
Clinical Evaluation of In-House-Produced 3D-Printed Nasopharyngeal Swabs for COVID-19 Testing


 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. 3D Printing
2.2. Sterilization
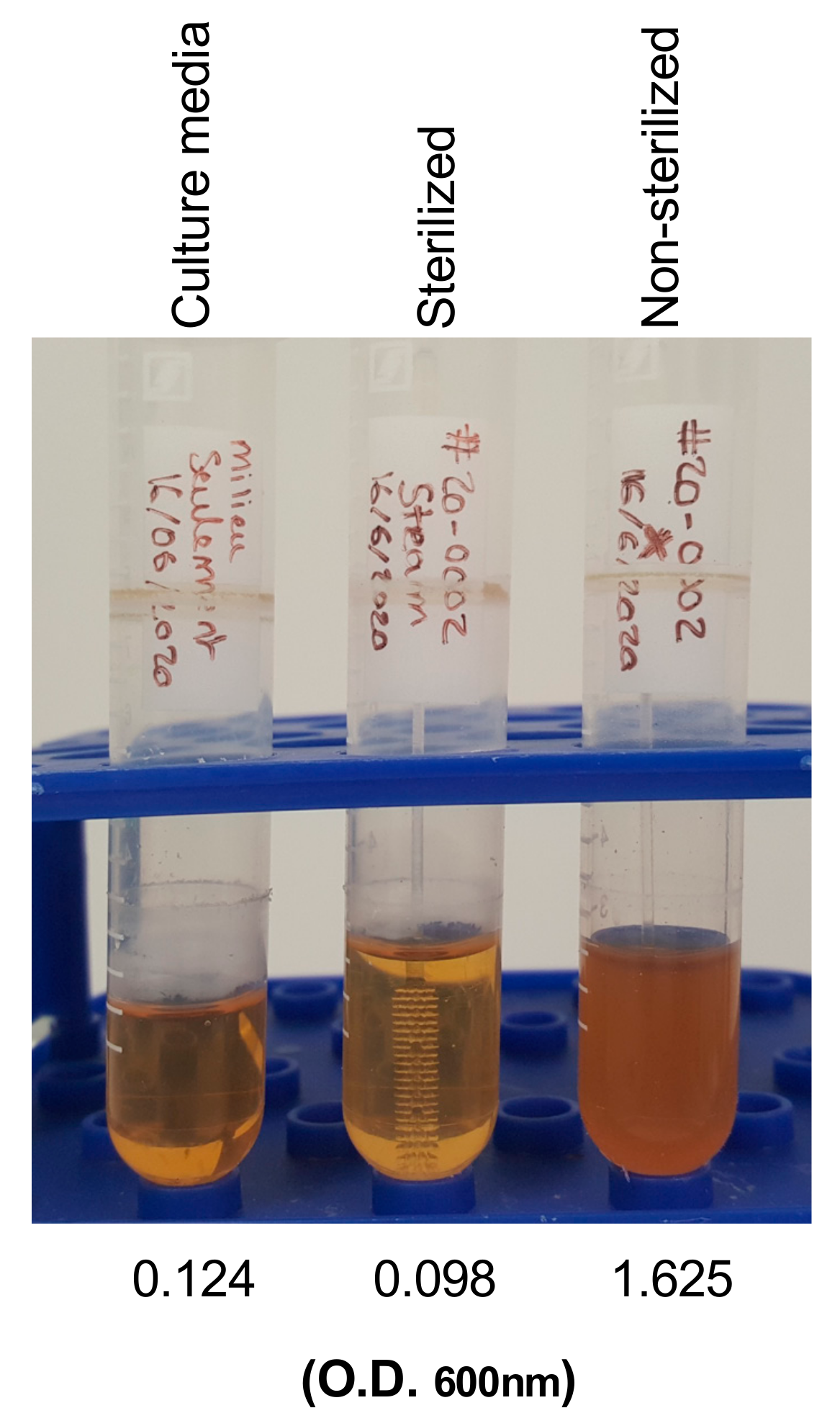
2.3. Quality Control
2.4. 3D Swab Clinical Evaluation and Study Participant Recruitment
2.5. Oro-Nasopharyngeal Swab Collection and SARS-CoV-2 PCR Testing
2.6. Statistical Analysis
3. Results
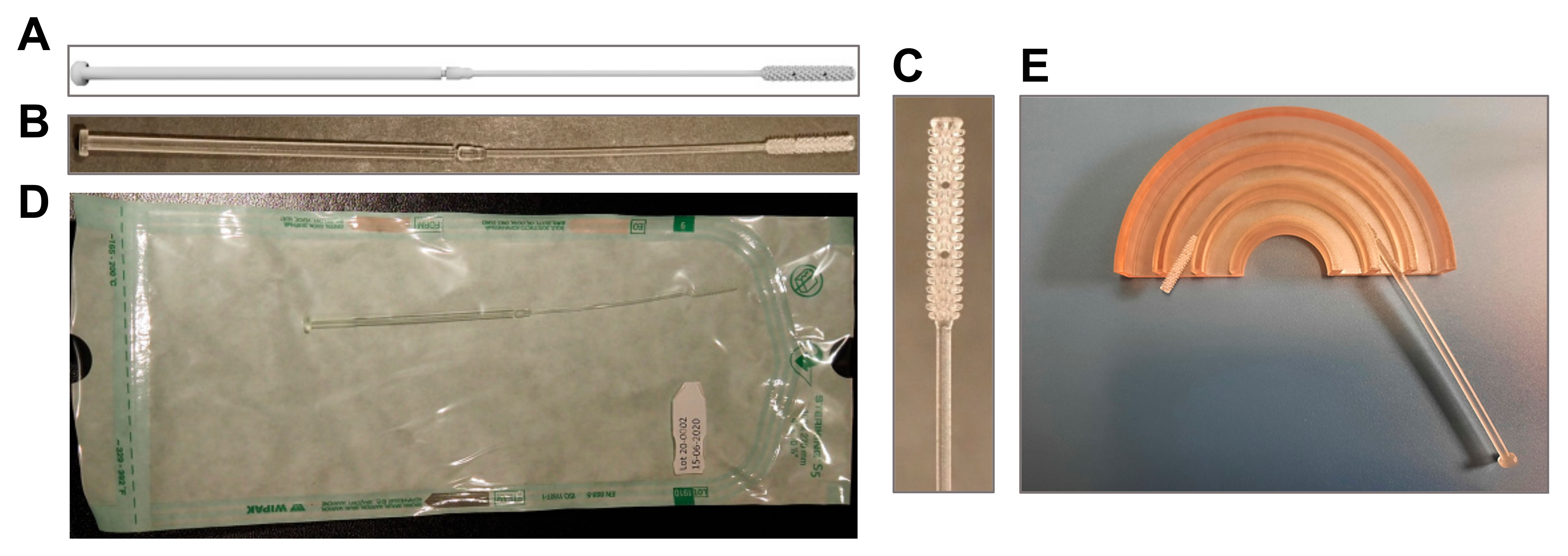
3.1. 3D-Printed Swab Model
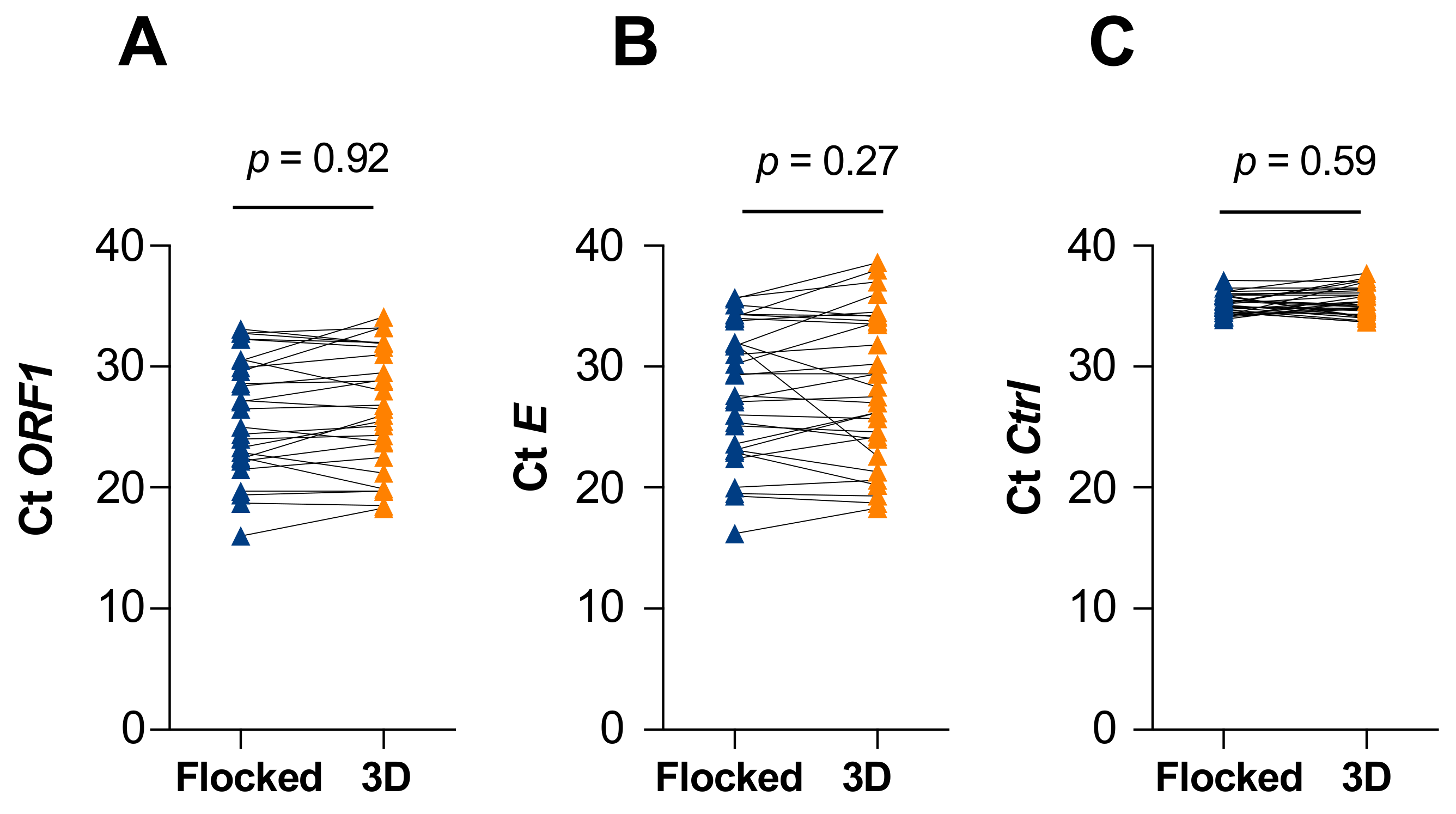
3.2. Clinical Testing
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Sanche, S.; Lin, Y.T.; Xu, C.; Romero-Severson, E.; Hengartner, N.; Ke, R. The Novel Coronavirus, 2019-nCoV, is Highly Contagious and More Infectious Than Initially Estimated. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Zheng, J. SARS-CoV-2: An Emerging Coronavirus that Causes a Global Threat. Int. J. Biol. Sci. 2020, 16, 1678–1685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19—11 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 1 March 2021).
- Cheng, M.P.; Papenburg, J.; Desjardins, M.; Kanjilal, S.; Quach, C.; Libman, M.; Dittrich, S.; Yansouni, C.P. Diagnostic Testing for Severe Acute Respiratory Syndrome-Related Coronavirus 2: A Narrative Review. Ann. Intern. Med. 2020, 172, 726–734. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, H.; Liu, Q.; Hu, J.; Zhou, M.; Yu, M.Q.; Li, K.Y.; Xu, D.; Xiao, Y.; Yang, J.Y.; Lu, Y.J.; et al. Nasopharyngeal Swabs Are More Sensitive Than Oropharyngeal Swabs for COVID-19 Diagnosis and Monitoring the SARS-CoV-2 Load. Front Med. 2020, 7, 334. [Google Scholar] [CrossRef] [PubMed]
- Choong, Y.Y.C.; Tan, H.W.; Patel, D.C.; Choong, W.T.N.; Chen, C.-H.; Low, H.Y.; Tan, M.J.; Patel, C.D.; Chua, C.K. The global rise of 3D printing during the COVID-19 pandemic. Nat. Rev. Mater. 2020, 5, 637–639. [Google Scholar] [CrossRef]
- Ford, J.; Goldstein, T.; Trahan, S.; Neuwirth, A.; Tatoris, K.; Decker, S. A 3D-printed nasopharyngeal swab for COVID-19 diagnostic testing. 3D Print. Med. 2020, 6, 21. [Google Scholar] [CrossRef] [PubMed]
- Rybicki, F.J. 3D Printing in Medicine: COVID-19 Testing with 3D Printed Nasopharyngeal Swabs. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Decker, S.J.; Goldstein, T.A.; Ford, J.M.; Teng, M.N.; Pugliese, R.S.; Berry, G.J.; Pettengill, M.; Silbert, S.; Hazelton, T.R.; Wilson, J.W.; et al. 3D Printed Alternative to the Standard Synthetic Flocked Nasopharyngeal Swabs Used for COVID-19 testing. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Spadaccini, C.; Duoss, E.; Shusteff, M.; Tooker, A.; Haque, R. Swab Tensile Testing Results and Procedures; USDOE National Nuclear Security Administration. Available online: https://www.osti.gov/servlets/purl/1623349/ (accessed on 1 March 2021).
- Albert, H.; Davies, D.J.; Woodson, L.P.; Soper, C.J. Biological indicators for steam sterilization: Characterization of a rapid biological indicator utilizing Bacillus stearothermophilus spore-associated alpha-glucosidase enzyme. J. Appl. Microbiol. 1998, 85, 865–874. [Google Scholar] [CrossRef] [PubMed]
- Boutin, C.A.; Grandjean-Lapierre, S.; Gagnon, S.; Labbé, A.C.; Charest, H.; Roger, M.; Coutlée, F. Comparison of SARS-CoV-2 detection from combined nasopharyngeal/oropharyngeal swab samples by a laboratory-developed real-time RT-PCR test and the Roche SARS-CoV-2 assay on a cobas 8800 instrument. J. Clin. Virol. 2020, 132, 104615. [Google Scholar] [CrossRef] [PubMed]
- Fleiss, J.L. Statistical Methods for Rates and Proportions, 2nd ed.; Wiley, John and Sons, Incorporated: New York, NY, USA, 1981. [Google Scholar]
- Canada, H. Health Canada Expedites Access to COVID-19 Diagnostic Laboratory Test Kits and Other Medical Devices. Available online: https://www.canada.ca/en/health-canada/news/2020/03/health-canada-expedites-access-to-covid-19-diagnostic-laboratory-test-kits-and-other-medical-devices.html (accessed on 1 March 2021).
- Callahan, C.J.; Lee, R.; Zulauf, K.E.; Tamburello, L.; Smith, K.P.; Previtera, J.; Cheng, A.; Green, A.; Abdul Azim, A.; Yano, A.; et al. Open Development and Clinical Validation of Multiple 3D-Printed Nasopharyngeal Collection Swabs: Rapid Resolution of a Critical COVID-19 Testing Bottleneck. J. Clin. Microbiol. 2020, 58, e00876-20. [Google Scholar] [CrossRef] [PubMed]
- Oland, G.; Garner, O.; de St Maurice, A. Prospective clinical validation of 3D printed nasopharyngeal swabs for diagnosis of COVID-19. Diagn. Microbiol. Infect. Dis. 2021, 99, 115257. [Google Scholar] [CrossRef] [PubMed]
- Sharma, N.; Cao, S.; Msallem, B.; Kunz, C.; Brantner, P.; Honigmann, P.; Thieringer, F.M. Effects of Steam Sterilization on 3D Printed Biocompatible Resin Materials for Surgical Guides-An Accuracy Assessment Study. J. Clin. Med. 2020, 9, 1506. [Google Scholar] [CrossRef] [PubMed]
- Sabino, E.C.; Buss, L.F.; Carvalho, M.P.S.; Prete, C.A., Jr.; Crispim, M.A.E.; Fraiji, N.A.; Pereira, R.H.M.; Parag, K.V.; da Silva Peixoto, P.; Kraemer, M.U.G.; et al. Resurgence of COVID-19 in Manaus, Brazil, despite high seroprevalence. Lancet 2021, 397, 452–455. [Google Scholar] [CrossRef]
- Abdool Karim, S.S.; de Oliveira, T. New SARS-CoV-2 Variants—Clinical, Public Health, and Vaccine Implications. N. Engl. J. Med. 2021, 384, 1866–1868. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Flocked Mean Ct | 3D Mean Ct | Delta Ct | p-Value 1 | |
|---|---|---|---|---|
| ORF1 | 26.06 | 26.51 | 0.44 | 0.92 |
| E | 28.03 | 28.30 | 0.26 | 0.27 |
| Ctrl | 35.16 | 35.35 | 0.19 | 0.59 |
| A | |||||
|---|---|---|---|---|---|
| 3D | 3D | 3D | Total | ||
| + | - | not conclusive | |||
| Flocked | + | 30 | 1 | 0 | 31 |
| Flocked | - | 1 | 31 | 0 | 32 |
| Flocked | not conclusive | 0 | 0 | 0 | 0 |
| Total | 31 | 32 | 0 | 63 | |
| B | |||||
| Concordance | % | 95% CI 1 | |||
| Positive | 96.8 | 82.4–99.9 | |||
| Negative | 96.9 | 82.9–99.9 | |||
| Total | 96.8 | 88.5–99.8 | |||
| Kappa value | 0.936 | 0.738–0.994 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grandjean Lapierre, S.; Bedwani, S.; DeBlois, F.; Fortin, A.; Zamorano Cuervo, N.; Zerouali, K.; Caron, E.; Morency-Potvin, P.; Gagnon, S.; Nguissan, N.; et al. Clinical Evaluation of In-House-Produced 3D-Printed Nasopharyngeal Swabs for COVID-19 Testing. Viruses 2021, 13, 1752. https://0-doi-org.brum.beds.ac.uk/10.3390/v13091752
Grandjean Lapierre S, Bedwani S, DeBlois F, Fortin A, Zamorano Cuervo N, Zerouali K, Caron E, Morency-Potvin P, Gagnon S, Nguissan N, et al. Clinical Evaluation of In-House-Produced 3D-Printed Nasopharyngeal Swabs for COVID-19 Testing. Viruses. 2021; 13(9):1752. https://0-doi-org.brum.beds.ac.uk/10.3390/v13091752
Chicago/Turabian StyleGrandjean Lapierre, Simon, Stéphane Bedwani, François DeBlois, Audray Fortin, Natalia Zamorano Cuervo, Karim Zerouali, Elise Caron, Philippe Morency-Potvin, Simon Gagnon, Nakome Nguissan, and et al. 2021. "Clinical Evaluation of In-House-Produced 3D-Printed Nasopharyngeal Swabs for COVID-19 Testing" Viruses 13, no. 9: 1752. https://0-doi-org.brum.beds.ac.uk/10.3390/v13091752