
SARS-CoV-2 Infection and C-Section: A Prospective Observational Study

 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Participants
2.3. Recorded Information
2.4. Statistical Analysis
3. Results
3.1. Results for the Entire SARS-CoV-2-Infected Cohort
3.1.1. General Data
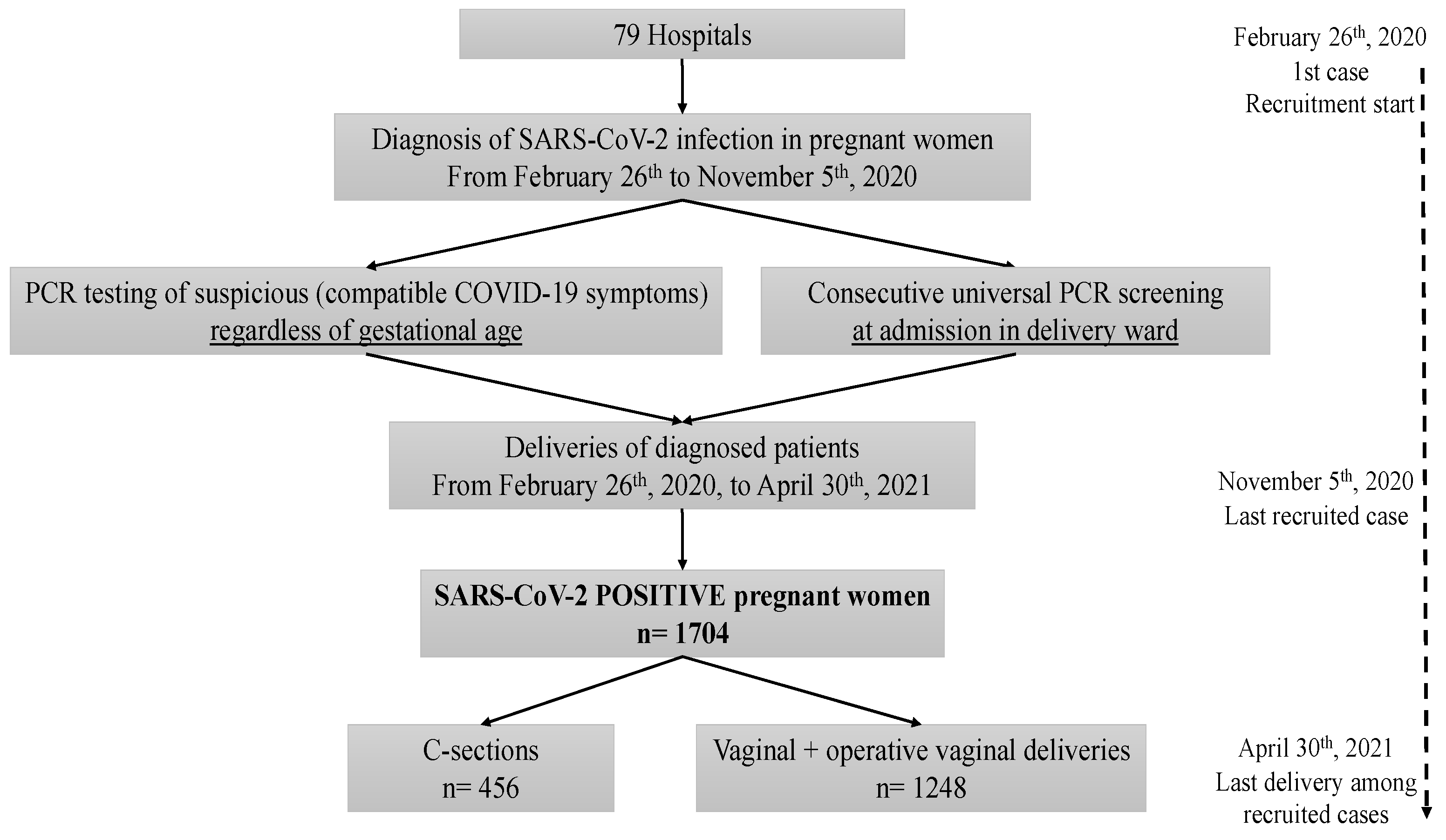
- During the study period, a total of 1704 pregnant women with SARS-CoV-2 infection were diagnosed, either because of suspicious symptoms or during admission to the delivery room.
- Of the 1704 SARS-CoV-2 positive women, 26.8% (456/1704) underwent a C-section and 73.2% (1248/1704) delivered vaginally, either via vaginal (1071, 62.9%) or operative vaginal (177, 10.4%) deliveries (Figure 1).
3.1.2. Baseline Characteristics, Maternal Comorbidities and Pregnancy Characteristics
- The maternal age of the women who underwent a C-section was statistically higher than the group of women who delivered vaginally (p < 0.001); of the former, up to 44.3% were older than 35 years (Table 1).
- A higher proportion of nulliparous and smokers was observed in the C-section group (Table 1).
- A higher proportion of pregnant women with comorbidities (obesity, thrombophilia, chronic kidney disease and diabetes mellitus) was observed among those who underwent a C-section (Table 1).
- There were significantly more IVF and multiple pregnancies observed in the C-section group (Table 1), in addition to more cases of intrauterine growth restrictions and gestational hypertension (p = 0.002 and p < 0.001, respectively).
- A total of 8.2% of women in the C-section group were classified as high risk for pre-eclampsia (by screening at 11–14 weeks of gestation) compared to 5.3% of women who delivered vaginally (p = 0.038, Table 1).
3.1.3. Gestational Age at the Moment of SARS-CoV-2 Infection Diagnosis
- Of the 1704 SARS-CoV-2-positive women in our cohort, 92 (5.4%) were diagnosed with SARS-CoV-2 infection in the first trimester of gestation, 292 (17.1%) in the second trimester and 1320 (77.5%) in the third trimester.
- The rates of C-sections among patients who were diagnosed in the first, second and third trimester of gestation were 16.35% (15/92), 24.7% (72/292) and 28.0% (369/1320), respectively, with the risk of a cesarean section being significantly higher when the infection took place late in pregnancy (p = 0.034).
3.1.4. Maternal and Neonatal Outcomes
- Gestational age at delivery was significantly lower among women who underwent a C-section (p < 0.001, Table 2), with higher rates of preterm delivery (<37 weeks of gestational age) in this group (23.5% vs. 6.3% of patients who delivered vaginally, p < 0.001).
- There were two cases of maternal death among the patients of the C-section group, both of which were associated with disseminated intravascular coagulation, and none in the vaginal delivery group (p = 0.071).
- Higher rates of newborns with low Apgar scores, low umbilical artery pH and NICU admissions were observed in the C-section group (Table 2).
3.2. Results for the Third Trimester Infections
3.2.1. COVID-19 Symptomatology and Delivery Characteristics
- More than a third of the patients had labor induced regardless of COVID-19 symptomatology (Table 3) and only 38.4% of patients who developed pneumonia had a spontaneous onset.
- The type of delivery varied according to COVID-19 symptomatology: the proportions of C-sections among the asymptomatic patients, the ones who had COVID-19 mild–moderate symptoms and the ones who developed pneumonia were 23.5, 28.1 and 40.8%, respectively (p < 0.001, Table 3).
- Among the patients who underwent a C-section (a total of 369), 38 (10.3%) were admitted to the ICU, whereas only 0.6% of patients who delivered vaginally (6/951) needed intensive care (p < 0.001).
- Regarding Robson’s classification of C-sections, there was a higher proportion of patients belonging to the 4th (multiparous without previous C-section, singleton pregnancy with cephalic presentation, ≥37 weeks’ gestation) and the 10th (singleton pregnancy with cephalic presentation, <37 weeks’ gestation, including those who had one or more previous C-section) categories among those who developed pneumonia (Table 3).
- Of the patients who developed pneumonia, underwent a C-section and belonged to Robson’s fourth category, 77.8% had an induced labor and 22.2% had a programmed C-section.
- Only 17.9% (17/95) of patients with pneumonia and who underwent a C-section had a spontaneous onset of labor.
- The highest proportion of asymptomatic patients who underwent a C-section belonged to Robson’s second category (24.7%: nulliparous women, singleton pregnancy with cephalic presentation, ≥37 weeks’ gestation, induced labor or programmed C-section) and mild–moderate symptomatic patients to the fifth category (22.5%: multiparous women with previous C-section, singleton pregnancy with cephalic presentation, ≥37 weeks’ gestation, spontaneous onset of labor).
- Nearly one-third of patients who developed pneumonia and underwent a C-section were admitted to the ICU (30/95, 31.6%); from these, 66.7% (20/30) underwent a C-section before ICU admission and 33.3% (10/30) afterward (Table 3).
3.2.2. Description of C-Sections by Gestational Age at Delivery
- Nearly 25% (89/369) of all C-sections (registered in mothers that were infected with SARS-CoV-2 in the third trimester of gestation) took place before the 37th week of gestation; of these, up to 76.4% (68/89) belonged to Robson’s 10th category (singletons pregnancies < 37 weeks with cephalic presentation, with or without previous C-sections).
- The C-section rate decreased as gestational age at delivery increased (and vice versa) (Table 4, p < 0.001).
- The main reason for C-section in very early preterms (<33 weeks of gestation) was COVID-19 worsening or complication and, as gestational age advanced, these were due to obstetric conditions (Table 4, p < 0.001).
- Up to 25% (70/279) of C-sections at term were due to induction failure or programmed C-section in nulliparous women (Robson’s second category) and nearly 20% (51/279) were due to the same reasons but in multiparous women (Robson’s fourth category).
3.3. Multivariable Analysis of Risk Factors for Undergoing a C-Section
- The multivariable logistic regression modeling results (Table 5) corroborated that the following conditions significantly increased the risk of C-section in SARS-CoV-2-infected mothers: being an IVF pregnancy, being diagnosed with a SARS-CoV-2 infection in the third trimester of gestation, prematurity in mothers with COVID-19 pneumonia (although both conditions, by themselves, were risk factors for a C-section) and developing pre-eclampsia.
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Coronavirus (COVID-19) Events as They Happen. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/events-as-they-happen (accessed on 25 May 2021).
- Ellington, S.; Strid, P.; Tong, V.T.; Woodworth, K.; Galang, R.R.; Zambrano, L.D.; Nahabedian, J.; Anderson, K.; Gilboa, S.M. Characteristics of Women of Reproductive Age with Laboratory-Confirmed SARS-CoV-2 Infection by Pregnancy Status—United States, January 22–June 7, 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 769–775. [Google Scholar] [CrossRef]
- Gheblawi, M.; Wang, K.; Viveiros, A.; Nguyen, Q.; Zhong, J.C.; Turner, A.J.; Raizada, M.K.; Grant, M.B.; Oudit, G.Y. Angiotensin-Converting Enzyme 2: SARS-CoV-2 Receptor and Regulator of the Renin-Angiotensin System: Celebrating the 20th Anniversary of the Discovery of ACE2. Circ. Res. 2020, 126, 1456–1474. [Google Scholar] [CrossRef] [PubMed]
- Knight, M.; Bunch, K.; Vousden, N.; Morris, E.; Simpson, N.; Gale, C.; O’Brien, P.; Quigley, M.; Brocklehurst, P.; Kurinczuk, J.J.; et al. Characteristics and outcomes of pregnant women admitted to hospital with confirmed SARS-CoV-2 infection in UK: National population based cohort study. BMJ 2020, 369, m2107. [Google Scholar] [CrossRef]
- Dong, L.; Tian, J.; He, S.; Zhu, C.; Wang, J.; Liu, C.; Yang, J. Possible Vertical Transmission of SARS-CoV-2 From an Infected Mother to Her Newborn. JAMA 2020, 323, 1846–1848. [Google Scholar] [CrossRef] [Green Version]
- Lee, D.H.; Lee, J.; Kim, E.; Woo, K.; Park, H.Y.; An, J. Emergency cesarean section performed in a patient with confirmed severe acute respiratory syndrome Coronavirus-2—A case report-. Korean J. Anesthesiol. 2020, 73, 347–351. [Google Scholar] [CrossRef]
- Hantoushzadeh, S.; Shamshirsaz, A.A.; Aleyasin, A.; Seferovic, M.D.; Aski, S.K.; Arian, S.E.; Pooransari, P.; Ghotbizadeh, F.; Aalipour, S.; Soleimani, Z.; et al. Maternal death due to COVID-19. Am. J. Obstet. Gynecol. 2020, 223, 109.e1–109.e16. [Google Scholar] [CrossRef]
- Ferrazzi, E.; Frigerio, L.; Savasi, V.; Vergani, P.; Prefumo, F.; Barresi, S.; Bianchi, S.; Ciriello, E.; Facchinetti, F.; Gervasi, M.T.; et al. Vaginal delivery in SARS-CoV-2-infected pregnant women in Northern Italy: A retrospective analysis. BJOG 2020, 127, 1116–1121. [Google Scholar] [CrossRef] [PubMed]
- Parazzini, F.; Bortolus, R.; Mauri, P.A.; Favilli, A.; Gerli, S.; Ferrazzi, E. Delivery in pregnant women infected with SARS-CoV-2: A fast review. Int. J. Gynaecol. Obstet. 2020, 150, 41–46. [Google Scholar] [CrossRef] [Green Version]
- Protocols Medicina Maternofetal. Hospital Clìnic-Hospital Sant Joan de Dèu-Universitat de Barcelona. Available online: https://medicinafetalbarcelona.org/protocolos/es/obstetricia/cesarea.html (accessed on 22 November 2021).
- Rottenstreich, A.; Tsur, A.; Braverman, N.; Kabiri, D.; Porat, S.; Benenson, S.; Oster, Y.; Kam, H.A.; Walfisch, A.; Bart, Y.; et al. Vaginal delivery in SARS-CoV-2-infected pregnant women in Israel: A multicenter prospective analysis. Arch. Gynecol. Obstet. 2020, 303, 1401–1405. [Google Scholar] [CrossRef] [PubMed]
- Carrasco, I.; Muñoz-Chapuli, M.; Vigil-Vázquez, S.; Aguilera-Alonso, D.; Hernández, C.; Sánchez-Sánchez, C.; Oliver, C.; Riaza, M.; Pareja, M.; Sanz, O.; et al. SARS-COV-2 infection in pregnant women and newborns in a Spanish cohort (GESNEO-COVID) during the first wave. BMC Pregnancy Childbirth 2021, 21, 326. [Google Scholar] [CrossRef]
- Melguizo, S.C.; Conty, M.D.L.C.; Payán, P.C.; Abascal-Saiz, A.; Recarte, P.P.; Rodríguez, L.G.; Marín, C.C.; Varea, A.M.; Cuesta, A.O.; Rodríguez, P.; et al. Pregnancy Outcomes and SARS-CoV-2 Infection: The Spanish Obstetric Emergency Group Study. Viruses 2021, 13, 853. [Google Scholar] [CrossRef]
- Siegler, Y.; Weiner, Z.; Solt, I. Prelabor Rupture of Membranes: ACOG Practice Bulletin, Number 217. Obstet. Gynecol. 2020, 135, e80–e97. [Google Scholar] [CrossRef]
- WHO. OMS|La Clasificación de Robson: Manual de Aplicación. 2018. Available online: http://www.who.int/reproductivehealth/publications/maternal_perinatal_health/robson-classification/es/ (accessed on 21 April 2021).
- O’Leary, B.D.; Kane, D.T.; Aretz, N.K.; Geary, M.P.; Malone, F.D.; Hehir, M.P. Use of the Robson Ten Group Classification System to categorise operative vaginal delivery. Aust. New Zealand J. Obstet. Gynecol. 2020, 60, 858–864. [Google Scholar] [CrossRef]
- Martínez-Perez, O.; Vouga, M.; Cruz Melguizo, S.; Forcen Acebal, L.; Panchaud, A.; Muñoz-Chápuli, M.; Baud, D. Association between Mode of Delivery among Pregnant Women with COVID-19 and Maternal and Neonatal Outcomes in Spain. JAMA 2020, 324, 296–299. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzschef, P.C.; Vandenbroucke, J.P. ARTÍCULO ESPECIAL Declaración de la Iniciativa STROBE (Strengthening the Reporting of Observational Studies in Epidemiology): Directrices Para la Comunicación de Estudios Observacionales (The Strengthening the Reporting of Observational Studies in Epidemiology [STROBE] statement: Guidelines for Reporting Observational Studies). Available online: http://www.epidem.com/ (accessed on 21 April 2021).
- Brown, M.A.; Magee, L.A.; Kenny, L.C.; Karumanchi, S.A.; McCarthy, F.; Saito, S.; Hall, D.R.; Warren, C.E.; Adoyi, G.; Ishaku, S. Hypertensive Disorders of Pregnancy. Hypertension 2018, 72, 24–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomson, A.J. Care of Women Presenting with Suspected Preterm Prelabour Rupture of Membranes from 24+0 Weeks of Gestation: Green-top Guideline No. 73. BJOG 2019, 126, e152–e166. [Google Scholar] [CrossRef] [Green Version]
- Bates, D.; Mächler, M.; Bolker, B.; Walker, S. Fitting Linear Mixed-Effects Models Using lme4. J. Stat. Softw. 2015, 67, 1–48. [Google Scholar] [CrossRef]
- Allotey, J.; Stallings, E.; Bonet, M.; Yap, M.; Chatterjee, S.; Kew, T.; Debenham, L.; Llavall, A.C.; Dixit, A.; Zhou, D.; et al. Clinical manifestations, risk factors, and maternal and perinatal outcomes of coronavirus disease 2019 in pregnancy: Living systematic review and meta-analysis. BMJ 2020, 370, m3320. [Google Scholar] [CrossRef] [PubMed]
- Zaigham, M.; Andersson, O. Maternal and perinatal outcomes with COVID-19: A systematic review of 108 pregnancies. Acta Obstet. Gynecol. Scand. 2020, 99, 823–829. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woo, I.; Hindoyan, R.; Landay, M.; Ho, J.; Ingles, S.A.; McGinnis, L.K.; Paulson, R.J.; Chung, K. Perinatal outcomes after natural conception versus in vitro fertilization (IVF) in gestational surrogates: A model to evaluate IVF treatment versus maternal effects. Fertil. Steril. 2017, 108, 993–998. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santana, D.S.; Surita, F.G.; Cecatti, J.G. Multiple Pregnancy: Epidemiology and Association with Maternal and Perinatal Morbidity. Rev. Bras. Ginecol. Obstet. 2018, 40, 554–562. [Google Scholar] [CrossRef] [Green Version]
- Han, H.; Yang, L.; Liu, R.; Liu, F.; Wu, K.L.; Li, J.; Liu, X.H.; Zhu, C.L. Prominent changes in blood coagulation of patients with SARS-CoV-2 infection. Clin. Chem. Lab. Med. 2020, 58, 1116–1120. [Google Scholar] [CrossRef] [Green Version]
- Wise, R.A.; Polito, A.J.; Krishnan, V. Respiratory physiologic changes in pregnancy. Immunol. Allergy Clin. North Am. 2006, 26, 1–12. [Google Scholar] [CrossRef]
- Conde-Agudelo, A.; Romero, R. SARS-CoV-2 infection during pregnancy and risk of preeclampsia: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. 2021. [Google Scholar] [CrossRef]
- Deneux-Tharaux, C.; Carmona, E.; Bouvier-Colle, M.H.; Bréart, G. Postpartum maternal mortality and cesarean delivery. Obstet. Gynecol. 2006, 108, 541–548. [Google Scholar] [CrossRef]
- Esteves-Pereira, A.P.; Deneux-Tharaux, C.; Nakamura-Pereira, M.; Saucedo, M.; Bouvier-Colle, M.H.; do Carmo Leal, M. Caesarean delivery and postpartum maternal mortality: A population-based case control study in Brazil. PLoS ONE 2016, 11, e0153396. [Google Scholar] [CrossRef]
- Yu, N.; Li, W.; Kang, Q.; Xiong, Z.; Wang, S.; Lin, X.; Liu, Y.; Xiao, J.; Liu, H.; Deng, D.; et al. Clinical Features and obstetric and neonatal outcomes of pregnancy patients with COVID-19 in Wuhan, China. A restrospective, single-centre, desctriptive study. Lancet Infect. Dis. 2020, 20, 559–564. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Infected Cohort | Vaginal + Operative Vaginal | C-Section | p-Value | ||
|---|---|---|---|---|---|
| Number | 1704 | 1248 (73.2) | 456 (26.8) | ||
| Maternal Characteristics | |||||
| Maternal age (years; median/IQR) | 32 (28–36) | 32 (27–36) | 34 (29–37) | <0.001 * | |
| Age Range | 18–24 years | 241/1689 (14.3) 825/1689 (48.8) 623/1689 (36.9) | 188 (15.2) 627 (50.6) 423 (34.2) | 53 (11.8) 198 (43.9) 200 (44.3) | 0.001 * |
| 25–34 years | |||||
| 35–49 years | |||||
| Ethnicity | White European | 947/1699 (55.7) 514/1699 (30.3) 44/1699 (2.6) 50/1699 (2.9) 144/1699 (8.5) | 689/1245 (55.3) 374/1245 (30.0) 34/1245 (2.7) 39/1245 (3.1) 109/1245 (8.8) | 258/454 (56.8) 140/454 (30.8) 10/454 (2.2) 11/454 (2.4) 35/454 (7.7) | 0.816 |
| Latino Americans | |||||
| Black non-Hispanic | |||||
| Asian non-Hispanic | |||||
| Arab | |||||
| Nulliparous | 616/1688 (36.5) | 431/1233 (35.0) | 185/455 (40.7) | 0.031 * | |
| Smoking a | 160 (9.7) | 105 (8.7) | 55 (12.7) | 0.016 * | |
| Maternal Comorbidities | |||||
| Obesity (BMI > 30 kg/m2) | 317 (18.6) | 203 (16.3) | 114 (25.0) | <0.001 * | |
| Thrombophilia | 28 (1.6) | 15 (1.2) | 13 (2.9) | 0.018 * | |
| Chronic kidney disease | 6 (0.4) | 2 (0.2) | 4 (0.9) | 0.047 * | |
| Diabetes mellitus | 36 (2.1) | 20 (1.6) | 16 (3.5) | 0.015 * | |
| Current Obstetric History | |||||
| Multiple pregnancy | 31 (1.8) | 12 (1.0) | 19 (4.2) | <0.001 * | |
| In vitro fertilization | 82 (4.8) | 37 (3.0) | 45 (9.9) | <0.001 * | |
| Intrauterine growth restriction | 61 (3.6) | 34 (2.7) | 27 (5.9) | 0.002 * | |
| Pregnancy-induced hypertension b | 42 (2.5) | 20 (1.6) | 22 (4.8) | <0.001 * | |
| High-risk pre-eclampsia screening | 90/1484 (6.1) | 58/1095 (5.3) | 32/389 (8.2) | 0.038 * | |
| Infected Cohort | Vaginal + Operative Vaginal | C-Section | p-Value | |
|---|---|---|---|---|
| Number | 1704 | 1248 (73.2) | 456 (26.8) | |
| Outcomes | ||||
| Gestational age at delivery (weeks + days; median/IQR) | 39 + 7 (38 + 2 to 40 + 3) | 39 + 4 (38 + 4 to 40 + 1) | 39 + 0 (37 + 0 to 40 + 1) | <0.001 * |
| Hemorrhagic events Abruptio placentae Postpartum hemorrhage | 93 (5.5) 18 (1.1) 79 (4.6) | 48 (3.8) 1 (0.1) 47 (3.8) | 45 (9.9) 17 (3.7) 32 (7.0) | <0.001 * <0.001 * 0.005 * |
| Hypertensive disorders Antepartum/postpartum hypertension Pre-eclampsia/eclampsia Moderate pre-eclampsia Severe pre-eclampsia/HELLP/eclampsia | 104/1661 (6.3) 87 (5.1) 56/87 (64.4) 31/87 (35.6) | 50/1222 (4.1) 42 (3.4) 30/42 (71.4) 12/42 (28.6) | 54/439 (12.3) 45 (9.9) 26/45 (57.8) 19/45 (42.2) | <0.001 * <0.001 * 0.184 |
| Thrombotic events Deep venous thrombosis Pulmonary embolism Disseminated intravascular coagulation | 18 (1.1) 3 (0.2) 10 (0.6) 6 (0.4) | 6 (0.5) 1 (0.1) 3 (0.2) 2 (0.2) | 12 (2.6) 2 (0.4) 7 (1.5) 4 (0.9) | <0.001 * 0.176 0.005 * 0.047 * |
| Admitted in ICU | 52 (3.1) | 7 (0.6) | 45 (9.9) | <0.001 * |
| Invasive mechanical ventilation | 31 (1.8) | 3 (0.2) | 28 (6.1) | <0.001 * |
| Maternal Mortality | 2 (0.1) | 0 (0.0) | 2 (0.4) | 0.071 |
| Neonatal Score | ||||
| Apgar 5 score < 7 Umbilical artery pH < 7.10 Birth weight (grams; median/IQR) | 17/1661 (1.0) 44/1359 (3.2) 3260 (2900–3570) | 3/1218 (0.2) 25/989 (2.5) 3290 (2940–3560) | 14/443 (3.2) 19/370 (5.1) 3170 (2628–3595) | <0.001 * 0.016 * <0.001 * |
| Admitted in NICU | 163/1684 (9.7) | 70/1234 (5.7) | 93/450 (20.7) | <0.001 * |
| Neonatal mortality | 6 (0.4) | 2 (0.2) | 4 (0.9) | 0.047 * |
| Asymptomatic | Mild–Moderate Symptoms | Pneumonia | p-Value | |
|---|---|---|---|---|
| Number | 689 (52.2) | 398 (30.2) | 233 (17.7) | |
| Onset of labor: Programmed C-section Spontaneous Induced | 46 (6.7) 392 (56.9) 251 (36.4) | 46 (11.6) 199 (50.0) 153 (38.4) | 54/232 (23.3) 89/232 (38.4) 89/232 (38.4) | <0.001 * |
| Type of delivery: Vaginal Operative vaginal C-section | 450 (65.3) 77 (11.2) 162 (23.5) | 242 (60.8) 44 (11.1) 112 (28.1) a | 119 (51.1) 19 (8.2) 95 (40.8) | <0.001 *,b |
| Robson classification of C-sections: 1 2 3 4 5 6 7 8 9 10 | 15/162 (9.3) 40/162 (24.7) 14/162 (8.6) 21/162 (13.0) 30/162 (18.5) 12/162 (7.4) 12/162 (7.4) 4/162 (2.5) 1/162 (0.6) 13/162 (8.0) | 8/111 (7.2) 20/111 (18.0) 10/111 (9.0) 12/111 (10.8) 25/111 (22.5) 9/111 (8.1) 6/111 (5.4) 5/111 (4.5) 0/111 (0.0) 16/111 (14.4) | 2/95 (2.1) 10/95 (10.5) 5/95 (5.3) 18/95 (18.9) 10/95 (10.5) 5/95 (5.3) 2/95 (2.1) 4/95 (4.2) 0/95 (0.0) 39/95 (41.1) | <0.001 * |
| C-section before or after ICU admission: Before ICU admission After ICU admission | 2/162 (1.2) 2/2 (100) 0/2 (0.0) | 6/112 (5.4) 4/6 (66.7) 2/6 (33.3) | 30/95 (31.6) 20/30 (66.7) 10/30 (33.3) | 0.614 |
| Gestational Age Range at Delivery | p-Value | ||||
|---|---|---|---|---|---|
| 28 to <33 Weeks | 33 to <37 Weeks | 37 to <41 Weeks | ≥41 Weeks | ||
| Number | n = 39 | n = 112 | n = 986 | n = 183 | |
| Type of delivery: Vaginal + operative vaginal C-section | 12 (30.8) 27 (69.2) | 50 (44.6) 62 (55.4) | 746 (75.7) 240 (24.3) a | 143 (78.1) 40 (21.9) | <0.001 * |
| Reasons for C-section: COVID-19 complication COVID-19 complication + pre-eclampsia COVID-19 complication + other obstetrical causes Pre-eclampsia without COVID-19 complication Other obstetrical causes without COVID-19 complication | 11/27 (40.7) 4/27 (14.8) 2/27 (7.4) 4/27 (14.8) 6/27 (22.2) | 19/62 (30.6) 4/62 (6.5) 7/62 (11.3) 5/62 (8.1) 27/62 (43.5) | 25/240 (10.4) 3/240 (1.2) 17/240 (7.1) 15/240 (6.2) 180/240 (75.0) | 5/40 (12.5) 0/40 (0.0) 0/40 (0.0) 1/40 (2.5) 34/40 (85.0) | <0.001 * |
| Robson classification of C-sections: 1 2 3 4 5 6 7 8 9 10 | 0/27 (0.0) 0/27 (0.0) 0/27 (0.0) 0/27 (0.0) 0/27 (0.0) 0/27 (0.0) 1/27 (3.7) 4/27 (14.8) 0/27 (0.0) 22/27 (81.5) | 0/62 (0.0) 0/62 (0.0) 0/62 (0.0) 0/62 (0.0) 0/62 (0.0) 7/62 (11.3) 4/62 (6.5) 5/62 (8.1) 0/62 (0.0) 46/62 (74.2) | 20/239 (8.4) 48/239 (20.1) 26/239 (10.9) 42/239 (17.6) 64/239 (26.8) 19/239 (7.9) 15/239 (6.3) 4/239 (1.7) 1/239 (0.4) 0/239 (0.0) | 5/40 (12.5) 22/40 (55.0) 3/40 (7.5) 9/40 (22.5) 1/40 (2.5) 0/40 (0.0) 0/40 (0.0) 0/40 (0.0) 0/40 (0.0) 0/40 (0.0) | <0.001 * |
| Multivariable Model | Variables Associated with C-Section | p-Value | aOR (95% CI) |
|---|---|---|---|
| C-section = COVID-19 symptoms + preterm delivery + interaction (COVID-19 symptoms and preterm delivery) + gestational age at diagnosis + pre-eclampsia + IVF | COVID-19 mild–moderate symptoms | 0.523 a | |
| COVID-19 pneumonia | 0.013 a | 1.55 (1.09–2.18) | |
| Preterm delivery | 0.003 | 2.44 (1.34–4.37) | |
| Interaction (COVID-19 mild–moderate symptoms and preterm delivery) | 0.456 | ||
| Interaction (COVID-19 pneumonia and preterm delivery) | 0.013 | 2.99 (1.27–7.25) | |
| Diagnosis in 2nd trimester | 0.141 b | ||
| Diagnosis in 3rd trimester | 0.029 b | 1.94 (1.10–3.64) | |
| Pre-eclampsia | <0.001 | 2.51 (1.55–4.04) | |
| IVF | <0.001 | 3.38 (2.10–5.44) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morán Antolín, E.; Broullón Molanes, J.R.; de la Cruz Conty, M.L.; Encinas Pardilla, M.B.; Guadix Martín, M.d.P.; Sainz Bueno, J.A.; Forcén Acebal, L.; Pintado Recarte, P.; Álvarez Bartolomé, A.; Martínez Cendán, J.P.; et al. SARS-CoV-2 Infection and C-Section: A Prospective Observational Study. Viruses 2021, 13, 2330. https://0-doi-org.brum.beds.ac.uk/10.3390/v13112330
Morán Antolín E, Broullón Molanes JR, de la Cruz Conty ML, Encinas Pardilla MB, Guadix Martín MdP, Sainz Bueno JA, Forcén Acebal L, Pintado Recarte P, Álvarez Bartolomé A, Martínez Cendán JP, et al. SARS-CoV-2 Infection and C-Section: A Prospective Observational Study. Viruses. 2021; 13(11):2330. https://0-doi-org.brum.beds.ac.uk/10.3390/v13112330
Chicago/Turabian StyleMorán Antolín, Eva, José Román Broullón Molanes, María Luisa de la Cruz Conty, María Begoña Encinas Pardilla, María del Pilar Guadix Martín, José Antonio Sainz Bueno, Laura Forcén Acebal, Pilar Pintado Recarte, Ana Álvarez Bartolomé, Juan Pedro Martínez Cendán, and et al. 2021. "SARS-CoV-2 Infection and C-Section: A Prospective Observational Study" Viruses 13, no. 11: 2330. https://0-doi-org.brum.beds.ac.uk/10.3390/v13112330