
The Pivotal Role of Viruses in the Pathogeny of Chronic Lymphocytic Leukemia: Monoclonal (Type 1) IgG K Cryoglobulinemia and Chronic Lymphocytic Leukemia Diagnosis in the Course of a Human Metapneumovirus Infection



Abstract
:1. Introduction
2. Case Presentation
3. Mini-Review and Discussion
3.1. Overview of Oncogenic Viruses
3.2. Viruses in Lymphoproliferative Disorders
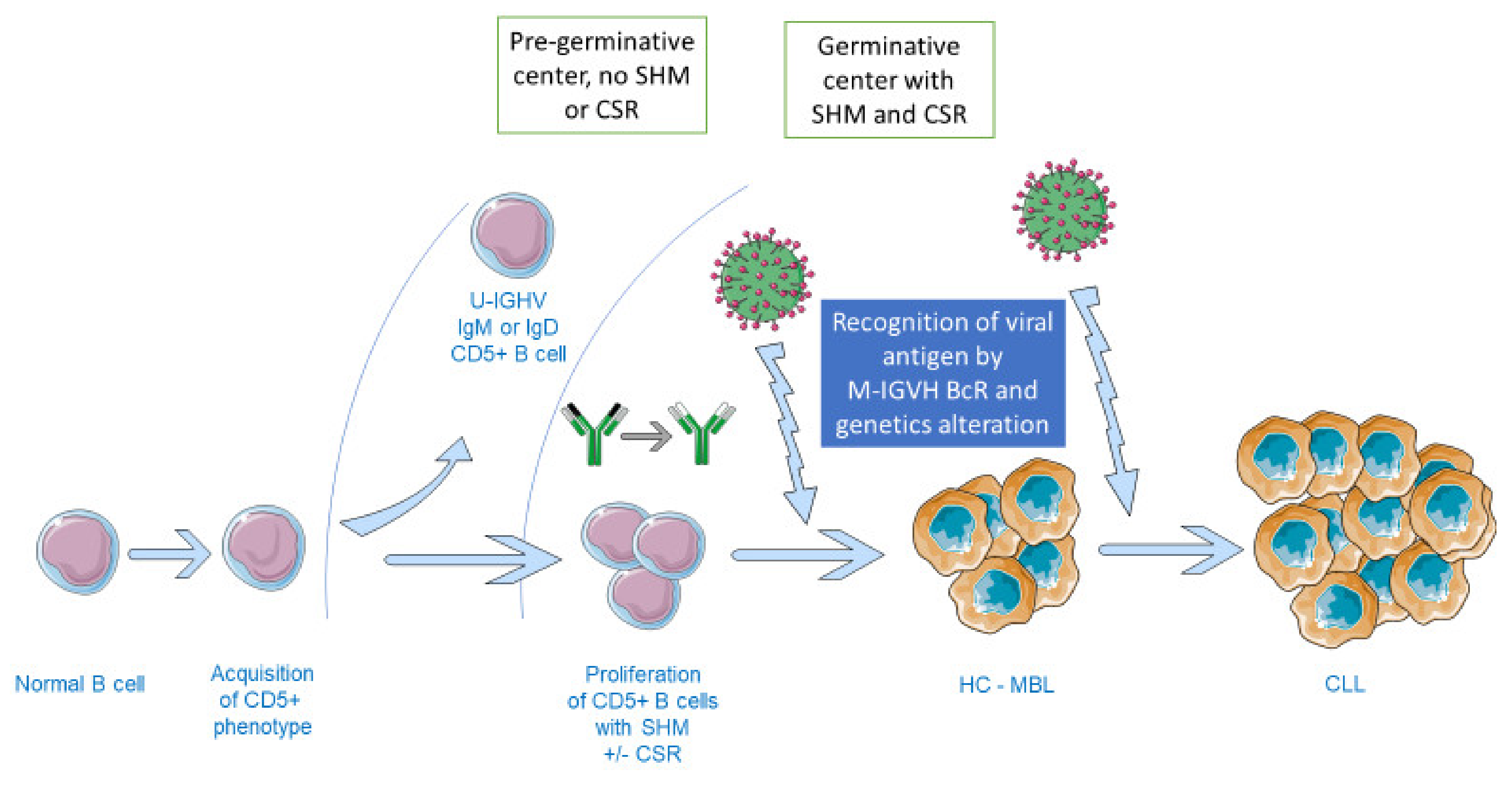
3.3. Pathophysiology of Chronic-Lymphocytic Leukemia and Virus Involvement
3.4. Prognostic Role of Viruses in CLL
3.5. hMPV Involvement in B-Cell Malignancies?
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Ethics Approval and Consent to Participate
Consent for Publication
References
- Roccatello, D.; Saadoun, D.; Ramos-Casals, M.; Tzioufas, A.G.; Fervenza, F.C.; Cacoub, P.; Zignego, A.L.; Ferri, C. Cryoglobulinaemia. Nat. Rev. Dis. Primers 2018, 4. [Google Scholar] [CrossRef] [PubMed]
- Nieto, W.G.; Almeida, J.; Romero, A.; Teodosio, C.; López, A.; Henriques, A.F.; Sánchez, M.L.; Jara-Acevedo, M.; Rasillo, A.; González, M.; et al. Increased Frequency (12%) of Circulating Chronic Lymphocytic Leukemia–like B-Cell Clones in Healthy Subjects Using a Highly Sensitive Multicolor Flow Cytometry Approach. Blood 2009, 114, 33–37. [Google Scholar] [CrossRef] [PubMed]
- Zur Hausen, H.; de Villiers, E.-M. Cancer “Causation” by Infections—Individual Contributions and Synergistic Networks. Semin. Oncol. 2014, 41, 860–875. [Google Scholar] [CrossRef] [PubMed]
- Raab-Traub, N. Novel Mechanisms of EBV-Induced Oncogenesis. Curr. Opin. Virol. 2012, 2, 453–458. [Google Scholar] [CrossRef] [Green Version]
- Levrero, M.; Zucman-Rossi, J. Mechanisms of HBV-Induced Hepatocellular Carcinoma. J. Hepatol. 2016, 64, S84–S101. [Google Scholar] [CrossRef]
- Jia, L.; Gao, Y.; He, Y.; Hooper, J.D.; Yang, P. HBV Induced Hepatocellular Carcinoma and Related Potential Immunotherapy. Pharmacol. Res. 2020, 159, 104992. [Google Scholar] [CrossRef]
- Goossens, N.; Hoshida, Y. Hepatitis C Virus-Induced Hepatocellular Carcinoma. Clin. Mol. Hepatol. 2015, 21, 105. [Google Scholar] [CrossRef]
- Defrancesco, I.; Zerbi, C.; Rattotti, S.; Merli, M.; Bruno, R.; Paulli, M.; Arcaini, L. HCV Infection and Non-Hodgkin Lymphomas: An Evolving Story. Clin. Exp. Med. 2020, 20, 321–328. [Google Scholar] [CrossRef]
- Schiffman, M.; Doorbar, J.; Wentzensen, N.; de Sanjosé, S.; Fakhry, C.; Monk, B.J.; Stanley, M.A.; Franceschi, S. Carcinogenic Human Papillomavirus Infection. Nat. Rev. Dis Primers 2016, 2, 16086. [Google Scholar] [CrossRef]
- Matsuoka, M.; Jeang, K.-T. Human T-Cell Leukaemia Virus Type 1 (HTLV-1) Infectivity and Cellular Transformation. Nat. Rev. Cancer 2007, 7, 270–280. [Google Scholar] [CrossRef]
- Schulz, T.F.; Cesarman, E. Kaposi Sarcoma-Associated Herpesvirus: Mechanisms of Oncogenesis. Curr. Opin. Virol. 2015, 14, 116–128. [Google Scholar] [CrossRef] [PubMed]
- Wendzicki, J.A.; Moore, P.S.; Chang, Y. Large T and Small T Antigens of Merkel Cell Polyomavirus. Curr. Opin. Virol. 2015, 11, 38–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krump, N.A.; You, J. Molecular Mechanisms of Viral Oncogenesis in Humans. Nat. Rev. Microbiol. 2018, 16, 684–698. [Google Scholar] [CrossRef] [PubMed]
- Gross, L. The Search for Viruses as Etiological Agents in Leukemia and Malignant Lymphomas: The Role of the Happy Accident and the Prepared Mind. Cancer Res. 1980, 40, 3405–3407. [Google Scholar] [PubMed]
- Epstein, M.A.; Achong, B.G.; Barr, Y.M. Virus Particles in Cultured Lymphoblasts from Burkitt’s Lymphoma. Lancet 1964, 283, 702–703. [Google Scholar] [CrossRef]
- Carbone, A.; Gloghini, A.; Dotti, G. EBV-Associated Lymphoproliferative Disorders: Classification and Treatment. Oncologust 2008, 13, 577–585. [Google Scholar] [CrossRef] [PubMed]
- Ok, C.Y.; Li, L.; Xu-Monette, Z.Y.; Visco, C.; Tzankov, A.; Manyam, G.C.; Montes-Moreno, S.; Dybkaer, K.; Dybaer, K.; Chiu, A.; et al. Prevalence and Clinical Implications of Epstein-Barr Virus Infection in de Novo Diffuse Large B-Cell Lymphoma in Western Countries. Clin. Cancer Res. 2014, 20, 2338–2349. [Google Scholar] [CrossRef] [Green Version]
- Ambinder, R.F. Epstein-Barr Virus-Associated Lymphoproliferative Disorders. Rev. Clin. Exp. Hematol. 2003, 7, 362–374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farrell, P.J. Epstein–Barr Virus and Cancer. Annu. Rev. Pathol. Mech. Dis. 2019, 14, 29–53. [Google Scholar] [CrossRef]
- Dai, B.; Chen, A.Y.; Corkum, C.P.; Peroutka, R.J.; Landon, A.; Houng, S.; Muniandy, P.A.; Zhang, Y.; Lehrmann, E.; Mazan-Mamczarz, K.; et al. Hepatitis C Virus Upregulates B-Cell Receptor Signaling: A Novel Mechanism for HCV-Associated B-Cell Lymphoproliferative Disorders. Oncogene 2016, 35, 2979–2990. [Google Scholar] [CrossRef]
- Ren, W.; Ye, X.; Su, H.; Li, W.; Liu, D.; Pirmoradian, M.; Wang, X.; Zhang, B.; Zhang, Q.; Chen, L.; et al. Genetic Landscape of Hepatitis B Virus–Associated Diffuse Large B-Cell Lymphoma. Blood 2018, 131, 2670–2681. [Google Scholar] [CrossRef] [PubMed]
- Chiorazzi, N.; Rai, K.R.; Ferrarini, M. Chronic Lymphocytic Leukemia. N. Engl J. Med. 2005, 352, 804–815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raval, A.; Byrd, J.C.; Plass, C. Epigenetics in Chronic Lymphocytic Leukemia. Semin. Oncol. 2006, 33, 157–166. [Google Scholar] [CrossRef]
- Delgado, J.; Nadeu, F.; Colomer, D.; Campo, E. Chronic Lymphocytic Leukemia: From Molecular Pathogenesis to Novel Therapeutic Strategies. Haematologica 2020, 105, 2205–2217. [Google Scholar] [CrossRef] [PubMed]
- Strati, P.; Shanafelt, T.D. Monoclonal B-Cell Lymphocytosis and Early-Stage Chronic Lymphocytic Leukemia: Diagnosis, Natural History, and Risk Stratification. Blood 2015, 126, 454–462. [Google Scholar] [CrossRef]
- Pontoriero, M.; Fiume, G.; Vecchio, E.; de Laurentiis, A.; Albano, F.; Iaccino, E.; Mimmi, S.; Pisano, A.; Agosti, V.; Giovannone, E.; et al. Activation of NF-ΚB in B Cell Receptor Signaling through Bruton’s Tyrosine Kinase-Dependent Phosphorylation of IκB-α. J. Mol. Med. 2019, 97, 675–690. [Google Scholar] [CrossRef]
- Vecchio, E.; Golino, G.; Pisano, A.; Albano, F.; Falcone, C.; Ceglia, S.; Iaccino, E.; Mimmi, S.; Fiume, G.; Giurato, G.; et al. IBTK Contributes to B-Cell Lymphomagenesis in Eμ-Myc Transgenic Mice Conferring Resistance to Apoptosis. Cell Death Dis. 2019, 10, 320. [Google Scholar] [CrossRef]
- South, A.P.; Cho, R.J.; Aster, J.C. The Double-Edged Sword of Notch Signaling in Cancer. Semin. Cell Dev. Biol. 2012, 23, 458–464. [Google Scholar] [CrossRef] [Green Version]
- Damle, R.N.; Wasil, T.; Fais, F.; Ghiotto, F.; Valetto, A.; Allen, S.L.; Buchbinder, A.; Budman, D.; Dittmar, K.; Kolitz, J.; et al. Ig V Gene Mutation Status and CD38 Expression As Novel Prognostic Indicators in Chronic Lymphocytic Leukemia. Blood 1999, 94, 1840–1847. [Google Scholar] [CrossRef]
- Kipps, T.J.; Stevenson, F.K.; Wu, C.J.; Croce, C.M.; Packham, G.; Wierda, W.G.; O’Brien, S.; Gribben, J.; Rai, K. Chronic Lymphocytic Leukaemia. Nat. Rev. Dis. Primers 2017, 3, 16096. [Google Scholar] [CrossRef] [Green Version]
- Gemenetzi, K.; Agathangelidis, A.; Zaragoza-Infante, L.; Sofou, E.; Papaioannou, M.; Chatzidimitriou, A.; Stamatopoulos, K. B Cell Receptor Immunogenetics in B Cell Lymphomas: Immunoglobulin Genes as Key to Ontogeny and Clinical Decision Making. Front. Oncol. 2020, 10, 67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moysiadis, T.; Baliakas, P.; Rossi, D.; Catherwood, M.; Strefford, J.C.; Delgado, J.; Anagnostopoulos, A.; Belessi, C.; Stavroyianni, N.; Pospisilova, S.; et al. Different Time-Dependent Changes of Risk for Evolution in Chronic Lymphocytic Leukemia with Mutated or Unmutated Antigen B Cell Receptors. Leukemia 2019, 33, 1801–1805. [Google Scholar] [CrossRef] [PubMed]
- Mimmi, S.; Vecchio, E.; Iaccino, E.; Rossi, M.; Lupia, A.; Albano, F.; Chiurazzi, F.; Fiume, G.; Pisano, A.; Ceglia, S.; et al. Evidence of Shared Epitopic Reactivity among Independent B-Cell Clones in Chronic Lymphocytic Leukemia Patients. Leukemia 2016, 30, 2419–2422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agathangelidis, A.; Darzentas, N.; Hadzidimitriou, A.; Brochet, X.; Murray, F.; Yan, X.-J.; Davis, Z.; van Gastel-Mol, E.J.; Tresoldi, C.; Chu, C.C.; et al. Stereotyped B-Cell Receptors in One-Third of Chronic Lymphocytic Leukemia: A Molecular Classification with Implications for Targeted Therapies. Blood 2012, 119, 4467–4475. [Google Scholar] [CrossRef] [PubMed]
- Agathangelidis, A.; Psomopoulos, F.; Stamatopoulos, K. Stereotyped B Cell Receptor Immunoglobulins in B Cell Lymphomas. Methods Mol. Biol. 2019, 1956, 139–155. [Google Scholar] [CrossRef] [PubMed]
- Messmer, B.T.; Albesiano, E.; Efremov, D.G.; Ghiotto, F.; Allen, S.L.; Kolitz, J.; Foa, R.; Damle, R.N.; Fais, F.; Messmer, D.; et al. Multiple Distinct Sets of Stereotyped Antigen Receptors Indicate a Role for Antigen in Promoting Chronic Lymphocytic Leukemia. J. Exp. Med. 2004, 200, 519–525. [Google Scholar] [CrossRef]
- Kostareli, E.; Gounari, M.; Janus, A.; Murray, F.; Brochet, X.; Giudicelli, V.; Pospisilova, S.; Oscier, D.; Foroni, L.; di Celle, P.F.; et al. Antigen Receptor Stereotypy across B-Cell Lymphoproliferations: The Case of IGHV4-59/IGKV3-20 Receptors with Rheumatoid Factor Activity. Leukemia 2012, 26, 1127–1131. [Google Scholar] [CrossRef]
- Tsimberidou, A.-M.; Keating, M.J.; Bueso-Ramos, C.E.; Kurzrock, R. Epstein-Barr Virus in Patients with Chronic Lymphocytic Leukemia: A Pilot Study. Leuk. Lymphoma 2006, 47, 827–836. [Google Scholar] [CrossRef]
- Hwang, K.-K.; Trama, A.M.; Kozink, D.M.; Chen, X.; Wiehe, K.; Cooper, A.J.; Xia, S.-M.; Wang, M.; Marshall, D.J.; Whitesides, J.; et al. IGHV1-69 B Cell Chronic Lymphocytic Leukemia Antibodies Cross-React with HIV-1 and Hepatitis C Virus Antigens as Well as Intestinal Commensal Bacteria. PLoS ONE 2014, 9, e90725. [Google Scholar] [CrossRef]
- García-Barchino, M.J.; Sarasquete, M.E.; Panizo, C.; Morscio, J.; Martinez, A.; Alcoceba, M.; Fresquet, V.; Gonzalez-Farre, B.; Paiva, B.; Young, K.H.; et al. Richter Transformation Driven by Epstein-Barr Virus Reactivation during Therapy-Related Immunosuppression in Chronic Lymphocytic Leukaemia: EBV in CLL Transformation to DLBCL. J. Pathol. 2018, 245, 61–73. [Google Scholar] [CrossRef]
- Ng, P.P.; Kuo, C.-C.; Wang, S.; Einav, S.; Arcaini, L.; Paulli, M.; Portlock, C.S.; Marcotrigiano, J.; Tarr, A.; Ball, J.; et al. B-Cell Receptors Expressed by Lymphomas of Hepatitis C Virus (HCV)-Infected Patients Rarely React with the Viral Proteins. Blood 2014, 123, 1512–1515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Minuk, G.Y.; Lerner, B.; Gibson, S.B.; Johnston, J.B.; Uhanova, J.; Andonov, A.; Wu, J. Hepatitis B and Hepatitis C Viral Infections in Patients with Chronic Lymphocytic Leukemia. Can. J. Gastroenterol. Hepatol. 2014, 28, 131–134. [Google Scholar] [CrossRef] [PubMed]
- Liang, J.-H.; Gao, R.; Dai, J.-C.; Gale, R.P.; Li, W.; Fan, L.; Hu, Z.-B.; Xu, W.; Li, J.-Y. The Prognostic Role of HBV Infection in Chronic Lymphocytic Leukemia. J. Cancer Res. Clin. Oncol. 2018, 144, 1309–1315. [Google Scholar] [CrossRef] [PubMed]
- Tadmor, T.; Aviv, A.; Polliack, A. Merkel Cell Carcinoma, Chronic Lymphocytic Leukemia and Other Lymphoproliferative Disorders: An Old Bond with Possible New Viral Ties. Ann. Oncol. 2011, 22, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Bloom, R.; Amber, K.T.; Nouri, K. An Increased Risk of Non-Hodgkin Lymphoma and Chronic Lymphocytic Leukemia in US Patients with Merkel Cell Carcinoma versus Australian Patients: A Clinical Clue to a Different Mechanism of Pathogenesis? Australas. J. Derm. 2016, 57, e114–e116. [Google Scholar] [CrossRef] [PubMed]
- Toracchio, S.; Foyle, A.; Sroller, V.; Reed, J.A.; Wu, J.; Kozinetz, C.A.; Butel, J.S. Lymphotropism of Merkel Cell Polyomavirus Infection, Nova Scotia, Canada. Emerg. Infect. Dis. 2010, 16, 1702–1709. [Google Scholar] [CrossRef]
- Haugg, A.M.; Speel, E.-J.M.; Pantulu, N.D.; Pallasch, C.; Kurz, A.K.; Kvasnicka, H.M.; Cathomas, G.; Wendtner, C.-M.; Hausen, A. zur Fluorescence in Situ Hybridization Confirms the Presence of Merkel Cell Polyomavirus in Chronic Lymphocytic Leukemia Cells. Blood 2011, 117, 5776–5777. [Google Scholar] [CrossRef] [Green Version]
- Tolstov, Y.L.; Arora, R.; Scudiere, S.C.; Busam, K.; Chaudhary, P.M.; Chang, Y.; Moore, P.S. Lack of Evidence for Direct Involvement of Merkel Cell Polyomavirus (MCV) in Chronic Lymphocytic Leukemia (CLL). Blood 2010, 115, 4973–4974. [Google Scholar] [CrossRef]
- Osterhaus, A.; Fouchier, R. Human Metapneumovirus in the Community. Lancet 2003, 361, 890–891. [Google Scholar] [CrossRef]
- Céspedes, P.F.; Palavecino, C.E.; Kalergis, A.M.; Bueno, S.M. Modulation of Host Immunity by the Human Metapneumovirus. Clin. Microbiol. Rev. 2016, 29, 795–818. [Google Scholar] [CrossRef] [Green Version]
- Hijano, D.R.; Maron, G.; Hayden, R.T. Respiratory Viral Infections in Patients with Cancer or Undergoing Hematopoietic Cell Transplant. Front. Microbiol. 2018, 9, 3097. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| 2015—Peripheral Neuropathy Diagnosis | 2019—Hospitalization Day 0. hMPV Infection Diagnosis | 2019—Hospitalisation Day 5. CLL Diagnosis | 2019—Hospitalization Day 13 | 2019—Hospitalization Day 15. Type-1 IgG K Cryoglobulin Diagnosis | 2019—Hospitalization Day 41. Discharge | 2019—4 Months after Discharge | |
|---|---|---|---|---|---|---|---|
| Lymphocyte count (×109/L) | 0.87 | 1.16 | 10.86 | 12.39 | 5.8 | 7.36 | 11.1 |
| Platelet count (×109/L) | 180 | 189 | 386 | 467 | 334 | 237 | 412 |
| Hemoglobin level (g/dL) | 13.5 | 13.9 | 13.9 | 13.6 | 13 | 12 | 12.4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barben, J.; Putot, A.; Mihai, A.-M.; Vovelle, J.; Manckoundia, P. The Pivotal Role of Viruses in the Pathogeny of Chronic Lymphocytic Leukemia: Monoclonal (Type 1) IgG K Cryoglobulinemia and Chronic Lymphocytic Leukemia Diagnosis in the Course of a Human Metapneumovirus Infection. Viruses 2021, 13, 115. https://0-doi-org.brum.beds.ac.uk/10.3390/v13010115
Barben J, Putot A, Mihai A-M, Vovelle J, Manckoundia P. The Pivotal Role of Viruses in the Pathogeny of Chronic Lymphocytic Leukemia: Monoclonal (Type 1) IgG K Cryoglobulinemia and Chronic Lymphocytic Leukemia Diagnosis in the Course of a Human Metapneumovirus Infection. Viruses. 2021; 13(1):115. https://0-doi-org.brum.beds.ac.uk/10.3390/v13010115
Chicago/Turabian StyleBarben, Jérémy, Alain Putot, Anca-Maria Mihai, Jérémie Vovelle, and Patrick Manckoundia. 2021. "The Pivotal Role of Viruses in the Pathogeny of Chronic Lymphocytic Leukemia: Monoclonal (Type 1) IgG K Cryoglobulinemia and Chronic Lymphocytic Leukemia Diagnosis in the Course of a Human Metapneumovirus Infection" Viruses 13, no. 1: 115. https://0-doi-org.brum.beds.ac.uk/10.3390/v13010115