
Social Restrictions versus Testing Campaigns in the COVID-19 Crisis: A Predictive Model Based on the Spanish Case

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
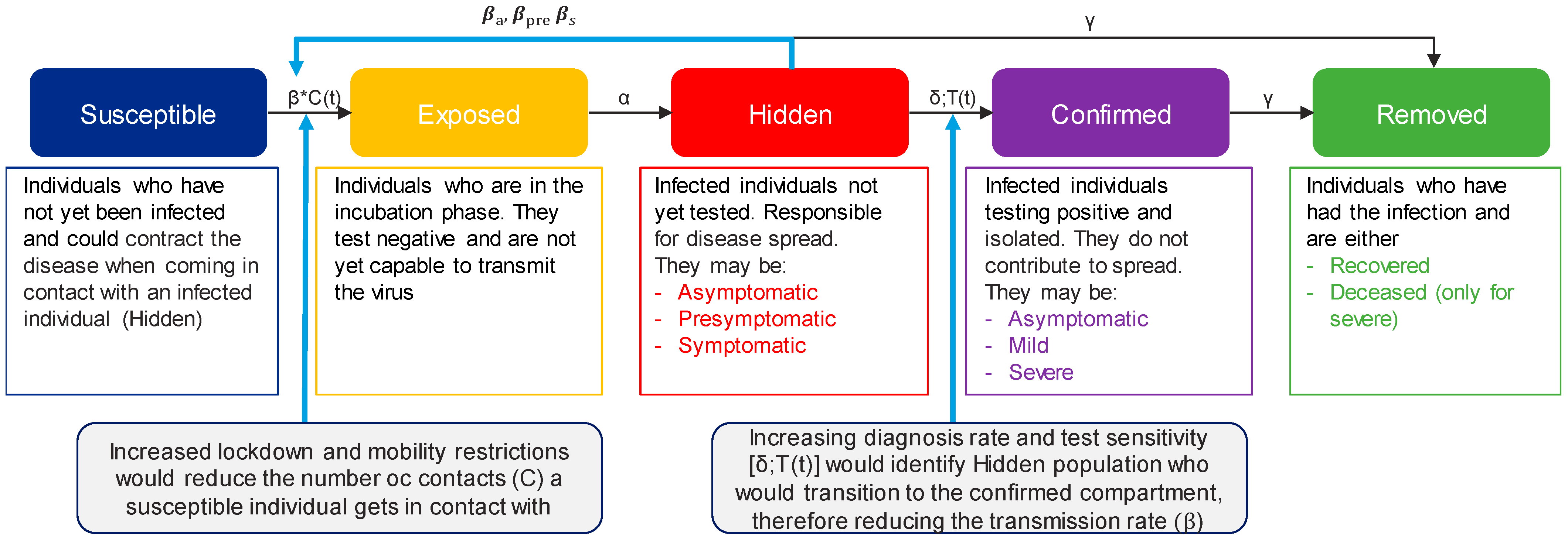
2.1. Epidemiological Model
- The simulation is initiated at the hidden compartment at the moment n for each age group and type (asymptomatic, pre-symptomatic, symptomatic);
- Then, the migration coefficient (constant number of pre-symptomatic individuals who are outside of the population) is added;
- Then, multiplied by the respective transmission probability (βa βpre or βs) and by the seasonal adjustment.
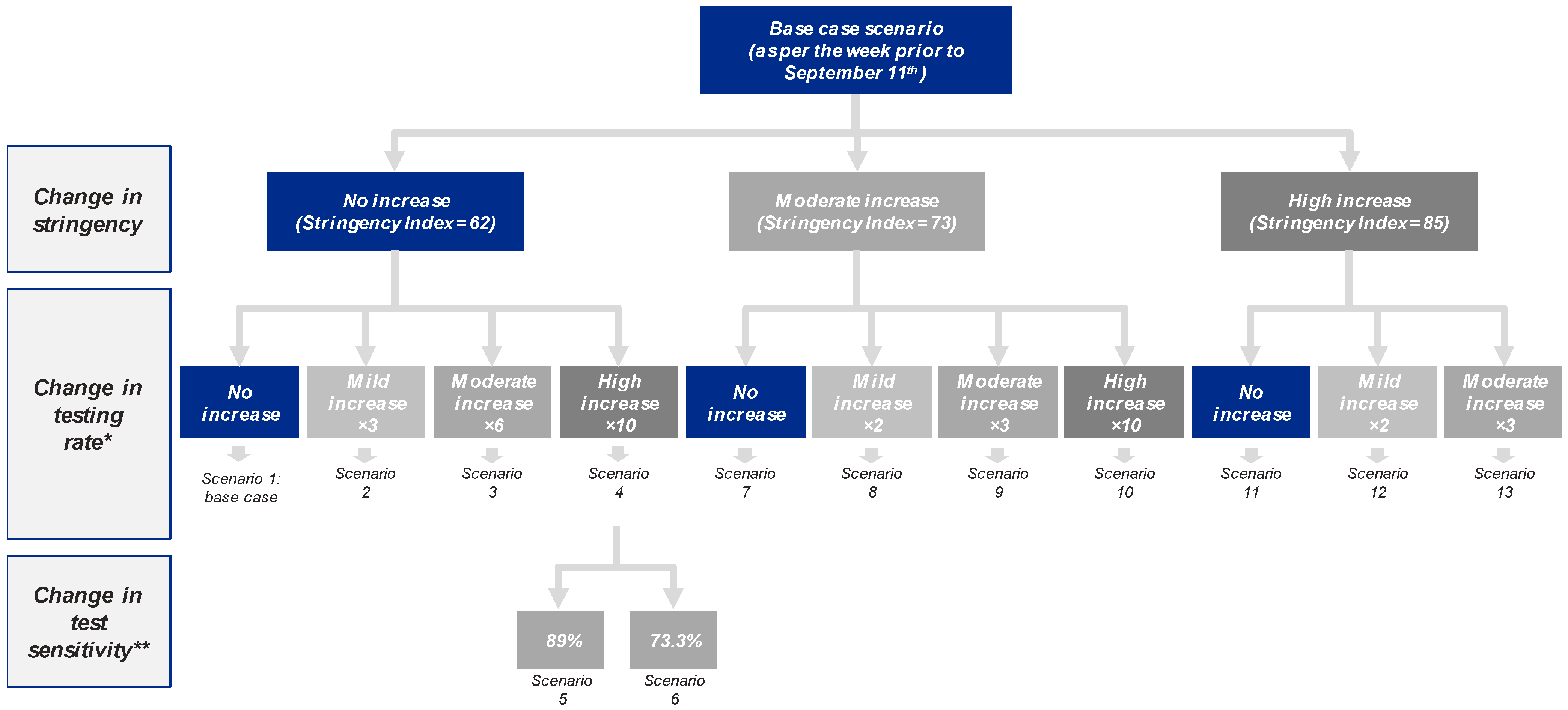
2.2. Scenario Definitions
- Level of restrictions/lockdown (stringency) based on the Government Response Stringency Index, a composite measure on a 0-to-100 scale (100 being the strictest) based on nine response indicators including school/workplace closures and travel bans among others, which is fully described and available for download from the Our World in Data website [3,4];
- Number of molecular tests per case [4];
- Test sensitivity was assumed to be 96% (i.e., 4% false negative rate) in all scenarios (lower 95% confidence interval of the SARS-CoV-2 transcription-mediated amplification (TMA) Procleix® test sensitivity) [23]. In two meta-analyses, other molecular tests had shown lower sensitivities [24,25]; conservatively, the sensitivity in the model was decreased to 89% and 73.3% to explore the relevance of this parameter [24,25].
2.3. Economic Model
2.3.1. Direct Healthcare Costs
2.3.2. Correlation between GDP Variation and NPI
3. Results
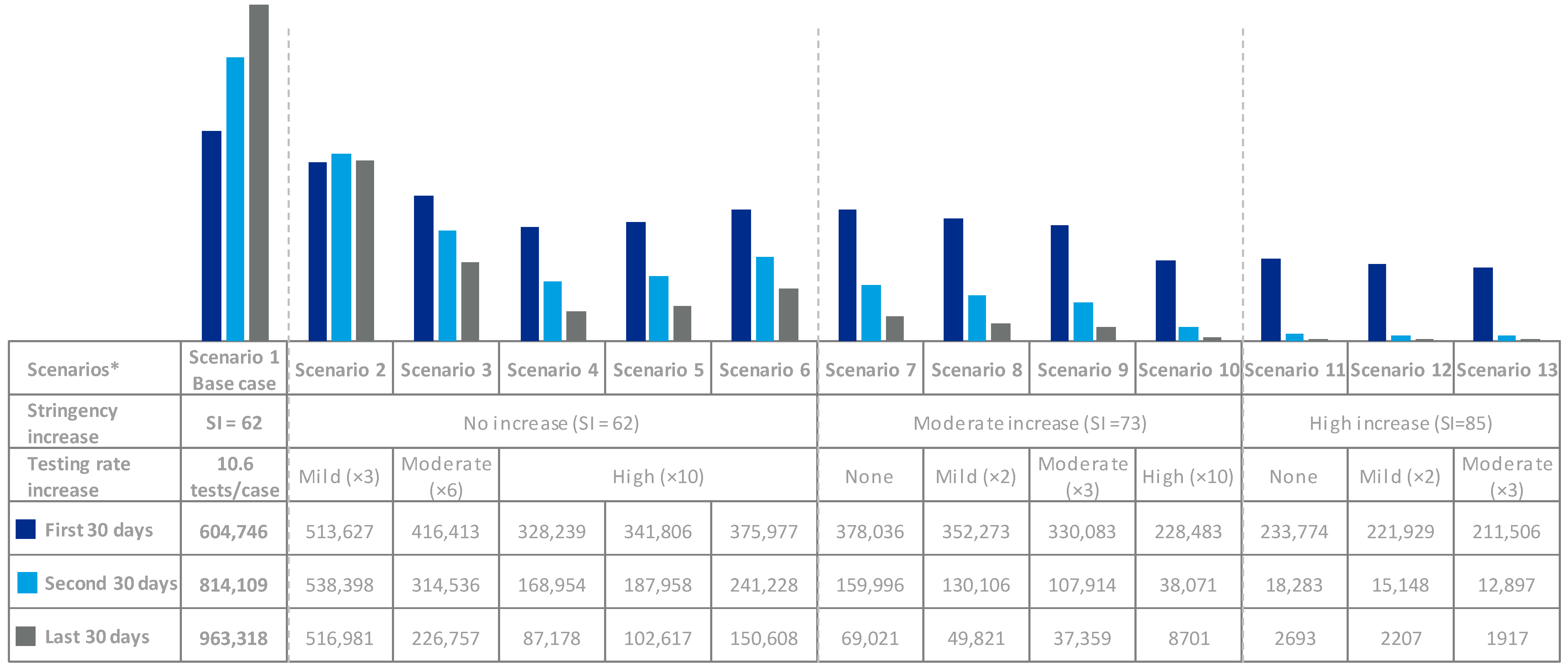
3.1. Epidemiological Outcomes
3.2. Economic Outcomes
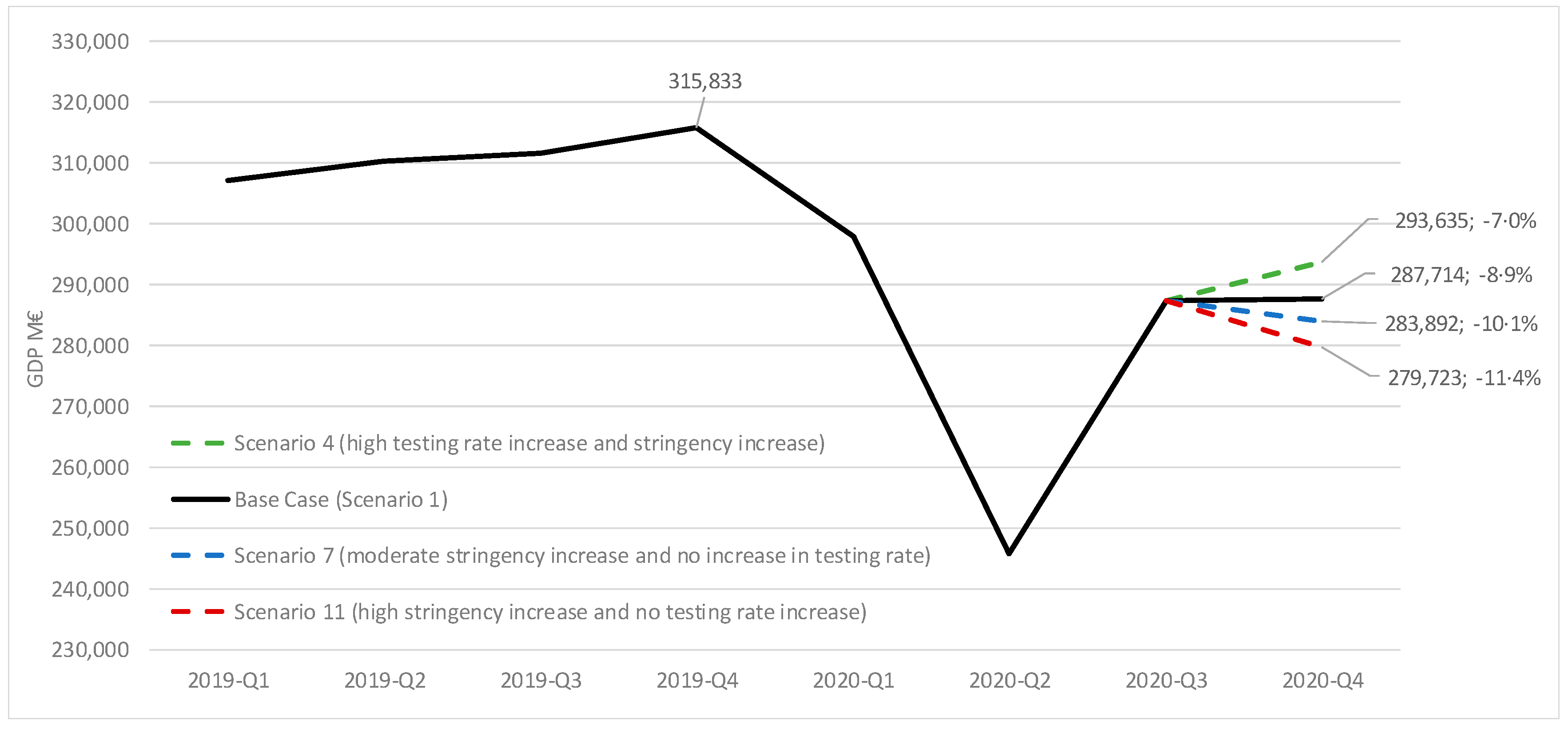
3.2.1. Potential Impact of NPI on GDP
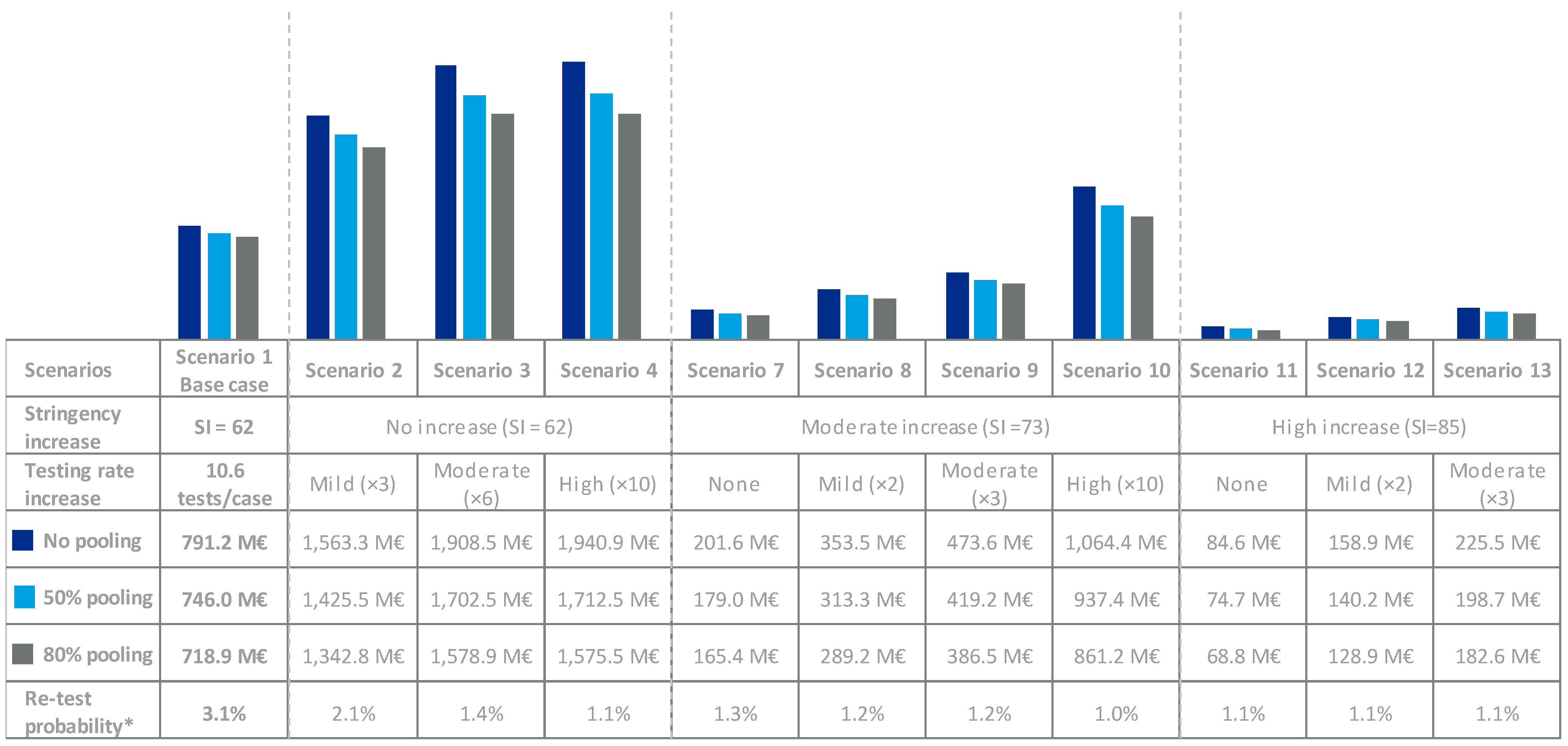
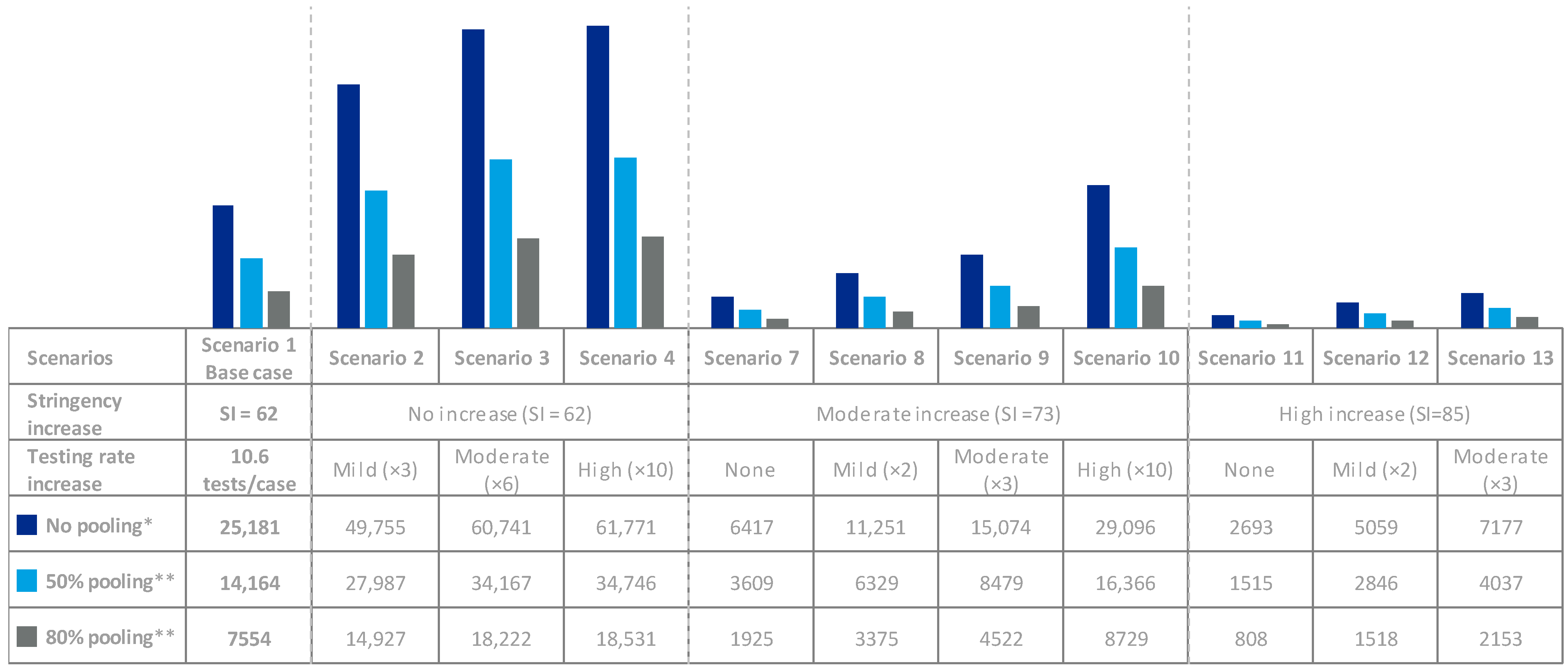
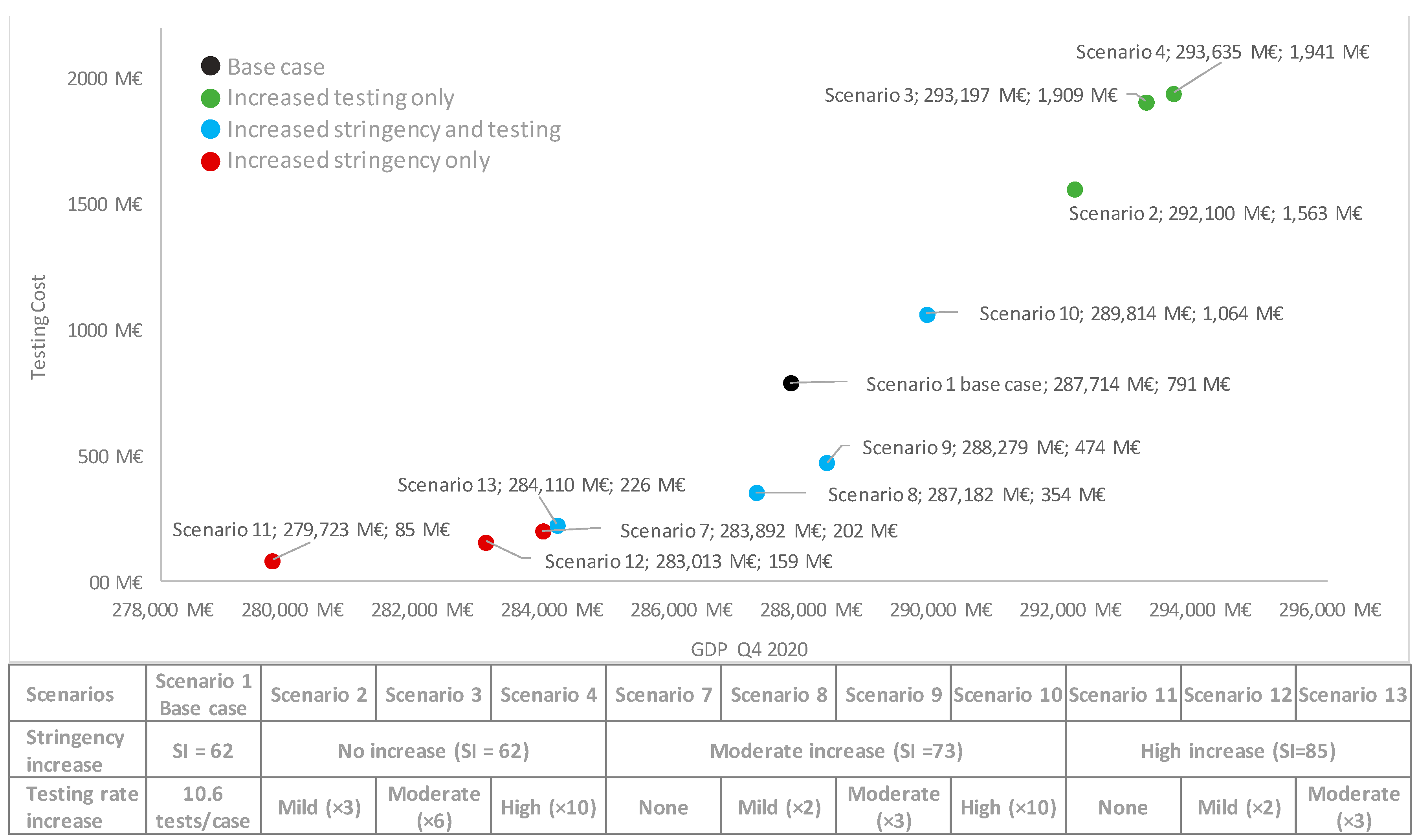
3.2.2. Economic Value of Testing
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 18 March 2021).
- European Centre for Disease Prevention and Control. Timeline of ECDC’s Response to COVID-19. Available online: https://www.ecdc.europa.eu/en/covid-19/timeline-ecdc-response (accessed on 4 November 2020).
- Hale, T.; Webster, S.; Petherick, A.; Phillips, T.; Kira, B.; Petherick, A.; Phillips, T.; Webster, S.; Cameron-Blake, E.; Hallas, L.; et al. A global panel database of pandemic policies (Oxford COVID-19 Government Response Tracker). Nat. Hum. Behav. 2021, 5, 529–538. [Google Scholar] [CrossRef]
- Hasell, J.; Mathieu, E.; Beltekian, D.; Macdonald, B.; Giattino, C.; Ortiz-Ospina, E.; Roser, M.; Ritchie, H. A cross-country database of COVID-19 testing. Sci. Data 2020, 7, 345. [Google Scholar] [CrossRef]
- The Organisation for Economic Co-operation and Development (OECD). Stat Quarterly National Accounts. Available online: https://stats.oecd.org/Index.aspx?QueryName=350 (accessed on 4 November 2020).
- Han, E.; Tan, M.M.J.; Turk, E.; Sridhar, D.; Leung, G.M.; Shibuya, K.; Asgari, N.; Oh, J.; García-Basteiro, A.L.; Hanefeld, J.; et al. Lessons learnt from easing COVID-19 restrictions: An analysis of countries and regions in Asia Pacific and Europe. Lancet 2020, 396, 1525–1534. [Google Scholar] [CrossRef]
- The Lancet Public Health. COVID-19 in Spain: A predictable storm? Lancet Public Health 2020, 5, e568. [Google Scholar] [CrossRef]
- Fullman, N.; Yearwood, J.; Abay, S.M.; Abbafati, C.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; Abebe, Z.; Abebo, T.A.; Aboyans, V.; et al. Measuring performance on the Healthcare Access and Quality Index for 195 countries and territories and selected subnational locations: A systematic analysis from the Global Burden of Disease Study 2016. Lancet 2018, 391, 2236–2271. [Google Scholar] [CrossRef]
- The Spanish Government Declares Emergency State to Stop the Spread of COVID-19. Available online: https://www.lamoncloa.gob.es/consejodeministros/resumenes/Paginas/2020/14032020_alarma.aspx (accessed on 4 November 2020).
- The Organisation for Economic Co-operation and Development (OECD). Policy Responses to Coronavirus (COVID-19). Testing for COVID-19: A Way to Lift Confinement Restrictions. Available online: https://www.oecd.org/coronavirus/policy-responses/testing-for-covid-19-a-way-to-lift-confinement-restrictions-89756248/ (accessed on 4 November 2020).
- Dighe, A.; Cattarino, L.; Cuomo-Dannenburg, G.; Skarp, J.; Imai, N.; Bhatia, S.; Gaythorpe, K.A.M.; Ainslie, K.E.C.; Baguelin, M.; Bhatt, S.; et al. Response to COVID-19 in South Korea and implications for lifting stringent interventions. BMC Med. 2020, 18, 321. [Google Scholar] [CrossRef]
- Gray, N.; Calleja, D.; Wimbush, A.; Miralles-Dolz, E.; Gray, A.; De Angelis, M.; Derrer-Merk, E.; Oparaji, B.U.; Stepanov, V.; Clearkin, L.; et al. Is “no test is better than a bad test”? Impact of diagnostic uncertainty in mass testing on the spread of COVID-19. PLoS ONE 2020, 15, e0240775. [Google Scholar] [CrossRef]
- Food and Drug Administration. SARS-CoV-2 Reference Panel Comparative Data. Available online: https://www.fda.gov/medical-devices/coronavirus-covid-19-and-medical-devices/sars-cov-2-reference-panel-comparative-data (accessed on 26 November 2020).
- Mackay, M.J.; Hooker, A.C.; Afshinnekoo, E.; Salit, M.; Kelly, J.; Feldstein, J.V.; Haft, N.; Schenkel, D.; Nambi, S.; Cai, Y.; et al. The COVID-19 XPRIZE and the need for scalable, fast, and widespread testing. Nat. Biotechnol. 2020, 38, 1021–1024. [Google Scholar] [CrossRef] [PubMed]
- Arnaout, R.; Lee, R.A.; Lee, G.R.; Callahan, C.; Yen, C.F.; Smith, K.P.; Arora, R.; Kirby, J.E. SARS-CoV2 Testing: The Limit of Detection Matters. bioRxiv 2020. [Google Scholar] [CrossRef]
- Acemoglu, D.; Chernozhukov, V.; Werning, I.; Whinston, M. Optimal Targeted Lockdowns in a Multi-Group SIR Model; Working Paper 27102; National Bureau of Economic Research: Cambridge, MA, USA, 2020. [Google Scholar]
- Brotherhood, L.; Kircher, P.; Santos, C.; Tertilt, M. An Economic Model of the Covid-19 Pandemic with Young and Old Agents: Behavior, Testing and Policies; Discussion Paper Series—CRC TR 224; University of Bonn: Bonn, Germany; University of Mannheim: Mannheim, Germany, 2020. [Google Scholar]
- Colbourn, T.; Waites, W.; Panovska-Griffiths, J.; Manheim, D.; Sturniolo, S.; Colbourn, G.; Bowie, C.; Godfrey, K.M.; Peto, J.; Burgess, R.A.; et al. Modelling the health and economic impacts of population-wide testing, contact tracing and isolation (PTTI) strategies for COVID-19 in the UK. SSRN Electron. J. 2020. [Google Scholar] [CrossRef]
- Prem, K.; Cook, A.R.; Jit, M. Projecting social contact matrices in 152 countries using contact surveys and demographic data. PLoS Comput. Biol. 2017, 13, e1005697. [Google Scholar] [CrossRef] [PubMed]
- Pollan, M.; Perez-Gomez, B.; Pastor-Barriuso, R.; Oteo, J.; Hernan, M.A.; Perez-Olmeda, M.; Sanmartín, J.L.; Fernández-García, A.; Cruz, I.; Fernández de Larrea, N.; et al. Prevalence of SARS-CoV-2 in Spain (ENE-COVID): A nationwide, population-based seroepidemiological study. Lancet 2020, 396, 535–544. [Google Scholar] [CrossRef]
- Davies, N.G.; Klepac, P.; Liu, Y.; Prem, K.; Jit, M.; CMMID COVID-19 Working Group; Eggo, R.M. Age-dependent effects in the transmission and control of COVID-19 epidemics. Nat. Med. 2020, 26, 1205–1211. [Google Scholar] [CrossRef] [PubMed]
- Ministerio de Sanidad. Red Nacional de Vigilancia Epidemiológica (RENAVE). Situación y Evolución de la Pandemia de COVID-19 en España. Panel COVID-19. Available online: https://cnecovid.isciii.es/covid19/ (accessed on 30 September 2020).
- Procleix SARS-CoV-2 Assay Package Insert. Available online: https://www.diagnostic.grifols.com/documents/28901102/1023822825/ Procleix+SARS-CoV-2+IFU_GDSS-IFU-000049/ed6b34af-a8f3-4011-b15c-9f0222a86136 (accessed on 2 November 2020).
- Kim, H.; Hong, H.; Yoon, S.H. Diagnostic Performance of CT and Reverse Transcriptase Polymerase Chain Reaction for Coronavirus Disease 2019: A Meta-Analysis. Radiology 2020, 296, E145–E155. [Google Scholar] [CrossRef] [PubMed]
- Boger, B.; Fachi, M.M.; Vilhena, R.O.; Cobre, A.F.; Tonin, F.S.; Pontarolo, R. Systematic review with meta-analysis of the accuracy of diagnostic tests for COVID-19. Am. J. Infect. Control 2020, 49, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Grabarczyk, P.; Koppelman, M.; Boland, F.; Sauleda, S.; Fabra, C.; Cambie, G.; Kopacz, A.; O’Riordan, K.; Van Drimmelen, H.; O’Riordan, J.; et al. Inclusion of human immunodeficiency virus Type 2 (HIV-2) in a multiplex transcription-mediated amplification assay does not affect detection of HIV-1 and hepatitis B and C virus genotypes: A multicenter performance evaluation study. Transfusion 2015, 55, 2246–2255. [Google Scholar] [CrossRef]
- Gollier, C.; Gossner, O. Group testing against Covid-19. In EconPol Policy Briefs; Research Report: EconPol Policy Brief No. 24; European Network for Economic and Fiscal Policy Research: Munich, Germany, 2020. [Google Scholar]
- Casas-Rojo, J.; Antón-Santos, J.; Millán-Núñez-Cortés, J.; Lumbreras-Bermejo, C.; Ramos-Rincón, J.; Roy-Vallejo, E.; Artero-Mora, A.; Arnalich-Fernández, F.; García-Bruñén, J.; Vargas-Núñez, J.; et al. Clinical characteristics of patients hospitalized with COVID-19 in Spain: Results from the SEMI-COVID-19 Registry. Rev. Clin. Esp. 2020, 220, 480–494. [Google Scholar] [CrossRef]
- Corregidor-Luna, L.; Hidalgo-Correas, F.J.; Garcia-Diaz, B. Pharmaceutical management of the COVID-19 pandemic in a mid-size hospital. Farm. Hosp. 2020, 44, 11–16. [Google Scholar]
- Ministerio de Sanidad Consumo y Bienestar Social (MSCBS). Portal Estadístico. Registro de Atención Especializada (RAE-CMBD). Available online: https://pestadistico.inteligenciadegestion.mscbs.es/publicoSNS/Comun/ArbolNodos.aspx?idNodo=23606 (accessed on 29 October 2020).
- Oblikue Consulting. eSalud—Información Económica del Sector Sanitario. 2020. Available online: http://esalud.oblikue.com/ (accessed on 29 October 2020).
- The World Bank. Industry (Including Construction), Value Added (% of GDP). 2020. Available online: https://data.worldbank.org/indicator/NV.IND.TOTL.ZS?view=chart (accessed on 4 November 2020).
- Ministry of Health. Spanish Government and Instituto de Salud Carlos III. Estrategia de Detección Precoz, Vigilancia y Control de COVID-19. 26 February 2021. Available online: https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/ nCov/documentos/COVID19_Estrategia_vigilancia_y_control_e_indicadores.pdf (accessed on 29 April 2021).
- Food and Drug Administration. Individual EUAs for Antigen Diagnostic Tests for SARS-CoV-2. Available online: https://www.fda.gov/medical-devices/coronavirus-disease-2019-covid-19-emergency-use-authorizations-medical-devices/vitro-diagnostics-euas#individual-antigen (accessed on 26 November 2020).
- Instituto de Salud Carlos III. ENE-COVID Study: Fourth Round. Available online: https://www.mscbs.gob.es/gabinetePrensa/ notaPrensa/pdf/15.12151220163348113.pdf (accessed on 18 January 2021).
- Banco Central de España. Macroeconomic Projections. 2020. Available online: https://www.bde.es/bde/en/areas/analisis-economi/analisis-economi/proyecciones-mac/Proyecciones_macroeconomicas.html (accessed on 20 November 2020).
- International Monetary Fund. World Economic Outlook, October 2020: A Long and Difficult Ascent. Chapter 2. Dissecting the Economic Effects. Annex 2.1. Available online: https://www.imf.org/en/Publications/WEO/Issues/2020/09/30/world-economic-outlook-october-2020 (accessed on 21 January 2021).
- United Nations Conference on Trade and Development. Impact of the COVID-19 Pandemic on Trade and Development. Transitioning to a New Normal. Available online: https://unctad.org/system/files/official-document/osg2020d1_en.pdf (accessed on 18 January 2021).
- Gandhi, M.; Rutherford, G. Facial masking for Covid-19-potential for “variolation” as we await a vaccine. N. Eng. J. Med. 2020, 383, e101. [Google Scholar] [CrossRef]
- Trias-Llimos, S.; Alustiza, A.; Prats, C.; Tobias, A.; Riffe, T. The need for detailed COVID-19 data in Spain. Lancet Public Health 2020, 5, e576. [Google Scholar] [CrossRef]
- De Vrieze, J. Reinfections, still rare, provide clues on immunity. Science 2020, 370, 895–897. [Google Scholar] [CrossRef]
- Wajnberg, A.; Amanat, F.; Firpo, A.; Altman, D.; Bailey, M.; Mansour, M.; McMahon, M.; Meade, P.; Mendu, D.R.; Muellers, K.; et al. Robust neutralizing antibodies to SARS-CoV-2 infection persist for months. Science 2020, 370, 1227–1230. [Google Scholar] [CrossRef]
- Ripperger, T.; Uhrlaub, J.; Watanabe, M.; Wong, R.; Castaneda, Y.; Pizzato, H.; Thompson, M.R.; Bradshaw, C.; Weinkauf, C.C.; Bime, C.; et al. Orthogonal SARS-CoV-2 serological assays enable surveillance of low-prevalence communities and reveal durable humoral immunity. Immunity 2020, 53, 925–933. [Google Scholar] [CrossRef]
- Lumley, S.; O’Donnell, D.; Stoesser, N.; Matthews, P.; Howarth, A.; Hatch, S.; Marsden, B.D.; Phil, D.; Cox, S.; James, T.; et al. Oxford University Hospitals Staff Testing Group. Antibody Status and Incidence of SARS-CoV-2 Infection in Health Care Workers. N. Engl. J. Med. 2021, 384, 533–540. [Google Scholar] [CrossRef]
- Ledford, H. COVID Reinfections Are Unusual—But Could Still Help the Virus to Spread. Nature News. 14 January 2021. Available online: https://0-www-nature-com.brum.beds.ac.uk/articles/d41586-021-00071-6 (accessed on 18 January 2021).
- World Health Organization. COVID-19 Virtual Press Conference Transcript—11 January 2021. Available online: https://www.who.int/publications/m/item/covid-19-virtual-press-conference-transcript---11-january-2021 (accessed on 18 January 2021).








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Scenario * | Stringency Increase | Testing Rate Increase | Exposed Cases | Hospitalizations | Deaths |
|---|---|---|---|---|---|
| Scenario 1: Base case | SI = 62 | 10.6 tests/case * | 2,382,172 | 97,488 | 18,676 |
| Scenario 2 | No increase SI = 62 | Mild (×3) * | 1,569,006 | 72,111 | 15,730 |
| Scenario 3 | No increase SI = 62 | Moderate (×6) * | 957,706 | 51,212 | 13,069 |
| Scenario 4 | No increase SI = 62 | High (×10) * | 584,371 | 37,099 | 11,058 |
| Scenario 5 | No increase SI = 62 | High (×10) ** | 632,381 | 38,996 | 11,343 |
| Scenario 6 | No increase SI = 62 | High (×10) *** | 767,814 | 44,206 | 12,100 |
| Scenario 7 | Moderate increase SI = 73 | None * | 607,053 | 38,502 | 11,440 |
| Scenario 8 | Moderate increase SI = 73 | Mild (×2) * | 532,199 | 35,450 | 10,964 |
| Scenario 9 | Moderate increase SI = 73 | Moderate (×3) * | 475,356 | 33,066 | 10,577 |
| Scenario 10 | Moderate increase SI = 73 | High (×10) * | 275,255 | 24,230 | 9005 |
| Scenario 11 | High increase SI = 85 | None * | 254,751 | 23,398 | 8902 |
| Scenario 12 | High increase SI = 85 | Mild (×2) * | 239,284 | 22,674 | 8757 |
| Scenario 13 | High increase SI = 85 | Moderate (×3) * | 226,320 | 22,064 | 8631 |
| Scenario * | Stringency Increase | Testing Rate Increase | Hospitalization | ICU | Primary Care | Individual Testing | Total |
|---|---|---|---|---|---|---|---|
| Scenario 1: Base case | SI = 62 | 10.6 tests/case * | 504.3 M€ | 347.6 M€ | 140.7 M€ | 791.2 M€ | 1783.7 M€ |
| Scenario 2 | No increase SI = 62 | Mild (×3) * | 373.0 M€ | 257.1 M€ | 101.6 M€ | 1563.3 M€ | 2295.1 M€ |
| Scenario 3 | No increase SI = 62 | Moderate (×6) * | 264.9 M€ | 182.6 M€ | 67.6 M€ | 1908.5 M€ | 2423.6 M€ |
| Scenario 4 | No increase SI = 62 | High (×10) * | 191.9 M€ | 132.3 M€ | 45.2 M€ | 1940.9 M€ | 2310.3 M€ |
| Scenario 5 | No increase SI = 62 | High (×10) ** | 201.7 M€ | 139.0 M€ | 48.2 M€ | 2100.3 M€ | 2489.3 M€ |
| Scenario 6 | No increase SI = 62 | High (×10) *** | 228.7 M€ | 157.6 M€ | 56.4 M€ | 2550.1 M€ | 2992.8 M€ |
| Scenario 7 | Moderate increase SI = 73 | None * | 199.2 M€ | 137.3 M€ | 47.5 M€ | 201.6 M€ | 585.6 M€ |
| Scenario 8 | Moderate increase SI = 73 | Mild (×2) * | 183.4 M€ | 126.4 M€ | 43.9 M€ | 353.5 M€ | 707.2 M€ |
| Scenario 9 | Moderate increase SI = 73 | Moderate (×3) * | 171.0 M€ | 117.9 M€ | 40.6 M€ | 473.6 M€ | 803.2 M€ |
| Scenario 10 | Moderate increase SI = 73 | High (×10) * | 125.3 M€ | 86.4 M€ | 27.1 M€ | 1064.4 M€ | 1303.3 M€ |
| Scenario 11 | High increase SI = 85 | None * | 121.0 M€ | 83.4 M€ | 26.1 M€ | 84.6 M€ | 315.2 M€ |
| Scenario 12 | High increase SI = 85 | Mild (×2) * | 117.3 M€ | 80.8 M€ | 25.6 M€ | 158.9 M€ | 382.7 M€ |
| Scenario 13 | High increase SI = 85 | Moderate (×3) * | 114.1 M€ | 78.7 M€ | 24.9 M€ | 225.5 M€ | 443.2 M€ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Candel, F.J.; Viayna, E.; Callejo, D.; Ramos, R.; San-Roman-Montero, J.; Barreiro, P.; Carretero, M.d.M.; Kolipiński, A.; Canora, J.; Zapatero, A.; et al. Social Restrictions versus Testing Campaigns in the COVID-19 Crisis: A Predictive Model Based on the Spanish Case. Viruses 2021, 13, 917. https://0-doi-org.brum.beds.ac.uk/10.3390/v13050917
Candel FJ, Viayna E, Callejo D, Ramos R, San-Roman-Montero J, Barreiro P, Carretero MdM, Kolipiński A, Canora J, Zapatero A, et al. Social Restrictions versus Testing Campaigns in the COVID-19 Crisis: A Predictive Model Based on the Spanish Case. Viruses. 2021; 13(5):917. https://0-doi-org.brum.beds.ac.uk/10.3390/v13050917
Chicago/Turabian StyleCandel, Francisco Javier, Elisabet Viayna, Daniel Callejo, Raul Ramos, Jesús San-Roman-Montero, Pablo Barreiro, María del Mar Carretero, Adam Kolipiński, Jesus Canora, Antonio Zapatero, and et al. 2021. "Social Restrictions versus Testing Campaigns in the COVID-19 Crisis: A Predictive Model Based on the Spanish Case" Viruses 13, no. 5: 917. https://0-doi-org.brum.beds.ac.uk/10.3390/v13050917