
Virological Correlates of IgM–IgG Patterns of Response to SARS-CoV-2 Infection According to Targeted Antigens

 , , ,
, , ,
Abstract
:1. Introduction
2. Methodology
2.1. Participants
2.2. Microbiological Assays
2.3. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mina, M.J.; Parker, R.; Larremore, D.B. Rethinking Covid-19 Test Sensitivity—A Strategy for Containment. N. Engl. J. Med. 2020, 383, e120. [Google Scholar] [CrossRef]
- Bouza, E.; Pérez-Granda, M.J.; Escribano, P.; Fernández-Del-Rey, R.; Pastor, I.; Moure, Z.; Catalán, P.; Alonso, R.; Muñoz, P.; Guinea, J.; et al. Outbreak of COVID-19 in a nursing home in Madrid. J. Infect. 2020, 81, 647–649. [Google Scholar] [CrossRef]
- Pollán, M.; Pérez-Gómez, B.; Pastor-Barriuso, R.; Oteo, J.; Hernán, M.A.; Pérez-Olmeda, M.; Fernández-García, A.; Cruz, I.; Merino-Amado, P.; Paniagua, L.J.; et al. Prevalence of SARS-CoV-2 in Spain (ENE-COVID): A nationwide, population-based seroepidemiological study. Lancet 2020, 396, 535–544. [Google Scholar] [CrossRef]
- Moderbacher, C.R.; Ramirez, S.I.; Dan, J.M.; Grifoni, A.; Hastie, K.M.; Weiskopf, D.; Belanger, S.; Abbot, R.K.; Kim, C.; Choi, J.; Kato, Y.; et al. Antigen-specific adaptive immunity to SARS-CoV-2 in acute COVID-19 and associations with age and disease severity. Cell 2020, 183, 996–1012. [Google Scholar] [CrossRef] [PubMed]
- Laing, A.G.; Lorenc, A.; Del Molino, I.; Das, A.; Fish, M.; Monin, L.; Muñoz-Ruiz, M.; McKenzie, D.R.; Hayday, T.S.; Francos-Quijorna, I.; et al. A dynamic COVID-19 immune signature includes associations with poor prognosis. Nat. Med. 2020, 26, 1623–1635. [Google Scholar] [CrossRef] [PubMed]
- Blanco-Melo, D.; Nilsson-Payant, B.E.; Liu, W.C.; Uhl, S.; Hoagland, D.; Møller, R.; Jordan, T.X.; Oishi, K.; Panis, M.; Sachs, D.; et al. Imbalanced Host Response to SARS-CoV-2 Drives Development of COVID-19. Cell 2020, 181, 1036–1045. [Google Scholar] [CrossRef] [PubMed]
- Arunachalam, P.S.; Wimmers, F.; Mok, C.K.P.; Perera, R.A.P.M.; Scott, M.; Hagan, T.; Sigal, N.; Feng, Y.; Bristow, L.; Tsang, O.T.-Y.; et al. Systems biological assessment of immunity to mild versus severe COVID-19 infection in humans. Science 2020, 369, 1210–1220. [Google Scholar] [CrossRef] [PubMed]
- Addetia, A.; Crawford, K.H.D.; Dingens, A.; Zhu, H.; Roychoudhury, P.; Huang, M.L.; Jerome, K.R.; Bloom, J.D.; Greninger, A.L. Neutralizing antibodies correlate with protection from SARS-CoV-2 in humans during a fishery vessel outbreak with a high attack rate. J. Clin. Microbiol. 2020, 58, 2107–2120. [Google Scholar] [CrossRef]
- Lederer, K.; Castaño, D.; Gómez, D.; Oguin, T.H.; Wang, S.; Manzoni, T.B.; Muramatsu, H.; Hogan, M.J.; Amanat, F.; Cherubin, P.; et al. SARS-CoV-2 mRNA vaccines foster potent anti-gen-specific germinal center responses associated with neutralizing antibody generation. Immunity 2020, 7613, 30496–30499. [Google Scholar]
- Centers for Disease Control and Prevention. Interim Guidelines for COVID-19 Antibody Testing. 2021. Available online: https://www.cdc.gov/coronavirus/2019-ncov/lab/resources/antibody-tests-guidelines.html#print (accessed on 5 April 2021).
- Hanson, K.; Caliendo, A.; Arias, C.; Englund, J.; Lee, M.; Loeb, M.; Patel, R.; el Alayli, A.; Kalot, M.A.; Falck-Ytter, Y.; et al. Infectious Diseases Society of America guidelines on the diagnosis of coronavirus disease 2019. Clin. Infect. Dis. 2020, in press. [Google Scholar] [CrossRef]
- Woo, P.C.; Lau, S.K.; Wong, B.H.; Chan, K.H.; Chu, C.M.; Tsoi, H.W.; Huang, Y.; Peiris, J.S.M.; Yuen, K. Longitudinal profile of immunoglobulin G (IgG), IgM, and IgA antibodies against the severe acute respiratory syndrome (SARS) coronavirus nucleocapsid protein in patients with pneu-monia due to the SARS coronavirus. Clin. Diagn. Lab. Immunol. 2004, 11, 665–668. [Google Scholar] [CrossRef] [Green Version]
- To, K.K.; Tsang, O.T.; Leung, W.S.; Tam, A.R.; Wu, T.C.; Lung, D.C.; Yip, C.C.-Y.; Cai, J.-P.; Chan, J.M.-C.; Chik, T.S.-H.; et al. Temporal profiles of viral load in posterior oropharyngeal saliva samples and serum antibody responses during infection by SARS-CoV-2: An observational cohort study. Lancet Infect Dis. 2020, 20, 565–574. [Google Scholar] [CrossRef] [Green Version]
- Trabaud, M.A.; Icard, V.; Milon, M.P.; Bal, A.; Lina, B.; Escuret, V. Comparison of eight commercial, high-throughput, automated or ELISA assays detecting SARS-CoV-2 IgG or total antibody. J. Clin. Virol. 2020, 132, 104613. [Google Scholar] [CrossRef] [PubMed]
- Wellinghausen, N.; Voss, M.; Ivanova, R.; Deininger, S. Evaluation of the SARS-CoV-2-IgG response in outpatients by five commercial immunoassays. GMS Infect. Dis. 2020, 8, Doc22. [Google Scholar] [PubMed]
- Prince, H.E.; Givens, T.S.; Lapé-Nixon, M.; Clarke, N.J.; Schwab, D.A.; Batterman, H.J.; Jones, R.S.; Meyer, W.A., III; Kapoor, H.; Rowland, C.M.; et al. Detection of SARS-CoV-2 IgG targeting nucleocapsid or spike Protein by four high-throughput immunoassays authorized for emergency use. J. Clin. Microbiol. 2020, 58, e01742-20. [Google Scholar] [CrossRef] [PubMed]
- Ripperger, T.J.; Uhrlaub, J.L.; Watanabe, M.; Wong, R.; Castaneda, Y.; Pizzato, H.A.; Thompson, M.R.; Bradshaw, C.; Weinkauf, C.C.; Bime, C.; et al. Detection, prevalence, and duration of humoral responses to SARS-CoV-2 under conditions of limited population exposure. Immunity 2020, in press. [Google Scholar]
- Maine, G.N.; Lao, K.M.; Krishnan, S.M.; Afolayan-Oloye, O.; Fatemi, S.; Kumar, S.; VanHorn, L.; Hurand, A.; Sykes, E.; Sun, Q. Longitudinal characterization of the IgM and IgG humoral response in symptomatic COVID-19 patients using the Abbott Architect. J. Clin. Virol. 2020, 133, 104663. [Google Scholar] [CrossRef] [PubMed]
- Candel, F.J.; Viñuela-Prieto, J.M.; González del Castillo, J.; Barreiro, P.; Fragiel, M.; Hernández-Píriz, A.; Virumbrales, D.J.; Lebrato, J.C.; de Casasola, G.G.; Prieto, R.G.; et al. Utility of lateral flow tests in SARS-CoV-2 infection monitorization. Rev. Esp. Quimioter. 2020, 33, 258–266. [Google Scholar] [CrossRef]
- Pham, J.; Meyer, S.; Nguyen, C.; Williams, A.; Hunsicker, M.; McHardy, I.; Gendlina, I.; Goldstein, D.Y.; Fox, A.S.; Hudson, A.; et al. Performance characteristics of a high-throughput automated transcription-mediated amplification test for SARS-CoV-2 detection. J. Clin. Microbiol. 2020, 58, 1669. [Google Scholar] [CrossRef]
- Gao, H.-X.; Li, Y.-N.; Xu, Z.-G.; Wang, Y.-L.; Wang, H.-B.; Cao, J.-F.; Yuan, D.-Q.; Li, L.; Xu, Y.; Zhang, Z.; et al. Detection of serum immunoglobulin M and immunoglobulin G antibodies in 2019 novel coronavirus infected patients from different stages. Chin. Med. J. 2020, 133, 1479–1480. [Google Scholar] [CrossRef]
- Qian, C.; Zhou, M.; Cheng, F.; Lin, X.; Gong, Y.; Xie, X.; Li, P.; Li, Z.; Zhang, P.; Liu, Z.; et al. Development and multicenter performance evaluation of fully automated SARS-CoV-2 IgM and IgG immunoassays. Clin. Chem. Lab. Med. 2020, 58, 1601–1607. [Google Scholar] [CrossRef] [PubMed]
- Rikhtegaran, Z.; Saadat, S.; Saleh, E.; Ouyang, X.; Constantine, N.; DeVico, A.L.; Harris, A.D.; Lewis, G.K.; Kottilil, S.; Sajadi, M.M. Performance of nucleocapsid and spike-based SARS-CoV-2 serologic assays. PLoS ONE 2020, 15, e0237828. [Google Scholar]
- Long, Q.X.; Liu, B.Z.; Deng, H.J.; Wu, G.C.; Deng, K.; Chen, Y.K.; Liao, P.; Qiu, J.F.; Lin, Y.; Cai, X.F.; et al. Antibody responses to SARS-CoV-2 in patients with COVID-19. Nat. Med. 2020, 26, 845–848. [Google Scholar] [CrossRef] [PubMed]
- Risch, M.; Weber, M.; Thiel, S.; Grossmann, K.; Wohlwend, N.; Lung, T.; Hillmann, D.; Ritzler, M.; Ferrara, F.; Bigler, S.; et al. Temporal course of SARS-CoV-2 antibody positivity in patients with COVID-19 following the first clinical presentation. Biomed. Res. Int. 2020, 16, 9878453. [Google Scholar] [CrossRef]
- Grandjean, L.; Saso, A.; Ortiz, A.; Lam, T.; Hatcher, J.; Thistlethwaite, R.; Harris, M.; Best, T.; Johnson, M.; Wagstaffe, H.; et al. Humoral response dynamics following infection with SARS-CoV-2. medRxiv 2020. [Google Scholar] [CrossRef]
- Long, Q.X.; Tang, X.J.; Shi, Q.L.; Li, Q.; Deng, H.J.; Yuan, J.; Hu, J.-L.; Xu, W.; Zhang, Y.; Lv, F.-J.; et al. Clinical and immunological assessment of asymptomatic SARS-CoV-2 infections. Nat. Med. 2020, 26, 1200–1204. [Google Scholar] [CrossRef]
- Siegrist, C.-A.; Aspinall, R. B-cell responses to vaccination at the extremes of age. Nat. Rev. Immunol. 2009, 9, 185–194. [Google Scholar] [CrossRef]
- Boraschi, D.; Italiani, P. Immunosenescence and vaccine failure in the elderly: Strategies for improving response. Immunol. Lett. 2014, 162, 346–353. [Google Scholar] [CrossRef]
- Ibarrondo, F.J.; Fulcher, J.A.; Goodman-Meza, D.; Elliott, J.; Hofmann, C.; Hausner, M.A.; Ferbas, K.G.; Tobin, N.H.; Aldrovandi, G.M.; Yang, O.O. Rapid decay of anti-SARS-CoV-2 an-tibodies in persons with mild Covid-19. N. Engl. J. Med. 2020, 383, 1085–1087. [Google Scholar] [CrossRef] [PubMed]
- Dan, J.; Mateus, J.; Kato, Y.; Hastie, K.M.; Faliti, C.E.; Ramirez, S.I.; Frazier, A.; Yu, E.D.; Grifoni, A.; Rawlings, S.A.; et al. Immunological memory to SARS-CoV-2 assessed for greater than six months after infection. bioRxiv 2020. [Google Scholar] [CrossRef]
- Gaebler, C.; Wang, Z.; Lorenzi, J.; Muecksch, F.; Finkin, S.; Tokuyama, M.; Ladinsky, M.; Cho, A.; Jankovic, M.; Schaefer-Babajew, D.; et al. Evolution of antibody immunity to SARS-CoV-2. BioRxiv 2020. [Google Scholar] [CrossRef]
- Demonbreun, A.R.; McDade, T.W.; Pesce, L.; Vaught, L.A.; Reiser, N.L.; Bogdanovic, E.; Velez, M.E.; Hsieh, R.R.; Klaisner, C.; Simons, L.M.; et al. Patterns and persistence of SARS-CoV-2 IgG antibodies in a US metropolitan site. medRxiv 2020. [Google Scholar] [CrossRef]
- Chi, X.; Yan, R.; Zhang, J.; Zhang, G.; Zhang, Y.; Hao, M.; Zhang, Z.; Fan, P.; Dong, Y.; Yang, Y.; et al. A neutralizing human antibody binds to the N-terminal domain of the Spike protein of SARS-CoV-2. Science 2020, 369, 650–655. [Google Scholar] [CrossRef] [PubMed]
- Mazzini, L.; Martinuzzi, D.; Hyseni, I.; Benincasa, L.; Molesti, E.; Casa, E.; Lapini, G.; Piu, P.; Trombetta, C.M.; Marchi, S.; et al. Comparative analyses of SARS-CoV-2 binding (IgG, IgM, IgA) and neutralizing antibodies from human serum samples. J. Immunol. Methods 2021, 489, 112937. [Google Scholar] [CrossRef]
- Samrat, S.K.; Tharappel, A.M.; Li, Z.; Li, H. Prospect of SARS-CoV-2 spike protein: Potential role in vaccine and therapeutic de-velopment. Virus Res. 2020, 288, 198141. [Google Scholar] [CrossRef]
- Luchsinger, L.L.; Ransegnola, B.P.; Jin, D.K.; Muecksch, F.; Weisblum, Y.; Bao, W.; George, P.J.; Rodriguez, M.; Tricoche, N.; Schmidt, F.; et al. Serological assays estimate highly variable SARS-CoV-2 neutralizing antibody activity in recovered COVID-19 patients. J. Clin. Microbiol. 2020, 58, e02005-20. [Google Scholar] [CrossRef]


{kind=link}
| All (%) | Residents (%) | Workers (%) | p Value | |
|---|---|---|---|---|
| No. | 712 | 449 (63.0) | 263 (37.0) | |
| IgM-S positive | 439 (61.7) | 229 (51.0) | 164 (62.4) | 0.004 |
| IgG-N positive | 498 (69.9) | 338 (75.3) | 167 (63.5) | <0.001 |
| Patterns: | ||||
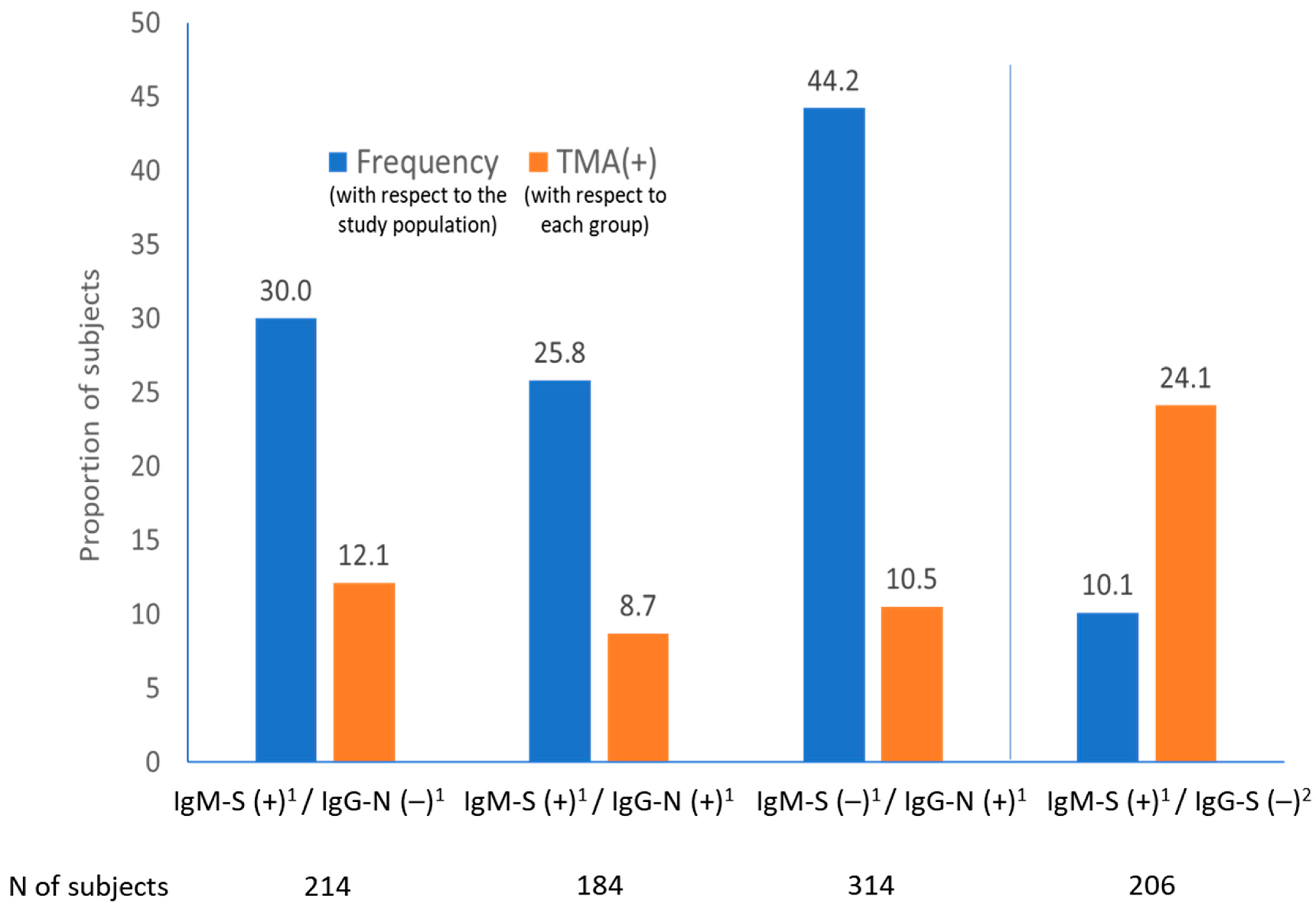
| IgM-S positive/IgG-N negative | 214 (30.0) | 108 (24.0) | 95 (36.1) | 0.001 |
| IgM-S positive/IgG-N positive | 184 (25.8) | 120 (26.8) | 69 (26.2) | NS |
| IgM-S negative/IgG-N positive | 314 (44.2) | 221 (49.2) | 99 (37.7) | 0.002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barreiro, P.; Candel, F.J.; Sanz, J.C.; San Román, J.; del Mar Carretero, M.; Pérez-Abeledo, M.; Ramos, B.; Viñuela-Prieto, J.M.; Canora, J.; Martínez-Peromingo, F.J.; et al. Virological Correlates of IgM–IgG Patterns of Response to SARS-CoV-2 Infection According to Targeted Antigens. Viruses 2021, 13, 874. https://0-doi-org.brum.beds.ac.uk/10.3390/v13050874
Barreiro P, Candel FJ, Sanz JC, San Román J, del Mar Carretero M, Pérez-Abeledo M, Ramos B, Viñuela-Prieto JM, Canora J, Martínez-Peromingo FJ, et al. Virological Correlates of IgM–IgG Patterns of Response to SARS-CoV-2 Infection According to Targeted Antigens. Viruses. 2021; 13(5):874. https://0-doi-org.brum.beds.ac.uk/10.3390/v13050874
Chicago/Turabian StyleBarreiro, Pablo, Francisco Javier Candel, Juan Carlos Sanz, Jesús San Román, María del Mar Carretero, Marta Pérez-Abeledo, Belén Ramos, José Manuel Viñuela-Prieto, Jesús Canora, Francisco Javier Martínez-Peromingo, and et al. 2021. "Virological Correlates of IgM–IgG Patterns of Response to SARS-CoV-2 Infection According to Targeted Antigens" Viruses 13, no. 5: 874. https://0-doi-org.brum.beds.ac.uk/10.3390/v13050874