Google Scholar] [CrossRef]
- Gernhardt, C.R. How valid and applicable are current diagnostic criteria and assessment methods for dentin hypersensitivity? An overview. Clin. Oral Investig. 2013, 17, S31–S40. [Google Scholar] [CrossRef] [Green Version]
- Addy, M. Tooth brushing, tooth wear and dentine hypersensitivity—Are they associated? Int. Dent. J. 2005, 55, 261–267. [Google Scholar] [CrossRef]
- Teixeira, D.N.R.; Zeola, L.F.; Machado, A.C.; Gomes, R.R.; Souza, P.G.; Mendes, D.C.; Soares, P.V. Relationship between noncarious cervical lesions, cervical dentin hypersensitivity, gingival recession, and associated risk factors: A cross-sectional study. J. Dent. 2018, 76, 93–97. [Google Scholar] [CrossRef]
- Peumans, M.; Politano, G.; Van Meerbeek, B. Treatment of noncarious cervical lesions: When, why, and how. Int. J. Esthet. Dent. 2020, 15, 16–42. [Google Scholar]
- Wang, B. Cleaning, abrasion, and polishing effect of novel perlite toothpaste abrasive. J. Clin. Dent. 2013, 24, 88–93. [Google Scholar]
- Warreth, A.; Abuhijleh, E.; Almaghribi, M.A.; Mahwal, G.; Ashawish, A. Tooth surface loss: A review of literature. Saudi Dent. J. 2020, 32, 53–60. [Google Scholar] [CrossRef]
- Baker, P. Gingival Recession—Causes and Management. Prim. Dent. J. 2020, 8, 40–47. [Google Scholar] [CrossRef]
- Goh, L.; Er, J.; Pham, Y.; Abbott, P.V. An evaluation of the repeatability of electric pulp sensibility tests. Aust. Endod. J. 2021. [Google Scholar] [CrossRef] [PubMed]
- Rokaya, D.; Amornvit, P.; Skallevold, H.E.; Trinh, H.A.; Imran, E.; Al-Quraini, A.A.A.; Khurshid, Z. Materials for Teeth Bleaching. In Biomaterials in Endodontics; Woodhead Publishing: Sawston, UK, 2022; pp. 113–130. ISBN 9780128217467. [Google Scholar] [CrossRef]
- Irwin, C.R.; McCusker, P. Prevalence of dentine hypersensitivity in a general dental population. J. Ir. Dent. Assoc. 1997, 43, 7–9. [Google Scholar]
- Gillam, D.G.; Orchardson, R. Advances in the treatment of root dentine sensitivity: Mechanisms and treatment principles. Endod. Top. 2006, 13, 13–33. [Google Scholar] [CrossRef]
- Smith, W.A.; Marchan, S.; Rafeek, R.N. The prevalence and severity of non-carious cervical lesions in a group of patients attending a university hospital in Trinidad. J. Oral Rehabil. 2008, 35, 128–134. [Google Scholar] [CrossRef]
- Tammaro, S.; Wennström, J.L.; Bergenholtz, G. Root-dentin sensitivity following non-surgical periodontal treatment. J. Clin. Periodontol. 2000, 27, 690–697. [Google Scholar] [CrossRef]
- Gillam, D.G.; Seo, H.S.; Bulman, J.S.; Newman, H.N. Perceptions of dentine hypersensitivity in a general practice population. J. Oral Rehabil. 1999, 26, 710–714. [Google Scholar] [CrossRef]
- Porto, I.C.; Andrade, A.K.; Montes, M.A. Diagnosis and treatment of dentinal hypersensitivity. J. Oral Sci. 2009, 51, 323–332. [Google Scholar] [CrossRef] [Green Version]
- Miglani, S.; Aggarwal, V.; Ahuja, B. Dentin hypersensitivity: Recent trends in management. J. Conserv. Dent. 2010, 13, 218–224. [Google Scholar] [CrossRef] [Green Version]
- Aranha, A.C.; Pimenta, L.A.; Marchi, G.M. Clinical evaluation of desensitizing treatments for cervical dentin hypersensitivity. Braz. Oral Res. 2009, 23, 333–339. [Google Scholar] [CrossRef] [Green Version]
- Chu, C.H.; Lo, E.C.M. Dentin hypersensitivity: A review. Hong Kong Dent. J. 2010, 7, 15–22. [Google Scholar]
- Cummins, D. Recent advances in dentin hypersensitivity: Clinically proven treatments for instant and lasting sensitivity relief. Am. J. Dent. 2010, 23, 3A–13A. [Google Scholar]
- Brannström, M.; Aström, A. A study on the mechanism of pain elicited from the dentin. J. Dent. Res. 1964, 43, 619–625. [Google Scholar] [CrossRef]
- Drisko, C.H. Dentine hypersensitivity—Dental hygiene and periodontal considerations. Int. Dent. J. 2002, 52, 385–393. [Google Scholar] [CrossRef]
- Fiorillo, L.; Cervino, G.; Herford, A.S.; Laino, L.; Cicciù, M. Stannous Fluoride Effects on Enamel: A Systematic Review. Biomimetics 2020, 5, 41. [Google Scholar] [CrossRef]
- Meto, A.; Colombari, B.; Odorici, A.; Giva, L.B.; Pericolini, E.; Regina, A.L.; Blasi, E. Antibacterial Effects of MicroRepair®BIOMA-Based Toothpaste and Chewing Gum on Orthodontic Elastics Contaminated In Vitro with Saliva from Healthy Donors: A Pilot Study. Appl. Sci. 2020, 10, 6721. [Google Scholar] [CrossRef]
- Gandolfi, M.G.; Silvia, F.H.P.D.; Gasparotto, G.; Carlo, P. Calcium silicate coating derived from Portland cement as treatment for hypersensitive dentine. J. Dent. 2008, 36, 565–578. [Google Scholar] [CrossRef]
- Dhillon, S.N.; Deshpande, A.N.; Macwan, C.; Patel, K.S.; Shah, Y.S.; Jain, A.A. Comparative Evaluation of Microhardness and Enamel Solubility of Treated Surface Enamel with Resin Infiltrant, Fluoride Varnish, and Casein Phosphopeptide-amorphous Calcium Phosphate: An In Vitro Study. Int. J. Clin. Pediatr. Dent. 2020, 13, S14–S25. [Google Scholar] [CrossRef]
- Shiau, H. Dentin hypersensitivity. J. Evid. Based Dent. Pract. 2012, 12, 220–228. [Google Scholar] [CrossRef]
- Tirapelli, C.; Panzeri, H.; Lara, E.H.; Soares, R.G.; Peitl, O.; Zanotto, E.D. The effect of a novel crystallised bioactive glass-ceramic powder on dentine hypersensitivity: A long-term clinical study. J. Oral Rehabil. 2011, 38, 253–262. [Google Scholar] [CrossRef]
- Skallevold, H.E.; Rokaya, D.; Khurshid, Z.; Zafar, M.S. Bioactive Glass Applications in Dentistry. Int. J. Mol. Sci. 2019, 20, 5960. [Google Scholar] [CrossRef] [Green Version]
- Tellez, M.; Gomez, J.; Kaur, S.; Pretty, I.A.; Ellwood, R.; Ismail, A.I. Non-surgical management methods of noncavitated carious lesions. Community Dent. Oral Epidemiol. 2013, 41, 79–96. [Google Scholar] [CrossRef]
- Shahmoradi, M.; Hunter, N.; Swain, M. Efficacy of fluoride varnishes with added calcium phosphate in the protection of the structural and mechanical properties of enamel. Biomed. Res. Int. 2017, 2017, 7834905. [Google Scholar] [CrossRef] [Green Version]
- Ogard, B.; Seppä, L.; Rølla, G. Professional topical fluoride applications—Clinical efficacy and mechanism of action. Adv. Dent. Res. 1994, 8, 190–201. [Google Scholar] [CrossRef]
- Chersoni, S.; Bertacci, A.; Pashley, D.H.; Tay, F.R.; Montebugnoli, L.; Prati, C. In vivo effects of fluoride on enamel permeability. Clin. Oral Investig. 2011, 15, 443–449. [Google Scholar] [CrossRef]
- Petersson, L.G. The role of fluoride in the preventive management of dentin hypersensitivity and root caries. Clin. Oral Investig. 2013, 17, 63–71. [Google Scholar] [CrossRef] [Green Version]
- Knappwost, A. Mineralische Schmelzversiegelung zur Kariesprophylaxe, ihre Grundlagen und Möglichkeiten. Dtsch. Zahnärztliche Ztg. 1978, 33, 192–195. [Google Scholar]
- Kanzow, P.; Wegehaupt, F.J.; Attin, T.; Wiegand, A. Etiology and pathogenesis of dental erosion. Quintessence Int. 2016, 47, 275–278. [Google Scholar] [CrossRef]
- Addy, M. Dentine hypersensitivity: New perspectives on an old problem. Int. Dent. J. 2002, 52, 367–375. [Google Scholar] [CrossRef]
- Canadian Advisory Board on dentin hypersensitivity. Consensus-based recommendations for the diagnosis and management of dentin hypersensitivity. J. Can. Dent. Assoc. 2003, 69, 221–226. [Google Scholar]
- Toledano-Osorio, M.; Osorio, E.; Aguilera, F.S.; Luis Medina-Castillo, A.; Toledano, M.; Osorio, R. Improved reactive nanoparticles to treat dentin hypersensitivity. Acta Biomater. 2018, 72, 371–380. [Google Scholar] [CrossRef]
- Rees, J.S.; Addy, M. A cross-sectional study of dentine hypersensitivity. J. Clin. Periodontol. 2002, 29, 997–1003. [Google Scholar] [CrossRef]
- West, N.X. Dentine hypersensitivity: Preventive and therapeutic approaches to treatment. Periodontol. 2000 2008, 48, 31–41. [Google Scholar] [CrossRef]
- Godoi, F.A.; Carlos, N.R.; Bridi, E.C.; Amaral, F.L.B.D.; França, F.M.G.; Turssi, C.P.; Kantovitz, K.R.; Basting, R.T. Remineralizing effect of commercial fluoride varnishes on artificial enamel lesions. Braz. Oral Res. 2019, 33, e044. [Google Scholar] [CrossRef] [Green Version]
- Manarelli, M.M.; Delbem, A.C.; Lima, T.M.; Castilho, F.C.; Pessan, J.P. In vitro remineralizing effect of fluoride varnishes containing sodium trimetaphosphate. Caries Res. 2014, 48, 299–305. [Google Scholar] [CrossRef]
- Lagerweij, M.D.; Buchalla, W.; Kohnke, S.; Becker, K.; Lennon, A.M.; Attin, T. Prevention of erosion and abrasion by a high fluoride concentration gel applied at high frequencies. Caries Res. 2006, 40, 148–153. [Google Scholar] [CrossRef]
- Roberson, T.; Heymann, H.O.; Swift, E.J., Jr. Sturdevant’s Art and Science of Operative Dentistry, 5th ed.; Mosby Elsevier: Edinburgh, UK, 2006; pp. 6–10. [Google Scholar]
- Curro, F.A. Tooth hypersensitivity in spectrum of pain. Dent. Clin. N. Am. 1990, 34, 429–437. [Google Scholar]
- Abou, T. Zahnhalshypersensibiliat: Tiefenfluoridierung mittels Scmelzversiegelugsliquid. Zahnarztl. Prax. 1984, 11, 12–14. [Google Scholar]
- Buchalla, W.; Wiegand, A.; Lennon, Á.M.; Trage, K.; Becker, K.; Attin, T. Fluoridaufnahme in demineralisierten Schmelz nach Fluoridierung und Fluoridfällung. Dtsch. Zahnarztl. Z. 2007, 62, 301–307. [Google Scholar]



{kind=link}
{kind=link}
| Material Description | Manufacturer | Trade Name | Chemical Composition (Ingredients) |
|---|---|---|---|
| Calcium-fluoride-forming solution | Humanchemie GmbH, Alfeld, Germany | Tiefenfluorid® | 1st solution: magnesia fluoro silicate (F18Mg16Na10O66Si27), copper (II) fluoro-silicate (CuF6Si), sodium fluoride (NaF) as stabilizer, distilled water 2nd solution: calcium hydroxide (Ca(OH)2)—highly dispersed, methylcellulose (C6H7O2(OH)x(OCH3)y), distilled water |
| Fluoride varnish | Ultradent Inc., Cologne, Germany | EnamelastTM | flavored, xylitol-sweetened, 5% NaF (22,600 ppm F−) resin |
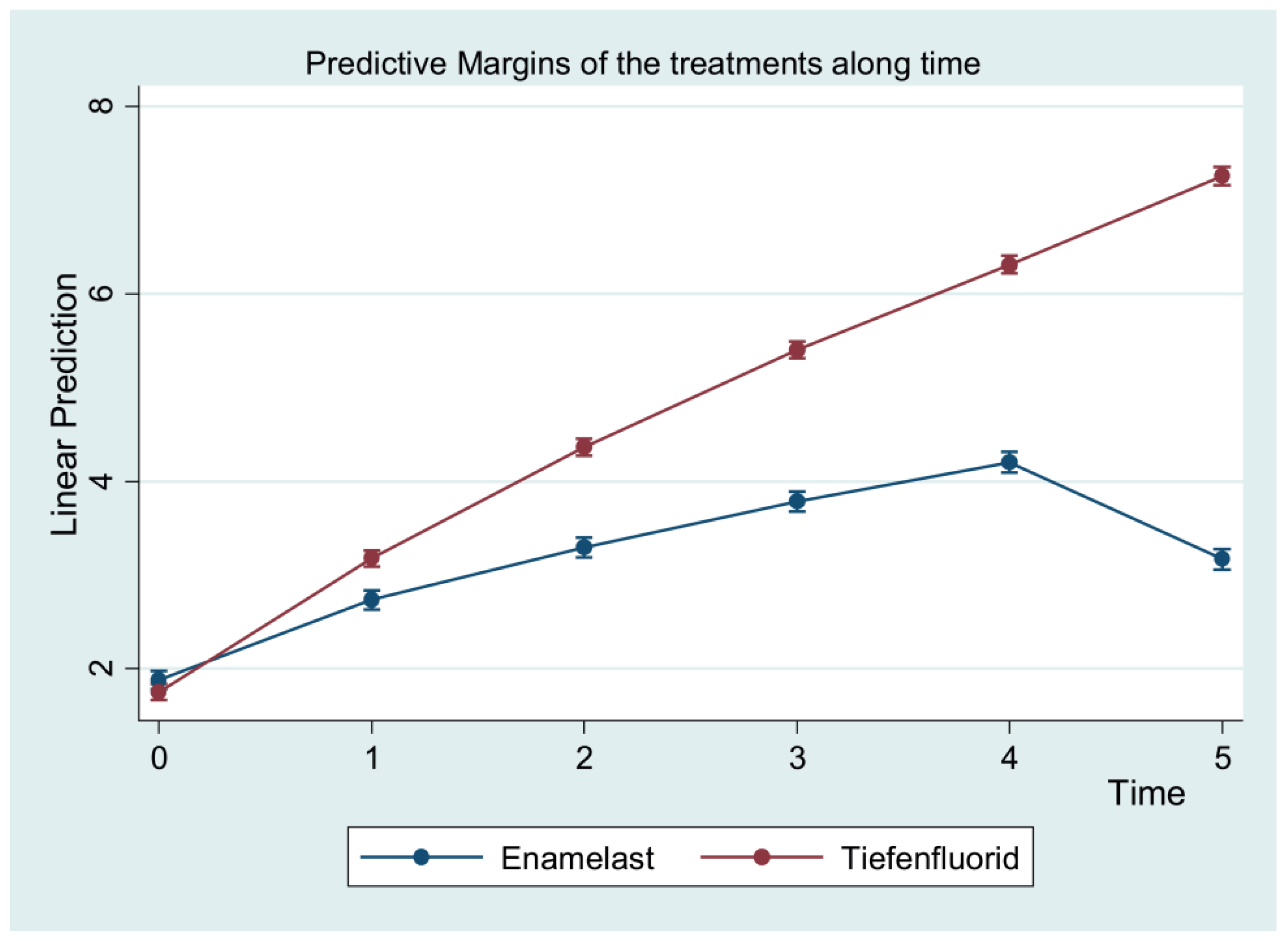
| Time-Point | Treatment Group | Control Group | ||
|---|---|---|---|---|
| Mean | SD | Mean | SD | |
| Before treatment | 1.75 | 0.72 | 1.88 | 0.63 |
| 7 days | 3.17 | 0.62 | 2.74 | 0.63 |
| 14 days | 4.36 | 0.54 | 3.30 | 0.67 |
| 1 month | 5.4 | 0.58 | 3.79 | 0.73 |
| 3 months | 6.31 | 0.73 | 4.21 | 0.81 |
| 6 months | 7.25 | 0.81 | 3.17 | 0.50 |
| Variable | Coefficient | Standard Error | z | p | 95% Confidence Interval | |
|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | |||||
| Treatment | 0.81 | 0.17 | 4.77 ** | <0.001 | 0.48 | 1.15 |
| Enamelast* hard tissue erosion | 0.18 | 0.13 | 1.32 | 0.189 | −0.09 | 0.44 |
| Enamelast* cuneiform defect | 0.17 | 0.14 | 1.22 | 0.222 | −0.11 | 0.45 |
| Enamelast* pathological abrasion | 0.11 | 0.15 | 0.70 | 0.481 | −0.19 | 0.40 |
| Tiefenfluorid* gingival recession | −0.15 | 0.13 | −1.21 | 0.225 | −0.40 | 0.09 |
| Tiefenfluorid* hard tissue erosion | −0.05 | 0.12 | −0.40 | 0.690 | −0.29 | 0.19 |
| Tiefenfluorid* cuneiform defect | 0.06 | 0.13 | 0.44 | 0.662 | −0.20 | 0.31 |
| Enamelast* 7 days | −0.09 | 0.03 | −2.72 ** | 0.007 | −0.15 | −0.02 |
| Enamelast* 14 days | −0.47 | 0.05 | −9.53 ** | <0.001 | −0.57 | −0.38 |
| Enamelast* 1 month | −0.93 | 0.07 | −13.33 ** | <0.001 | −1.06 | −0.79 |
| Enamelast* 3 months | −1.45 | 0.09 | −16.11 ** | <0.001 | −1.63 | −1.28 |
| Enamelast* 6 months | −3.43 | 0.11 | −30.84 ** | <0.001 | −3.65 | −3.22 |
| Tiefenfluorid* before treatment | −0.78 | 0.10 | −8.12 ** | <0.001 | −1.00 | −0.60 |
| Tiefenfluorid* 7 days | −0.30 | 0.08 | −4.00 ** | <0.001 | −0.45 | −0.15 |
| Tiefenfluorid* 14 days | −0.06 | 0.06 | −1.08 | 0.281 | −0.17 | 0.049 |
| Tiefenfluorid* 1 month | 0.03 | 0.04 | 0.90 | 0.367 | −0.04 | 0.10 |
| Variables | Contrast | SE | z | p | 95% Confidence Intervals | |
|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | |||||
| Tiefenfluorid vs. Enamelast before treatment | −0.13 | 0.07 | −1.92 | 0.055 | −0.26 | 0.00 |
| after 7 days | 0.44 ** | 0.07 | 6.45 | <0.001 | 0.31 | 0.57 |
| after 14 days | 1.07 ** | 0.07 | 15.39 | <0.001 | 0.93 | 1.21 |
| after 1 month | 1.62 ** | 0.07 | 22.71 | <0.001 | 1.48 | 1.76 |
| after 3 months | 2.11 ** | 0.07 | 28.86 | <0.001 | 1.97 | 2.25 |
| after 6 months | 4.09 ** | 0.07 | 54.28 | <0.001 | 3.94 | 4.24 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qeli, E.; Toti, Ç.; Odorici, A.; Blasi, E.; Tragaj, E.; Tepedino, M.; Masedu, F.; Kaçani, G.; Hysi, D.; Meto, A.; et al. Effectiveness of Two Different Fluoride-Based Agents in the Treatment of Dentin Hypersensitivity: A Prospective Clinical Trial. Materials 2022, 15, 1266. https://0-doi-org.brum.beds.ac.uk/10.3390/ma15031266
Qeli E, Toti Ç, Odorici A, Blasi E, Tragaj E, Tepedino M, Masedu F, Kaçani G, Hysi D, Meto A, et al. Effectiveness of Two Different Fluoride-Based Agents in the Treatment of Dentin Hypersensitivity: A Prospective Clinical Trial. Materials. 2022; 15(3):1266. https://0-doi-org.brum.beds.ac.uk/10.3390/ma15031266
Chicago/Turabian StyleQeli, Etleva, Çeljana Toti, Alessandra Odorici, Elisabetta Blasi, Emiljano Tragaj, Michele Tepedino, Francesco Masedu, Gerta Kaçani, Dorjan Hysi, Agron Meto, and et al. 2022. "Effectiveness of Two Different Fluoride-Based Agents in the Treatment of Dentin Hypersensitivity: A Prospective Clinical Trial" Materials 15, no. 3: 1266. https://0-doi-org.brum.beds.ac.uk/10.3390/ma15031266