
Effects of a Single Dose of Ivermectin on Viral and Clinical Outcomes in Asymptomatic SARS-CoV-2 Infected Subjects: A Pilot Clinical Trial in Lebanon

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
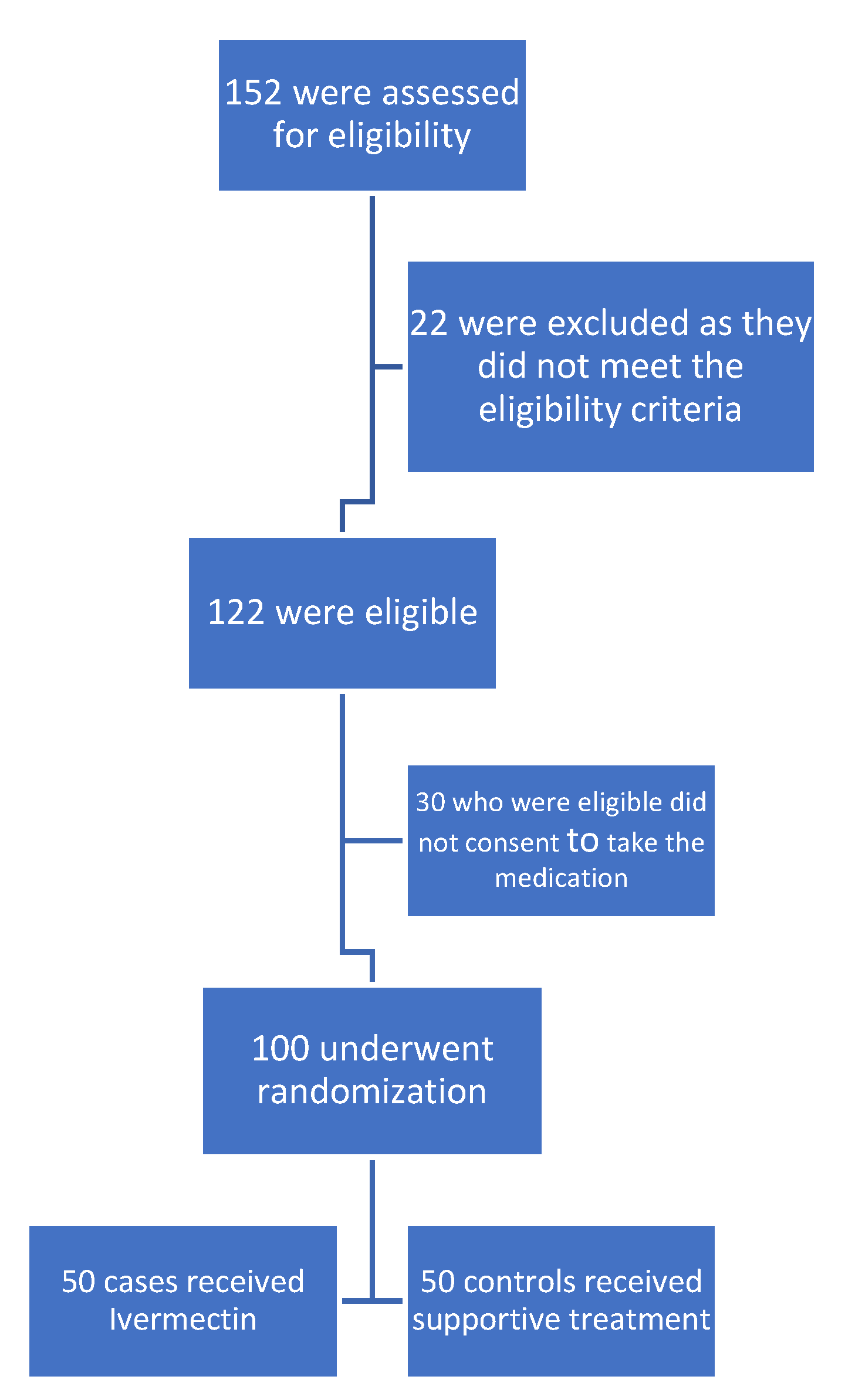
3.1. Subjects
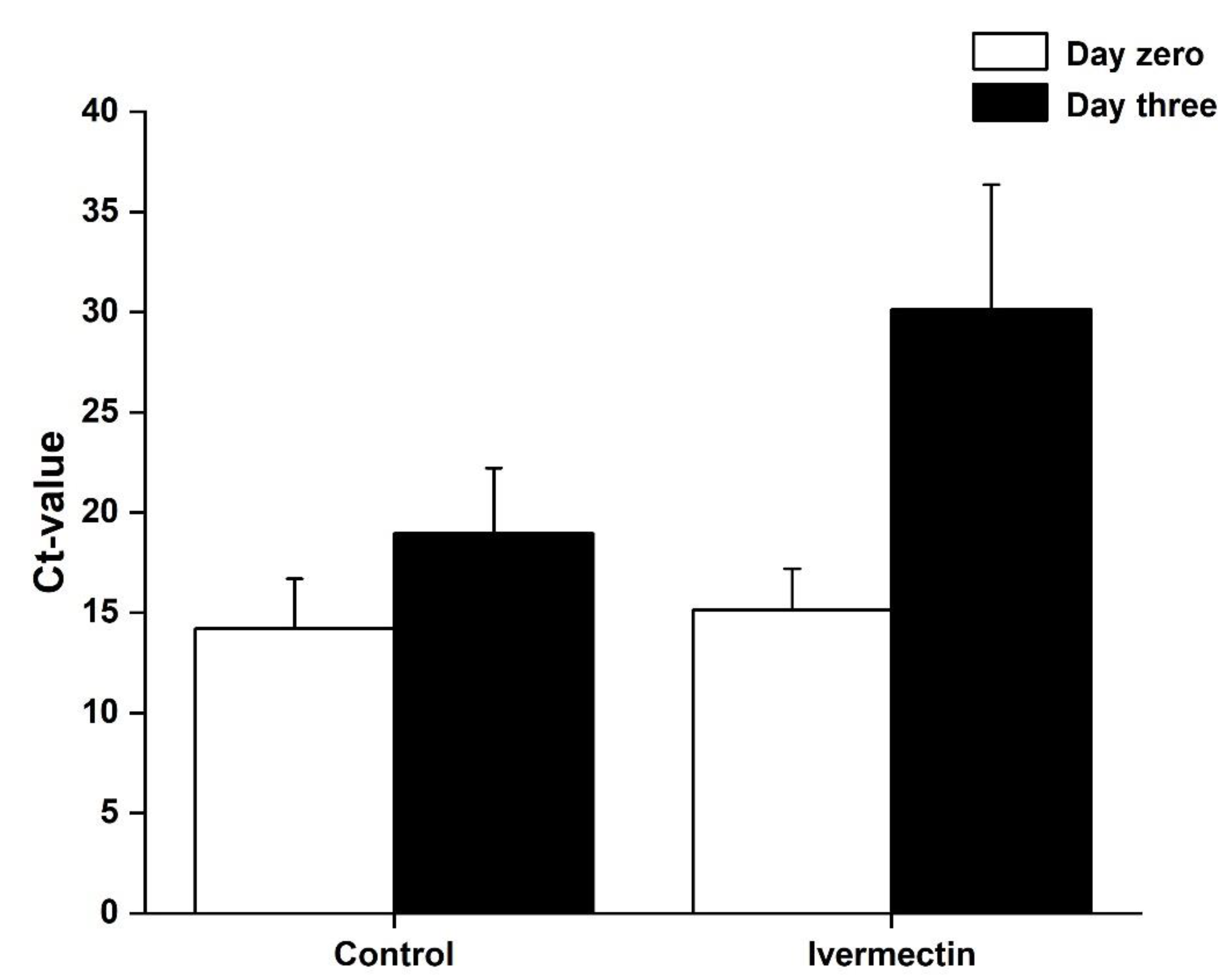
3.2. Clinical and Viral Outcomes
4. Discussion
5. Conclusions and Recommendations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lorenz, C.; Dias Bocewicz, A.C.; Correa de Azevedo Marques, C.; Reis Santana, L.M.; Chiaravalloti-Neto, F.; Alves Gomes, A.H.; Barbosa, G.L. Have measures against COVID-19 helped to reduce dengue cases in Brazil? Travel. Med. Infect. Dis. 2020, 37, 101827. [Google Scholar] [CrossRef]
- Hu, B.; Guo, H.; Zhou, P.; Shi, Z.L. Characteristics of SARS-CoV-2 and COVID-19. Nat. Rev. Microbiol. 2021, 19, 141–154. [Google Scholar] [CrossRef]
- Rabi, F.A.; Al Zoubi, M.S.; Kasasbeh, G.A.; Salameh, D.M.; Al-Nasser, A.D. SARS-CoV-2 and Coronavirus Disease 2019: What We Know So Far. Pathogens 2020, 9, 231. [Google Scholar] [CrossRef]
- Shakkour, Z.; Habashy, K.J.; Berro, M.; Takkoush, S.; Abdelhady, S.; Koleilat, N.; Eid, A.H.; Zibara, K.; Obeid, M.; Shear, D.; et al. Drug Repurposing in Neurological Disorders: Implications for Neurotherapy in Traumatic Brain Injury. Neuroscientist 2020, 1073858420961078. [Google Scholar] [CrossRef]
- Hammoud, S.H.; Wehbe, Z.; Abdelhady, S.; Kobeissy, F.; Eid, A.H.; El-Yazbi, A.F. Dysregulation of Angiotensin Converting Enzyme 2 Expression and Function in Comorbid Disease Conditions Possibly Contributes to Coronavirus Infectious Disease 2019 Complication Severity. Mol. Pharmacol. 2021, 99, 17–28. [Google Scholar] [CrossRef]
- Wehbe, Z.; Hammoud, S.; Soudani, N.; Zaraket, H.; El-Yazbi, A.; Eid, A.H. Molecular Insights Into SARS COV-2 Interaction With Cardiovascular Disease: Role of RAAS and MAPK Signaling. Front. Pharmacol. 2020, 11, 836. [Google Scholar] [CrossRef]
- Zareef, R.O.; Younis, N.K.; Bitar, F.; Eid, A.H.; Arabi, M. COVID-19 in Pediatric Patients: A Focus on CHD Patients. Front. Cardiovasc. Med. 2020, 7, 612460. [Google Scholar] [CrossRef]
- Hall, D.C., Jr.; Ji, H.F. A search for medications to treat COVID-19 via in silico molecular docking models of the SARS-CoV-2 spike glycoprotein and 3CL protease. Travel. Med. Infect. Dis. 2020, 35, 101646. [Google Scholar] [CrossRef]
- Giordo, R.; Zinellu, A.; Eid, A.H.; Pintus, G. Therapeutic Potential of Resveratrol in COVID-19-Associated Hemostatic Disorders. Molecules 2021, 26, 856. [Google Scholar] [CrossRef]
- Younis, N.K.; Zareef, R.O.; Al Hassan, S.N.; Bitar, F.; Eid, A.H.; Arabi, M. Hydroxychloroquine in COVID-19 Patients: Pros and Cons. Front. Pharmacol. 2020, 11, 597985. [Google Scholar] [CrossRef] [PubMed]
- Booz, G.W.; Altara, R.; Eid, A.H.; Wehbe, Z.; Fares, S.; Zaraket, H.; Habeichi, N.J.; Zouein, F.A. Macrophage responses associated with COVID-19: A pharmacological perspective. Eur. J. Pharmacol. 2020, 887, 173547. [Google Scholar] [CrossRef]
- Kinobe, R.T.; Owens, L. A systematic review of experimental evidence for antiviral effects of ivermectin and an in-silico analysis of ivermectin’s possible mode of action against SARS-CoV-2. Fundam Clin. Pharmacol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Arévalo, A.; Pagotto, R.; Pórfido, J.; Daghero, H.; Segovia, M.; Yamasaki, K.; Varela, B.; Hill, M.; Verdes, J.; Duhalde Vega, M.; et al. Ivermectin reduces coronavirus infection in vivo: A mouse experimental model. bioRxiv 2020. [Google Scholar] [CrossRef]
- Zhang, P.; Ni, H.; Zhang, Y.; Xu, W.; Gao, J.; Cheng, J.; Tao, L. Ivermectin confers its cytotoxic effects by inducing AMPK/mTOR-mediated autophagy and DNA damage. Chemosphere 2020, 259, 127448. [Google Scholar] [CrossRef]
- Yang, S.N.Y.; Atkinson, S.C.; Wang, C.; Lee, A.; Bogoyevitch, M.A.; Borg, N.A.; Jans, D.A. The broad spectrum antiviral ivermectin targets the host nuclear transport importin alpha/beta1 heterodimer. Antivir. Res. 2020, 177, 104760. [Google Scholar] [CrossRef]
- Wagstaff, K.M.; Sivakumaran, H.; Heaton, S.M.; Harrich, D.; Jans, D.A. Ivermectin is a specific inhibitor of importin alpha/beta-mediated nuclear import able to inhibit replication of HIV-1 and dengue virus. Biochem. J. 2012, 443, 851–856. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tay, M.Y.; Fraser, J.E.; Chan, W.K.; Moreland, N.J.; Rathore, A.P.; Wang, C.; Vasudevan, S.G.; Jans, D.A. Nuclear localization of dengue virus (DENV) 1-4 non-structural protein 5; protection against all 4 DENV serotypes by the inhibitor Ivermectin. Antivir. Res. 2013, 99, 301–306. [Google Scholar] [CrossRef]
- Gotz, V.; Magar, L.; Dornfeld, D.; Giese, S.; Pohlmann, A.; Hoper, D.; Kong, B.W.; Jans, D.A.; Beer, M.; Haller, O.; et al. Influenza A viruses escape from MxA restriction at the expense of efficient nuclear vRNP import. Sci. Rep. 2016, 6, 23138. [Google Scholar] [CrossRef] [Green Version]
- Caly, L.; Druce, J.D.; Catton, M.G.; Jans, D.A.; Wagstaff, K.M. The FDA-approved drug ivermectin inhibits the replication of SARS-CoV-2 in vitro. Antivir. Res. 2020, 178, 104787. [Google Scholar] [CrossRef]
- Jans, D.A.; Martin, A.J.; Wagstaff, K.M. Inhibitors of nuclear transport. Curr. Opin. Cell Biol 2019, 58, 50–60. [Google Scholar] [CrossRef]
- Martin, A.J.; Jans, D.A. Antivirals that target the host IMPalpha/beta1-virus interface. Biochem. Soc. Trans. 2021. [Google Scholar] [CrossRef]
- Joob, B.; Wiwanitkit, V. COVID-19 can present with a rash and be mistaken for dengue. J. Am. Acad. Dermatol. 2020, 82, e177. [Google Scholar] [CrossRef]
- Kaddoura, M.; AlIbrahim, M.; Hijazi, G.; Soudani, N.; Audi, A.; Alkalamouni, H.; Haddad, S.; Eid, A.; Zaraket, H. COVID-19 Therapeutic Options Under Investigation. Front. Pharmacol. 2020, 11, 1196. [Google Scholar] [CrossRef]
- Dingens, A.S.; Crawford, K.H.D.; Adler, A.; Steele, S.L.; Lacombe, K.; Eguia, R.; Amanat, F.; Walls, A.C.; Wolf, C.R.; Murphy, M.; et al. Serological identification of SARS-CoV-2 infections among children visiting a hospital during the initial Seattle outbreak. Nat. Commun. 2020, 11, 4378. [Google Scholar] [CrossRef]
- Kaur, H.; Shekhar, N.; Sharma, S.; Sarma, P.; Prakash, A.; Medhi, B. Ivermectin as a potential drug for treatment of COVID-19: An in-sync review with clinical and computational attributes. Pharmacol. Rep. 2021. [Google Scholar] [CrossRef]
- Thomas, S.; Patel, D.; Bittel, B.; Wolski, K.; Wang, Q.; Kumar, A.; Il’Giovine, Z.J.; Mehra, R.; McWilliams, C.; Nissen, S.E.; et al. Effect of High-Dose Zinc and Ascorbic Acid Supplementation vs Usual Care on Symptom Length and Reduction Among Ambulatory Patients With SARS-CoV-2 Infection: The COVID A to Z Randomized Clinical Trial. JAMA Netw. Open 2021, 4, e210369. [Google Scholar] [CrossRef]
- Finzi, E.; Harrington, A. Zinc treatment of outpatient COVID-19: A retrospective review of 28 consecutive patients. J. Med. Virol. 2021. [Google Scholar] [CrossRef]
- DiNicolantonio, J.J.; Barroso, J.; McCarty, M. Ivermectin may be a clinically useful anti-inflammatory agent for late-stage COVID-19. Open Heart 2020, 7. [Google Scholar] [CrossRef]
- Ahmed, S.; Karim, M.M.; Ross, A.G.; Hossain, M.S.; Clemens, J.D.; Sumiya, M.K.; Phru, C.S.; Rahman, M.; Zaman, K.; Somani, J.; et al. A five-day course of ivermectin for the treatment of COVID-19 may reduce the duration of illness. Int. J. Infect. Dis. 2021, 103, 214–216. [Google Scholar] [CrossRef]
- Navarro, M.; Camprubi, D.; Requena-Mendez, A.; Buonfrate, D.; Giorli, G.; Kamgno, J.; Gardon, J.; Boussinesq, M.; Munoz, J.; Krolewiecki, A. Safety of high-dose ivermectin: A systematic review and meta-analysis. J. Antimicrob. Chemother. 2020, 75, 827–834. [Google Scholar] [CrossRef]
- Kampf, G.; Lemmen, S.; Suchomel, M. Ct values and infectivity of SARS-CoV-2 on surfaces. Lancet Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Shakoor, H.; Feehan, J.; Al Dhaheri, A.S.; Ali, H.I.; Platat, C.; Ismail, L.C.; Apostolopoulos, V.; Stojanovska, L. Immune-boosting role of vitamins D, C, E, zinc, selenium and omega-3 fatty acids: Could they help against COVID-19? Maturitas 2021, 143, 1–9. [Google Scholar] [CrossRef]
- Alexander, J.; Tinkov, A.; Strand, T.A.; Alehagen, U.; Skalny, A.; Aaseth, J. Early Nutritional Interventions with Zinc, Selenium and Vitamin D for Raising Anti-Viral Resistance Against Progressive COVID-19. Nutrients 2020, 12, 2358. [Google Scholar] [CrossRef]
- Noreen, S.; Maqbool, I.; Madni, A. Dexamethasone: Therapeutic potential, risks, and future projection during COVID-19 pandemic. Eur. J. Pharmacol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Hussein, R.K.; Elkhair, H.M. Molecular docking identification for the efficacy of some zinc complexes with chloroquine and hydroxychloroquine against main protease of COVID-19. J. Mol. Struct. 2021, 1231, 129979. [Google Scholar] [CrossRef] [PubMed]
- Westblade, L.F.; Brar, G.; Pinheiro, L.C.; Paidoussis, D.; Rajan, M.; Martin, P.; Goyal, P.; Sepulveda, J.L.; Zhang, L.; George, G.; et al. SARS-CoV-2 Viral Load Predicts Mortality in Patients with and without Cancer Who Are Hospitalized with COVID-19. Cancer Cell 2020, 38, 661–671 e662. [Google Scholar] [CrossRef] [PubMed]
- Pujadas, E.; Chaudhry, F.; McBride, R.; Richter, F.; Zhao, S.; Wajnberg, A.; Nadkarni, G.; Glicksberg, B.S.; Houldsworth, J.; Cordon-Cardo, C. SARS-CoV-2 viral load predicts COVID-19 mortality. Lancet Respir. Med. 2020, 8, e70. [Google Scholar] [CrossRef]
- Buonfrate, D.; Salas-Coronas, J.; Munoz, J.; Maruri, B.T.; Rodari, P.; Castelli, F.; Zammarchi, L.; Bianchi, L.; Gobbi, F.; Cabezas-Fernandez, T.; et al. Multiple-dose versus single-dose ivermectin for Strongyloides stercoralis infection (Strong Treat 1 to 4): A multicentre, open-label, phase 3, randomised controlled superiority trial. Lancet Infect. Dis. 2019, 19, 1181–1190. [Google Scholar] [CrossRef]
- Rajter, J.C.; Sherman, M.S.; Fatteh, N.; Vogel, F.; Sacks, J.; Rajter, J.J. Use of Ivermectin Is Associated With Lower Mortality in Hospitalized Patients With Coronavirus Disease 2019: The Ivermectin in COVID Nineteen Study. Chest 2021, 159, 85–92. [Google Scholar] [CrossRef]
- Vargas-Estrada, D.; Gutierrez, L.; Juarez-Rodriguez, I.; Sumano, H. Pharmacokinetics of doxycycline and tissue concentrations of an experimental long-acting parenteral formulation of doxycycline in Wistar rats. Arzneimittelforschung 2008, 58, 310–315. [Google Scholar] [CrossRef]
- Hashim, H.A.; Maulood, M.F.; Rasheed, A.M.; Fatak, D.F.; Kabah, K.K.; Abdulamir, A.S. Controlled randomized clinical trial on using Ivermectin with Doxycycline for treating COVID-19 patients in Baghdad, Iraq. medRxiv 2020. [Google Scholar] [CrossRef]
- Chaccour, C.; Casellas, A.; Blanco-Di Matteo, A.; Pineda, I.; Fernandez-Montero, A.; Ruiz-Castillo, P.; Richardson, M.A.; Rodriguez-Mateos, M.; Jordan-Iborra, C.; Brew, J.; et al. The effect of early treatment with ivermectin on viral load, symptoms and humoral response in patients with non-severe COVID-19: A pilot, double-blind, placebo-controlled, randomized clinical trial. EClinicalMedicine 2021, 100720. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Control Group | Ivermectin | p-Value | ||
|---|---|---|---|---|
| Gender | Male | 25 (50%) | 25 (50%) | 1.000 |
| Female | 25 (50%) | 25 (50%) | ||
| Marital Status | Single | 20 (40%) | 29 (58%) | 0.072 |
| Married | 30 (60%) | 21 (42%) | ||
| Age (mean ± SD) | 31.58 ± 7.68 | 31.78 ± 7.85 | 0.830 | |
| Height (mean ± SD) | 172.54 ± 7.84 | 172.72 ± 14.39 | 0.098 | |
| Weight (mean ± SD) | 72.52 ± 17.28 | 78.00 ± 16.32 | 0.231 | |
| Co-existing Conditions | ||||
| Diabetes mellitus | 3 (6%) | 3 (6%) | 1.000 | |
| Hypertension | 4 (8%) | 4 (8%) | 1.000 | |
| Dyslipidemia | 3 (6%) | 3 (6%) | 1.000 | |
| Neuropathy | 4 (8%) | 4 (8%) | 1.000 | |
| Vit. D deficiency | 4 (8%) | 4 (8%) | 1.000 | |
| Hyperuricemia | 0 (0%) | 3 (6%) | 0.079 |
| Control | Ivermectin | p-Value | |||
|---|---|---|---|---|---|
| N | % | N | % | ||
| Fever | 11 | 22 | 1 | 2 | 0.002 |
| Cough | 5 | 10 | 2 | 4 | 0.240 |
| Runny Nose | 2 | 4 | 1 | 2 | 0.558 |
| Headache | 5 | 10 | 2 | 4 | 0.240 |
| Anosmia | 16 | 32 | 3 | 6 | 0.001 |
| Myalgia | 9 | 18 | 0 | 0 | 0.002 |
| Loss of Taste | 12 | 24 | 3 | 6 | 0.012 |
| Fatigue | 3 | 6 | 0 | 0 | 0.079 |
| Dizziness | 2 | 4 | 0 | 0 | 0.153 |
| Hospitalization | 3 | 6 | 0 | 0 | 0.079 |
| Ct-value; Day zero | 14.20 ± 2.48 | 15.13 ± 2.07 | 0.058 | ||
| Ct-value; Day three | 18.96 ± 3.26 | 30.14 ± 6.22 | <0.001 |
| Female | Male | ||||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | p-Value | |
| Ct-value (Day zero) | 14.93 | 2.71 | 15.27 | 2.87 | 0.544 |
| Ct-value (Day three) | 24.39 | 7.10 | 24.72 | 7.93 | 0.828 |
| Control | Ivermectin | p-Value | ||
|---|---|---|---|---|
| Females | Ct-value (Day zero) | 14.40 ± 2.56 | 15.46 ± 2.81 | 0.375 |
| Ct-value (Day three) | 18.76 ± 3.36 | 30.02 ± 5.06 | <0.001 | |
| Males | Ct-value (Day zero) | 13.99 ± 2.42 | 15.47 ± 1.87 | 0.058 |
| Ct-value (Day three) | 19.16 ± 3.22 | 30.27 ± 7.32 | <0.001 |
| Coefficients | Standard Error | p-Value | |
|---|---|---|---|
| Age | 0.03 | 0.06 | 0.655 |
| Gender | −0.35 | 1.00 | 0.731 |
| Group | 11.18 | 1.00 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Samaha, A.A.; Mouawia, H.; Fawaz, M.; Hassan, H.; Salami, A.; Bazzal, A.A.; Saab, H.B.; Al-Wakeel, M.; Alsaabi, A.; Chouman, M.; et al. Effects of a Single Dose of Ivermectin on Viral and Clinical Outcomes in Asymptomatic SARS-CoV-2 Infected Subjects: A Pilot Clinical Trial in Lebanon. Viruses 2021, 13, 989. https://0-doi-org.brum.beds.ac.uk/10.3390/v13060989
Samaha AA, Mouawia H, Fawaz M, Hassan H, Salami A, Bazzal AA, Saab HB, Al-Wakeel M, Alsaabi A, Chouman M, et al. Effects of a Single Dose of Ivermectin on Viral and Clinical Outcomes in Asymptomatic SARS-CoV-2 Infected Subjects: A Pilot Clinical Trial in Lebanon. Viruses. 2021; 13(6):989. https://0-doi-org.brum.beds.ac.uk/10.3390/v13060989
Chicago/Turabian StyleSamaha, Ali A., Hussein Mouawia, Mirna Fawaz, Hamad Hassan, Ali Salami, Ali Al Bazzal, Hamid Bou Saab, Mohamed Al-Wakeel, Ahmad Alsaabi, Mohamad Chouman, and et al. 2021. "Effects of a Single Dose of Ivermectin on Viral and Clinical Outcomes in Asymptomatic SARS-CoV-2 Infected Subjects: A Pilot Clinical Trial in Lebanon" Viruses 13, no. 6: 989. https://0-doi-org.brum.beds.ac.uk/10.3390/v13060989