
Seroprevalence of SARS-CoV-2 Binding and Neutralizing Antibodies in Healthcare Workers during the Epidemic Peak in Referral Hospitals and Quarantine Sites: Saudi Arabia

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Population and Setting
2.2. Ethical Approval
2.3. Procedures
2.4. SARS-CoV-2 Antibodies Determination by ELISA
2.5. Cells
2.6. rVSV-ΔG/SARS-2-S*-Luciferase Pseudovirus Neutralization Assay
2.7. Sample Size and Statistical Analysis
3. Results
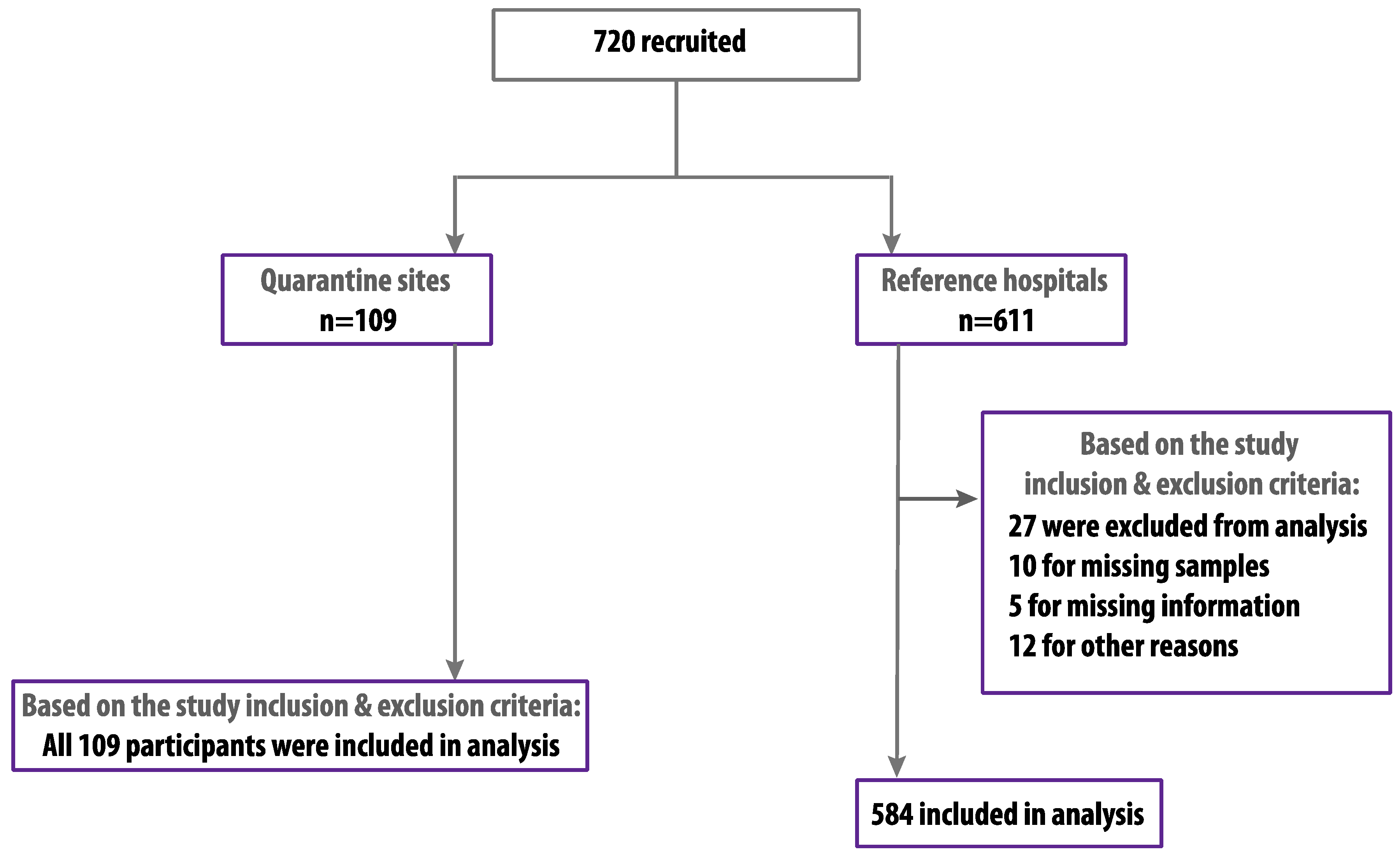
3.1. Characteristics of the Study Participants
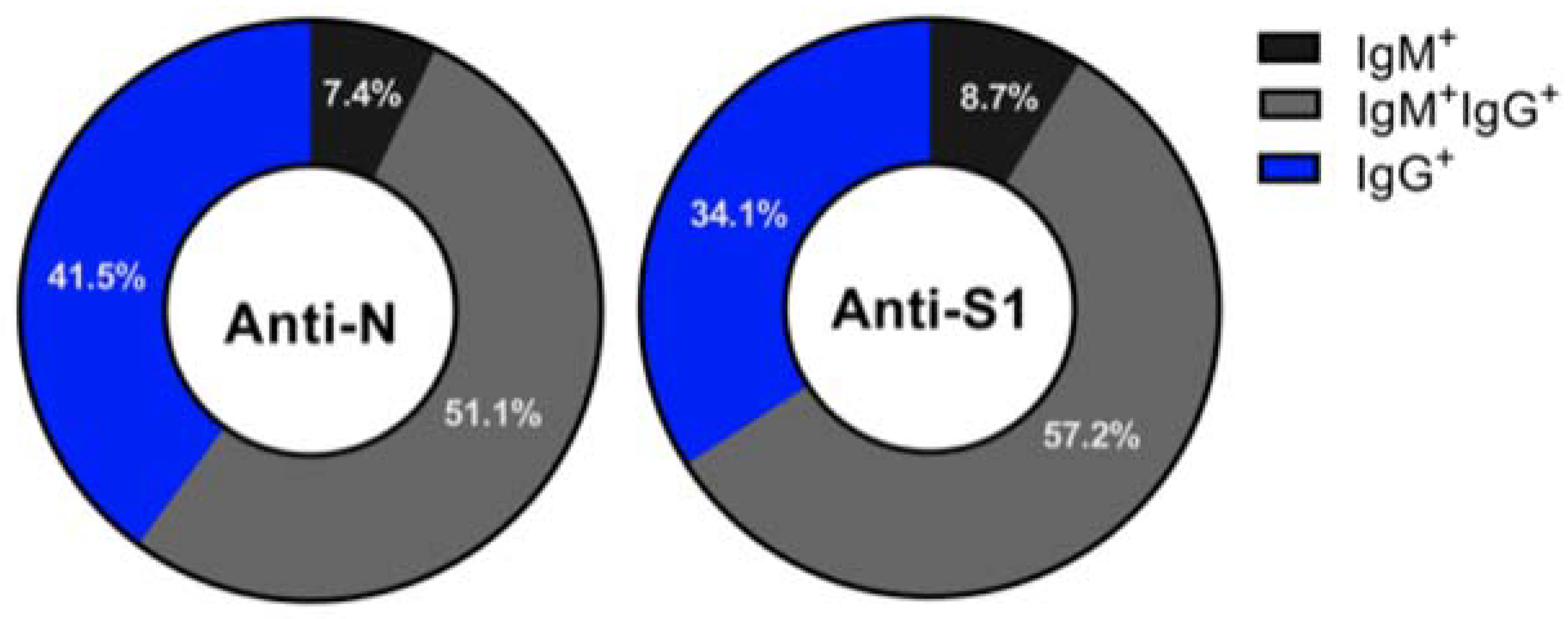
3.2. Seroprevalence of SARS-CoV-2 Antibodies in HCWs
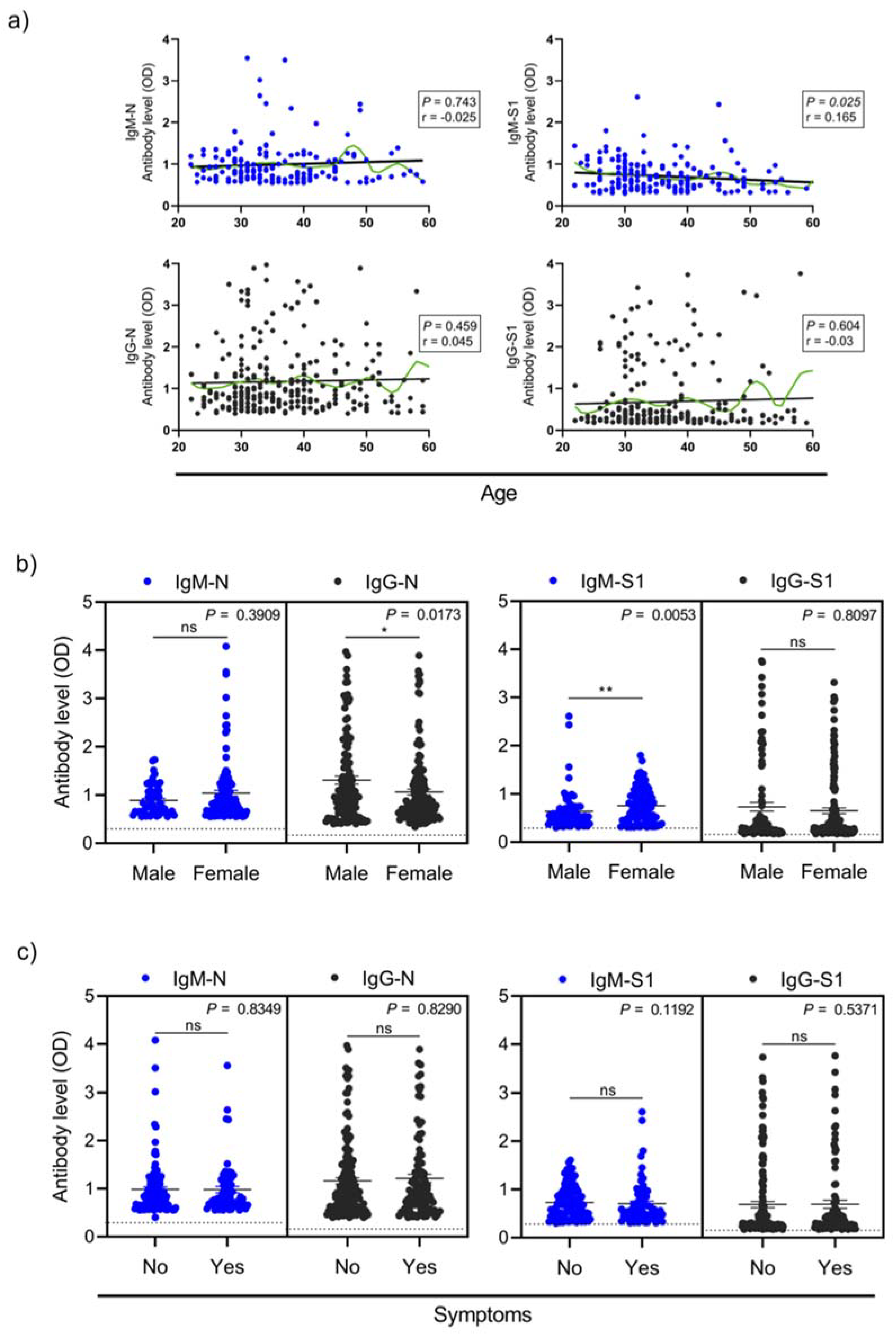
3.3. Factors Association with Seropositivity
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Basteiro, A.L.; Moncunill, G.; Tortajada, M.; Vidal, M.; Guinovart, C.; Jimenez, A.; Santano, R.; Sanz, S.; Méndez, S.; Llupià, A.; et al. Seroprevalence of antibodies against SARS-CoV-2 among health care workers in a large Spanish reference hospital. Nat. Commun. 2020, 11, 3500. [Google Scholar] [CrossRef]
- Guan, W.-J.; Ni, Z.-Y.; Hu, Y.; Liang, W.-H.; Ou, C.-Q.; He, J.-X.; Liu, L.; Shan, H.; Lei, C.-L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Day, M. Covid-19: Four fifths of cases are asymptomatic, China figures indicate. BMJ 2020, 369, m1375. [Google Scholar] [CrossRef] [Green Version]
- Sutton, D.; Fuchs, K.; D’Alton, M.; Goffman, D. Universal Screening for SARS-CoV-2 in Women Admitted for Delivery. N. Engl. J. Med. 2020, 382, 2163–2164. [Google Scholar] [CrossRef]
- Mizumoto, K.; Kagaya, K.; Zarebski, A.; Chowell, G. Estimating the asymptomatic proportion of coronavirus disease 2019 (COVID-19) cases on board the Diamond Princess cruise ship, Yokohama, Japan. Eurosurveillance 2020, 25, 2000180. [Google Scholar] [CrossRef] [Green Version]
- Ng, K.; Poon, B.H.; Puar, T.H.K.; Quah, J.L.S.; Loh, W.J.; Wong, Y.-J.; Tan, T.Y.; Raghuram, J. COVID-19 and the Risk to Health Care Workers: A Case Report. Ann. Intern. Med. 2020, 172, 766–767. [Google Scholar] [CrossRef] [Green Version]
- Black, J.R.M.; Bailey, C.; Przewrocka, A.; Dijkstra, K.K.; Swanton, C. COVID-19: The case for health-care worker screening to prevent hospital transmission. Lancet 2020, 395, 1418–1420. [Google Scholar] [CrossRef]
- Algaissi, A.; Alfaleh, M.A.; Hala, S.; Abujamel, T.S.; Alamri, S.S.; Almahboub, S.A.; Alluhaybi, K.A.; Hobani, H.I.; Alsulaiman, R.M.; AlHarbi, R.H.; et al. SARS-CoV-2 S1 and N-based serological as-says reveal rapid seroconversion and induction of specific antibody response in COVID-19 patients. Sci. Rep. 2020, 10, 16561. [Google Scholar] [CrossRef] [PubMed]
- Almahboub, S.A.; Algaissi, A.; AlFaleh, M.A.; ElAssouli, M.-Z.; Hashem, A.M. Evaluation of Neutralizing Antibodies against Highly Pathogenic Coronaviruses: A Detailed Protocol for a Rapid Evaluation of Neutralizing Antibodies Using Vesicular Stomatitis Virus Pseudovirus-Based Assay. Front. Microbiol. 2020, 11. [Google Scholar] [CrossRef]
- Alserehi, H.A.; Alqunaibet, A.M.; Al-Tawfiq, J.A.; Alharbi, N.K.; Alshukairi, A.N.; Alanazi, K.H.; Mohammed, G.; Saleh, B.; Alshehri, A.M.; Almasoud, A.; et al. Seroprevalence of SARS-CoV-2 (COVID-19) among healthcare workers in Saudi Arabia: Comparing case and control hospitals. Diagn. Microbiol. Infect. Dis. 2021, 99, 115273. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, W.A.; Dada, A.; Alshukairi, A.N.; Sohrab, S.S.; Faizo, A.A.; Tolah, A.M.; El-Kafrawy, S.A.; Bajrai, L.H.; Moalim, H.M.; Aly, M.H.; et al. Seroprevalence of neutralizing antibodies to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) among healthcare workers in Makkah, Saudi Arabia. J. King Saud Univ. Sci. 2021, 33, 101366. [Google Scholar] [CrossRef] [PubMed]
- Tian, S.; Hu, N.; Lou, J.; Chen, K.; Kang, X.; Xiang, Z.; Chen, H.; Wang, D.; Liu, N.; Liu, D.; et al. Characteristics of COVID-19 infection in Beijing. J. Infect. 2020, 80, 401–406. [Google Scholar] [CrossRef] [Green Version]
- Htun, H.L.; Lim, D.W.; Kyaw, W.M.; Loh, W.-N.J.; Lee, L.T.; Ang, B.; Chow, A. Responding to the COVID-19 Outbreak in Singapore: Staff Protection and Staff Temperature and Sickness Surveillance Systems. Clin. Infect. Dis. 2020, 71, 1947–1952. [Google Scholar] [CrossRef]
- Dobaño, C.; Vidal, M.; Santano, R.; Jiménez, A.; Chi, J.; Barrios, D.; Ruiz-Olalla, G.; Melero, N.R.; Carolis, C.; Parras, D.; et al. Highly Sensitive and Specific Multiplex Antibody Assays To Quantify Immunoglobulins M, A, and G against SARS-CoV-2 Antigens. J. Clin. Microbiol. 2021, 59, e01731-20. [Google Scholar] [CrossRef] [PubMed]
- Burbelo, P.D.; Riedo, F.X.; Morishima, C.; Rawlings, S.; Smith, D.; Das, S.; Strich, J.R.; Chertow, D.S.; Davey, R.T.; Cohen, J.I. Sensitivity in Detection of Antibodies to Nucleocapsid and Spike Proteins of Severe Acute Respiratory Syndrome Coronavirus 2 in Patients with Coronavirus Disease. J. Infect. Dis. 2020, 222, 206–213. [Google Scholar] [CrossRef]
- Jonsdottir, H.R.; Bielecki, M.; Siegrist, D.; Buehrer, T.W.; Zust, R.; Deuel, J.W. Titers of Neutralizing Antibodies against SARS-CoV-2 Are Independent of Symptoms of Non-Severe COVID-19 in Young Adults. Viruses 2021, 13, 284. [Google Scholar] [CrossRef] [PubMed]
- Rydyznski Moderbacher, C.; Ramirez, S.I.; Dan, J.M.; Grifoni, A.; Hastie, K.M.; Weiskopf, D.; Belanger, S.; Abbott, R.K.; Kim, C.; Choi, J.; et al. Antigen-Specific Adaptive Immunity to SARS-CoV-2 in Acute COVID-19 and Associations with Age and Disease Severity. Cell 2020, 183, 996–1012.e19. [Google Scholar] [CrossRef] [PubMed]
- Baumgarth, N.; Nikolich-Zugich, J.; Lee, F.E.; Bhattacharya, D. Antibody Responses to SARS-CoV-2: Let’s Stick to Known Knowns. J. Immunol. 2020, 205, 2342–2350. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhang, L.; Sang, L.; Ye, F.; Ruan, S.; Zhong, B.; Song, T.; Alshukairi, A.N.; Chen, R.; Zhang, Z.; et al. Kinetics of viral load and antibody response in relation to COVID-19 severity. J. Clin. Investig. 2020, 130, 5235–5244. [Google Scholar] [CrossRef]
- Hashem, A.M.; Algaissi, A.; Almahboub, S.A.; AlFaleh, M.A.; Abujamel, T.S.; Alamri, S.S.; Alluhaybi, K.A.; Hobani, H.I.; Alharbi, R.H.; Alsulaiman, R.M.; et al. Early Humoral Response Correlates with Disease Severity and Outcomes in COVID-19 Patients. Viruses 2020, 12, 1390. [Google Scholar] [CrossRef] [PubMed]
- Marot, S.; Malet, I.; Leducq, V.; Zafilaza, K.; Sterlin, D.; Planas, D.; Gothland, A.; Jary, A.; Dorgham, K.; Bruel, T.; et al. Rapid decline of neutralizing antibodies against SARS-CoV-2 among infected healthcare workers. Nat. Commun. 2021, 12, 844. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Category | Number of Participants n (%) |
|---|---|---|
| Overall | 693 | |
| Gender | Male | 346 (49.9%) |
| Female | 347 (50.1%) | |
| Age a | 36.5 ± 8.1 | |
| Professional category | HCW | 557 (80.4%) |
| Non HCW | 136 (19.6%) | |
| Site | Referral hospitals | 584 (84.3%) |
| Quarantine sites | 109 (15.7%) | |
| Working in COVID-19 unit | Yes | 170 (24.5%) |
| No | 523 (75.5%) | |
| Diagnosed previously with COVID-19 | Yes | 31 (4.5%) |
| No | 662 (95.5%) | |
| Diagnosed previously with MERS | Yes | 3 (0.4%) |
| No | 690 (99.6) | |
| Reported any COVID-19 related symptoms | Yes | 276 (39.8%) |
| No | 417 (60.2%) |
| Total (n) | Seropositivity n (%; 95% CI) | ||||
|---|---|---|---|---|---|
| Anti-N IgM ± IgG | Anti-S1 IgM ± IgG | nAbs | |||
| Overall | 693 | 272 (39.3%; 35.7–42.9) | 264 (38.1%; 34.5–41.7) | 223 (32.2%; 28.8–35.8) | |
| Gender | Male | 346 | 118 (34.1%; 29.3–39.3) | 114 (33.0%; 28.2–38.1) | 98 (28.3%; 23.8–33.3) |
| Female | 347 | 154 (44.4%; 39.2–49.6) | 150 (43.2%; 38.1–48.5) | 125 (36.0%; 31.2–41.2) | |
| Age group | >36 | 378 | 155 (41.0%; 36.2–46.0) | 150 (39.7%; 34.9–44.7) | 127 (33.6%; 29.0–38.5) |
| <36 | 315 | 117 (37.1%; 32.0–42.6) | 114 (36.2%; 31.1–41.6) | 96 (30.5%; 25.7–35.8) | |
| Professional category | HCW | 557 | 225 (40.4%; 36.4–44.5) | 221 (39.7%; 35.7–43.8) | 182 (32.7%; 28.9–36.7) |
| Admin | 136 | 47 (34.6%; 27.1–42.9) | 43 (31.6%; 24.4–39.9) | 41 (30.2%; 23.1–38.3) | |
| Site | Referral hospitals | 584 | 246 (42.1%; 38.2–46.2) | 238 (40.8%; 36.8–44.8) | 207 (35.5%; 31.7–39.4) |
| Quarantine sites | 109 | 26 (23.9%; 16.8–32.6) | 26 (23.9%; 16.8–32.6) | 16 (14.7%; 9.2–22.5) | |
| Working in COVID-19 unit | 170 | 55 (32.4%; 25.8–39.7) | 55 (32.4%; 25.8–39.7) | 47 (27.7%; 21.5–34.8) | |
| Diagnosed previously with COVID-19 | 31 | 26 (83.9%; 67.4–92.9) | 26 (83.9%; 67.4–92.9) | 26 (83.9%; 67.4–92.9) | |
| Diagnosed previously with MERS | 3 | 3 (100%; 43.9–100) | 3 (100%; 43.9–100) | 3 (100%; 43.9–100) | |
| Reported any COVID-19 related symptoms | 276 | 107 (38.8%; 33.2–44.6) | 101 (36.6%; 31.1–42.4) | 83 (30.1%; 25.0–35.7) | |
| Characteristic | Category | Seronegative | Seropositive | p Value | Univariable Analysis | Multivariable Analysis | |
|---|---|---|---|---|---|---|---|
| (n = 470) | (n = 223) | OR (95% CI) | OR (95% CI) | p Value | |||
| Gender a | Male Female | 248 (52.8%) 222 (47.2%) | 98 (43.9%) 125 (56.1%) | 0.030 b | 1 1.41 (1.03–1.95) | 1 1.59 (1.14–2.23) | 0.006 e |
| Age c | 36 ± 8.1 | 37 ± 8.0 | 0.860 d | 1.04 (0.75–1.44) | |||
| Professional category a | HCW Admin | 375 (79.8%) 95 (20.2%) | 182 (81.6%) 41 (18.4%) | 0.572 b | 1 1.12 (0.75–1.70) | 1 1.03 (0.67–1.59) | 0.877 e |
| Working in COVID-19 unit a | Yes No | 123 (26.2%) 347 (73.8%) | 47 (21.1%) 176 (78.9%) | 0.145 b | 0.75 (0.51–1.09) 1 | ||
| Diagnosed previously with COVID-19 a | Yes No | 5 (1.1%) 465 (98.9%) | 26 (11.7%) 197 (88.3%) | <0.0001 b | 12.27 (5.04–36.7) 1 | 13.4 (5.48–40.4) 1 | <0.0001 e |
| Diagnosed previously with MERS a | Yes No | 0 (0%) 470 (100%) | 3 (1.3%) 220 (98.7%) | 0.012 b | |||
| Reported any COVID-19 related symptoms a | Yes No | 193 (41.1%) 277 (58.9%) | 83 (37.2%) 140 (62.8%) | 0.334 b | 0.84 (0.60–1.17) 1 | ||
| Total (n = 693) | Seropositive a (n = 223) | Seronegative a (n = 470) | p Value b | ||
|---|---|---|---|---|---|
| Headache | Yes No | 182 (26.3%) 511 (73.7%) | 59 (26.5%) 164 (73.5%) | 123 (26.2%) 347 (73.8%) | 0.936 |
| Dry throat | Yes No | 149 (21.5%) 544 (78.5%) | 40 (17.9%) 183 (82.1%) | 109 (23.2%) 361 (76.8%) | 0.116 |
| Diarrhea | Yes No | 91 (13.1%) 602 (86.9%) | 25 (11.2%) 198 (88.8%) | 66 (14.0%) 404 (86.0%) | 0.303 |
| Fever | Yes No | 61 (8.8%) 632 (91.2%) | 21 (9.4%) 202 (90.6%) | 40 (8.5%) 430 (91.5%) | 0.694 |
| Ageusia | Yes No | 47 (6.8%) 646 (93.2%) | 19 (8.5%) 204 (91.5%) | 28 (6.0%) 442 (94%) | 0.210 |
| Anosmia | Yes No | 44 (6.4%) 649 (93.6%) | 18 (8.1%) 205 (91.9%) | 26 (5.5%) 444 (94.5%) | 0.200 |
| Nausea/vomiting | Yes No | 43 (6.2%) 650 (93.8%) | 11 (4.9%) 212 (95.1%) | 32 (6.8%) 438 (93.2%) | 0.339 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alhabbab, R.Y.; Alsaieedi, A.; Algaissi, A.; Almahboub, S.; Al-Raddadi, R.M.; Shabouni, O.I.; Alhabbab, R.; Alfaraj, A.A.; Alamri, S.S.; Aljehani, N.D.; et al. Seroprevalence of SARS-CoV-2 Binding and Neutralizing Antibodies in Healthcare Workers during the Epidemic Peak in Referral Hospitals and Quarantine Sites: Saudi Arabia. Viruses 2021, 13, 1413. https://0-doi-org.brum.beds.ac.uk/10.3390/v13071413
Alhabbab RY, Alsaieedi A, Algaissi A, Almahboub S, Al-Raddadi RM, Shabouni OI, Alhabbab R, Alfaraj AA, Alamri SS, Aljehani ND, et al. Seroprevalence of SARS-CoV-2 Binding and Neutralizing Antibodies in Healthcare Workers during the Epidemic Peak in Referral Hospitals and Quarantine Sites: Saudi Arabia. Viruses. 2021; 13(7):1413. https://0-doi-org.brum.beds.ac.uk/10.3390/v13071413
Chicago/Turabian StyleAlhabbab, Rowa Y., Ahdab Alsaieedi, Abdullah Algaissi, Sara Almahboub, Rajaa M. Al-Raddadi, Omaima I. Shabouni, Rahaf Alhabbab, Abdulelah A. Alfaraj, Sawsan S. Alamri, Najwa D. Aljehani, and et al. 2021. "Seroprevalence of SARS-CoV-2 Binding and Neutralizing Antibodies in Healthcare Workers during the Epidemic Peak in Referral Hospitals and Quarantine Sites: Saudi Arabia" Viruses 13, no. 7: 1413. https://0-doi-org.brum.beds.ac.uk/10.3390/v13071413