Cervical Cancer Screening Programs in Europe: The Transition Towards HPV Vaccination and Population-Based HPV Testing



Abstract
:1. Introduction
2. Methodologies for Cervical Cancer Screening
2.1. Cervical Cytology
2.1.1. Conventional Pap Test and Its Alternatives
2.1.2. Liquid-Based Cytology
2.1.3. Visual Inspection by Acetic Acid and Visual Inspection with Lugol’s Iodine
2.2. HPV Testing
2.2.1. Advantages and Limitations
2.2.2. Clinical Validation of HPV Tests
3. Primary Cervical Cancer Prevention by HPV Vaccination
3.1. HPV Vaccines
3.2. Improving HPV Vaccination Coverage
4. Cervical Cancer Screening Programs
4.1. Organization of Screening
4.2. Primary Screening Tests and Specifications
4.2.1. Primary Cytology Testing
4.2.2. Primary HPV Testing
4.2.3. Primary HPV Cotesting
4.3. Management of Women after Primary Screening
4.3.1. Management of Women after a Positive HPV Primary Test Result
4.3.2. Management of Women after a Positive HPV Primary Test Result and Negative Cytology Triage Results
4.3.3. Post-Treatment Follow-up
5. The Current Landscape of Cervical Cancer Screening in the E.U. and Some E.U.-Associated Countries
5.1. The Implementation Status of Organized Population-Based Programs for Cervical Cancer Screening
5.2. The Implementation Status of Primary HPV Testing
5.3. The Importance of Coverage and Acceptance of Cervical Cancer Screening Programs
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef] [PubMed]
- Bruni, L.; Albero, G.; Serrano, B.; Mena, M.; Gómez, D.; Muñoz, J.; Bosch, F.X.; de Sanjosé, S.; ICO/IARC Information Centre on HPV and Cancer (HPV Information Centre). Human Papillomavirus and Related Diseases Report in EUROPE. Summary Report. Available online: http://www.hpvcentre.net/statistics/reports/XEX.pdf (accessed on 15 February 2018).
- Shingleton, H.M.; Patrick, R.L.; Johnston, W.W.; Smith, R.A. The current status of the Papanicolaou smear. CA Cancer J. Clin. 1995, 45, 305–320. [Google Scholar] [CrossRef] [PubMed]
- Petry, K.U. HPV and cervical cancer. Scand. J. Clin. Lab. Investig. 2014, 74, 59–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koh, W.-J.; Greer, B.E.; Abu-Rustum, N.R.; Apte, S.M.; Campos, S.M.; Cho, K.R.; Chu, C.; Cohn, D.; Crispens, M.A.; Dorigo, O.; et al. Cervical Cancer, Version 2.2015. J. Natl. Compr. Cancer Netw. 2015, 13, 395–404. [Google Scholar] [CrossRef]
- Elfström, K.M.; Arnheim-Dahlström, L.; von Karsa, L.; Dillner, J. Cervical cancer screening in Europe: Quality assurance and organisation of programmes. Eur. J. Cancer 2015, 51, 950–968. [Google Scholar] [CrossRef] [PubMed]
- Ferlay, J.; Steliarova-Foucher, E.; Lortet-Tieulent, J.; Rosso, S.; Coebergh, J.W.W.; Comber, H.; Forman, D.; Bray, F. Cancer incidence and mortality patterns in Europe: Estimates for 40 countries in 2012. Eur. J. Cancer 2013, 49, 1374–1403. [Google Scholar] [CrossRef] [Green Version]
- Bray, F.; Ren, J.-S.; Masuyer, E.; Ferlay, J. Global estimates of cancer prevalence for 27 sites in the adult population in 2008. Int. J. Cancer 2013, 132, 1133–1145. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Loos, A.H.; McCarron, P.; Weiderpass, E.; Arbyn, M.; Møller, H.; Hakama, M.; Parkin, D.M. Trends in Cervical Squamous Cell Carcinoma Incidence in 13 European Countries: Changing Risk and the Effects of Screening. Cancer Epidemiol. Biomarkers Prev. 2005, 14, 677–686. [Google Scholar] [CrossRef] [Green Version]
- Dürst, M.; Gissmann, L.; Ikenberg, H.; zur Hausen, H. A papillomavirus DNA from a cervical carcinoma and its prevalence in cancer biopsy samples from different geographic regions. Proc. Natl. Acad. Sci. USA 1983, 80, 3812–3815. [Google Scholar] [CrossRef]
- Cox, J.T. History of the use of HPV testing in cervical screening and in the management of abnormal cervical screening results. J. Clin. Virol. 2009, 45, S3–S12. [Google Scholar] [CrossRef]
- Walboomers, J.M.M.; Jacobs, M.V.; Manos, M.M.; Bosch, F.X.; Kummer, J.A.; Shah, K.V.; Snijders, P.J.F.; Peto, J.; Meijer, C.J.L.M.; Muñoz, N. Human papillomavirus is a necessary cause of invasive cervical cancer worldwide. J. Pathol. 1999, 189, 12–19. [Google Scholar] [CrossRef]
- Clifford, G.M.; Smith, J.S.; Plummer, M.; Muñoz, N.; Franceschi, S. Human papillomavirus types in invasive cervical cancer worldwide: A meta-analysis. Br. J. Cancer 2003, 88, 63–73. [Google Scholar] [CrossRef] [PubMed]
- Mühr, L.S.A.; Eklund, C.; Dillner, J. Towards quality and order in human papillomavirus research. Virology 2018, 519, 74–76. [Google Scholar] [CrossRef] [PubMed]
- Lyu, Z.; Feng, X.; Li, N.; Zhao, W.; Wei, L.; Chen, Y.; Yang, W.; Ma, H.; Yao, B.; Zhang, K.; et al. Human papillomavirus in semen and the risk for male infertility: A systematic review and meta-analysis. BMC Infect. Dis. 2017, 17, 714. [Google Scholar] [CrossRef] [PubMed]
- Chabeda, A.; Yanez, R.J.R.; Lamprecht, R.; Meyers, A.E.; Rybicki, E.P.; Hitzeroth, I.I. Therapeutic vaccines for high-risk HPV-associated diseases. Papillomavirus Res. 2018, 5, 46–58. [Google Scholar] [CrossRef]
- Tommasino, M. The human papillomavirus family and its role in carcinogenesis. Semin. Cancer Biol. 2014, 26, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Moscicki, A.-B.; Schiffman, M.; Kjaer, S.; Villa, L.L. Chapter 5: Updating the natural history of HPV and anogenital cancer. Vaccine 2006, 24, S42–S51. [Google Scholar] [CrossRef]
- Berman, T.A.; Schiller, J.T. Human papillomavirus in cervical cancer and oropharyngeal cancer: One cause, two diseases. Cancer 2017, 123, 2219–2229. [Google Scholar] [CrossRef]
- Ermel, A.; Shew, M.L.; Imburgia, T.M.; Brown, M.; Qadadri, B.; Tong, Y.; Brown, D.R. Redetection of human papillomavirus type 16 infections of the cervix in mid-adult life. Papillomavirus Res. 2018, 5, 75–79. [Google Scholar] [CrossRef]
- Ostör, A.G. Natural history of cervical intraepithelial neoplasia: A critical review. Int. J. Gynecol. Pathol. 1993, 12, 186–192. [Google Scholar] [CrossRef]
- De Villiers, E.-M. Cross-roads in the classification of papillomaviruses. Virology 2013, 445, 2–10. [Google Scholar] [CrossRef] [PubMed]
- Xi, L.F.; Schiffman, M.; Koutsky, L.A.; Hughes, J.P.; Hulbert, A.; Shen, Z.; Galloway, D.A.; Kiviat, N.B. Variant-specific persistence of infections with human papillomavirus Types 31, 33, 45, 56 and 58 and risk of cervical intraepithelial neoplasia. Int. J. Cancer 2016, 139, 1098–1105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halec, G.; Alemany, L.; Lloveras, B.; Schmitt, M.; Alejo, M.; Bosch, F.X.; Tous, S.; Klaustermeier, J.E.; Guimerà, N.; Grabe, N.; et al. Pathogenic role of the eight probably/possibly carcinogenic HPV types 26, 53, 66, 67, 68, 70, 73 and 82 in cervical cancer. J. Pathol. 2014, 234, 441–451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muñoz, N.; Bosch, F.X.; de Sanjosé, S.; Herrero, R.; Castellsagué, X.; Shah, K.V.; Snijders, P.J.F.; Meijer, C.J.L.M. Epidemiologic Classification of Human Papillomavirus Types Associated with Cervical Cancer. N. Engl. J. Med. 2003, 348, 518–527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, J.S.; Lindsay, L.; Hoots, B.; Keys, J.; Franceschi, S.; Winer, R.; Clifford, G.M. Human papillomavirus type distribution in invasive cervical cancer and high-grade cervical lesions: A meta-analysis update. Int. J. Cancer 2007, 121, 621–632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Breitenecker, G. Zervixkarzinom-Screening. Der Pathologe 2009, 30, 128. [Google Scholar] [CrossRef]
- Diamantis, A.; Magiorkinis, E. Pioneers of exfoliative cytology in the 19th century: The predecessors of George Papanicolaou. Cytopathology 2014, 25, 215–224. [Google Scholar] [CrossRef] [PubMed]
- Tan, S.Y.; Tatsumura, Y. George Papanicolaou (1883–1962): Discoverer of the Pap smear. Singap. Med. J. 2015, 56, 586–587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chantziantoniou, N.; Donnelly, A.D.; Mukherjee, M.; Boon, M.E.; Austin, R.M. Inception and Development of the Papanicolaou Stain Method. Acta Cytol. 2017, 61, 266–280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papanicolaou, G.N.; Traut, H.F. The Diagnostic Value of Vaginal Smears in Carcinoma of the Uterus. Am. J. Obstet. Gynecol. 1941, 42, 193–206. [Google Scholar] [CrossRef]
- Dighe, S.B.; Ajit, D.; Pathuthara, S.; Chinoy, R. Papanicolaou Stain. Acta Cytol. 2006, 50, 643–646. [Google Scholar] [CrossRef] [PubMed]
- Siebers, A.G.; Klinkhamer, P.J.; Grefte, J.M.; Massuger, L.F.; Vedder, J.E.; Beijers-Broos, A.; Bulten, J.; Arbyn, M. Comparison of liquid-based cytology with conventional cytology for detection of cervical cancer precursors: A randomized controlled trial. JAMA 2009, 302, 1757–1764. [Google Scholar] [CrossRef] [PubMed]
- Gibb, R.K.; Martens, M.G. The Impact of Liquid-Based Cytology in Decreasing the Incidence of Cervical Cancer. Rev. Obstet. Gynecol. 2011, 4, S2–S11. [Google Scholar] [PubMed]
- Prasaad, P.R. Short-duration Papanicolaou stain (SPS)—An alternative to conventional Papanicolaou stain in routine cytopathology? Comp. Clin. Pathol. 2017, 26, 1285–1288. [Google Scholar] [CrossRef]
- Yang, G.C.; Alvarez, I.I. Ultrafast Papanicolaou stain. An alternative preparation for fine needle aspiration cytology. Acta Cytol. 1995, 39, 55–60. [Google Scholar] [PubMed]
- Gill, G.W. Enviro-Pap: An Environmentally Friendly, Economical, and Effective Pap Stain. Lab. Med. 2006, 37, 105–108. [Google Scholar] [CrossRef] [Green Version]
- Thakur, M.; Guttikonda, V.R. Modified ultrafast Papanicolaou staining technique: A comparative study. J. Cytol. 2017, 34, 149–153. [Google Scholar] [CrossRef]
- Izhar, S.; Kaur, R.; Masih, K. Efficacy of rapid, economical, acetic acid, Papanicolaou stain in cervical smears as an alternative to conventional Papanicolaou stain. J. Cytol./Indian Acad. Cytol. 2014, 31, 154–157. [Google Scholar] [CrossRef]
- Lyng, F.M.; Traynor, D.; Ramos, I.R.M.; Bonnier, F.; Byrne, H.J. Raman spectroscopy for screening and diagnosis of cervical cancer. Anal. Bioanal. Chem. 2015, 407, 8279–8289. [Google Scholar] [CrossRef] [Green Version]
- Strander, B.; Andersson-Ellström, A.; Milsom, I.; Rådberg, T.; Ryd, W. Liquid-based cytology versus conventional Papanicolaou smear in an organized screening program. Cancer Cytopathol. 2007, 111, 285–291. [Google Scholar] [CrossRef] [Green Version]
- Sakamoto, H.; Takenaka, M.; Ushimaru, K.; Tanaka, T. Use of Liquid-Based Cytology (LBC) and Cell Blocks from Cell Remnants for Cytologic, Immunohistochemical, and Immunocytochemical Diagnosis of Malignancy. Open J. Pathol. 2012, 2, 58–65. [Google Scholar] [CrossRef]
- Moseley, R.P.; Paget, S. Liquid-based cytology: Is this the way forward for cervical screening? Cytopathology 2002, 13, 71–82. [Google Scholar] [CrossRef] [PubMed]
- Davey, E.; Barratt, A.; Irwig, L.; Chan, S.F.; Macaskill, P.; Mannes, P.; Saville, A.M. Effect of study design and quality on unsatisfactory rates, cytology classifications, and accuracy in liquid-based versus conventional cervical cytology: A systematic review. Lancet 2006, 367, 122–132. [Google Scholar] [CrossRef]
- Jeong, H.; Hong, S.R.; Chae, S.-W.; Jin, S.-Y.; Yoon, H.K.; Lee, J.; Kim, E.K.; Ha, S.T.; Kim, S.N.; Park, E.-J.; et al. Comparison of Unsatisfactory Samples from Conventional Smear versus Liquid-Based Cytology in Uterine Cervical Cancer Screening Test. J. Pathol. Transl. Med. 2017, 51, 314–319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, V.; Gupta, N.; Nijhawan, R.; Srinivasan, R.; Suri, V.; Rajwanshi, A. Liquid-based cytology versus conventional cytology for evaluation of cervical Pap smears: Experience from the first 1000 split samples. Indian J. Pathol. Microbiol. 2015, 58, 17–21. [Google Scholar] [CrossRef] [PubMed]
- Basu, P.; Mittal, S.; Bhadra Vale, D.; Chami Kharaji, Y. Secondary prevention of cervical cancer. Best Pract. Res. Clin. Obstet. Gynaecol. 2018, 47, 73–85. [Google Scholar] [CrossRef] [PubMed]
- Huchko, M.J.; Sneden, J.; Zakaras, J.M.; Smith-McCune, K.; Sawaya, G.; Maloba, M.; Bukusi, E.A.; Cohen, C.R. A Randomized Trial Comparing the Diagnostic Accuracy of Visual Inspection with Acetic Acid to Visual Inspection with Lugol’s Iodine for Cervical Cancer Screening in HIV-Infected Women. PLoS ONE 2015, 10, e0118568. [Google Scholar] [CrossRef] [PubMed]
- Belinson, J.; Pretorius, R.; Zhang, W.; Wu, L.; Qiao, Y.; Elson, P. Cervical cancer screening by simple visual inspection after acetic acid. Obstet. Gynecol. 2001, 98, 441–444. [Google Scholar] [PubMed]
- Soloman, D. The 1988 bethesda system for reporting cervical/vaginal cytologic diagnoses: Developed and approved at the National Cancer Institute workshop in Bethesda, Maryland, December 12–13, 1988. Hum. Pathol. 1990, 21, 704–708. [Google Scholar] [CrossRef]
- Nayar, R.; Wilbur, D.C. The Bethesda System for Reporting Cervical Cytology: Definitions, Criteria, and Explanatory Notes; Springer: New York, NY, USA, 2015. [Google Scholar] [CrossRef]
- Stoler, M.H.; Ronnett, B.M.; Joste, N.E.; Hunt, W.C.; Cuzick, J.; Wheeler, C.M.; New Mexico HPV Pap Registry Steering Committee. The Interpretive Variability of Cervical Biopsies and its Relationship to HPV status. Am. J. Surg. Pathol. 2015, 39, 729–736. [Google Scholar] [CrossRef] [PubMed]
- Arbyn, M.; Ronco, G.; Anttila, A.; Meijer, C.J.L.M.; Poljak, M.; Ogilvie, G.; Koliopoulos, G.; Naucler, P.; Sankaranarayanan, R.; Peto, J. Evidence Regarding Human Papillomavirus Testing in Secondary Prevention of Cervical Cancer. Vaccine 2012, 30, F88–F99. [Google Scholar] [CrossRef] [PubMed]
- Von Karsa, L.; Arbyn, M.; De Vuyst, H.; Dillner, J.; Dillner, L.; Franceschi, S.; Patnick, J.; Ronco, G.; Segnan, N.; Suonio, E.; et al. European guidelines for quality assurance in cervical cancer screening. Summary of the supplements on HPV screening and vaccination. Papillomavirus Res. 2015, 1, 22–31. [Google Scholar] [CrossRef] [Green Version]
- Von Karsa, L.; Arbyn, A.; De Vuyst, H.; Dillner, J.; Dillner, L.; Franceschi, S.; Patnick, J.; Ronco, G.; Segnan, N.; Suonio, E.; et al. Executive summary. In European Guidelines for Quality Assurance in Cervical Cancer Screening, 2nd ed.; Supplements; Office for Official Publications of the European Union: Luxembourg, 2015; pp. XIII–XXIV. [Google Scholar]
- Poljak, M.; Kocjan, B.J. Commercially available assays for multiplex detection of alpha human papillomaviruses. Expert Rev. Anti-infect. Ther. 2010, 8, 1139–1162. [Google Scholar] [CrossRef] [Green Version]
- Poljak, M.; Cuzick, J.; Kocjan, B.J.; Iftner, T.; Dillner, J.; Arbyn, M. Nucleic Acid Tests for the Detection of Alpha Human Papillomaviruses. Vaccine 2012, 30, F100–F106. [Google Scholar] [CrossRef] [PubMed]
- Poljak, M.; Kocjan, B.J.; Oštrbenk, A.; Seme, K. Commercially available molecular tests for human papillomaviruses (HPV): 2015 update. J. Clin. Virol. 2016, 76, S3–S13. [Google Scholar] [CrossRef]
- Arbyn, M.; Snijders, P.J.F.; Meijer, C.J.L.M.; Berkhof, J.; Cuschieri, K.; Kocjan, B.J.; Poljak, M. Which high-risk HPV assays fulfil criteria for use in primary cervical cancer screening? Clin. Microbiol. Infect. 2015, 21, 817–826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ronco, G.; Giorgi-Rossi, P.; Carozzi, F.; Confortini, M.; Palma, P.D.; Del Mistro, A.; Ghiringhello, B.; Girlando, S.; Gillio-Tos, A.; De Marco, L.; et al. Efficacy of human papillomavirus testing for the detection of invasive cervical cancers and cervical intraepithelial neoplasia: A randomised controlled trial. Lancet Oncol. 2010, 11, 249–257. [Google Scholar] [CrossRef]
- Meijer, C.; Berkhof, J.; Castle, P.E.; Hesselink, A.; Franco, E.L.; Ronco, G.; Arbyn, M.; Bosch, F.X.; Cuzick, J.; Dillner, J.; et al. Guidelines for human papillomavirus DNA test requirements for primary cervical cancer screening in women of 30 years and older. Int. J. Cancer 2009, 124, 516–520. [Google Scholar] [CrossRef] [PubMed]
- Arbyn, M.; Depuydt, C.; Benoy, I.; Bogers, J.; Cuschieri, K.; Schmitt, M.; Pawlita, M.; Geraets, D.; Heard, I.; Gheit, T.; et al. VALGENT: A protocol for clinical validation of human papillomavirus assays. J. Clin. Virol. 2016, 76, S14–S21. [Google Scholar] [CrossRef] [PubMed]
- Muñoz, N.; Kjaer, S.K.; Sigurdsson, K.; Iversen, O.-E.; Hernandez-Avila, M.; Wheeler, C.M.; Perez, G.; Brown, D.R.; Koutsky, L.A.; Tay, E.H.; et al. Impact of Human Papillomavirus (HPV)-6/11/16/18 Vaccine on All HPV-Associated Genital Diseases in Young Women. JNCI J. Natl. Cancer Inst. 2010, 102, 325–339. [Google Scholar] [CrossRef] [Green Version]
- Schülein, S.; Taylor, K.J.; König, J.; Claus, M.; Blettner, M.; Klug, S.J. Factors influencing uptake of HPV vaccination among girls in Germany. BMC Public Health 2016, 16, 995. [Google Scholar] [CrossRef] [PubMed]
- Dilley, S.; Miller, K.; Huh, W. HPV vaccination. Gynecol. Oncol. 2018, 148, 3–4. [Google Scholar] [CrossRef] [PubMed]
- Braaten, K.P.; Laufer, M.R. Human Papillomavirus (HPV), HPV-Related Disease, and the HPV Vaccine. Rev. Obstet. Gynecol. 2008, 1, 2–10. [Google Scholar] [PubMed]
- Brotherton, J.M.L.; Bloem, P.N. Population-based HPV vaccination programmes are safe and effective: 2017 update and the impetus for achieving better global coverage. Best Pract. Res. Clin. Obstet. Gynaecol. 2017, 47, 42–58. [Google Scholar] [CrossRef]
- Higgins, L.M.; Dirksing, K.N.; Ding, L.; Morrow, C.D.; Widdice, L.A.; Kahn, J.A. Adolescents’ intention and self-efficacy to follow Pap testing recommendations after receiving the HPV vaccine. Hum. Vaccines Immunother. 2016, 12, 1498–1503. [Google Scholar] [CrossRef] [PubMed]
- Jacot-Guillarmod, M.; Pasquier, J.; Greub, G.; Bongiovanni, M.; Achtari, C.; Sahli, R. Impact of HPV vaccination with Gardasil® in Switzerland. BMC Infect. Dis. 2017, 17, 790. [Google Scholar] [CrossRef]
- Meites, E.; Kempe, A.; Markowitz, L.E. Use of a 2-Dose Schedule for Human Papillomavirus Vaccination—Updated Recommendations of the Advisory Committee on Immunization Practices. Am. J. Transplant. 2017, 17, 834–837. [Google Scholar] [CrossRef] [PubMed]
- Iversen, O.E.; Miranda, M.J.; Ulied, A.; Soerdal, T.; Lazarus, E.; Chokephaibulkit, K.; Block, S.L.; Skrivanek, A.; Nur Azurah, A.G.; Fong, S.M.; et al. Immunogenicity of the 9-valent hpv vaccine using 2-dose regimens in girls and boys vs a 3-dose regimen in women. JAMA 2016, 316, 2411–2421. [Google Scholar] [CrossRef]
- Jiang, R.T.; Wang, J.W.; Peng, S.; Huang, T.-C.; Wang, C.; Cannella, F.; Chang, Y.-N.; Viscidi, R.P.; Best, S.R.A.; Hung, C.-F.; et al. Spontaneous and Vaccine-Induced Clearance of Mus Musculus Papillomavirus 1 Infection. J. Virol. 2017, 91, e00699-17. [Google Scholar] [CrossRef]
- Romanowski, B.; Schwarz, T.F.; Ferguson, L.; Peters, K.; Dionne, M.; Behre, U.; Schulze, K.; Hillemanns, P.; Suryakiran, P.; Thomas, F.; et al. Sustained immunogenicity of the HPV-16/18 AS04-adjuvanted vaccine administered as a two-dose schedule in adolescent girls: Five-year clinical data and modeling predictions from a randomized study. Hum. Vaccines Immunother. 2016, 12, 20–29. [Google Scholar] [CrossRef]
- Stanley, M. HPV vaccination in boys and men. Hum. Vaccines Immunother. 2014, 10, 2109–2111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Audisio, R.A.; Icardi, G.; Isidori, A.M.; Liverani, C.A.; Lombardi, A.; Mariani, L.; Mennini, F.S.; Mitchell, D.A.; Peracino, A.; Pecorelli, S.; et al. Public health value of universal HPV vaccination. Crit. Rev. Oncol./Hematol. 2016, 97, 157–167. [Google Scholar] [CrossRef] [Green Version]
- Bosch, F.X.; Robles, C.; Díaz, M.; Arbyn, M.; Baussano, I.; Clavel, C.; Ronco, G.; Dillner, J.; Lehtinen, M.; Petry, K.-U.; et al. HPV-FASTER: Broadening the scope for prevention of HPV-related cancer. Nat. Rev. Clin. Oncol. 2015, 13, 119–132. [Google Scholar] [CrossRef]
- Nygård, M. Screening for cervical cancer: When theory meets reality. BMC Cancer 2011, 11, 240. [Google Scholar] [CrossRef] [PubMed]
- Wilson, J.M.G.; Jungner, G.; World Health Organization. Principles and Practice of Screening for Disease; World Health Organization: Geneva, Switzerland, 1968; Available online: http://www.who.int/iris/handle/10665/37650 (accessed on 19 July 2018).
- Coleman, D.; Day, N.; Douglas, G.; Farmery, E.; Lynge, E.; Philip, J.; Segnan, N. European Guidelines for Quality Assurance in Cervical Cancer Screening. Europe against cancer programme. Eur. J. Cancer 1993, 29, S1–S38. [Google Scholar]
- Arbyn, M.; Anttila, A.; Jordan, J.; Ronco, G.; Schenck, U.; Segnan, N.; Wiener, H.G.; Herbert, A.; Daniel, J.; von Karsa, L. (Eds.) European Guidelines for Quality Assurance in Cervical Cancer Screening, 2nd ed.; Office for Official Publications of the European Communities: Luxembourg, 2008; Available online: http://screening.iarc.fr/doc/ND7007117ENC_002.pdf (accessed on 21 May 2018).
- Arbyn, M.; Anttila, A.; Jordan, J.; Ronco, G.; Schenck, U.; Segnan, N.; Wiener, H.; Herbert, A.; von Karsa, L. European Guidelines for Quality Assurance in Cervical Cancer Screening. Second Edition—Summary Document. Ann. Oncol. 2010, 21, 448–458. [Google Scholar] [CrossRef]
- Hanselaar, A.G.J.M. Criteria for Organized Cervical Screening Programs. Acta Cytol. 2002, 46, 619–629. [Google Scholar] [CrossRef]
- Wentzensen, N.; Schiffman, M.; Palmer, T.; Arbyn, M. Triage of HPV positive women in cervical cancer screening. J. Clin. Virol. 2016, 76, S49–S55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franco, E.L.; Cuzick, J.; Hildesheim, A.; de Sanjosé, S. Chapter 20: Issues in planning cervical cancer screening in the era of HPV vaccination. Vaccine 2006, 24, S171–S177. [Google Scholar] [CrossRef]
- Toliman, P.J.; Kaldor, J.M.; Tabrizi, S.N.; Vallely, A.J. Innovative approaches to cervical cancer screening in low- and middle-income countries. Climacteric 2018, 21, 235–238. [Google Scholar] [CrossRef]
- Isidean, S.D.; Mayrand, M.H.; Ramanakumar, A.V.; Gilbert, L.; Reid, S.L.; Rodrigues, I.; Ferenczy, A.; Ratnam, S.; Coutlée, F.; Franco, E.L. Human papillomavirus testing versus cytology in primary cervical cancer screening: End-of-study and extended follow-up results from the Canadian cervical cancer screening trial. Int. J. Cancer 2016, 139, 2456–2466. [Google Scholar] [CrossRef] [PubMed]
- Wentzensen, N.; Arbyn, M. HPV-based cervical cancer screening- facts, fiction, and misperceptions. Prev. Med. 2017, 98, 33–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basu, P.; Meheus, F.; Chami, Y.; Hariprasad, R.; Zhao, F.; Sankaranarayanan, R. Management algorithms for cervical cancer screening and precancer treatment for resource-limited settings. Int. J. Gynecol. Obstet. 2017, 138, 26–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jin, X.W.; Lipold, L.; Foucher, J.; Sikon, A.; Brainard, J.; Belinson, J.; Schramm, S.; Nottingham, K.; Hu, B.; Rothberg, M.B. Cost-Effectiveness of Primary HPV Testing, Cytology and Co-testing as Cervical Cancer Screening for Women Above Age 30 Years. J. Gen. Intern. Med. 2016, 31, 1338–1344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kothari, A. The introduction of the HPV primary screening programme. Pract. Nurs. 2017, 28, 162–166. [Google Scholar] [CrossRef] [Green Version]
- Tota, J.E.; Bentley, J.; Blake, J.; Coutlée, F.; Duggan, M.A.; Ferenczy, A.; Franco, E.L.; Fung-Kee-Fung, M.; Gotlieb, W.; Mayrand, M.-H.; et al. Introduction of molecular HPV testing as the primary technology in cervical cancer screening: Acting on evidence to change the current paradigm. Prev. Med. 2017, 98, 5–14. [Google Scholar] [CrossRef] [PubMed]
- Georgalis, L.; de Sanjosé, S.; Esnaola, M.; Bosch, F.X.; Diaz, M. Present and future of cervical cancer prevention in Spain: A cost-effectiveness analysis. Eur. J. Cancer Prev. 2016, 25, 430–439. [Google Scholar] [CrossRef]
- De Thurah, L.; Bonde, J.; Lam, J.U.H.; Rebolj, M. Concordant testing results between various human papillomavirus assays in primary cervical cancer screening: Systematic review. Clin. Microbiol. Infect. 2018, 24, 29–36. [Google Scholar] [CrossRef]
- Isidean, S.D.; Mayrand, M.-H.; Ramanakumar, A.V.; Rodrigues, I.; Ferenczy, A.; Ratnam, S.; Coutlée, F.; Franco, E.L. Comparison of Triage Strategies for HPV-Positive Women: Canadian Cervical Cancer Screening Trial Results. Cancer Epidemiol. Biomarkers Prev. 2017, 26, 923–929. [Google Scholar] [CrossRef]
- Schlichte, M.J.; Guidry, J. Current Cervical Carcinoma Screening Guidelines. J. Clin. Med. 2015, 4, 918–932. [Google Scholar] [CrossRef] [Green Version]
- Castañón, A.; Landy, R.; Cuzick, J.; Sasieni, P. Cervical Screening at Age 50–64 Years and the Risk of Cervical Cancer at Age 65 Years and Older: Population-Based Case Control Study. PLoS Med. 2014, 11, e1001585. [Google Scholar] [CrossRef] [PubMed]
- Gyllensten, U.; Lindell, M.; Gustafsson, I.; Wilander, E. HPV test shows low sensitivity of Pap screen in older women. Lancet Oncol. 2010, 11, 509–510. [Google Scholar] [CrossRef]
- Hermansson, R.S.; Olovsson, M.; Hoxell, E.; Lindström, A.K. HPV prevalence and HPV-related dysplasia in elderly women. PLoS ONE 2018, 13, e0189300. [Google Scholar] [CrossRef]
- Naucler, P.; Ryd, W.; Törnberg, S.; Strand, A.; Wadell, G.; Elfgren, K.; Rådberg, T.; Strander, B.; Forslund, O.; Hansson, B.-G.; et al. Efficacy of HPV DNA Testing With Cytology Triage and/or Repeat HPV DNA Testing in Primary Cervical Cancer Screening. JNCI J. Natl. Cancer Inst. 2009, 101, 88–99. [Google Scholar] [CrossRef] [Green Version]
- Cuzick, J.; Wheeler, C. Need for expanded HPV genotyping for cervical screening. Papillomavirus Res. 2016, 2, 112–115. [Google Scholar] [CrossRef] [PubMed]
- Gustinucci, D.; Rossi, P.G.; Cesarini, E.; Broccolini, M.; Bulletti, S.; Carlani, A.; D’angelo, V.; D’amico, M.R.; Di Dato, E.; Galeazzi, P.; et al. Use of Cytology, E6/E7 mRNA, and p16INK4a–Ki-67 to Define the Management of Human Papillomavirus (HPV)–Positive Women in Cervical Cancer Screening. Am. J. Clin. Pathol. 2016, 145, 35–45. [Google Scholar] [CrossRef]
- Cuschieri, K.; Ronco, G.; Lorincz, A.; Smith, L.; Ogilvie, G.; Mirabello, L.; Carozzi, F.; Cubie, H.; Wentzensen, N.; Snijders, P.; et al. Eurogin roadmap 2017: Triage strategies for the management of HPV-positive women in cervical screening programs. Int. J. Cancer 2018, 143, 735–745. [Google Scholar] [CrossRef]
- Cuzick, J.; Szarewski, A.; Cubie, H.; Hulman, G.; Kitchener, H.; Luesley, D.; McGoogan, E.; Menon, U.; Terry, G.; Edwards, R.; et al. Management of women who test positive for high-risk types of human papillomavirus: The HART study. Lancet 2003, 362, 1871–1876. [Google Scholar] [CrossRef]
- Dijkstra, M.G.; van Niekerk, D.; Rijkaart, D.C.; van Kemenade, F.J.; Heideman, D.A.M.; Snijders, P.J.F.; Meijer, C.J.L.M.; Berkhof, J. Primary hrHPV DNA Testing in Cervical Cancer Screening: How to Manage Screen-Positive Women? A POBASCAM Trial Substudy. Cancer Epidemiol. Biomarkers Prev. 2014, 23, 55–63. [Google Scholar] [CrossRef]
- Ronco, G.; Dillner, J.; Elfström, K.M.; Tunesi, S.; Snijders, P.J.F.; Arbyn, M.; Kitchener, H.; Segnan, N.; Gilham, C.; Giorgi-Rossi, P.; et al. Efficacy of HPV-based screening for prevention of invasive cervical cancer: Follow-up of four European randomised controlled trials. Lancet 2014, 383, 524–532. [Google Scholar] [CrossRef]
- Ronco, G.; Giorgi Rossi, P. Role of HPV DNA testing in modern gynaecological practice. Best Pract. Res. Clin. Obstet. Gynaecol. 2018, 47, 107–118. [Google Scholar] [CrossRef] [PubMed]
- Polman, N.J.; Veldhuijzen, N.J.; Heideman, D.A.M.; Snijders, P.J.F.; Meijer, C.J.L.M.; Berkhof, J. HPV-positive women with normal cytology remain at increased risk of CIN3 after a negative repeat HPV test. Br. J. Cancer 2017, 117, 1557–1561. [Google Scholar] [CrossRef]
- Mariani, L.; Sandri, M.T.; Preti, M.; Origoni, M.; Costa, S.; Cristoforoni, P.; Bottari, F.; Sideri, M. HPV-Testing in Follow-up of Patients Treated for CIN2+ Lesions. J. Cancer 2016, 7, 107–114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Onuki, M.; Matsumoto, K.; Sakurai, M.; Ochi, H.; Minaguchi, T.; Satoh, T.; Yoshikawa, H. Posttreatment human papillomavirus testing for residual or recurrent high-grade cervical intraepithelial neoplasia: A pooled analysis. J. Gynecol. Oncol. 2016, 27, e3. [Google Scholar] [CrossRef] [PubMed]
- Cuschieri, K.; Bhatia, R.; Cruickshank, M.; Hillemanns, P.; Arbyn, M. HPV testing in the context of post-treatment follow up (test of cure). J. Clin. Virol. 2016, 76, S56–S61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ribaldone, R.; Boldorini, R.; Capuano, A.; Arrigoni, S.; Di Oto, A.; Surico, N. Role of HPV testing in the follow-up of women treated for cervical dysplasia. Arch. Gynecol. Obstet. 2010, 282, 193–197. [Google Scholar] [CrossRef] [PubMed]
- Jordan, J.; Martin-Hirsch, P.; Arbyn, M.; Schenck, U.; Baldauf, J.J.; Silva, D.D.; Anttila, A.; Nieminen, P.; Prendiville, W. European guidelines for clinical management of abnormal cervical cytology, Part 2. Cytopathology 2009, 20, 5–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costa, S.; Venturoli, S.; Origoni, M.; Preti, M.; Mariani, L.; Cristoforoni, P.; Sandri, M.T. Performance of HPV DNA testing in the follow-up after treatment of high-grade cervical lesions, adenocarcinoma in situ (AIS) and microinvasive carcinoma. Ecancermedicalscience 2015, 9, 528. [Google Scholar] [CrossRef]
- Asciutto, K.C.; Henic, E.; Darlin, L.; Forslund, O.; Borgfeldt, C. Follow up with HPV test and cytology as test of cure, 6 months after conization, is reliable. Acta Obstet. Gynecol. Scand. 2016, 95, 1251–1257. [Google Scholar] [CrossRef]
- Basu, P.; Ponti, A.; Anttila, A.; Ronco, G.; Senore, C.; Vale, D.B.; Segnan, N.; Tomatis, M.; Soerjomataram, I.; Primic Žakelj, M. Status of implementation and organization of cancer screening in The European Union Member States—Summary results from the second European screening report. Int. J. Cancer 2018, 142, 44–56. [Google Scholar] [CrossRef]
- Stefan, L.; Terning, H.B.; Tor, H.; Suzanne, C.; Kristina, S.; Mari, N. Cervical cancer prevented by screening: Long-term incidence trends by morphology in Norway. Int. J. Cancer 2015, 137, 1758–1764. [Google Scholar] [CrossRef] [Green Version]
- Paul, K.T. “Saving lives”: Adapting and adopting Human Papilloma Virus (HPV) vaccination in Austria. Soc. Sci. Med. 2016, 153, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Anttila, A.; Ronco, G. Description of the national situation of cervical cancer screening in the member states of the European Union. Eur. J. Cancer 2009, 45, 2685–2708. [Google Scholar] [CrossRef]
- Breitenecker, G.; Dinges, H.P.; Regitnig, P.; Wiener, H.; Vutuc, C. Cytopathology in Austria. Cytopathology 2004, 15, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Rásky, É.; Regitnig, P.; Schenouda, M.; Burkert, N.; Freidl, W. Quality of screening with conventional Pap smear in Austria—A longitudinal evaluation. BMC Public Health 2013, 13, 998. [Google Scholar] [CrossRef]
- Schejter, E.; Bornstein, J.; Siegler, E. Cervical Cancer Screening, Human Papillomavirus Vaccination Practices and Current Infrastructure in Israel. Vaccine 2013, 31, I42–I45. [Google Scholar] [CrossRef]
- Bassal, R.; Schejter, E.; Bachar, R.; Shapira, H.; Kaufman, Z.; Cohen, D.; Keinan-Boker, L. Recent trends of cervical cancer and Cervical Intraepithelial Neoplasia 3 (CIN3) in Israel. Arch. Gynecol. Obstet. 2015, 292, 405–413. [Google Scholar] [CrossRef]
- Wymann, M.N.; Zographos, A.S.; Altpeter, E.; Spicher, V.M.; Low, N.; Mäusezahl-Feuz, M. Human papillomavirus vaccine uptake in adolescence and adherence to cervical cancer screening in Switzerland: A national cross-sectional survey. Int. J. Public Health 2018, 63, 105–114. [Google Scholar] [CrossRef]
- Boiron, L.; Joura, E.; Largeron, N.; Prager, B.; Uhart, M. Estimating the cost-effectiveness profile of a universal vaccination programme with a nine-valent HPV vaccine in Austria. BMC Infect. Dis. 2016, 16, 153. [Google Scholar] [CrossRef]
- Altobelli, E.; Lattanzi, A. Cervical Carcinoma in the European Union: An Update on Disease Burden, Screening Program State of Activation, and Coverage as of March 2014. Int. J. Gynecol. Cancer 2015, 25, 474–483. [Google Scholar] [CrossRef]
- Ponti, A.; Anttila, A.; Ronco, G.; Senore, C.; Basu, P.; Segnan, N. Cancer Screening in the European Union (2017): Report on the Implementation of the Council Recommendation on Cancer Screening; International Agency for Research Cancer: Lyon, France, 2017; Available online: https://ec.europa.eu/health/sites/health/files/major_chronic_diseases/docs/2017_cancerscreening_2ndreportimplementation_en.pdf (accessed on 29 January 2018).
- Borena, W.; Grünberger, M.; Widschwendter, A.; Kraxner, K.H.; Marth, E.; Mayr, P.; Meier, J.; Ruth, N.; Guerrero, A.T.; Marth, C. Pre-vaccine era cervical human papillomavirus infection among screening population of women in west Austria. BMC Public Health 2016, 16, 889. [Google Scholar] [CrossRef] [PubMed]
- Poncet, L.; Rigal, L.; Panjo, H.; Gautier, A.; Chauvin, P.; Menvielle, G.; Cadot, E.; Ringa, V. Disengagement of general practitioners in cervical cancer screening. Eur. J. Cancer Prev. 2016, 25, 547–555. [Google Scholar] [CrossRef] [PubMed]
- Paul, K.T.; Wallenburg, I.; Bal, R. Putting public health infrastructures to the test: Introducing HPV vaccination in Austria and the Netherlands. Sociol. Health Illn. 2018, 40, 67–81. [Google Scholar] [CrossRef] [PubMed]
- Lill, C.; Bachtiary, B.; Selzer, E.; Mittlboeck, M.; Thurnher, D. A 5-year update of patients with HPV positive versus negative oropharyngeal cancer after radiochemotherapy in Austria. Wiener klinische Wochenschrift 2017, 129, 398–403. [Google Scholar] [CrossRef]
- World Health Organization. Immunization, Vaccines and Biologicals. Available online: http://www.who.int/immunization/monitoring_surveillance/data/en/ (accessed on 16 July 2018).
- Vandeweyer, K.; Tjalma, W. PMD37—Cost-Effectiveness Analysis Of Primary HPV Screening With Dual-Stain Cytology Triage In The Cervical Cancer Screening Program Of Belgium. Value Health 2017, 20, A578. [Google Scholar] [CrossRef]
- Tjalma, W.A.; Kim, E.; Vandeweyer, K. The impact on women’s health and the cervical cancer screening budget of primary HPV screening with dual-stain cytology triage in Belgium. Eur. J. Obstet. Gynecol. Reprod. Biol. 2017, 212, 171–181. [Google Scholar] [CrossRef] [PubMed]
- Tjalma, W.A.A.; Trinh, X.B.; Rosenlund, M.; Makar, A.P.; Kridelka, F.; Rosillon, D.; Van Dam, P.A.; Collas De Souza, S.; Holl, K.; Simon, P.; et al. A cross-sectional, multicentre, epidemiological study on human papillomavirus (HPV) type distribution in adult women diagnosed with invasive cervical cancer in Belgium. Facts Views Vis. ObGyn 2015, 7, 101–108. [Google Scholar]
- Van Kerrebroeck, H.; Makar, A. Cervical cancer screening in Belgium and overscreening of adolescents. Eur. J. Cancer Prev. 2016, 25, 142–148. [Google Scholar] [CrossRef]
- Coorevits, L.; Traen, A.; Bingé, L.; Van Dorpe, J.; Praet, M.; Boelens, J.; Padalko, E. Are vaginal swabs comparable to cervical smears for human papillomavirus DNA testing? J. Gynecol. Oncol. 2018, 29, e8. [Google Scholar] [CrossRef]
- Flemish Minister for Welfare, Public Health and Family. Centrum Voor Kankeropsporing-CvKO. Available online: https://baarmoederhalskanker.bevolkingsonderzoek.be/nl/wij-doen-het-en-wat-doe-jij (accessed on 29 January 2018).
- Arbyn, M.; Broeck, D.V.; Benoy, I.; Bogers, J.; Depuydt, C.; Praet, M.; De Sutter, P.; Hoorens, A.; Hauben, E.; Poppe, W. Surveillance of effects of HPV vaccination in Belgium. Cancer Epidemiol. 2016, 41, 152–158. [Google Scholar] [CrossRef] [Green Version]
- Arbyn, M.; Haelens, A.; Desomer, A.; Verdoodt, F.; Thiry, N.; Francart, J.; Hanquet, G.; Robays, J. Cervical Cancer Screening Program and Human Papillomavirus (HPV) Testing, Part II: Update on HPV Primary Screening; Health Technology Assessment (HTA) KCE Reports 238Cs. D/2015/10.273/16; Belgian Health Care Knowledge Centre (KCE): Brussels, Belgium, 2015. [Google Scholar]
- Lefevere, E.; Theeten, H.; Hens, N.; De Smet, F.; Top, G.; Van Damme, P. From non school-based, co-payment to school-based, free Human Papillomavirus vaccination in Flanders (Belgium): A retrospective cohort study describing vaccination coverage, age-specific coverage and socio-economic inequalities. Vaccine 2015, 33, 5188–5195. [Google Scholar] [CrossRef]
- Lefevere, E.; Hens, N.; Theeten, H.; Van den Bosch, K.; Beutels, P.; De Smet, F.; Van Damme, P. Like mother, like daughter? Mother’s history of cervical cancer screening and daughter’s Human Papillomavirus vaccine uptake in Flanders (Belgium). Vaccine 2011, 29, 8390–8396. [Google Scholar] [CrossRef] [PubMed]
- Wentzensen, N.; Arbyn, M.; Berkhof, J.; Bower, M.; Canfell, K.; Einstein, M.; Farley, C.; Monsonego, J.; Franceschi, S. Eurogin 2016 Roadmap: How HPV knowledge is changing screening practice. Int. J. Cancer 2017, 140, 2192–2200. [Google Scholar] [CrossRef] [PubMed]
- Tjalma, W.A.A. Diagnostic performance of dual-staining cytology for cervical cancer screening: A systematic literature review. Eur. J. Obstet. Gynecol. Reprod. Biol. 2017, 210, 275–280. [Google Scholar] [CrossRef]
- Kesic, V.; Poljak, M.; Rogovskaya, S. Cervical cancer burden and prevention activities in Europe. Cancer Epidemiol. Prev. Biomarkers 2012, 21, 1423–1433. [Google Scholar] [CrossRef] [PubMed]
- Todorova, I.; Alexandrova-Karamanova, A.; Panayotova, Y.; Dimitrova, E.; Kotzeva, T. Managing uncertainty: Healthcare professionals’ meanings regarding the HPV vaccine. Int. J. Behav. Med. 2014, 21, 29–36. [Google Scholar] [CrossRef]
- Samson, K.K.; Haynatzki, G.; Soliman, A.S.; Valerianova, Z. Temporal changes in the cervical cancer burden in Bulgaria: Implications for eastern european countries going through transition. Cancer Epidemiol. 2016, 44, 154–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maver, P.J.; Seme, K.; Korac, T.; Dimitrov, G.; Dobrossy, L.; Engele, L.; Iljazovic, E.; Kesic, V.; Kostova, P.; Lausevic, D. Cervical cancer screening practices in central and eastern Europe in 2012. Acta Dermatovenerol. Alp. Pannonica Adriat. 2013, 22, 7–19. [Google Scholar] [CrossRef] [PubMed]
- Vaccarella, S.; Franceschi, S.; Zaridze, D.; Poljak, M.; Veerus, P.; Plummer, M.; Bray, F. Preventable fractions of cervical cancer via effective screening in six Baltic, central, and eastern European countries 2017–40: A population-based study. Lancet Oncol. 2016, 17, 1445–1452. [Google Scholar] [CrossRef]
- Sabol, I.; Milutin Gašperov, N.; Matovina, M.; Božinović, K.; Grubišić, G.; Fistonić, I.; Belci, D.; Alemany, L.; Džebro, S.; Dominis, M.; et al. Cervical HPV type-specific pre-vaccination prevalence and age distribution in Croatia. PLoS ONE 2017, 12, e0180480. [Google Scholar] [CrossRef]
- Štemberger-Papić, S.; Vrdoljak-Mozetič, D.; Verša Ostojić, D.; Rubeša-Mihaljević, R.; Dinter, M. Cervical cytology (Pap test)–terminology and importance in screening for cervical cancer. Med. Flum. 2016, 52, 324–336. [Google Scholar] [CrossRef]
- Krashias, G.; Koptides, D.; Christodoulou, C. HPV prevalence and type distribution in Cypriot women with cervical cytological abnormalities. BMC Infect. Dis. 2017, 17, 346. [Google Scholar] [CrossRef] [PubMed]
- Papapetrou, I.; Charalambous, G.; Sissouras, A.; Jelastopulu, E. Cervical Cancer Screening in the Municipality of Nicosia, Cyprus-Coverage and Association with Socioeconomic Determinants. Austin J Public Health Epidemiol. 2016, 3, 1032. [Google Scholar]
- Farazi, P.A. Cancer trends and risk factors in Cyprus. Ecancermedicalscience 2014, 8, 839. [Google Scholar] [CrossRef]
- Charalambous, H. Cancer Care in an Economically Torn Country: Cyprus. In Cancer Care in Countries and Societies in Transition; Springer: Cham, Switzerland, 2016; pp. 163–192. [Google Scholar] [CrossRef]
- Májek, O.; Dušková, J.; Dvorák, V.; Beková, A.; Klimeš, D.; Blaha, M.; Anttila, A.; Dušek, L. Performance indicators in a newly established organized cervical screening programme: Registry-based analysis in the Czech Republic. Eur. J. Cancer Prev. 2017, 26, 232–239. [Google Scholar] [CrossRef] [PubMed]
- Májek, O.; Dvořák, V.; Dušek, L.; Mužík, J.; Šnajdrová, L.; Gregor, J. Cervix. cz–Proč Pozvala Vaše Zdravotní Pojišťovna Právě Vás? Available online: http://www.cervix.cz/index.php?pg=cervikalni-screening--adresne-zvani-obcanu-do-programu-screeningu-zhoubnych-nadoru--proc-prave-vy#top (accessed on 4 December 2017).
- Dušková, J.; Beková, A.; Dvořák, V.; Májek, O.; Dušek, L. Results of the Czech National Cervical Cancer screening programme. Klinicka Onkologie: Casopis Ceske a Slovenske Onkologicke Spolecnosti 2014, 27, 79–86. [Google Scholar] [CrossRef]
- Hamsikova, E.; Smahelova, J.; Ludvikova, V.; Salakova, M.; Rychla, J.; Skrenkova, J.; Rob, L.; Tachezy, R. The prevalence of HPV infections in HPV-vaccinated women from the general population. APMIS 2017, 125, 585–595. [Google Scholar] [CrossRef]
- Brotherton, J.M.L.; Zuber, P.L.F.; Bloem, P.J.N. Primary Prevention of HPV through Vaccination: Update on the Current Global Status. Curr. Obstet. Gynecol. Rep. 2016, 5, 210–224. [Google Scholar] [CrossRef]
- Elfström, K.M.; Dillner, J.; Arnheim-Dahlström, L. Organization and quality of HPV vaccination programs in Europe. Vaccine 2015, 33, 1673–1681. [Google Scholar] [CrossRef]
- Rygaard, C. The Danish Quality Database for Cervical Cancer Screening. Clin. Epidemiol. 2016, 8, 655–660. [Google Scholar] [CrossRef]
- Lynge, E.; Andersen, B.; Christensen, J.; Ejersbo, D.; Jochumsen, K.; Johansen, T.; Kristensen, J.K.; Larsen, L.G.; Mehnert, F.; Mikkelsen, E.; et al. Cervical screening in Denmark—A success followed by stagnation. Acta Oncol. 2018, 57, 354–361. [Google Scholar] [CrossRef] [PubMed]
- Kristiansen, B.K.; Andersen, B.; Bro, F.; Svanholm, H.; Vedsted, P. Impact of GP reminders on follow-up of abnormal cervical cytology: A before–after study in Danish general practice. Br. J. Gen. Pract. 2017, 67, e580–e587. [Google Scholar] [CrossRef] [PubMed]
- Azerkan, F.; Widmark, C.; Sparén, P.; Weiderpass, E.; Tillgren, P.; Faxelid, E. When Life Got in the Way: How Danish and Norwegian Immigrant Women in Sweden Reason about Cervical Screening and Why They Postpone Attendance. PLoS ONE 2015, 10, e0107624. [Google Scholar] [CrossRef] [PubMed]
- Baandrup, L.; Blomberg, M.; Dehlendorff, C.; Sand, C.; Andersen, K.K.; Kjaer, S.K. Significant decrease in the incidence of genital warts in young Danish women after implementation of a national human papillomavirus vaccination program. Sex. Transm. Dis. 2013, 40, 130–135. [Google Scholar] [CrossRef] [PubMed]
- Skorstengaard, M.; Thamsborg, L.H.; Lynge, E. Burden of HPV-caused cancers in Denmark and the potential effect of HPV-vaccination. Vaccine 2017, 35, 5939–5945. [Google Scholar] [CrossRef] [PubMed]
- Olsen, J.; Jørgensen, T.R. Revisiting the cost-effectiveness of universal HPV-vaccination in Denmark accounting for all potentially vaccine preventable HPV-related diseases in males and females. Cost Eff. Resour. Alloc. 2015, 13, 4. [Google Scholar] [CrossRef] [PubMed]
- Hariri, S.; Markowitz, L.E.; Dunne, E.F.; Unger, E.R. Population impact of HPV vaccines: Summary of early evidence. J. Adolesc. Health 2013, 53, 679–682. [Google Scholar] [CrossRef]
- Kempers, J.; Narvestad, J.; Kofod, M.; Mikkelsen, R. Budget Impact Analysis of National Cervical Cancer Screening Program in Denmark: Cytology with HPV triage vs. HPV Primary Screening with Reflex Cytology Triage & Cintec Plus Cytology. Value Health 2016, 19, A689. [Google Scholar] [CrossRef]
- Rebolj, M.; Njor, S.; Lynge, E.; Preisler, S.; Ejegod, D.; Rygaard, C.; Bonde, J. Referral population studies underestimate differences between human papillomavirus assays in primary cervical screening. Cytopathology 2017, 28, 419–428. [Google Scholar] [CrossRef] [Green Version]
- Von Euler-Chelpin, M.; Lynge, E.; Rebolj, M. Register-based studies of cancer screening effects. Scand. J. Public Health 2011, 39, 158–164. [Google Scholar] [CrossRef] [Green Version]
- Kivistik, A.; Lang, K.; Baili, P.; Anttila, A.; Veerus, P. Women’s knowledge about cervical cancer risk factors, screening, and reasons for non-participation in cervical cancer screening programme in Estonia. BMC Womens Health 2011, 11, 43. [Google Scholar] [CrossRef] [PubMed]
- Uusküla, A.; Müürsepp, A.; Kawai, K.; Raag, M.; Jürisson, M.; Pillsbury, M. The epidemiological and economic impact of a quadrivalent human papillomavirus (hpv) vaccine in Estonia. BMC Infect. Dis. 2013, 13, 304. [Google Scholar] [CrossRef]
- Võrno, T.; Lutsar, K.; Uusküla, A.; Padrik, L.; Raud, T.; Reile, R.; Nahkur, O.; Kiivet, R.-A. Cost-effectiveness of HPV vaccination in the context of high cervical cancer incidence and low screening coverage. Vaccine 2017, 35, 6329–6335. [Google Scholar] [CrossRef] [PubMed]
- Malila, N.; Leinonen, M.; Kotaniemi-Talonen, L.; Laurila, P.; Tarkkanen, J.; Hakama, M. The HPV test has similar sensitivity but more overdiagnosis than the Pap test—A randomised health services study on cervical cancer screening in Finland. Int. J. Cancer 2013, 132, 2141–2147. [Google Scholar] [CrossRef] [PubMed]
- Lönnberg, S.; Anttila, A.; Luostarinen, T.; Nieminen, P. Age-specific effectiveness of the Finnish cervical cancer screening programme. Cancer Epidemiol. Prev. Biomarkers 2012, 21, 1354–1361. [Google Scholar] [CrossRef]
- Makkonen, P.; Heinävaara, S.; Sarkeala, T.; Anttila, A. Impact of organized and opportunistic Pap testing on the risk of cervical cancer in young women—A case-control study from Finland. Gynecol. Oncol. 2017, 147, 601–606. [Google Scholar] [CrossRef] [PubMed]
- Veijalainen, O.; Tuomisaari, S.; Luukkaala, T.; Mäenpää, J. High risk HPV testing in the triage of repeat ASC-US and LSIL. Acta Obstetr. Gynecol. Scand. 2015, 94, 931–936. [Google Scholar] [CrossRef]
- Idehen, E.E.; Korhonen, T.; Castaneda, A.; Juntunen, T.; Kangasniemi, M.; Pietilä, A.-M.; Koponen, P. Factors associated with cervical cancer screening participation among immigrants of Russian, Somali and Kurdish origin: A population-based study in Finland. BMC Womens Health 2017, 17, 19. [Google Scholar] [CrossRef]
- Van der Aa, M.A.; Pukkala, E.; Coebergh, J.W.W.; Anttila, A.; Siesling, S. Mass screening programmes and trends in cervical cancer in Finland and the Netherlands. Int. J. Cancer 2008, 122, 1854–1858. [Google Scholar] [CrossRef]
- Anttila, A.; Kotaniemi-Talonen, L.; Leinonen, M.; Hakama, M.; Laurila, P.; Tarkkanen, J.; Malila, N.; Nieminen, P. Rate of cervical cancer, severe intraepithelial neoplasia, and adenocarcinoma in situ in primary HPV DNA screening with cytology triage: Randomised study within organised screening programme. BMJ 2010, 340, c1804. [Google Scholar] [CrossRef] [PubMed]
- Skufca, J.; Ollgren, J.; Ruokokoski, E.; Lyytikäinen, O.; Nohynek, H. Incidence rates of Guillain Barré (GBS), chronic fatigue/systemic exertion intolerance disease (CFS/SEID) and postural orthostatic tachycardia syndrome (POTS) prior to introduction of human papilloma virus (HPV) vaccination among adolescent girls in Finland, 2002–2012. Papillomavirus Res. 2017, 3, 91–96. [Google Scholar] [CrossRef]
- Virtanen, A.; Anttila, A.; Luostarinen, T.; Nieminen, P. Self-sampling versus reminder letter: Effects on cervical cancer screening attendance and coverage in Finland. Int. J. Cancer 2011, 128, 2681–2687. [Google Scholar] [CrossRef] [PubMed]
- Karjalainen, L.; Anttila, A.; Nieminen, P.; Luostarinen, T.; Virtanen, A. Self-sampling in cervical cancer screening: Comparison of a brush-based and a lavage-based cervicovaginal self-sampling device. BMC Cancer 2016, 16, 221. [Google Scholar] [CrossRef]
- Hamers, F.F.; Duport, N.; Beltzer, N. Population-based organized cervical cancer screening pilot program in France. Eur. J. Cancer Prev. 2018, 27, 486–492. [Google Scholar] [CrossRef] [PubMed]
- Barré, S.; Massetti, M.; Leleu, H.; De Bels, F. Organised screening for cervical cancer in France: A cost-effectiveness assessment. BMJ Open 2017, 7, e014626. [Google Scholar] [CrossRef]
- Uhart, M.; Adam, M.; Dahlab, A.; Bresse, X. Loss of chance associated with sub-optimal HPV vaccination coverage rate in France. Papillomavirus Res. 2017, 3, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Schaffer, P.; Sancho-Garnier, H.; Fender, M.; Dellenbach, P.; Carbillet, J.; Monnet, E.; Gauthier, G.; Garnier, A. Cervical cancer screening in France. Eur. J. Cancer 2000, 36, 2215–2220. [Google Scholar] [CrossRef]
- Miranda, S.; Chaignot, C.; Collin, C.; Dray-Spira, R.; Weill, A.; Zureik, M. Human papillomavirus vaccination and risk of autoimmune diseases: A large cohort study of over 2 million young girls in France. Vaccine 2017, 35, 4761–4768. [Google Scholar] [CrossRef] [PubMed]
- Fagot, J.-P.; Boutrelle, A.; Ricordeau, P.; Weill, A.; Allemand, H. HPV vaccination in France: Uptake, costs and issues for the National Health Insurance. Vaccine 2011, 29, 3610–3616. [Google Scholar] [CrossRef]
- Shield, K.D.; Marant Micallef, C.; de Martel, C.; Heard, I.; Megraud, F.; Plummer, M.; Vignat, J.; Bray, F.; Soerjomataram, I. New cancer cases in France in 2015 attributable to infectious agents: A systematic review and meta-analysis. Eur. J. Epidemiol. 2018, 33, 263–274. [Google Scholar] [CrossRef]
- Guenat, D.; Launay, S.; Riethmuller, D.; Mougin, C.; Prétet, J.-L. Validation of Novaprep® HQ+ liquid-based cytology medium for high-risk human papillomavirus detection by hc2. Infect. Agents Cancer 2016, 11, 41. [Google Scholar] [CrossRef] [PubMed]
- Radde, K.; Gottschalk, A.; Bussas, U.; Schülein, S.; Schriefer, D.; Seifert, U.; Neumann, A.; Kaiser, M.; Blettner, M.; Klug, S.J. Invitation to cervical cancer screening does increase participation in Germany: Results from the MARZY study. Int. J. Cancer 2016, 139, 1018–1030. [Google Scholar] [CrossRef] [Green Version]
- Garbe, Y.; Klug, S.J. Aktueller Stand der HPV-Impfung in Deutschland. Der Onkologe 2017, 23, 409–414. [Google Scholar] [CrossRef]
- Geyer, S.; Jaunzeme, J.; Hillemanns, P. Cervical cancer screening in Germany: Group-specific participation rates in the state of Niedersachsen (Lower Saxony). A study with health insurance data. Arch. Gynecol. Obstet. 2015, 291, 623–629. [Google Scholar] [CrossRef]
- Damm, O.; Horn, J.; Mikolajczyk, R.T.; Kretzschmar, M.E.E.; Kaufmann, A.M.; Deleré, Y.; Ultsch, B.; Wichmann, O.; Krämer, A.; Greiner, W. Cost-effectiveness of human papillomavirus vaccination in Germany. Cost Eff. Resour. Alloc. 2017, 15, 18. [Google Scholar] [CrossRef] [PubMed]
- Hillemanns, P. The paradigm shift in cervical cancer screening in Germany. Arch. Gynecol. Obstet. 2016, 293, 3–4. [Google Scholar] [CrossRef]
- Schneider, V. Gynäkologische Krebsvorsorge in Deutschland. Der Pathologe 2012, 33, 286–292. [Google Scholar] [CrossRef]
- Schmidt, D.; Neumann, H.H. Wer macht die gynäkologische Zytologie und wie? Der Pathologe 2015, 36, 553–558. [Google Scholar] [CrossRef] [PubMed]
- Horn, J.; Damm, O.; Kretzschmar, M.E.E.; Deleré, Y.; Wichmann, O.; Kaufmann, A.M.; Garbe, E.; Krämer, A.; Greiner, W.; Mikolajczyk, R.T. Estimating the long-term effects of HPV vaccination in Germany. Vaccine 2013, 31, 2372–2380. [Google Scholar] [CrossRef]
- Petry, K.U.; Barth, C.; Wasem, J.; Neumann, A. A model to evaluate the costs and clinical effectiveness of human papilloma virus screening compared with annual papanicolaou cytology in Germany. Eur. J. Obstet. Gynecol. Reprod. Biol. 2017, 212, 132–139. [Google Scholar] [CrossRef]
- Farazi, P.A.; Hadji, P.; Roupa, Z. Awareness of human papilloma virus and cervical cancer prevention among Greek female healthcare workers. Eur. J. Cancer Prev. 2017, 26, 330–335. [Google Scholar] [CrossRef] [PubMed]
- Bacopoulou, F.; Karakitsos, P.; Kottaridi, C.; Stefanaki, C.; Deligeoroglou, E.; Theodoridou, K.; Chrousos, G.P.; Michos, A. Genital HPV in Children and Adolescents: Does Sexual Activity Make a Difference? J. Pediatr. Adolesc. Gynecol. 2016, 29, 228–233. [Google Scholar] [CrossRef] [PubMed]
- Chatzistamatiou, K.; Chatzaki, E.; Constantinidis, T.; Nena, E.; Tsertanidou, A.; Agorastos, T. Self-collected cervicovaginal sampling for site-of-care primary HPV-based cervical cancer screening: A pilot study in a rural underserved Greek population. J. Obstet. Gynaecol. 2017, 37, 1059–1064. [Google Scholar] [CrossRef] [PubMed]
- Vaidakis, D.; Moustaki, I.; Zervas, I.; Barbouni, A.; Merakou, K.; Chrysi, M.S.; Creatsa, G.; Panoskaltsis, T. Knowledge of Greek adolescents on human papilloma virus (HPV) and vaccination: A national epidemiologic study. Medicine 2017, 96, e5287. [Google Scholar] [CrossRef]
- Jelastopulu, E.; Karnaki, P.; Bartsokas, C.; Plotas, P.; Sissouras, A. Screening for Cervical Cancer-Uptake and Associated Factors in a Representative Sample in the City of Patras, West-Greece. Univers. J. Public Health 2013, 1, 7–13. [Google Scholar] [CrossRef]
- Karamanidou, C.; Dimopoulos, K. Greek health professionals’ perceptions of the HPV vaccine, state policy recommendations and their own role with regards to communication of relevant health information. BMC Public Health 2016, 16, 467. [Google Scholar] [CrossRef] [PubMed]
- Gyulai, A.; Nagy, A.; Pataki, V.; Tonté, D.; Ádány, R.; Vokó, Z. Survey of participation in organised cervical cancer-screening programme in hungary. Cent. Eur. J. Public Health 2015, 23, 360. [Google Scholar] [CrossRef]
- Balla, B.; Terebessy, A.; Tóth, E.; Balázs, P. Young Hungarian Students’ Knowledge about HPV and Their Attitude Toward HPV Vaccination. Vaccines 2016, 5, 1. [Google Scholar] [CrossRef]
- Pakai, A.; Brantmüller, É.; Réka, V.; Karácsony, I.; Balázs, P. Reasons for Non-appearance on Organized Cervical Screening in Hungary. Pract. Theory Syst. Educ. 2016, 11, 142–154. [Google Scholar] [CrossRef] [Green Version]
- Döbrőssy, L.; Oroszi, B.; Kovács, A.; Budai, A. Comprehensive Programme to Prevent Cervical Cancer-the Case of Hungary. Int. J. Virol. AIDS 2016, 3, 021. [Google Scholar] [CrossRef]
- Marek, E.; Berenyi, K.; Dergez, T.; Kiss, I.; D’Cruz, G. Influence of risk-taking health behaviours of adolescents on cervical cancer prevention: A Hungarian survey. Eur. J. Cancer Care 2016, 25, 57–68. [Google Scholar] [CrossRef] [PubMed]
- Szentirmay, Z.; Veleczki, Z.; Kásler, M. Human papillomavirus associated cervix uteri morbidity in Hungary: Epidemiology and correlation with the HPV types and the simultaneous cytological diagnosis. Orv. Hetil. 2017, 158, 1213–1221. [Google Scholar] [CrossRef] [PubMed]
- Vokó, Z.; Nagyjánosi, L.; Margitai, B.; Kövi, R.; Tóth, Z.; László, D.; Kaló, Z. Modeling Cost-Effectiveness of Cervical Cancer Screening in Hungary. Value Health 2012, 15, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Tsonev, A.; Ivanov, S.; Kovachev, E. Liquid-based cytology and its practicability in Bulgaria. Scr. Sci. Med. 2013, 45, 66–69. [Google Scholar] [CrossRef]
- McCarthy, C.M.; Ramphul, M.; Madden, M.; Hickey, K. The use and success of cold coagulation for the treatment of high grade squamous cervical intra-epithelial neoplasia: A retrospective review. Eur. J. Obstet. Gynecol. Reprod. Biol. 2016, 203, 225–228. [Google Scholar] [CrossRef]
- Flannelly, G.M.; Mooney, M.T.; Greehy, G.M.; Keogh, E.B.; McNally, S.A.; Fitzpatrick, P.E. Establishment of a national cervical screening programme in Ireland, CervicalCheck: The first 6 years. Eur. J. Cancer Prev. 2018, 27, 158–163. [Google Scholar] [CrossRef] [PubMed]
- Teljeur, C.; Tyrrell, E.; Kelly, A.; O’Dowd, T.; Thomas, S. Getting a handle on the general practice workforce in Ireland. Ir. J. Med. Sci. 2014, 183, 207–213. [Google Scholar] [CrossRef]
- O’Connor, M.; Costello, L.; Murphy, J.; Prendiville, W.; Martin, C.M.; O’Leary, J.J.; Sharp, L.; Irish Screening Research Consortium. ‘I don’t care whether it’s HPV or ABC, I just want to know if I have cancer.’ Factors influencing women’s emotional responses to undergoing human papillomavirus testing in routine management in cervical screening: A qualitative study. BJOG Int. J. Obstet. Gynaecol. 2014, 121, 1421–1430. [Google Scholar] [CrossRef]
- Giorgi Rossi, P.; Carozzi, F.; Federici, A.; Ronco, G.; Zappa, M.; Franceschi, S. Cervical cancer screening in women vaccinated against human papillomavirus infection: Recommendations from a consensus conference. Prev. Med. 2017, 98, 21–30. [Google Scholar] [CrossRef]
- Di Stefano, F.; Giorgi Rossi, P.; Carozzi, F.; Ronco, G.; Cacciani, L.; Vecchi, S.; Naldoni, C.; Segnan, N.; Gruppo di Lavoro MIDDIR—HPV Test In Primary Screening. [Implementation of DNA-HPV primary screening in Italian cervical cancer screening programmes. Results of the MIDDIR Project]. Epidemiol. Prev. 2017, 41, 116–124. [Google Scholar] [CrossRef]
- Ronco, G.; Zappa, M.; Franceschi, S.; Tunesi, S.; Caprioglio, A.; Confortini, M.; Del Mistro, A.; Carozzi, F.; Segnan, N.; Zorzi, M.; et al. Impact of variations in triage cytology interpretation on human papillomavirus–based cervical screening and implications for screening algorithms. Eur. J. Cancer 2016, 68, 148–155. [Google Scholar] [CrossRef] [Green Version]
- Bucchi, L.; Cristiani, P.; Costa, S.; Schincaglia, P.; Garutti, P.; Sassoli de Bianchi, P.; Naldoni, C.; Olea, O.; Sideri, M. Rationale and development of an on-line quality assurance programme for colposcopy in a population-based cervical screening setting in Italy. BMC Health Serv. Res. 2013, 13, 237. [Google Scholar] [CrossRef] [PubMed]
- Pasquale, L.; Rossi, P.G.; Carozzi, F.; Pedretti, C.; Ruggeri, C.; Scalvinoni, V.; Cottini, M.C.; Tosini, A.; Morana, C.; Chiaramonte, M.; et al. Cervical cancer screening with HPV testing in the Valcamonica (Italy) screening programme. J. Med. Screen. 2015, 22, 38–48. [Google Scholar] [CrossRef] [PubMed]
- Maggino, T.; Sciarrone, R.; Murer, B.; Dei Rossi, M.R.; Fedato, C.; Maran, M.; Lorio, M.; Soldà, M.; Zago, F.; Rossi, P.G.; et al. Screening women for cervical cancer carcinoma with a HPV mRNA test: First results from the Venice pilot program. Br. J. Cancer 2016, 115, 525–532. [Google Scholar] [CrossRef] [PubMed]
- Carozzi, F.M.; Iossa, A.; Scalisi, A.; Sideri, M.; Andersson, K.L.; Confortini, M.; Del Mistro, A.; Maina, G.; Ronco, G.; Raggi, P.; et al. hr-HPV testing in the management of women with ASC-US+ and in the follow-up of women with cytological abnormalities and negative colposcopy. Recommendations of the Italian group for cervical cancer screening (GISCi). Epidemiol. Prev. 2015, 39, 84–90. [Google Scholar]
- Carozzi, F.; Visioli, C.B.; Confortini, M.; Iossa, A.; Mantellini, P.; Burroni, E.; Zappa, M. hr-HPV testing in the follow-up of women with cytological abnormalities and negative colposcopy. Br. J. Cancer 2013, 109, 1766–1774. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vīberga, I.; Poljak, M. Cervical cancer screening in Latvia: A brief history and recent improvements (2009–2011). Acta Dermatovenerol. Alp. Pannonica Adriat. 2013, 22, 27–30. [Google Scholar]
- Kornete, A.; Pumpure, E.; Macuks, R. Analysis of invasive cervical cancer cases in Latvia. Int. J. Reprod. Contracept. Obstet. Gynecol. 2016, 5, 3789–3794. [Google Scholar] [CrossRef]
- Viberga, I.; Engele, L.; Kojalo, U.; Santare, D. Professionals’ role in implementing a cervical cancer screening program. Acta Dermatovenerol. Alp. Pannonica Adriat. 2014, 23, 69–73. [Google Scholar] [CrossRef]
- Patel, H.; Pčolkina, K.; Strazdina, K.; Viberga, I.; Sherman, S.M.; Tincello, D.G.; Redman, C.W.; Rezeberga, D.; Moss, E.L. Awareness of HPV infection and attitudes toward HPV vaccination among Latvian adolescents. Int. J. Gynecol. Obstet. 2017, 137, 138–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurtinaitienė, R.; Rimienė, J.; Labanauskaitė, I.; Lipunova, N.; Smailytė, G. Increasing attendance in a cervical cancer screening programme by personal invitation: Experience of a Lithuanian primary health care centre. Acta Med. Litu. 2016, 23, 180–184. [Google Scholar] [CrossRef] [PubMed]
- Kurtinaitienė, R.; Drąsutienė, G.; Labanauskaitė, I.; Akelytė, A.; Drąsutytė, L. Vilniaus miesto moterų žinios apie gimdos kaklelio vėžio rizikos veiksnius ir patikros programą. MTP 2008, 14, 325–330. [Google Scholar]
- Latsuzbaia, A.; Hebette, G.; Fischer, M.; Arbyn, M.; Weyers, S.; Vielh, P.; Schmitt, F.; Mossong, J. Introduction of liquid-based cytology and human papillomavirus testing in cervical cancer screening in Luxembourg. Diagn. Cytopathol. 2017, 45, 384–390. [Google Scholar] [CrossRef]
- Sankaranarayanan, R.; Qiao, Y.-L.; Keita, N. The Next Steps in Cervical Screening. Women’s Health 2015, 11, 201–212. [Google Scholar] [CrossRef]
- Scheiden, R.; Knolle, U.; Wagener, C.; Wehenkel, A.M.; Capesius, C. Cervical cancer screening in Luxembourg. Eur. J. Cancer 2000, 36, 2240–2243. [Google Scholar] [CrossRef]
- Scheiden, R.; Wagener, C.; Knolle, U.; Wehenkel, A.; Dippel, W.; Capesius, C. Cervical screening in Luxembourg: 1990–1999. Cytopathology 2003, 14, 235–240. [Google Scholar] [CrossRef] [PubMed]
- Anttila, A.; von Karsa, L.; Aasmaa, A.; Fender, M.; Patnick, J.; Rebolj, M.; Nicula, F.; Vass, L.; Valerianova, Z.; Voti, L.; et al. Cervical cancer screening policies and coverage in Europe. Eur. J. Cancer 2009, 45, 2649–2658. [Google Scholar] [CrossRef] [PubMed]
- Latsuzbaia, A.; Tapp, J.; Nguyen, T.; Fischer, M.; Arbyn, M.; Weyers, S.; Mossong, J. Analytical performance evaluation of Anyplex II HPV28 and Euroarray HPV for genotyping of cervical samples. Diagn. Microbiol. Infect. Dis. 2016, 85, 318–322. [Google Scholar] [CrossRef]
- Government of Malta. Cervix Screening Programme in Malta. Available online: https://deputyprimeminister.gov.mt/en/phc/nbs/Pages/Cervix-Screening-Programme.aspx (accessed on 4 January 2018).
- Huijsmans, C.J.J.; Geurts-Giele, W.R.R.; Leeijen, C.; Hazenberg, H.L.C.M.; van Beek, J.; de Wild, C.; van der Linden, J.C.; van den Brule, A.J.C. HPV Prevalence in the Dutch cervical cancer screening population (DuSC study): HPV testing using automated HC2, cobas and Aptima workflows. BMC Cancer 2016, 16, 922. [Google Scholar] [CrossRef]
- Van Ballegooijen, M.; Hermens, R. Cervical cancer screening in The Netherlands. Eur. J. Cancer 2000, 36, 2244–2246. [Google Scholar] [CrossRef]
- Rozemeijer, K.; de Kok, I.M.C.M.; Naber, S.K.; van Kemenade, F.J.; Penning, C.; van Rosmalen, J.; van Ballegooijen, M. Offering Self-Sampling to Non-Attendees of Organized Primary HPV Screening: When Do Harms Outweigh the Benefits? Cancer Epidemiol. Biomarkers Prev. 2015, 24, 773–782. [Google Scholar] [CrossRef]
- Ketelaars, P.J.W.; Bosgraaf, R.P.; Siebers, A.G.; Massuger, L.F.A.G.; van der Linden, J.C.; Wauters, C.A.P.; Rahamat-Langendoen, J.C.; van den Brule, A.J.C.; IntHout, J.; Melchers, W.J.G.; et al. High-risk human papillomavirus detection in self-sampling compared to physician-taken smear in a responder population of the Dutch cervical screening: Results of the VERA study. Prev. Med. 2017, 101, 96–101. [Google Scholar] [CrossRef] [PubMed]
- Qendri, V.; Bogaards, J.A.; Berkhof, J. Health and Economic Impact of a Tender-Based, Sex-Neutral Human Papillomavirus 16/18 Vaccination Program in the Netherlands. J. Infect. Dis. 2017, 216, 210–219. [Google Scholar] [CrossRef] [PubMed]
- Naber, S.K.; Matthijsse, S.M.; Rozemeijer, K.; Penning, C.; de Kok, I.M.C.M.; van Ballegooijen, M. Cervical Cancer Screening in Partly HPV Vaccinated Cohorts—A Cost-Effectiveness Analysis. PLoS ONE 2016, 11, e0145548. [Google Scholar] [CrossRef] [PubMed]
- Nowakowski, A.; Cybulski, M.; Śliwczyński, A.; Chil, A.; Teter, Z.; Seroczyński, P.; Arbyn, M.; Anttila, A. The implementation of an organised cervical screening programme in Poland: An analysis of the adherence to European guidelines. BMC Cancer 2015, 15, 279. [Google Scholar] [CrossRef]
- Nowakowski, A.; Wojciechowska, U.; Wieszczy, P.; Cybulski, M.; Kamiński, M.F.; Didkowska, J. Trends in cervical cancer incidence and mortality in Poland: Is there an impact of the introduction of the organised screening? Eur. J. Epidemiol. 2017, 32, 529–532. [Google Scholar] [CrossRef]
- Kalinowski, P.; Grządziel, A. HPV Vaccinations in Lublin Region, Poland. Postepy Hig. Med. Doswiadczalnej (Online) 2017, 71, 92–97. [Google Scholar] [CrossRef]
- Nowakowski, A.; de Souza, S.C.; Jach, R.; Rosillon, D.; Książek, A.; Holl, K. HPV-Type Distribution and Reproducibility of Histological Diagnosis in Cervical Neoplasia in Poland. Pathol. Oncol. Res. 2015, 21, 703–711. [Google Scholar] [CrossRef]
- Costa, A.R.; Silva, S.; Moura-Ferreira, P.; Villaverde-Cabral, M.; Santos, O.; do Carmo, I.; Barros, H.; Lunet, N. Cancer screening in Portugal: Sex differences in prevalence, awareness of organized programmes and perception of benefits and adverse effects. Health Expect. 2017, 20, 211–220. [Google Scholar] [CrossRef]
- Real, O.; Silva, D.; Leitão, M.A.; Oliveira, H.M.; Rocha Alves, J.G. Cervical cancer screening in the central region of Portugal. Eur. J. Cancer 2000, 36, 2247–2249. [Google Scholar] [CrossRef]
- Firmino-Machado, J.; Mendes, R.; Moreira, A.; Lunet, N. Stepwise strategy to improve Cervical Cancer Screening Adherence (SCAN-CC): Automated text messages, phone calls and face-to-face interviews: Protocol of a population-based randomised controlled trial. BMJ Open 2017, 7, e017730. [Google Scholar] [CrossRef] [PubMed]
- Pista, A.; de Oliveira, C.F.; Lopes, C.; Cunha, M.J.; CLEOPATRE Portugal Study Group. Potential impact of nonavalent HPV vaccine in the prevention of high-grade cervical lesions and cervical cancer in Portugal. Int. J. Gynecol. Obstet. 2017, 139, 90–94. [Google Scholar] [CrossRef] [PubMed]
- Grigore, M.; Popovici, R.; Pristavu, A.; Grigore, A.M.; Matei, M.; Gafitanu, D. Perception and use of Pap smear screening among rural and urban women in Romania. Eur. J. Public Health 2017, 27, 1084–1088. [Google Scholar] [CrossRef] [PubMed]
- Penţa, M.A.; Băban, A. Mass media coverage of HPV vaccination in Romania: A content analysis. Health Educ. Res. 2014, 29, 977–992. [Google Scholar] [CrossRef]
- Vorsters, A.; Arbyn, M.; Baay, M.; Bosch, X.; de Sanjosé, S.; Hanley, S.; Karafillakis, E.; Lopalco, P.L.; Pollock, K.G.; Yarwood, J.; et al. Overcoming barriers in HPV vaccination and screening programs. Papillomavirus Res. 2017, 4, 45–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grigore, M.; Teleman, S.I.; Pristavu, A.; Matei, M. Awareness and Knowledge About HPV and HPV Vaccine Among Romanian Women. J. Cancer Educ. 2018, 33, 154–159. [Google Scholar] [CrossRef] [PubMed]
- Craciun, C.; Baban, A. “Who will take the blame?”: Understanding the reasons why Romanian mothers decline HPV vaccination for their daughters. Vaccine 2012, 30, 6789–6793. [Google Scholar] [CrossRef]
- Andreassen, T.; Melnic, A.; Figueiredo, R.; Moen, K.; Şuteu, O.; Nicula, F.; Ursin, G.; Weiderpass, E. Attendance to cervical cancer screening among Roma and non-Roma women living in North-Western region of Romania. Int. J. Public Health 2018, 63, 609–619. [Google Scholar] [CrossRef] [PubMed]
- Obročníková, A.; Majerníková, Ľ. Knowledge, attitudes and practices of cervical cancer prevention. Pielegniarstwo XXI Wieku/Nurs. 21st Century 2017, 16, 18–22. [Google Scholar] [CrossRef] [Green Version]
- Jackowska, M.; von Wagner, C.; Wardle, J.; Juszczyk, D.; Luszczynska, A.; Waller, J. Cervical screening among migrant women: A qualitative study of Polish, Slovak and Romanian women in London, UK. J. Fam. Plan. Reprod. Health Care 2012, 38, 229–238. [Google Scholar] [CrossRef]
- Bastos, J.; Peleteiro, B.; Gouveia, J.; Coleman, M.P.; Lunet, N. The state of the art of cancer control in 30 European countries in 2008. Int. J. Cancer 2010, 126, 2700–2715. [Google Scholar] [CrossRef] [PubMed]
- Rajčáni, J.; Kajo, K.; Hassoun, O.E.; Adamkov, M.; Benčat, M. The Diagnostic of Cervical Carcinoma: From Theory to Practice. In Human Papillomavirus—Research in a Global Perspective; Rajkumar, R., Ed.; InTech: Rijeka, Croatia, 2016. [Google Scholar]
- Jančar, N.; Mihevc Ponikvar, B.; Tomšič, S. Cold-knife conisation and large loop excision of transformation zone significantly increase the risk for spontaneous preterm birth: A population-based cohort study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2016, 203, 245–249. [Google Scholar] [CrossRef]
- Zadnik, V.; Primic Zakelj, M.; Lokar, K.; Jarm, K.; Ivanus, U.; Zagar, T. Cancer burden in slovenia with the time trends analysis. Radiol. Oncol. 2017, 51, 47–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Učakar, V.; Jelen, M.M.; Faust, H.; Poljak, M.; Dillner, J.; Klavs, I. Pre-vaccination seroprevalence of 15 human papillomavirus (HPV) types among women in the population-based Slovenian cervical screening program. Vaccine 2013, 31, 4935–4939. [Google Scholar] [CrossRef] [Green Version]
- Prevention; Šubelj, M.; Učakar, V.; Kraigher, A.; Klavs, I. Adverse events following school-based vaccination of girls with quadrivalent human papillomavirus vaccine in Slovenia, 2009 to 2013. Euro Surveill. 2016, 21. [Google Scholar] [CrossRef] [Green Version]
- Marzo-Castillejo, M.; Bellas-Beceiro, B.; Vela-Vallespín, C.; Nuin-Villanueva, M.; Bartolomé-Moreno, C.; Melús-Palazón, E.; Vilarrubí-Estrella, M. Recomendaciones de prevención del cáncer. Actualización 2016. Aten. Primaria 2016, 48, 39–59. [Google Scholar] [CrossRef] [Green Version]
- Trapero-Bertran, M.; Acera Pérez, A.; de Sanjosé, S.; Manresa Domínguez, J.M.; Rodríguez Capriles, D.; Rodriguez Martinez, A.; Bonet Simó, J.M.; Sanchez Sanchez, N.; Hidalgo Valls, P.; Díaz Sanchis, M. Cost-effectiveness of strategies to increase screening coverage for cervical cancer in Spain: The CRIVERVA study. BMC Public Health 2017, 17, 194. [Google Scholar] [CrossRef] [PubMed]
- Fernández Calvo, M.T.; Hernández Rubio, A.; Rosell Aguilar, I. Cervical cancer screening in Spain. Eur. J. Cancer 2000, 36, 2250–2254. [Google Scholar] [CrossRef]
- Limia, A.; Pachón, I. Coverage of human papillomavirus vaccination during the first year of its introduction in Spain. Euro Surveill. 2011, 16, 310–318. [Google Scholar]
- Ibáñez, R.; Moreno-Crespi, J.; Sardà, M.; Autonell, J.; Fibla, M.; Gutiérrez, C.; Lloveras, B.; Alejo, M.; Català, I.; Alameda, F.; et al. Prediction of cervical intraepithelial neoplasia grade 2+ (CIN2+) using HPV DNA testing after a diagnosis of atypical squamous cell of undetermined significance (ASC-US) in Catalonia, Spain. BMC Infect. Dis. 2012, 12, 25. [Google Scholar] [CrossRef]
- Yuan, L.; Hu, Y.; Zhou, Z.; Gong, Y.; Wang, R.; Li, N. Quantitative methylation analysis to detect cervical (pre)-cancerous lesions in high-risk HPV-positive women. Int. J. Clin. Exp. Med. 2017, 10, 10577–10586. [Google Scholar]
- Pérez-Castro, S.; Lorenzo-Mahía, Y.; Iñarrea Fernández, A.; Lamas-González, M.J.; Sarán-Díez, M.T.; Rubio-Alarcón, J.; Reboredo-Reboredo, M.C.; Mosteiro-Lobato, S.; López-Miragaya, I.; Torres-Piñón, J.; et al. Cervical intraepithelial neoplasia grade 2 or worse in Galicia, Spain: HPV 16 prevalence and vaccination impact. Enferm. Infecc. Microbiol. Clín. 2014, 32, 479–485. [Google Scholar] [CrossRef] [PubMed]
- Castillo, M.; Astudillo, A.; Clavero, O.; Velasco, J.; Ibáñez, R.; de Sanjosé, S. Poor Cervical Cancer Screening Attendance and False Negatives. A Call for Organized Screening. PLoS ONE 2016, 11, e0161403. [Google Scholar] [CrossRef] [PubMed]
- Cervantes-Amat, M.; López-Abente, G.; Aragonés, N.; Pollán, M.; Pastor-Barriuso, R.; Pérez-Gómez, B. The end of the decline in cervical cancer mortality in Spain: Trends across the period 1981–2012. BMC Cancer 2015, 15, 287. [Google Scholar] [CrossRef] [PubMed]
- Ascunce, N.; Salas, D.; Zubizarreta, R.; Almazán, R.; Ibáñez, J.; Ederra, M. Cancer screening in Spain. Ann. Oncol. 2010, 21, iii43–iii51. [Google Scholar] [CrossRef] [PubMed]
- Östensson, E.; Fröberg, M.; Leval, A.; Hellström, A.-C.; Bäcklund, M.; Zethraeus, N.; Andersson, S. Cost of Preventing, Managing, and Treating Human Papillomavirus (HPV)-Related Diseases in Sweden before the Introduction of Quadrivalent HPV Vaccination. PLoS ONE 2015, 10, e0139062. [Google Scholar] [CrossRef]
- Baltzer, N.; Sundström, K.; Nygård, J.F.; Dillner, J.; Komorowski, J. Risk stratification in cervical cancer screening by complete screening history: Applying bioinformatics to a general screening population. Int. J. Cancer 2017, 141, 200–209. [Google Scholar] [CrossRef]
- Andrae, B.; Kemetli, L.; Sparén, P.; Silfverdal, L.; Strander, B.; Ryd, W.; Dillner, J.; Törnberg, S. Screening-Preventable Cervical Cancer Risks: Evidence From a Nationwide Audit in Sweden. JNCI J. Natl. Cancer Inst. 2008, 100, 622–629. [Google Scholar] [CrossRef] [Green Version]
- Alfonzo, E.; Andersson Ellström, A.; Nemes, S.; Strander, B. Effect of Fee on Cervical Cancer Screening Attendance—ScreenFee, a Swedish Population-Based Randomised Trial. PLoS ONE 2016, 11, e0150888. [Google Scholar] [CrossRef]
- Thomsen, L.T.; Nygård, M.; Stensen, S.; Terning Hansen, B.; Arnheim Dahlström, L.; Liaw, K.-L.; Munk, C.; Kjaer, S.K. Awareness of human papillomavirus after introduction of HPV vaccination: A large population-based survey of Scandinavian women. Eur. J. Cancer Prev. 2017, 26, 170–178. [Google Scholar] [CrossRef] [PubMed]
- Hortlund, M.; Sundström, K.; Lamin, H.; Hjerpe, A.; Dillner, J. Laboratory audit as part of the quality assessment of a primary HPV-screening program. J. Clin. Virol. 2016, 75, 33–36. [Google Scholar] [CrossRef] [PubMed]
- Lamin, H.; Eklund, C.; Elfström, K.M.; Carlsten-Thor, A.; Hortlund, M.; Elfgren, K.; Törnberg, S.; Dillner, J. Randomised healthcare policy evaluation of organised primary human papillomavirus screening of women aged 56–60. BMJ Open 2017, 7, e014788. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, K.; Fogelberg, S.; Thamsborg, L.H.; Clements, M.; Nygård, M.; Kristiansen, I.S.; Lynge, E.; Sparén, P.; Kim, J.J.; Burger, E.A. An overview of cervical cancer epidemiology and prevention in Scandinavia. Acta Obstet. Gynecol. Scand 2018, 97, 795–807. [Google Scholar] [CrossRef] [PubMed]
- Aref-Adib, M.; Freeman-Wang, T. Cervical cancer prevention and screening: The role of human papillomavirus testing. Obstet. Gynaecol. 2016, 18, 251–263. [Google Scholar] [CrossRef] [Green Version]
- Albrow, R.; Kitchener, H.; Gupta, N.; Desai, M. Cervical screening in England: The past, present, and future. Cancer Cytopathol. 2012, 120, 87–96. [Google Scholar] [CrossRef]
- Anwar, M.; Abdullah, A. Importance Of Cervical Screening In Women. J. Nurs. 2014, 4, 5. [Google Scholar] [CrossRef]
- Kitchener, H.C.; Gilham, C.; Sargent, A.; Bailey, A.; Albrow, R.; Roberts, C.; Desai, M.; Mather, J.; Turner, A.; Moss, S.; et al. A comparison of HPV DNA testing and liquid based cytology over three rounds of primary cervical screening: Extended follow up in the ARTISTIC trial. Eur. J. Cancer 2011, 47, 864–871. [Google Scholar] [CrossRef]
- Hilton, S.; Hunt, K.; Langan, M.; Bedford, H.; Petticrew, M. Newsprint media representations of the introduction of the HPV vaccination programme for cervical cancer prevention in the UK (2005–2008). Soc. Sci. Med. 2010, 70, 942–950. [Google Scholar] [CrossRef] [Green Version]
- Smith, J.H.F. Cervical Screening: History, Current Algorithms, and Future Directions. In Pathology of the Cervix; Herrington, C.S., Ed.; Springer International Publishing: Cham, Switzerland, 2017; pp. 45–65. [Google Scholar] [CrossRef]
- Williams, D.; Davies, M.; Fiander, A.; Farewell, D.; Hillier, S.; Brain, K. Women’s perspectives on human papillomavirus self-sampling in the context of the UK cervical screening programme. Health Expect. 2017, 20, 1031–1040. [Google Scholar] [CrossRef]
- Westre, B.; Giske, A.; Guttormsen, H.; Sørbye, S.W.; Skjeldestad, F.E. 5-type HPV mRNA versus 14-type HPV DNA test: Test performance, over-diagnosis and overtreatment in triage of women with minor cervical lesions. BMC Clin. Pathol. 2016, 16, 9. [Google Scholar] [CrossRef]
- Leinonen, M.K.; Campbell, S.; Ursin, G.; Tropé, A.; Nygård, M. Barriers to cervical cancer screening faced by immigrants: A registry-based study of 1.4 million women in Norway. Eur. J. Public Health 2017, 27, 873–879. [Google Scholar] [CrossRef]
- Nygård, J.F.; Skare, G.B.; Thoresen, S.Ø. The cervical cancer screening programme in Norway, 1992–2000: Changes in Pap smear coverage and incidence of cervical cancer. J. Med. Screen. 2002, 9, 86–91. [Google Scholar] [CrossRef] [PubMed]
- Haldorsen, T.; Skare, G.B.; Ursin, G.; Bjørge, T. Results of delayed triage by HPV testing and cytology in the Norwegian Cervical Cancer Screening Programme. Acta Oncol. 2015, 54, 200–209. [Google Scholar] [CrossRef] [PubMed]
- Sørbye, S.W.; Suhrke, P.; Revå, B.W.; Berland, J.; Maurseth, R.J.; Al-Shibli, K. Accuracy of cervical cytology: Comparison of diagnoses of 100 Pap smears read by four pathologists at three hospitals in Norway. BMC Clin. Pathol. 2017, 17, 18. [Google Scholar] [CrossRef] [PubMed]
- Engesæter, B.; van Diermen Hidle, B.; Hansen, M.; Moltu, P.; Staby, K.M.; Borchgrevink-Persen, S.; Vintermyr, O.K.; Lönnberg, S.; Nygård, M.; Janssen, E.A.M.; et al. Quality assurance of human papillomavirus (HPV) testing in the implementation of HPV primary screening in Norway: An inter-laboratory reproducibility study. BMC Infect. Dis. 2016, 16, 698. [Google Scholar] [CrossRef] [PubMed]
- Caspi, R.; Schejter, E.; Groutz, A. Screening for Cervical Cancer Among Low-Risk Populations: Orthodox Jewish Women as a Model. J. Women’s Health 2016, 25, 747–751. [Google Scholar] [CrossRef]
- Bassal, R.; Schejter, E.; Bachar, R.; Shapira, H.; Sandbank, J.; Supino Rosin, L.; Schvimer, M.; Cohen, D.; Keinan-Boker, L. Cervical Pap screening among Israeli women, 2005–2010. Arch. Gynecol. Obstet. 2014, 289, 615–622. [Google Scholar] [CrossRef] [PubMed]
- Bassal, R.; Schejter, E.; Bachar, R.; Perri, T.; Korach, J.; Jakobson-Setton, A.; Ben-David, L.H.; Cohen, D.; Keinan-Boker, L. Risk Factors for Cervical Cancer and CIN3 in Jewish Women in Israel—Two Case Control Studies. Asian Pac. J. Cancer Prev. APJCP 2016, 17, 2067–2073. [Google Scholar] [CrossRef]
- Amir, H.; Gophen, R.; Amir Levy, Y.; Hasson, J.; Gordon, D.; Amit, A.; Azem, F. Obstetricians and gynecologists: Which characteristics do Israeli lesbians prefer? J. Obstet. Gynaecol. Res. 2015, 41, 283–293. [Google Scholar] [CrossRef]
- Lurie, S.; Mizrachi, Y.; Chodick, G.; Katz, R.; Schejter, E. Impact of quadrivalent human papillomavirus vaccine on genital warts in an opportunistic vaccination structure. Gynecol. Oncol. 2017, 146, 299–304. [Google Scholar] [CrossRef]
- Vassilakos, P.; Petignat, P.; Boulvain, M.; Campana, A. Primary screening for cervical cancer precursors by the combined use of liquid-based cytology, computer-assisted cytology and HPV DNA testing. Br. J. Cancer 2002, 86, 382–388. [Google Scholar] [CrossRef] [PubMed]
- Dobec, M.; Bannwart, F.; Kilgus, S.; Kaeppeli, F.; Cassinotti, P. Human papillomavirus infection among women with cytological abnormalities in Switzerland investigated by an automated linear array genotyping test. J. Med. Virol. 2011, 83, 1370–1376. [Google Scholar] [CrossRef] [PubMed]
- Viviano, M.; Catarino, R.; Jeannot, E.; Boulvain, M.; Malinverno, M.U.; Vassilakos, P.; Petignat, P. Self-sampling to improve cervical cancer screening coverage in Switzerland: A randomised controlled trial. Br. J. Cancer 2017, 116, 1382–1388. [Google Scholar] [CrossRef] [PubMed]
- Burton-Jeangros, C.; Cullati, S.; Manor, O.; Courvoisier, D.S.; Bouchardy, C.; Guessous, I. Cervical cancer screening in Switzerland: Cross-sectional trends (1992–2012) in social inequalities. Eur. J. Public Health 2017, 27, 167–173. [Google Scholar] [CrossRef]
- Fargnoli, V.; Petignat, P.; Burton-Jeangros, C. To what extent will women accept HPV self-sampling for cervical cancer screening? A qualitative study conducted in Switzerland. Int. J. Women’s Health 2015, 7, 883–888. [Google Scholar] [CrossRef]
- Raineri, I. Cervical Screening In Switzerland: The Opportunistic Approach. Cytopathology 2015, 26, 4–5. [Google Scholar]
- Szucs, T.D.; Largeron, N.; Dedes, K.J.; Rafia, R.; Bénard, S. Cost-effectiveness analysis of adding a quadrivalent HPV vaccine to the cervical cancer screening programme in Switzerland. Curr. Med. Res. Opin. 2008, 24, 1473–1483. [Google Scholar] [CrossRef]
- Karasu, A.F.G.; Adanir, I.; Aydin, S.; Ilhan, G.K.; Ofli, T. Nurses’ Knowledge and Opinions on HPV Vaccination: A Cross-Sectional Study from Istanbul. J. Cancer Educ. 2017. [Google Scholar] [CrossRef]
- Demir, L.S.; Asuk, N.A.; Demir, N.A. Screening for breast and cervix cancers in a rural part of Turkey. Biomed. Res. 2017, 28, 7647–7650. [Google Scholar]
- Ozlem, A.; Umit, I. Comparative analysis of cervical cytology screening methods and staining protocols for detection rate and accurate interpretation of ASC-H: Data from a high-volume laboratory in Turkey. Diagn. Cytopathol. 2015, 43, 863–869. [Google Scholar] [CrossRef]
- Gultekin, M.; Zayifoglu Karaca, M.; Kucukyildiz, I.; Dundar, S.; Boztas, G.; Semra Turan, H.; Hacikamiloglu, E.; Murtuza, K.; Keskinkilic, B.; Sencan, I. Initial results of population based cervical cancer screening program using HPV testing in one million Turkish women. Int. J. Cancer 2018, 142, 1952–1958. [Google Scholar] [CrossRef] [PubMed]
- Kir, G.; Seneldir, H.; Cosan Sarbay, B. The clinical performance of computer-assisted liquid-based cytology, primary hrHPV screening, and cotesting at a Turkish Tertiary Care Hospital. Diagn. Cytopathol. 2018, 46, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Erbarut Seven, I.; Mollamemisoglu, H.; Eren, F. Reliability of reporting the presence of transformation zone material in Papanicolaou smears using an automated screening system. Cytopathology 2017, 28, 280–283. [Google Scholar] [CrossRef] [PubMed]
- Türkmen, İ.Ç.; Usubütün, A.; Çakir, A.; Aydin, Ö.; Bolat, F.A.; Akbulut, M.; Altinay, S.; Arici, S.; Aslan, F.; Astarci, M. What does the Data of 354,725 Patients from Turkey Tell Us About Cervical Smear Epithelial Cell Abnormalities?-The Epithelial Cell Abnormality Rate is Increasing-Quality Control Studies and Corrective Activity are Musts. Turk. J. Pathol. 2017, 33, 134–143. [Google Scholar] [CrossRef] [PubMed]
- Yanikkerem, E.; Koker, G. Knowledge, attitudes, practices and barriers towards HPV vaccination among nurses in Turkey: A longitudinal study. Asian Pac. J. Cancer Prev. APJCP 2014, 15, 7693–7702. [Google Scholar] [CrossRef]
- Oz, M.; Cetinkaya, N.; Apaydin, A.; Korkmaz, E.; Bas, S.; Ozgu, E.; Gungor, T. Awareness and Knowledge Levels of Turkish College Students about Human Papilloma Virus Infection and Vaccine Acceptance. J. Cancer Educ. 2018, 33, 260–268. [Google Scholar] [CrossRef] [PubMed]
- Bal-Yılmaz, H.; Koniak-Griffin, D. Knowledge, Behaviors, and Attitudes About Human Papilloma Virus Among Nursing Students in Izmir, Turkey. J. Cancer Educ. 2018, 33, 814–820. [Google Scholar] [CrossRef]
- Dzhafer, N. The programme “Stop and get checked”—An attempt to restore cancer screening in Bulgaria. Scripta Scientifica Salutis Publicae 2016, 2, 108–112. [Google Scholar] [CrossRef]
- Enerly, E.; Bonde, J.; Schee, K.; Pedersen, H.; Lönnberg, S.; Nygård, M. Self-Sampling for Human Papillomavirus Testing among Non-Attenders Increases Attendance to the Norwegian Cervical Cancer Screening Programme. PLoS ONE 2016, 11, e0151978. [Google Scholar] [CrossRef]
- Tamalet, C.; Halfon, P.; Retraite, L.L.; Grob, A.; Leandri, F.X.; Heid, P.; Sancho-Garnier, H.; Piana, L. Genotyping and follow-up of HR-HPV types detected by self-sampling in women from low socioeconomic groups not participating in regular cervical cancer screening in France. J. Clin. Virol. 2016, 78, 102–107. [Google Scholar] [CrossRef]
- Garcia, F.; Barker, B.; Santos, C.; Brown, E.M.; Nuño, T.; Giuliano, A.; Davis, J. Cross-sectional study of patient- and physician-collected cervical cytology and human papillomavirus. Obstet. Gynecol. 2003, 102, 266–272. [Google Scholar] [CrossRef] [PubMed]
- Szarewski, A.; Cadman, L.; Mesher, D.; Austin, J.; Ashdown-Barr, L.; Edwards, R.; Lyons, D.; Walker, J.; Christison, J.; Frater, A.; et al. HPV self-sampling as an alternative strategy in non-attenders for cervical screening—A randomised controlled trial. Br. J. Cancer 2011, 104, 915–920. [Google Scholar] [CrossRef] [PubMed]
- McSherry, L.A.; Dombrowski, S.U.; Francis, J.J.; Murphy, J.; Martin, C.M.; O’Leary, J.J.; Sharp, L. ‘It’s a can of worms’: Understanding primary care practitioners’ behaviours in relation to HPV using the theoretical domains framework. Implement. Sci. 2012, 7, 73. [Google Scholar] [CrossRef] [PubMed]





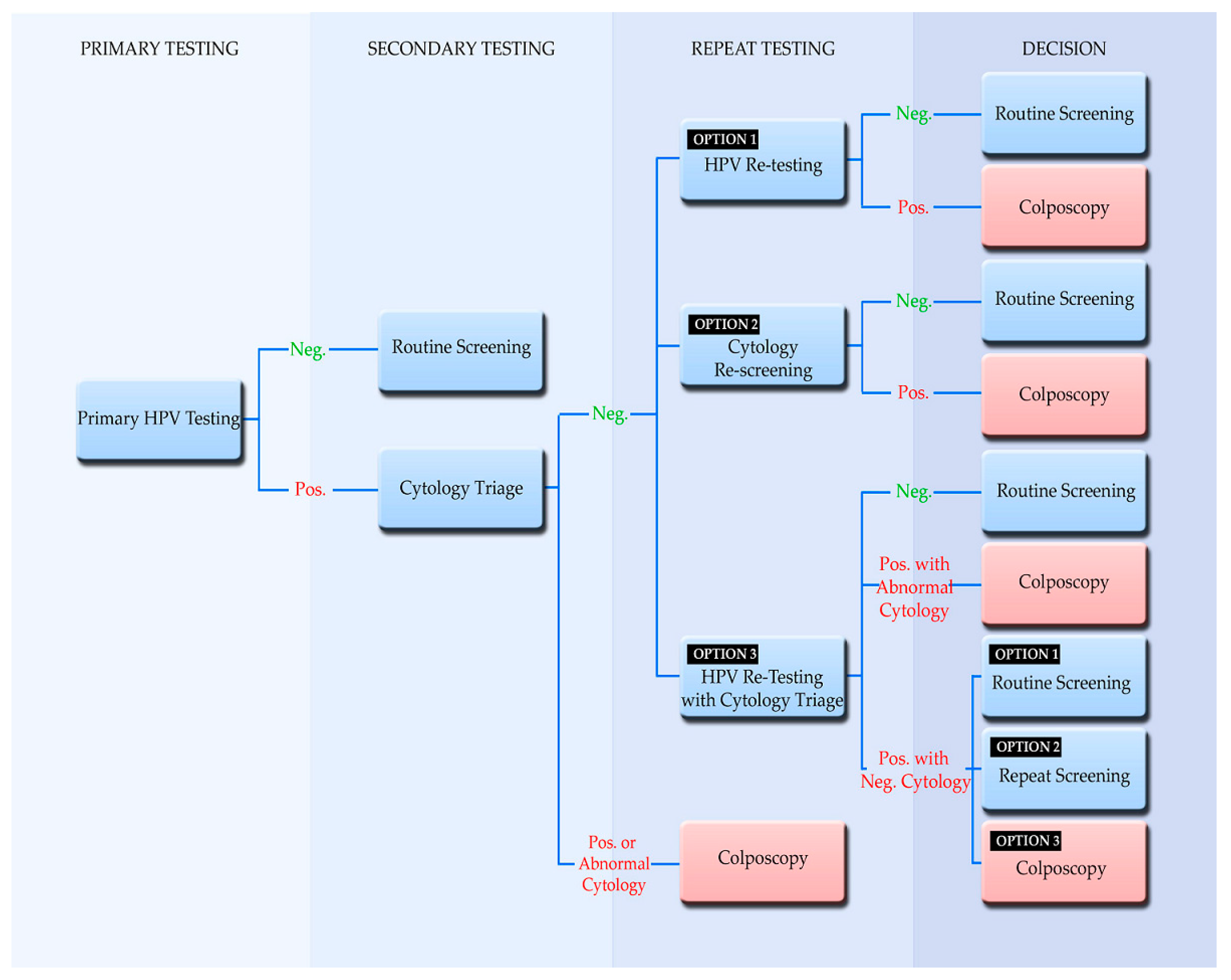{kind=link}
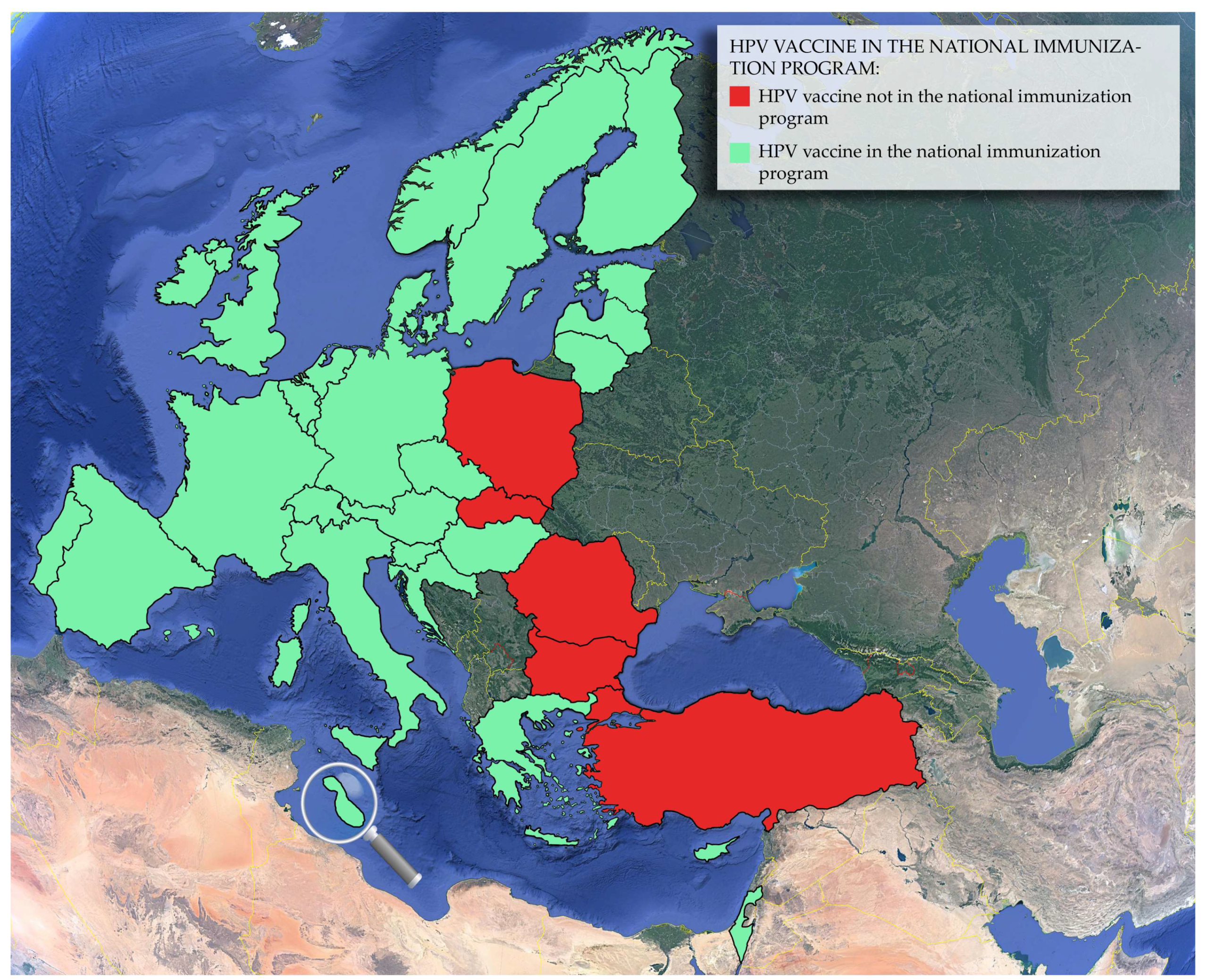{kind=link}
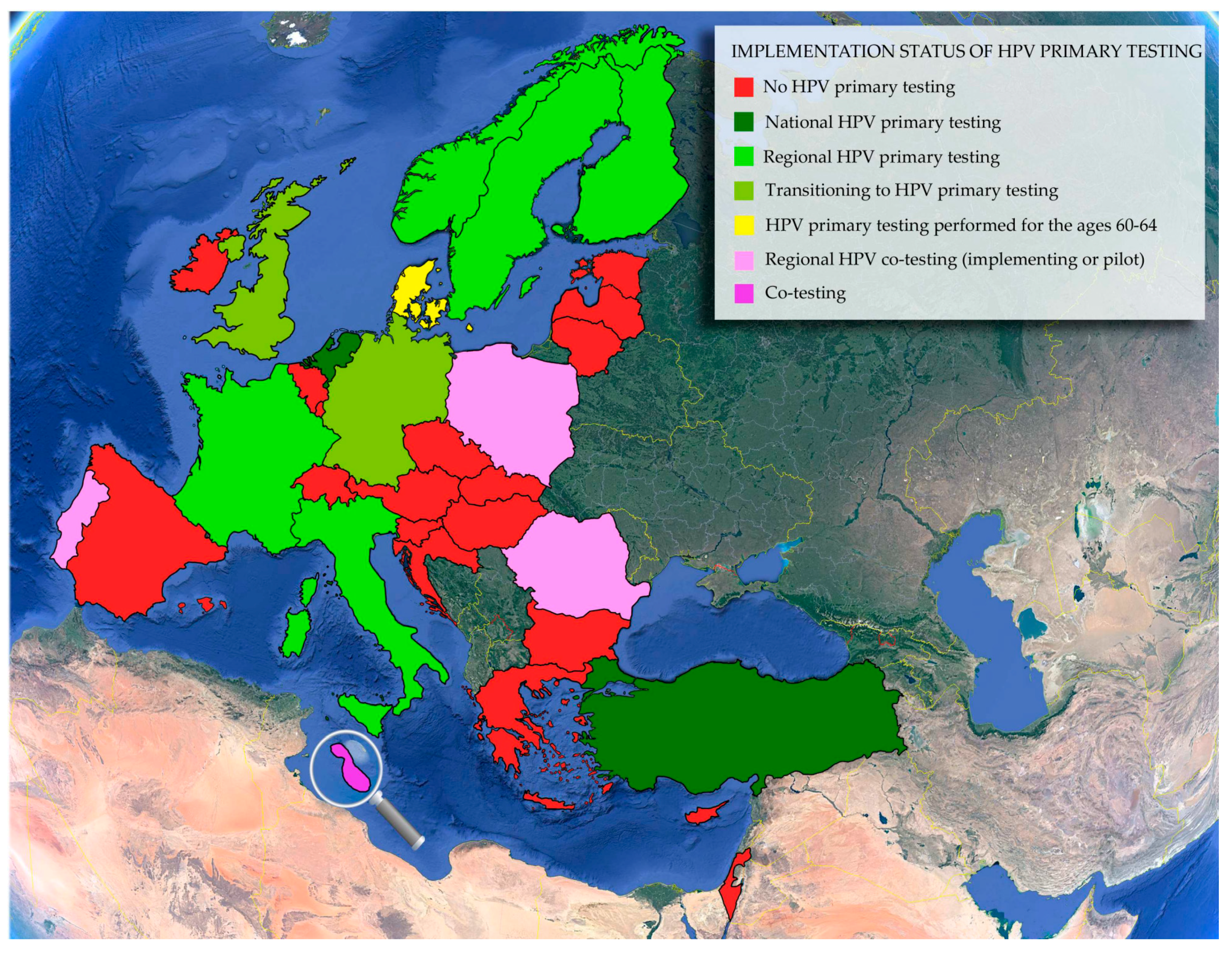{kind=link}
{kind=link}
| Countries | Presence and Type of Cervical Screening Program (Year of Initiation) | Screening Ages (Years) | Screening Interval (Years) | Primary Screening Test Used | Sample Taker | Use of HPV Testing | HPV Vaccine in the National Immunization Program (Year of Initiation) | References |
|---|---|---|---|---|---|---|---|---|
| E.U. Member Countries | ||||||||
| Austria | Opportunistic | 18+ or 2 years after sexual onset | 1 | CC | GYN, GPs | HPV testing funded in certain cases | 2014 | [117,120,124,125,126,127,128,129,130,131] |
| Belgium 1 | Organized population-based, in some regions, roll-out ongoing, 2013 | 25–64 | 3 | CC & LBC | GYN, GPs | HPV triage testing | 2010: Flemish community, 2011: French community | [131,132,133,134,135,136,137,138,139,140,141,142,143] |
| Bulgaria | Opportunistic | N/A | N/A | N/A | GPs | N/A | - | [115,131,144,145,146,147,148] |
| Croatia | Organized population-based, roll-out ongoing, 2012 | 25–64 | 3 | CC | GYN | HPV triage testing, test for cure | 2016 | [115,131,149,150] |
| Cyprus 2 | Opportunistic | N/A | N/A | N/A | GYN | N/A | 2016 | [131,151,152,153,154] |
| Czech Republic | Organized population-based, roll-out ongoing, 2008 | 15+ | 1 | CC | GYN | HPV triage testing | 2012 | [115,131,155,156,157,158,159,160] |
| Denmark | Organized population-based, 2006 | 23–64 | 3 (ages: 23–59); 5 (ages: 60–64) | LBC (ages: 23–59); HPV test (ages: 60–64) | GYN, GPs | HPV primary testing performed for the ages 60–64, HPV triage testing, test for cure | 2009 | [6,131,161,162,163,164,165,166,167,168,169,170,171] |
| Estonia | Organized population-based, 2006 | 30–59 | 5 | CC | GYN, Midwives | Not in use | 2018 | [6,131,172,173,174] |
| Finland 3 | Organized population-based, 1963 | 25/30–60/65 | 5 | CC, HPV test | Midwives, Nurses | HPV primary testing in some regions, HPV triage testing | 2013 | [131,175,176,177,178,179,180,181,182,183,184] |
| France | Transitioning to organized population-based planned for 2018, 1991 | 25–64 | 3 (CC), 5 (HPV test) | CC & LBC (ages: 25–64); HPV test (ages: 30–64) | GYN, GPs, Midwives | HPV primary testing in regional pilot projects, HPV triage testing | 2007 | [6,115,131,142,160,185,186,187,188,189,190,191,192] |
| Germany | Transitioning to organized population-based planned for 2018, 1971 | 20+ | 1 | CC | GYN | HPV primary testing in implementation, HPV triage testing | 2007 | [64,115,131,160,193,194,195,196,197,198,199,200,201] |
| Greece 4 | Opportunistic | Sexual onset | 1 | CC | GYN, GPs | Not in use | 2008 | [128,131,202,203,204,205,206,207] |
| Hungary | Organized population-based, roll-out ongoing, 2003 | 25–65 | 3 | CC | GYN, Primary care personnel | Not in use | 2014 | [6,115,131,208,209,210,211,212,213,214] |
| Ireland | Organized population-based, roll-out ongoing, 2008 | 25–60 | 3 (ages: 25–44); 5 (ages: 45–60) | LBC | Various healthcare providers termed registered smear-takers | HPV triage testing, test for cure | 2010 | [6,115,131,215,216,217,218,219] |
| Italy 3 | Organized population-based, roll-out ongoing, 1989 | 25–64 | 3 (ages: 25–30/35); 5 (ages: 30/35–64) | CC & LBC (ages: 25–30/35); HPV test (ages: 30/34–64) | Midwives, Nurses | HPV primary testing in some regions, HPV triage testing, test for cure | 2008 | [6,115,118,131,220,221,222,223,224,225,226,227] |
| Latvia | Organized population-based, 2009 | 25–69 | 3 | CC | GYN, GPs | Not in use | 2010 | [6,131,228,229,230,231] |
| Lithuania | Organized population-based, roll-out ongoing, 2004 | 25–59 | 3 | CC | GYN, GPs | Not in use | 2016 | [6,67,115,131,232,233] |
| Luxembourg | Opportunistic | 15+ | 1 | LBC | GYN, GPs | HPV triage testing | 2008 | [131,234,235,236,237,238,239] |
| Malta | Organized population-based, (Piloting), 2015 | 25–35 | 3 | CC & HPV test | Doctors, Nurses | Cotesting | 2012 | [67,115,131,159,160,240] |
| Netherlands | Organized population-based, 1970 | 30–64 | 5 | HPV test | GPs, Physicians, Clinicians, Midwives | HPV primary testing, HPV triage testing | 2010 | [87,115,131,241,242,243,244,245,246] |
| Poland | Organized population-based, 2006 | 25–59 | 3 | CC (ages: 25–59); CC & HPV test (ages: 30–59) | GYN, Midwives | Regional pilot for Cotesting, HPV triage testing | - | [6,115,131,160,247,248,249,250] |
| Portugal 3 | Organized population-based, in some regions, roll-out ongoing, 1990 | 25–59 | 3 | CC & LBC | GPs | Cotesting in some regions | 2008 | [115,131,251,252,253,254] |
| Romania 5 | Organized population-based, in some regions, roll-out ongoing, 2012 | 25–64 | 5 | CC & HPV test | GYN, GPs | Cotesting in some regions | - | [115,131,255,256,257,258,259,260] |
| Slovakia | Transitioning to organized population-based, 2008 | 23–64 | Yearly x 2; then 3 yearly | CC | GYN | HPV triage testing | - | [75,115,131,147,159,261,262,263,264] |
| Slovenia | Organized population-based, 2003 | 20–64 | Yearly x 2; then 3 yearly | CC | GYN | HPV triage testing, test of cure | 2009 | [6,115,131,147,160,265,266,267,268] |
| Spain 3 | Opportunistic | 25–65 | 3 | CC | GYN, Nurses, Midwives | HPV triage testing in some regions | 2007 | [92,115,118,131,160,269,270,271,272,273,274,275,276,277,278] |
| Sweden | Organized population-based, 1967 | 23–60 | 3 (ages: 23–50); 5 (ages: 51–60) | HPV test replacing CC & LBC | Midwives | HPV primary testing in some regions HPV triage testing, test for cure | 2012 | [114,115,131,142,279,280,281,282,283,284,285,286] |
| United Kingdom | Organized population-based, 1988 | 25–64 | 3 (ages: 25–49); 5 (ages: 50–64) | HPV test replacing LBC | GYN, GPs, Nurses, Midwives | HPV primary testing in implementation, HPV triage testing, test for cure | 2008 | [115,128,131,287,288,289,290,291,292,293] |
| E.U. Associated Countries | ||||||||
| Norway | Organized population-based, 1995 | 25–69 | 3 | CC & LBC, HPV test | GYN, GPs | Regional pilot for HPV primary testing, HPV triage testing | 2009 | [131,294,295,296,297,298,299] |
| Israel | Opportunistic | 35–54 | 3 | LBC | GYN, Obstetricians | Not in use | 2013 | [121,122,131,300,301,302,303,304] |
| Switzerland | Opportunistic | Sexual onset/21–70 | 2 (ages: Sexual onset/21–29); 3 (ages: 30–70) | CC & LBC | GYN, GPs | HPV triage testing | 2008 | [69,123,131,305,306,307,308,309,310,311] |
| Turkey | Organized population-based, roll-out ongoing, 2004 | 30–65 | 5 | HPV test, CC & LBC, | GYN, Doctors, Nurses | HPV primary testing | - | [131,312,313,314,315,316,317,318,319,320,321] |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chrysostomou, A.C.; Stylianou, D.C.; Constantinidou, A.; Kostrikis, L.G. Cervical Cancer Screening Programs in Europe: The Transition Towards HPV Vaccination and Population-Based HPV Testing. Viruses 2018, 10, 729. https://0-doi-org.brum.beds.ac.uk/10.3390/v10120729
Chrysostomou AC, Stylianou DC, Constantinidou A, Kostrikis LG. Cervical Cancer Screening Programs in Europe: The Transition Towards HPV Vaccination and Population-Based HPV Testing. Viruses. 2018; 10(12):729. https://0-doi-org.brum.beds.ac.uk/10.3390/v10120729
Chicago/Turabian StyleChrysostomou, Andreas C., Dora C. Stylianou, Anastasia Constantinidou, and Leondios G. Kostrikis. 2018. "Cervical Cancer Screening Programs in Europe: The Transition Towards HPV Vaccination and Population-Based HPV Testing" Viruses 10, no. 12: 729. https://0-doi-org.brum.beds.ac.uk/10.3390/v10120729