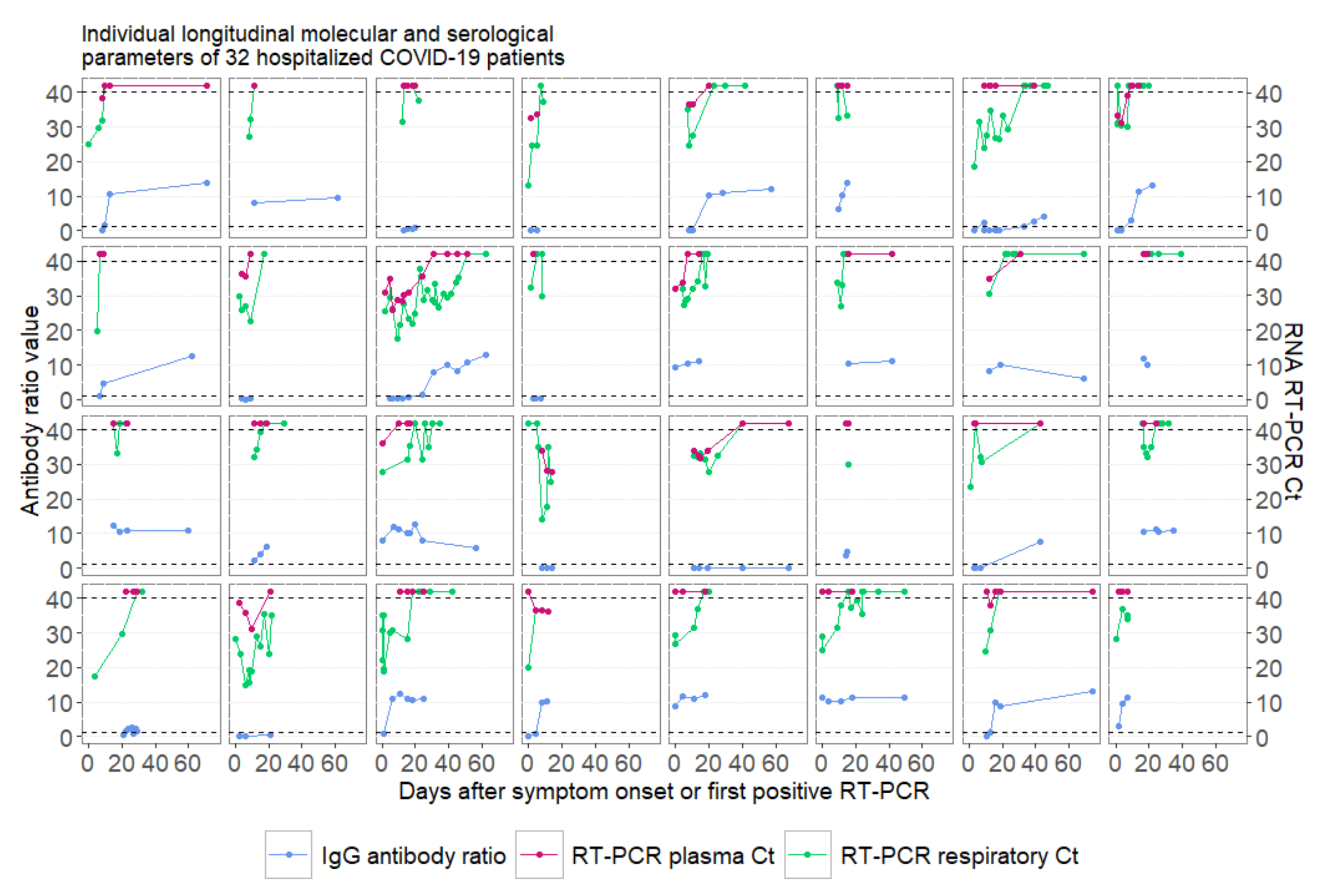
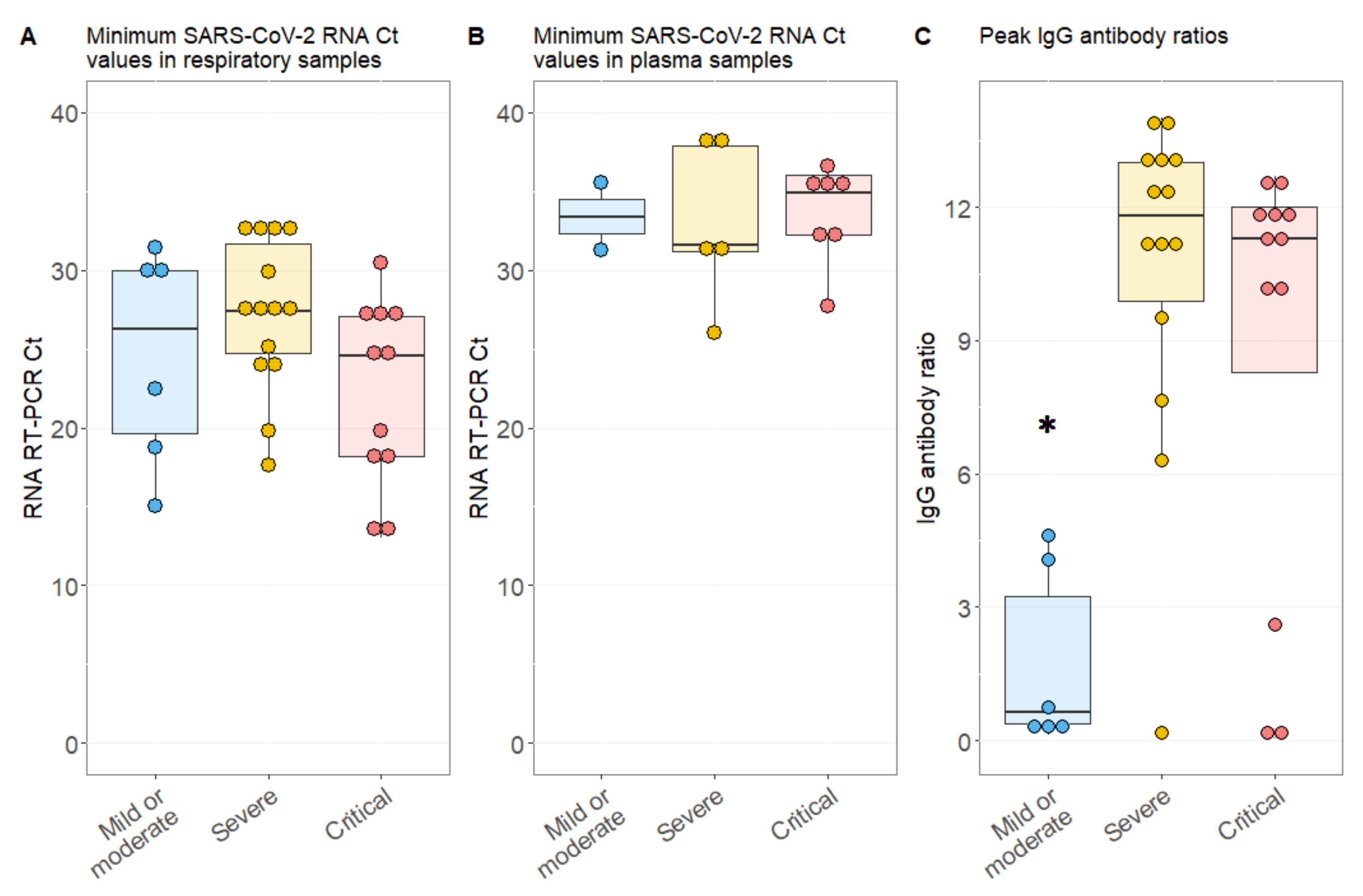
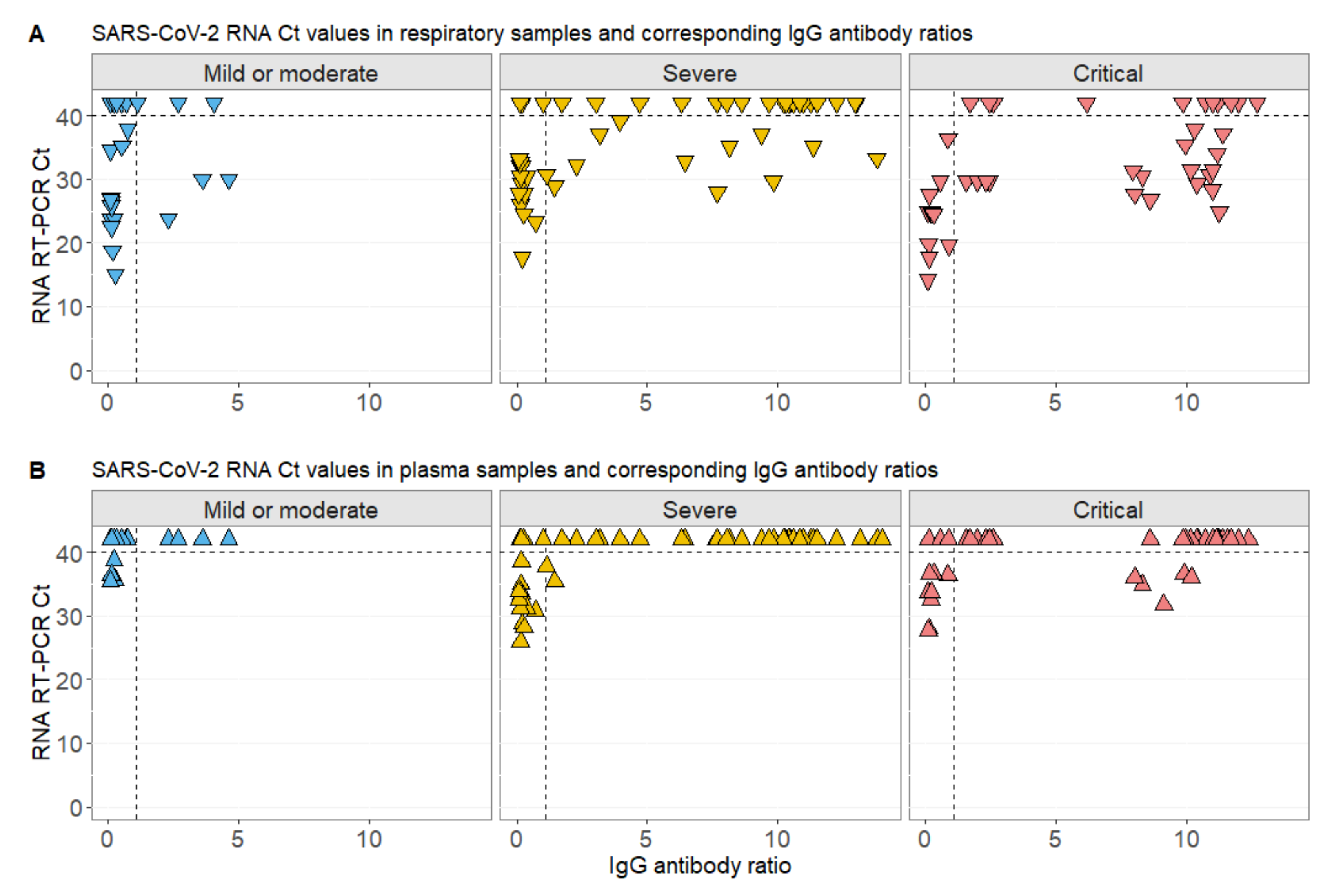
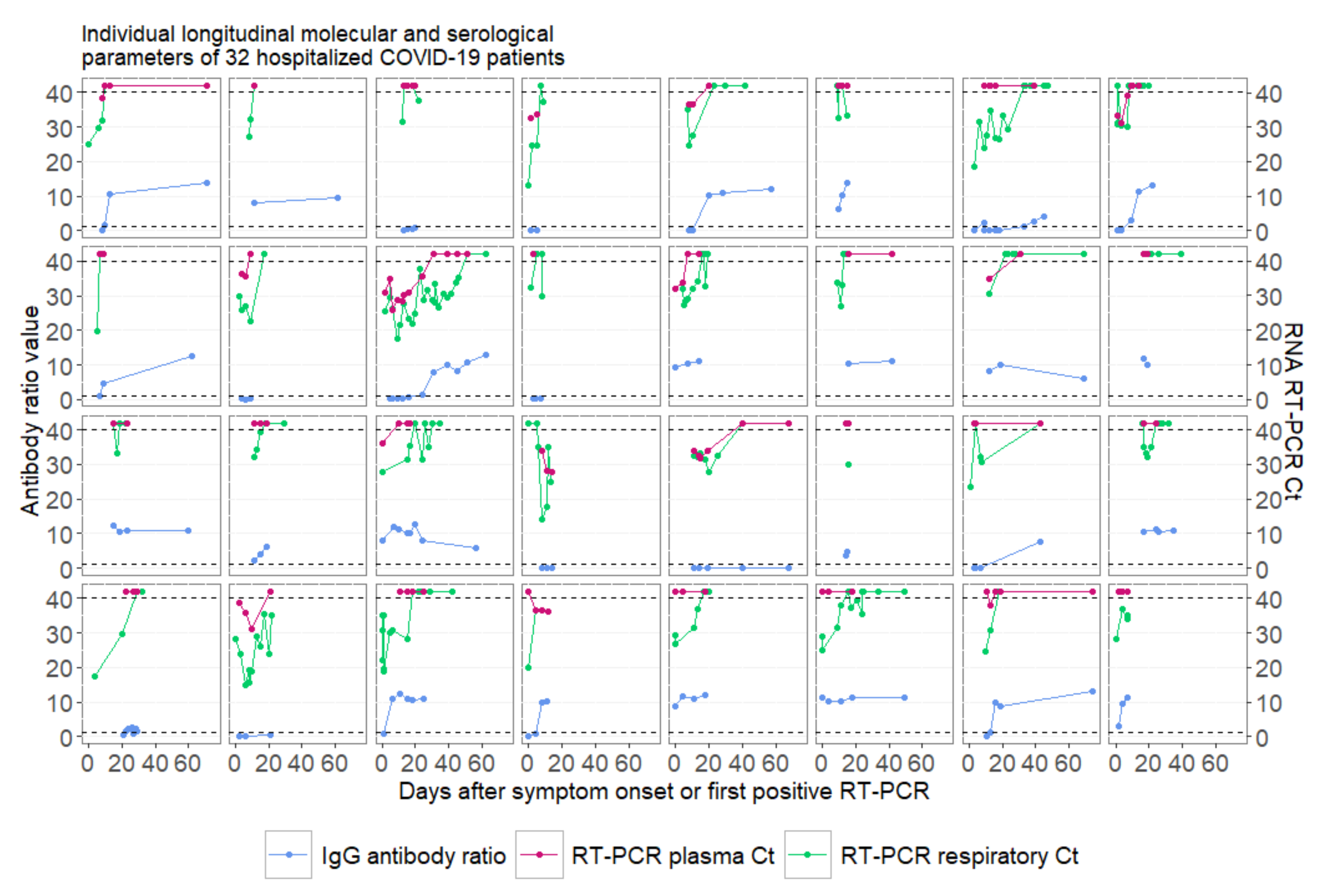
RNAemia Corresponds to Disease Severity and Antibody Response in Hospitalized COVID-19 Patients

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Molecular Detection of SARS-CoV-2 RNA in Respiratory and Plasma Samples
2.3. Detection of SARS-CoV-2 IgG
2.4. Statistical Analysis
3. Results
Patient Characteristics
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- JohnsHopkins. COVID-19 Map. Available online: https://0-coronavirus-jhu-edu.brum.beds.ac.uk/map.html (accessed on 17 September 2020).
- WHO. Laboratory Testing for 2019 Novel Coronavirus (2019-nCoV) in Suspected Human Cases. Available online: https://www.who.int/publications-detail/laboratory-testing-for-2019-novel-coronavirus-in-suspected-human-cases-20200117 (accessed on 17 September 2020).
- Rabaan, A.A.; Al-Ahmed, S.H.; Haque, S.; Sah, R.; Tiwari, R.; Malik, Y.S.; Dhama, K.; Yatoo, M.I.; Bonilla-Aldana, D.K.; Rodriguez-Morales, A.J. SARS-CoV-2, SARS-CoV, and MERS-COV: A comparative overview. Infez. Med. 2020, 28, 174–184. [Google Scholar] [PubMed]
- Chang, L.; Yan, Y.; Wang, L. Coronavirus disease 2019: Coronaviruses and blood safety. Transfus. Med. Rev. 2020. [Google Scholar] [CrossRef] [PubMed]
- Chang, L.; Zhao, L.; Gong, H.; Wang, L. Severe acute respiratory syndrome coronavirus 2 RNA detected in blood donations. Emerg. Infect. Dis. 2020, 26. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- De Jong, M.D.; Bach, V.C.; Phan, T.Q.; Vo, M.H.; Tran, T.T.; Nguyen, B.H.; Beld, M.; Le, T.P.; Truong, H.K.; Nguyen, V.V.; et al. Fatal avian influenza A (H5N1) in a child presenting with diarrhea followed by coma. N. Engl. J. Med. 2005, 352, 686–691. [Google Scholar] [CrossRef] [Green Version]
- De Jong, M.D.; Simmons, C.P.; Thanh, T.T.; Hien, V.M.; Smith, G.J.; Chau, T.N.; Hoang, D.M.; Chau, N.V.; Khanh, T.H.; Dong, V.C.; et al. Fatal outcome of human influenza A (H5N1) is associated with high viral load and hypercytokinemia. Nat. Med. 2006, 12, 1203–1207. [Google Scholar] [CrossRef]
- Desforges, M.; Le Coupanec, A.; Stodola, J.K.; Meessen-Pinard, M.; Talbot, P.J. Human coronaviruses: Viral and cellular factors involved in neuroinvasiveness and neuropathogenesis. Virus Res. 2014, 194, 145–158. [Google Scholar] [CrossRef]
- Gu, J.; Gong, E.; Zhang, B.; Zheng, J.; Gao, Z.; Zhong, Y.; Zou, W.; Zhan, J.; Wang, S.; Xie, Z.; et al. Multiple organ infection and the pathogenesis of SARS. J. Exp. Med. 2005, 202, 415–424. [Google Scholar] [CrossRef]
- Behzad, S.; Aghaghazvini, L.; Radmard, A.R.; Gholamrezanezhad, A. Extrapulmonary manifestations of COVID-19: Radiologic and clinical overview. Clin. Imaging 2020, 66, 35–41. [Google Scholar] [CrossRef]
- Farkash, E.A.; Wilson, A.M.; Jentzen, J.M. Ultrastructural evidence for direct renal infection with SARS-CoV-2. J. Am. Soc. Nephrol. 2020. [Google Scholar] [CrossRef]
- Moccia, F.; Gerbino, A.; Lionetti, V.; Miragoli, M.; Munaron, L.M.; Pagliaro, P.; Pasqua, T.; Penna, C.; Rocca, C.; Samaja, M.; et al. COVID-19-associated cardiovascular morbidity in older adults: A position paper from the Italian society of cardiovascular researches. Geroscience 2020. [Google Scholar] [CrossRef] [PubMed]
- Nörz, D.; Frontzek, A.; Eigner, U.; Oestereich, L.; Fischer, N.; Aepfelbacher, M.; Pfefferle, S.; Lütgehetmann, M. Pushing beyond specifications: Evaluation of linearity and clinical performance of a fully automated SARS-CoV-2 RT-PCR assay for reliable quantification in blood and other materials outside recommendations. medRxiv 2020. [Google Scholar] [CrossRef]
- INSTAND. Available online: https://www.instand-ev.de/ (accessed on 17 September 2020).
- Benjamini, Y.; Hochberg, Y. Controlling the false discovery rate: A practical and powerful approach to multiple testing. J. R. Stat. Soc. Ser. B Methodol. 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Gandhi, R.T.; Lynch, J.B.; Del Rio, C. Mild or moderate Covid-19. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; McGoogan, J.M. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72 314 cases from the Chinese center for disease control and prevention. JAMA 2020. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Zhao, B.; Qu, Y.; Chen, Y.; Xiong, J.; Feng, Y.; Men, D.; Huang, Q.; Liu, Y.; Yang, B.; et al. Detectable serum SARS-CoV-2 viral load (RNAaemia) is closely correlated with drastically elevated interleukin 6 (IL-6) level in critically ill COVID-19 patients. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Wang, W.; Xu, Y.; Gao, R.; Lu, R.; Han, K.; Wu, G.; Tan, W. Detection of SARS-CoV-2 in different types of clinical specimens. JAMA 2020. [Google Scholar] [CrossRef] [Green Version]
- Zheng, S.; Fan, J.; Yu, F.; Feng, B.; Lou, B.; Zou, Q.; Xie, G.; Lin, S.; Wang, R.; Yang, X.; et al. Viral load dynamics and disease severity in patients infected with SARS-CoV-2 in Zhejiang province, China, January-March 2020: Retrospective cohort study. BMJ 2020, 369, m1443. [Google Scholar] [CrossRef] [Green Version]
- Wölfel, R.; Corman, V.M.; Guggemos, W.; Seilmaier, M.; Zange, S.; Müller, M.A.; Niemeyer, D.; Jones, T.C.; Vollmar, P.; Rothe, C.; et al. Virological assessment of hospitalized patients with COVID-2019. Nature 2020, 581, 465–469. [Google Scholar] [CrossRef] [Green Version]
- Veyer, D.; Kernéis, S.; Poulet, G.; Wack, M.; Robillard, N.; Taly, V.; L’Honneur, A.S.; Rozenberg, F.; Laurent-Puig, P.; Bélec, L.; et al. Highly sensitive quantification of plasma SARS-CoV-2 RNA shelds light on its potential clinical value. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Desforges, M.; Le Coupanec, A.; Dubeau, P.; Bourgouin, A.; Lajoie, L.; Dubé, M.; Talbot, P.J. Human coronaviruses and other respiratory viruses: Underestimated opportunistic pathogens of the central nervous system? Viruses 2019, 12, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, X.; Schneider, E.; Jain, S.; Bramley, A.M.; Hymas, W.; Stockmann, C.; Ampofo, K.; Arnold, S.R.; Williams, D.J.; Self, W.H.; et al. Rhinovirus viremia in patients hospitalized with community-acquired pneumonia. J. Infect. Dis. 2017, 216, 1104–1111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halfhide, C.P.; Flanagan, B.F.; Brearey, S.P.; Hunt, J.A.; Fonceca, A.M.; McNamara, P.S.; Howarth, D.; Edwards, S.; Smyth, R.L. Respiratory syncytial virus binds and undergoes transcription in neutrophils from the blood and airways of infants with severe bronchiolitis. J. Infect. Dis. 2011, 204, 451–458. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.K.; Fang, C.T.; Chen, H.L.; Yang, C.F.; Chen, Y.C.; Chen, M.L.; Chen, S.Y.; Yang, J.Y.; Lin, J.H.; Yang, P.C.; et al. Detection of severe acute respiratory syndrome coronavirus RNA in plasma during the course of infection. J. Clin. Microbiol. 2005, 43, 962–965. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grant, P.R.; Garson, J.A.; Tedder, R.S.; Chan, P.K.; Tam, J.S.; Sung, J.J. Detection of SARS coronavirus in plasma by real-time RT-PCR. N. Engl. J. Med. 2003, 349, 2468–2469. [Google Scholar] [CrossRef] [Green Version]
- Ng, E.K.; Hui, D.S.; Chan, K.C.; Hung, E.C.; Chiu, R.W.; Lee, N.; Wu, A.; Chim, S.S.; Tong, Y.K.; Sung, J.J.; et al. Quantitative analysis and prognostic implication of SARS coronavirus RNA in the plasma and serum of patients with severe acute respiratory syndrome. Clin. Chem. 2003, 49, 1976–1980. [Google Scholar] [CrossRef]
- Likos, A.M.; Kelvin, D.J.; Cameron, C.M.; Rowe, T.; Kuehnert, M.J.; Norris, P.J. National Heart, Lung, Blood Institute Retrovirus Epidemiology Donor Study-II (REDS-II). Influenza viremia and the potential for blood-borne transmission. Transfusion 2007, 47, 1080–1088. [Google Scholar] [CrossRef] [Green Version]
- Naficy, K. Human influenza infection with proved viremia. Report of a case. N. Engl. J. Med. 1963, 269, 964–966. [Google Scholar] [CrossRef]
- Khakpour, M.; Saidi, A.; Naficy, K. Proved viraemia in Asian influenza (Hong Kong variant) during incubation period. Br. Med. J. 1969, 4, 208–209. [Google Scholar] [CrossRef] [Green Version]
- Poliakova, T.G.; Ivanova, L.A.; Kniazeva, L.D.; Krylov, V.F.; Demidova, S.A. Virological studies in fatal outcomes in influenza and its complications in adults during the period of influenza A (H3N2) virus circulation from 1969 to 1983. Vopr. Virusol. 1987, 32, 524–528. [Google Scholar]
- Tse, H.; To, K.K.; Wen, X.; Chen, H.; Chan, K.H.; Tsoi, H.W.; Li, I.W.; Yuen, K.Y. Clinical and virological factors associated with viremia in pandemic influenza A/H1N1/2009 virus infection. PLoS ONE 2011, 6, e22534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, S.M.; Xie, H.; Campbell, A.P.; Kuypers, J.; Leisenring, W.; Boudreault, A.A.; Englund, J.A.; Corey, L.; Boeckh, M. Influenza viral RNA detection in blood as a marker to predict disease severity in hematopoietic cell transplant recipients. J. Infect. Dis. 2012, 206, 1872–1877. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, J.; Yuan, Q.; Wang, H.; Liu, W.; Liao, X.; Su, Y.; Wang, X.; Yuan, J.; Li, T.; Li, J.; et al. Antibody responses to SARS-CoV-2 in patients of novel coronavirus disease 2019. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Corman, V.M.; Albarrak, A.M.; Omrani, A.S.; Albarrak, M.M.; Farah, M.E.; Almasri, M.; Muth, D.; Sieberg, A.; Meyer, B.; Assiri, A.M.; et al. Viral shedding and antibody response in 37 patients with middle east respiratory syndrome coronavirus infection. Clin. Infect. Dis. 2016, 62, 477–483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sethuraman, N.; Jeremiah, S.S.; Ryo, A. Interpreting diagnostic tests for SARS-CoV-2. JAMA 2020. [Google Scholar] [CrossRef] [PubMed]
- Bullard, J.; Dust, K.; Funk, D.; Strong, J.E.; Alexander, D.; Garnett, L.; Boodman, C.; Bello, A.; Hedley, A.; Schiffman, Z.; et al. Predicting infectious SARS-CoV-2 from diagnostic samples. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Mild or Moderate Cases, n = 6 (19%) | Severe Cases, n = 14 (44%) | Critical Cases, n = 12 (37%) | p Value | Adjusted p Value | |
|---|---|---|---|---|---|
| Age in years, median (IQR) | 60 (55–65) | 55 (50–66) | 67 (57–76) | 0.273 | |
| Female, n (%) | 5 (83) | 6 (43) | 3 (25) | 0.063 | |
| Detection of viremia, n (%) | 2 (33) | 5 (36) | 7 (58) | 0.434 | |
| Fatal outcome, n (%) | 1 (17) | 0 (0) | 5 (42) | 0.025 * | |
| Leucocytes, median (IQR) | 5.06 (2.79–7.02) | 5.72 (3.82–7.43) | 7.49 (6.71–10.06) | 0.170 | |
| Lymphocytes, median (IQR) | 0.9 (0.62–1.44) | 0.89 (0.80–1.37) | 0.78 (0.54–0.89) | 0.461 | |
| CRP, median (IQR) | 15 (9–80) | 102 (60–193) | 215 (101–263) | 0.009 * | m/s: 0.076 m/c: 0.010 s/c: 0.076 |
| IL-6, median (IQR) | 26 (10–30) | 52 (30–90) | 156 (48–319) | 0.005 * | m/s: 0.035 m/c: 0.015 s/c: 0.035 |
| SARS-CoV-2 Ct in Respiratory Samples | SARS-CoV-2 Ct in Plasma Samples | ||||||
|---|---|---|---|---|---|---|---|
| Random Effect | Patient | Estimate | 95% CI | p Value | Estimate | 95% CI | p Value |
| Fixed Effects | IgG titer | 0.50 | 0.21; 0.81 | 0.002 * | 0.38 | 0.22; 0.55 | <0.001 * |
| Male Female | 1 0.08 | −3.59; 3.73 | 0.968 | 1 −0.76 | −2.64; 1.09 | 0.457 | |
| Age in years | −0.10 | −0.22; 0.02 | 0.128 | −0.04 | −0.10; 0.03 | 0.307 | |
| Days after onset of symptoms or first positive PCR | 0.26 | 0.16; 0.34 | <0.001 * | 0.06 | −0.01; 0.11 | 0.017 * | |
| Severity: mild/moderate Severe Critical | 1 1.54 −3.55 | −3.40; 6.42 −8.95; 1.80 | 0.565 0.232 | 1 −3.26 −4.39 | −5.83; −0.75 −7.19; −1.61 | 0.024 * 0.007 * | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eberhardt, K.A.; Meyer-Schwickerath, C.; Heger, E.; Knops, E.; Lehmann, C.; Rybniker, J.; Schommers, P.; Eichenauer, D.A.; Kurth, F.; Ramharter, M.; et al. RNAemia Corresponds to Disease Severity and Antibody Response in Hospitalized COVID-19 Patients. Viruses 2020, 12, 1045. https://0-doi-org.brum.beds.ac.uk/10.3390/v12091045
Eberhardt KA, Meyer-Schwickerath C, Heger E, Knops E, Lehmann C, Rybniker J, Schommers P, Eichenauer DA, Kurth F, Ramharter M, et al. RNAemia Corresponds to Disease Severity and Antibody Response in Hospitalized COVID-19 Patients. Viruses. 2020; 12(9):1045. https://0-doi-org.brum.beds.ac.uk/10.3390/v12091045
Chicago/Turabian StyleEberhardt, Kirsten Alexandra, Charlotte Meyer-Schwickerath, Eva Heger, Elena Knops, Clara Lehmann, Jan Rybniker, Philipp Schommers, Dennis A. Eichenauer, Florian Kurth, Michael Ramharter, and et al. 2020. "RNAemia Corresponds to Disease Severity and Antibody Response in Hospitalized COVID-19 Patients" Viruses 12, no. 9: 1045. https://0-doi-org.brum.beds.ac.uk/10.3390/v12091045