
Comparison of Throat Washings, Nasopharyngeal Swabs and Oropharyngeal Swabs for Detection of SARS-CoV-2

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects and Specimens
2.2. Molecular Detection
2.3. Statistical Analysis
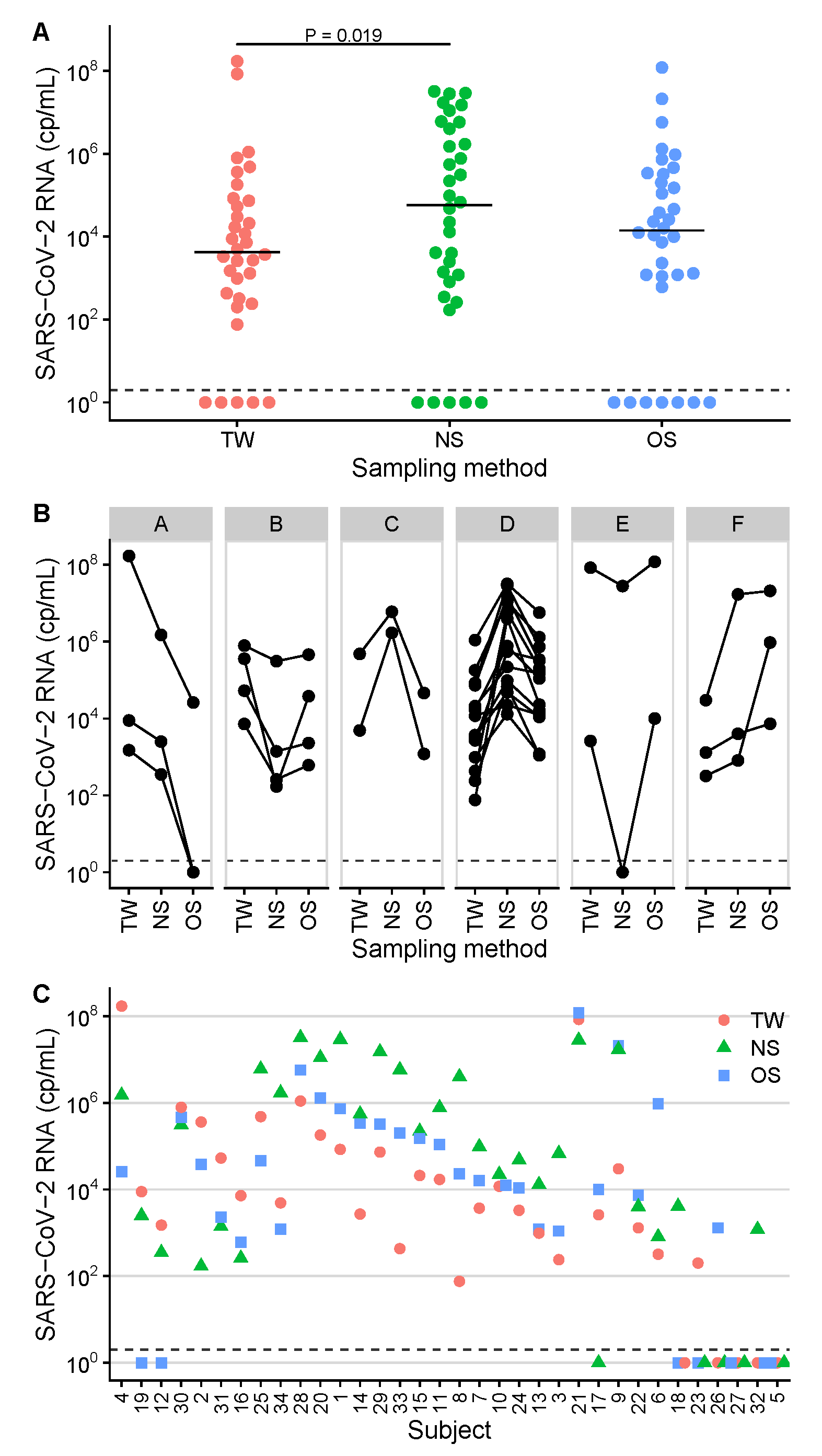
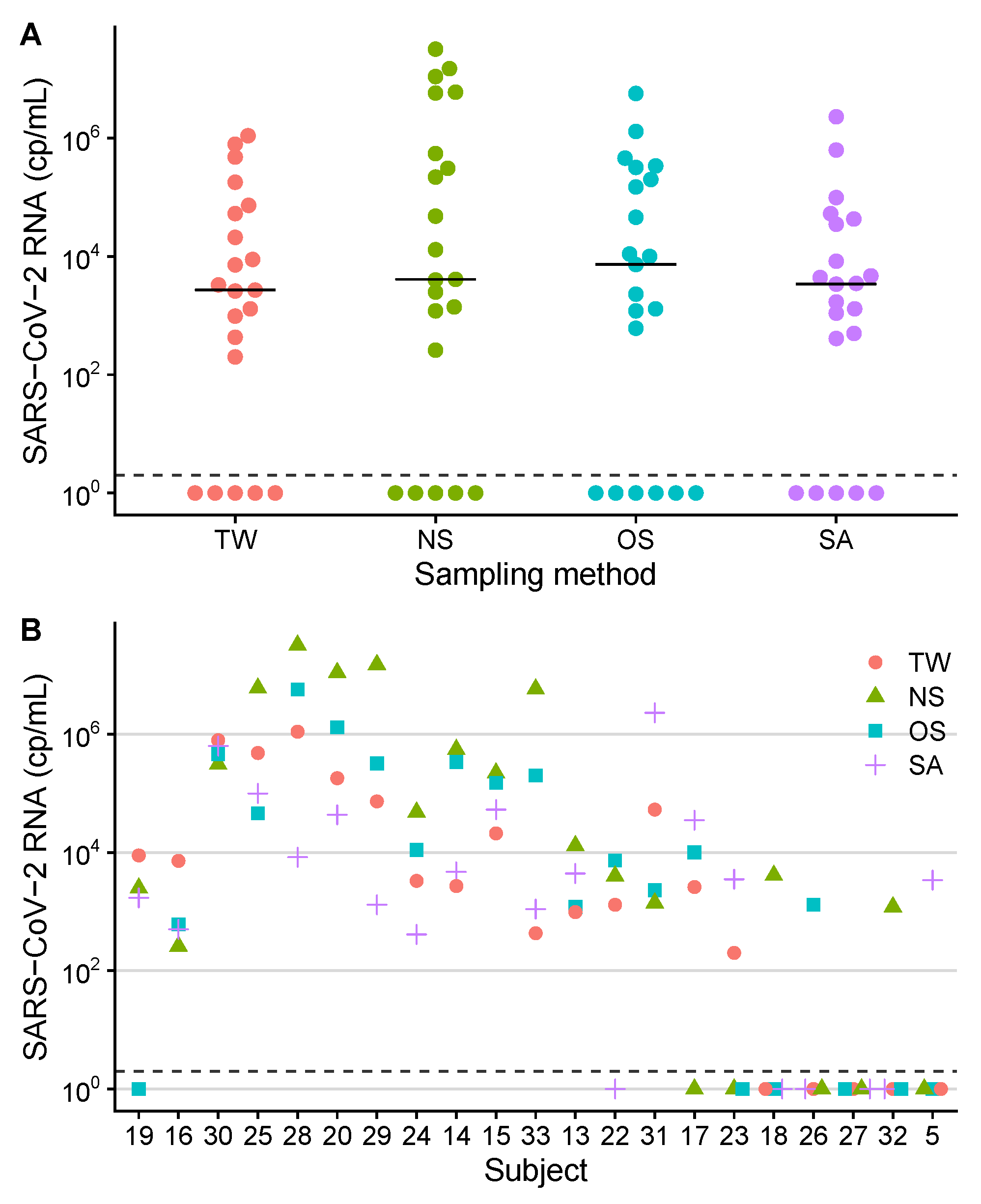
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CDC | Centers for disease control and prevention, Atlanta, GA, USA |
| COVID-19 | Coronavirus disease 2019 |
| Cp/mL | Copies per milliliter |
| CT | Computed tomography |
| F | Female |
| Null hypothesis | |
| ICU | Intensive care unit |
| IQR | Interquartile range |
| LME | Linear mixed-effects model |
| LoD95 | Limit of detection (95%) |
| M | Male |
| NA | Not available |
| NS | Nasopharyngeal swabs |
| OS | Oropharyngeal swabs |
| PCR | Polymerase chain reaction |
| RT-qPCR | Reverse-transcription quantitative real-time PCR |
| SARS-CoV-2 | Severe acute respiratory syndrome coronavirus 2 |
| SD | Standard deviation |
| TW | Throat washings |
| Y | Years |
References
- Fajnzylber, J.; Regan, J.; Coxen, K.; Corry, H.; Wong, C.; Rosenthal, A.; Worrall, D.; Giguel, F.; Piechocka-Trocha, A.; Atyeo, C.; et al. SARS-CoV-2 viral load is associated with increased disease severity and mortality. Nat. Commun. 2020, 11, 5493. [Google Scholar] [CrossRef] [PubMed]
- Wyllie, A.L.; Fournier, J.; Casanovas-Massana, A.; Campbell, M.; Tokuyama, M.; Vijayakumar, P.; Warren, J.L.; Geng, B.; Muenker, M.C.; Moore, A.J.; et al. Saliva or Nasopharyngeal Swab Specimens for Detection of SARS-CoV-2. N. Engl. J. Med. 2020, 383, 1283–1286. [Google Scholar] [CrossRef] [PubMed]
- Jamal, A.J.; Mozafarihashjin, M.; Coomes, E.; Powis, J.; Li, A.X.; Paterson, A.; Anceva-Sami, S.; Barati, S.; Crowl, G.; Faheem, A.; et al. Sensitivity of Nasopharyngeal Swabs and Saliva for the Detection of Severe Acute Respiratory Syndrome Coronavirus 2. Clin. Infect. Dis. 2021, 72, 1064–1066. [Google Scholar] [CrossRef]
- Wang, W.; Xu, Y.; Gao, R.; Lu, R.; Han, K.; Wu, G.; Tan, W. Detection of SARS-CoV-2 in Different Types of Clinical Specimens. JAMA 2020, 323, 1843–1844. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corman, V.M.; Landt, O.; Kaiser, M.; Molenkamp, R.; Meijer, A.; Chu, D.K.; Bleicker, T.; Brünink, S.; Schneider, J.; Schmidt, M.L.; et al. Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR. Eur. Surveill. 2020, 25, 2000045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wenzel, J.J.; Walch, H.; Bollwein, M.; Niller, H.H.; Ankenbauer, W.; Mauritz, R.; Höltke, H.J.; Zepeda, H.M.; Wolf, H.; Jilg, W.; et al. Library of prefabricated locked nucleic acid hydrolysis probes facilitates rapid development of reverse-transcription quantitative real-time PCR assays for detection of novel influenza A/H1N1/09 virus. Clin. Chem. 2009, 55, 2218–2222. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic. Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Guo, W.L.; Jiang, Q.; Ye, F.; Li, S.Q.; Hong, C.; Chen, L.Y.; Li, S.Y. Effect of Throat Washings on Detection of 2019 Novel Coronavirus. Clin. Infect. Dis. 2020, 71, 1980–1981. [Google Scholar] [CrossRef] [PubMed]
- Desmet, T.; Paepe, P.D.; Boelens, J.; Coorevits, L.; Padalko, E.; Vandendriessche, S.; Leroux-Roels, I.; Aerssens, A.; Callens, S.; Braeckel, E.V.; et al. Combined oropharyngeal/nasal swab is equivalent to nasopharyngeal sampling for SARS-CoV-2 diagnostic PCR. BMC Microbiol. 2021, 21, 31. [Google Scholar] [CrossRef] [PubMed]
- LeBlanc, J.J.; Heinstein, C.; MacDonald, J.; Pettipas, J.; Hatchette, T.F.; Patriquin, G. A combined oropharyngeal/nares swab is a suitable alternative to nasopharyngeal swabs for the detection of SARS-CoV-2. J. Clin. Virol. 2020, 128, 104442. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Patient | Age, y | Sex | Oxygen Therapy | ICU Therapy | Days Hospi- talized | Charlson Score a | CT- Infiltrates b | Days Sympto- matic |
|---|---|---|---|---|---|---|---|---|
| 1 | 77 | M | + | − | 18 | 6 | + | 4 |
| 2 | 55 | F | + | − | 22 | 4 | + | 10 |
| 3 | 56 | M | − | − | 6 | 10 | − | 1 |
| 4 | 58 | F | − | − | 25 | 4 | + | 1 |
| 5 | 60 | F | + | − | 19 | 2 | + | 11 |
| 6 | 22 | M | + | − | 4 | 0 | + | 8 |
| 7 | 67 | M | − | − | 30 | 3 | − | 0 |
| 8 | 39 | F | − | − | 2 | 2 | − | 6 |
| 9 | 61 | M | + | + | 34 | 8 | + | 10 |
| 10 | 46 | M | − | − | 6 | 0 | + | 8 |
| 11 | 48 | M | − | − | 1 | 1 | + | 3 |
| 12 | 38 | M | + | − | 9 | 0 | + | 7 |
| 13 | 39 | F | − | − | 4 | 0 | + | 4 |
| 14 | 34 | M | − | − | 4 | 0 | NA | 4 |
| 15 | 57 | M | + | − | 6 | 2 | − | 6 |
| 16 | 58 | M | − | − | 7 | 1 | + | 11 |
| 17 | 65 | M | − | − | 7 | 5 | + | 1 |
| 18 | 67 | M | − | − | 13 | 4 | + | 3 |
| 19 | 48 | F | − | − | 8 | 7 | + | 7 |
| 20 | 46 | M | − | − | 2 | 0 | NA | 8 |
| 21 | 78 | F | + | − | 28 | 11 | + | 7 |
| 22 | 83 | M | − | − | 14 | 7 | NA | 2 |
| 23 | 49 | M | + | − | 13 | 2 | + | 15 |
| 24 | 74 | F | + | − | 4 | 2 | + | 9 |
| 25 | 77 | M | + | − | 31 | 7 | + | 0 |
| 26 | 45 | F | + | − | 7 | 1 | + | 7 |
| 27 | 59 | M | + | − | 7 | 2 | + | 9 |
| 28 | 73 | F | − | − | 11 | 3 | NA | 2 |
| 29 | 68 | F | + | − | 19 | 3 | + | 5 |
| 30 | 72 | M | + | − | 5 | 3 | + | 5 |
| 31 | 43 | M | + | − | 6 | 0 | + | 9 |
| 32 | 71 | M | + | − | 5 | 4 | + | 12 |
| 33 | 76 | M | + | − | 13 | 6 | + | 4 |
| 34 | 45 | M | + | − | 10 | 2 | + | 7 |
| Summary c | Mean 57.5 | F 32% | 56% | 3% | Median 7.5 | Median 2.5 | 87% | Mean 6.1 |
| SD 14.9 | M 68% | IQR 5.25–17 | IQR 1–4.75 | SD 3.7 |
| Patient | TW | NS | OS | SA |
|---|---|---|---|---|
| 1 | NA | |||
| 2 | NA | |||
| 3 | NA | |||
| 4 | NA | |||
| 5 | 0 | 0 | 0 | |
| 6 | NA | |||
| 7 | NA | |||
| 8 | NA | |||
| 9 | NA | |||
| 10 | NA | |||
| 11 | NA | |||
| 12 | 0 | NA | ||
| 13 | ||||
| 14 | ||||
| 15 | ||||
| 16 | ||||
| 17 | 0 | |||
| 18 | 0 | 0 | 0 | |
| 19 | 0 | |||
| 20 | ||||
| 21 | NA | |||
| 22 | 0 | |||
| 23 | 0 | 0 | ||
| 24 | ||||
| 25 | ||||
| 26 | 0 | 0 | 0 | |
| 27 | 0 | 0 | 0 | 0 |
| 28 | ||||
| 29 | ||||
| 30 | ||||
| 31 | ||||
| 32 | 0 | 0 | 0 | |
| 33 | ||||
| 34 | NA | |||
| Sensitivity a | 85% | 85% | 79% | 76% |
| Summary b | Median | Median | Median | Median |
| IQR – | IQR – | IQR – | IQR – |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hitzenbichler, F.; Bauernfeind, S.; Salzberger, B.; Schmidt, B.; Wenzel, J.J. Comparison of Throat Washings, Nasopharyngeal Swabs and Oropharyngeal Swabs for Detection of SARS-CoV-2. Viruses 2021, 13, 653. https://0-doi-org.brum.beds.ac.uk/10.3390/v13040653
Hitzenbichler F, Bauernfeind S, Salzberger B, Schmidt B, Wenzel JJ. Comparison of Throat Washings, Nasopharyngeal Swabs and Oropharyngeal Swabs for Detection of SARS-CoV-2. Viruses. 2021; 13(4):653. https://0-doi-org.brum.beds.ac.uk/10.3390/v13040653
Chicago/Turabian StyleHitzenbichler, Florian, Stilla Bauernfeind, Bernd Salzberger, Barbara Schmidt, and Jürgen J. Wenzel. 2021. "Comparison of Throat Washings, Nasopharyngeal Swabs and Oropharyngeal Swabs for Detection of SARS-CoV-2" Viruses 13, no. 4: 653. https://0-doi-org.brum.beds.ac.uk/10.3390/v13040653